
LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability

1
Institute for Mental Health Policy Research, Centre for Addictions and Mental Health, Toronto, ON M6J 1H4, Canada
2
Dalla Lana School of Public Health, University of Toronto, Toronto, ON M5T 3M7, Canada
3
Ontario Institute for Studies in Education, University of Toronto, Toronto, ON M5S 1V6, Canada
4
Schulich School of Medicine & Dentistry, Western University, London, ON N6A 3K7, Canada
5
Strategic Foresight and Innovation Program, OCAD University, Toronto, ON M5T 1W1, Canada
*
Author to whom correspondence should be addressed.
Youth 2023, 3(1), 93-106; https://doi.org/10.3390/youth3010006
Submission received: 1 December 2022
/
Revised: 30 December 2022
/
Accepted: 9 January 2023
/
Published: 12 January 2023
(This article belongs to the Special Issue LGBTIQ+ Youth: Experiences, Needs, and Aspirations)
Abstract
:This study explores the experiences of LGBTQ2S+ youth while accessing mental health and substance use care services during the COVID-19 pandemic. Through a series of facilitated virtual meetings, 33 LGBTQ2S+ youth from across Ontario participated in collaborative activities to identify barriers they have experienced when accessing mental health services, as well as potential solutions to these barriers. Discussions were recorded, transcribed, and analyzed using thematic analysis. The study revealed that LGBTQ2S+ youth disproportionately experience bias, discrimination, and heteronormative assumptions when accessing mental health services, resulting in negative care experiences. Youth also reported insufficient availability of quality care, little continuity in care, and a lack of educated providers capable of effectively addressing the needs of the community. Potential solutions proposed by youth include training resources for providers, LGBTQ2S+ specific care centers, better continuity of care, and assessments to ensure care providers are culturally competent. These results show the COVID-19 pandemic has exacerbated the disparities LGBTQ2S+ youth experience when accessing mental health services and highlight the urgent need to implement policies and programs that will advance the standards of care for LGBTQ2S+ youth.
1. Introduction
Lesbian, gay, bisexual, transgender, queer, questioning, and 2-spirit (LGBTQ2S+) youth and young adults are more likely to experience mental health problems, suicidality, and substance use problems in comparison to their heterosexual counterparts [1]. Global studies have shown that discrimination, stigma, and minority stress contribute towards this heightened risk [2,3,4,5,6,7]. Shared experiences such as social exclusion, violence, and peer bullying were found across a wide berth of studies on this population [2,3,4,5,6,7]. Cisnormative and heteronormative biases of mental health (MH) care institutions are known to create barriers for LGBTQ2S+ youth who attempt to access these services [8]. Thus, it is essential to establish a culturally safe environment for LGBTQ2S+ youth accessing MH care.
The concept of cultural safety refers to “providing a focus for the delivery of quality care and through changes in thinking about power relations and patients’ rights” [9] (p. 3). Cultural safety recognizes the multiple barriers that prevent minority communities from accessing safe and affirming care [9]. The clinician can create a culturally safe environment by using reflexive practices and offering clients autonomy over their personal health decisions [9]. Previous research has demonstrated that negative experiences with healthcare providers contribute to “the erosion of a sense of safety in the healthcare system” [2] (p. 8).
Health inequities experienced by queer youth have been exasperated throughout the COVID-19 pandemic, which has enhanced the vulnerability of this population [7]. During COVID-19, LGBTQ2S+ youth are at risk of experiencing higher rates of domestic abuse, unstable housing, unpredictable employment, and worsening social isolation due to physical distancing and quarantine measures [7,10]. Young adulthood is a critical developmental period for LGBTQ2S+ youth and a period that requires appropriate familial, social, and professional support [10]. During COVID-19, LGBTQ2S+ youth are accessing services less than before in a time when they need these services the most. The lack of availability of services increases already present stressors and places a greater strain on LGBTQ2S+ youth seeking physical and mental health services [7]. Due to a lack of research on this population in disaster contexts, COVID-19 related policies do not consider the unique needs of LGBTQ2S+ youth [10]. Transgender youth are experiencing delays in gender-affirming treatment, such as hormone therapy, transition-related surgeries, and psychological support, which can perpetuate depression, anxiety, and suicidality [1]. More research is urgently needed to understand the specific cultural safety needs of LGBTQ2S+ youth in Canada and how providers can best meet these needs, especially within the context of the COVID-19 pandemic.
Current research indicates an urgent need for mental health policies promoting cultural safety for LGBTQ2S+ youth. Existing literature from international studies suggests that policy change can be effective in reducing mental health disparities, including halving LGBTQ+ youth suicides in schools [11,12]. Further research has demonstrated the impact of GSAs on LGBTQ2+ youth mental health [13], explored the impact of programs on intersex youth health disparities [14], and examined the effect of training and technical assistance programs for care providers working with LGBTQ2S+ youth [15]. This rich body of literature indicates that policy solutions are effective for addressing LGBTQ2S+ youth wellbeing. Research is urgently needed that expands on these findings to understand the policy needs of LGBTQ2S+ youth in Canada experiencing barriers to mental healthcare.
2. Materials and Methods
2.1. Study Aim and Design
This study is embedded in a larger research program entitled “Sexual & Gender Minority Youth Access to Services in Mental Health During the COVID-19 Pandemic” (S.M.A.S.H COVID). S.M.A.S.H COVID was a community-based participatory research project that sought to better understand the characteristics of LGBTQ2S+ youth who are facing barriers to accessing mental health and substance use care services in the context of the COVID-19 pandemic. Our research provides youth-generated ideas about the barriers LGBTQ2S+ youth face when accessing care during the pandemic, hypothetical interventions, and suggestions about how accountability and standards of care could be developed. Rees et al. suggest that research with this population should promote affirming care and seek to gain knowledge of the raw, direct experiences of LGBTQ2S+ interaction with mental health services [16]. While many studies have surveyed this population, our study uses a participatory design systems collaboration model to highlight the experience of participants, create community-led collaboration, promote equity and inclusion, and construct a trustworthy and enjoyable research process for participants. In addition, our study goes on to describe youth-suggested models for culturally safe provider training, as well as methods to ensure provider accountability.
Three participant engagement sessions were held virtually over Webex, a virtual meeting tool, in June 2021. Six facilitators consisting of LGBTQ2S+ community members and allies from the project’s planning committee, as well as graduate students from OCAD university, led the sessions.
In the first session, participants engaged in discussions about barriers sexual and gender diverse youth face when accessing mental healthcare during the COVID-19 pandemic. These discussions were mapped by a graphic illustrator in a process called Journey Mapping to reveal the holistic interactions that participants encountered during the pre-engagement, engagement, and post-engagement stages of accessing services. The sessions were audio recorded and transcribed for analysis.
In the second and third sessions, participants broke into smaller groups to design solutions to specific barriers identified in session one. They engaged in a series of structured collaborative activities (see Appendix A) to identify the problem, brainstorm solutions, and identify mechanisms for change. These activities included discussion components as well as opportunities for graphic illustration. In these sessions, participants recorded their ideas visually and in writing using Miro, a cloud-based, online white-board used for collaboration of small to mid-sized groups. Our analysis focuses on the small groups that discussed solutions and mechanisms for culturally safe care.
2.2. Study Sample and Setting
Thirty-three LGBTQ2S+ culturally diverse, English-speaking youth and young adults ages 16–29 participated in the program (see Table 1 for participant demographics). The sample was limited to LGBTQ2S+ youth currently living in Ontario and Quebec. Participants were recruited through email invitation to the PHAC 2SLGBTQI+ Campaign on Commercial Tobacco Use & Its Culture cohort network, and by referent recruitment through research team members. Participants required a computer and technological competence to be eligible, as the activities were held virtually. Informed consent was given prior to participants beginning sessions, and participants were compensated $100 after each session.
2.3. Data Analysis
Thematic analysis was used to categorize quotes from the session 1 and visuals from sessions 2 and 3 into themes of provider competencies and biases, and to identify proposed solutions and mechanisms for change.
For session 1 data, the audio recordings were transcribed, and the research team engaged in Braun and Clarke’s six stages of thematic analysis to sort the data into themes: familiarization, generation, searching, reviewing, defining, and producing [17]. Themes pertinent to participant barriers, solutions, and mechanisms for change regarding LGBTQ2S+ affirming care were established and discussed in depth.
For the visual and written data collected in sessions 2 and 3, the research team participated in the same six stages to sort the visual and written data in Miro into themes related to proposed solutions, as well as mechanisms for change.
3. Results
Results are split into two main sections. The first section, provider competencies and gaps, describes themes in session one related to youth experiences when accessing care related to provider competency. The second section, solutions to provider gaps, identifies the solutions and mechanisms for change identified by young people in this study during sessions two and three.
3.1. Provider Competencies and Gaps
Participants in session one discussed their experiences accessing MH services. While the discussion occurred, a graphic illustrator visually depicted the journey to care described by participants (see Figure 1). Analysis of these discussions revealed some positive experiences with providers, which were categorized as provider competencies, as well as negative experiences with providers, which were categorized as provider gaps. Sub-themes within provider competencies and gaps were then explored further.
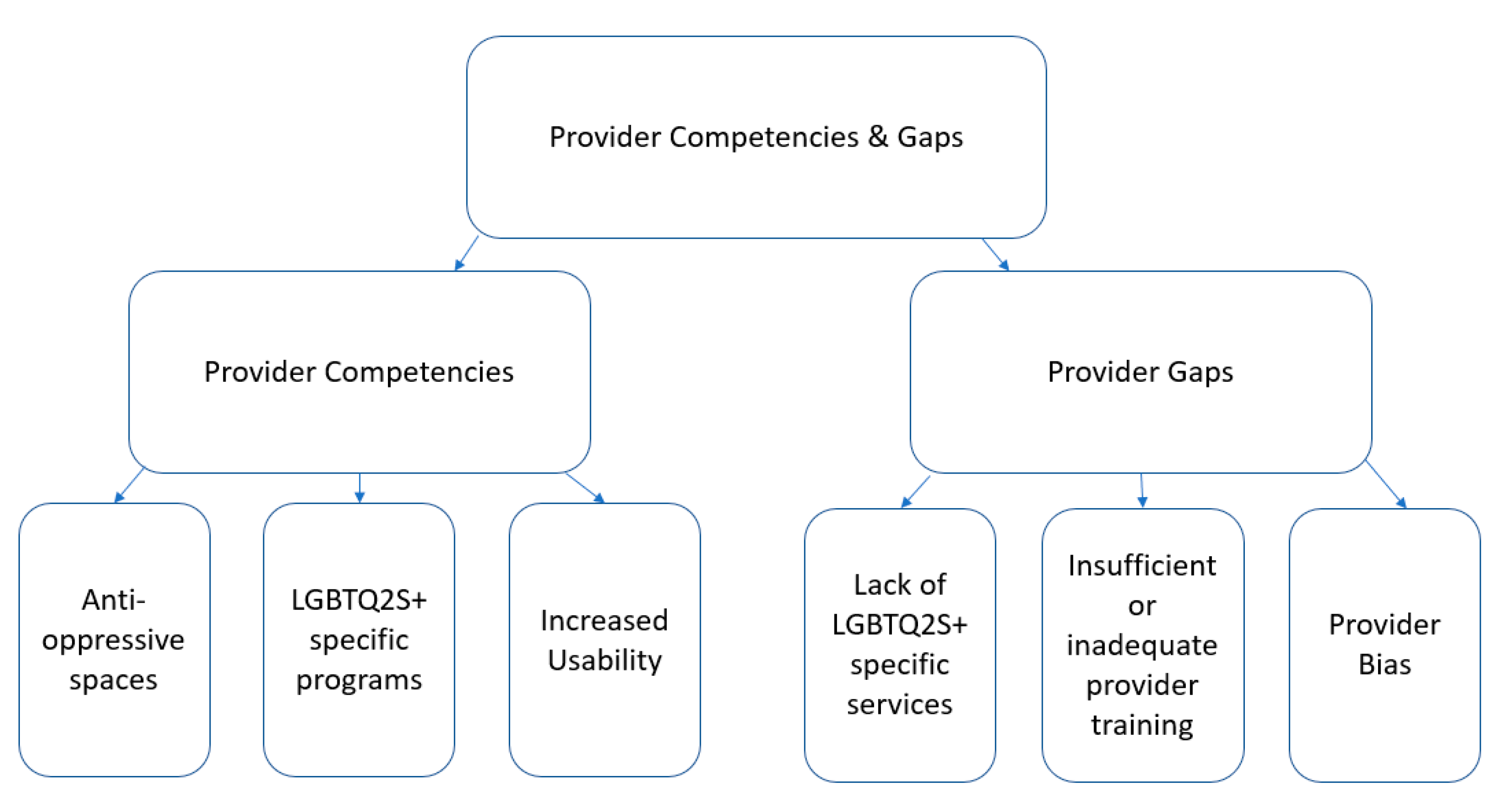
Themes addressing provider competencies included anti-oppressive spaces, LGBTQ2S+ specific programs, and increased usability due to virtual appointments/telemedicine. Themes addressing provider gaps were identified as lack of LGBTQ2S+ specific services, insufficient and/or inadequate provider training, and general provider bias. For a visual representation of themes, see Figure 2.
3.1.1. Anti-Oppressive Spaces
Participants of this study defined an anti-oppressive space as an accepting, welcoming and non-judgmental environment where youth can find the support that they need. Study participants explained that “spaces such as these involve non-judgmental and accepting professionals, occasionally individuals who are members of the community themselves, and individuals who leave their biases outside of the space”.
Participants stated that providers who were able to successfully generate anti-oppressive spaces ensured that they left any biases or preconceived notions outside of the service. Such spaces are important in ensuring cultural safety as it allows one to feel welcome, supported, and safe. Most importantly, such spaces allow LGBTQ2S+ youth to feel as though their provider understands their unique experience, and ultimately makes the service useful. Without such traits, the user cannot receive effective care, and may even be discouraged from seeking further treatment, even if additional services are needed. To add, providers who are able to create an anti-oppressive space must have an understanding of cultural safety, and actively take steps to maintain such a space, ultimately displaying competency in working with LGBTQ2S+ youth. Unfortunately, the current heteronormative and cisnormative standard of MH services does not encourage the existence of such spaces, thus participants reported that accessing anti-oppressive spaces was not an easy task.
3.1.2. LGBTQ2S+ Specific Programs
Many LGBTQ2S+ programs exist with the goal of providing specific, tailored support for youth. Study participants explained that there are a variety of programs for LGBTQ2S+ youth who are “seeking community, whether that person is [...] looking for very specific groups, like a group for people with a specific gender orientation or sexual orientation, [...] something for friends and non-binary folks, or a woman’s only space”. These identity-specific spaces enable LGBTQ2S+ youth to connect with resources tailored to their specific needs, such as “gender journeys, crisis lines, transgender competent healthcare, medication diagnosis for accommodations”. These spaces, when managed correctly, represent provider competency as they are well suited to effectively meet the needs of LGBTQ2S+ youth.
3.1.3. Virtual Usability
Participants expressed that virtual appointments reduced the anxiety that they experienced surrounding in-person appointments, and that the shift to telemedicine has improved the quality of their care in this way. One transgender participant stated that “[they] had a gender affirming surgery and I found it really helpful to not actually have to go in and talk to the doctor in person about what I was feeling and just being able to disconnect, write it down, and send it off [...] If they needed to see me, I could just take a picture, send it, delete it and not [think] about it instead of having to sit there with the anxiety of that, like someone is looking at me”. This modification to traditional healthcare services demonstrates provider competency as it facilitates access to care for LGBTQ2S individuals, particularly members of the transgender community.
3.1.4. Lack of LGBTQ2S+ Specific Services
Participants described various issues concerning the lack of available, diverse, and personalized LGBTQ2S+ services.
“I wish there would have been, they would have asked me what I think would have helped me or based on like, my culture or my personality, they would have asked me what I think would have been best, instead of just telling you this is what I’m going to do and it will make them better when it did not help.”
Standardized approaches to care can be ineffective for addressing service users’ individual needs. This is especially the case for LGBTQ2S+ youth, as service services are not always designed to attend to the particular needs of LGBTQ2S+ individuals. This lack of appropriate services results in negative experiences for youth receiving care.
This lack of affirming care was especially an issue for youth living in rural areas.
“I live in a rural community, [...] and there’s like only one therapist that I can access in my town through my family health team, if not, I have to go into the city, and [the local therapist] was very heteronormative.”
Rural LGBTQ2S+ youth often experience limited access to MH services. In addition to the limited services, the resources that are present are often not tailored to their needs. Such services tend to follow a cisnormative and heteronormative standard of care and create an additional barrier to care for rural LGBTQ2S+ youth.
3.1.5. Insufficient and Inadequate Training
Participants recounted experiences that highlighted the lack of education and awareness that various providers demonstrate.
“I would say that like for all healthcare providers, regardless of whether you’re working, specifically with LGBTQ youth, or racialized youth, and whatever, there has to be a standard of like, education and training that they go through. Like, I understand that, it doesn’t just stop once you receive like, a decree whatever letters that you offer them, like learning workshops, and I recognize that but when I say standard, I mean, like mandatory anti oppressive training. [...] I think it just be a standard for anyone who’s offering some kind of healthcare service, just so that like, you can avoid causing further trauma or like gone, just being more empathetic with patients and clients”.
Study participants stated that they found it difficult to engage with MH providers who were not knowledgeable on LGBTQ2S+ identities or other aspects of the experiences of LGBTQ2S+ youth. They stated that this knowledge gap can cause youth to feel as if they are obligated to teach the provider, or as if they must reexplain various elements of their experience many times. Both situations were explained as retraumatizing the individual, as they must relive their trauma due to homophobia and ignorance on more occasions than necessary. This provider ignorance can reduce or eliminate the effectiveness of the MH service overall. Ultimately this poses another barrier for LGBTQ2S+ youth seeking care.
3.1.6. Provider Bias
Lastly, participants attested that providers can also display general biases towards LGBTQ2S+ youth, decreasing or eliminating the effectiveness of their service.
“I had one of my counselors trying to talk me out of getting my trans affirming surgery, they said they’re playing quote, unquote, devil’s advocate, trying to tell me, I was seeking therapy because I had anxiety about going in for surgery. In addition, they were trying to talk me out of, Oh, well, do you really want the surgery? […] Encountering service providers like that can be really tough because they’re the only counseling agency that I can access”
Young people in this study indicate that it is imperative MH service providers do not allow their personal beliefs or ideologies to influence the way in which they attend to those seeking services. Whether such biases come from a lack of knowledge, ignorance, or disapproval of various communities, participants asserted that they do not belong in healthcare, and their presence threatens the safety of LGBTQ2S+ youth.
3.2. Solutions to Provider Gaps
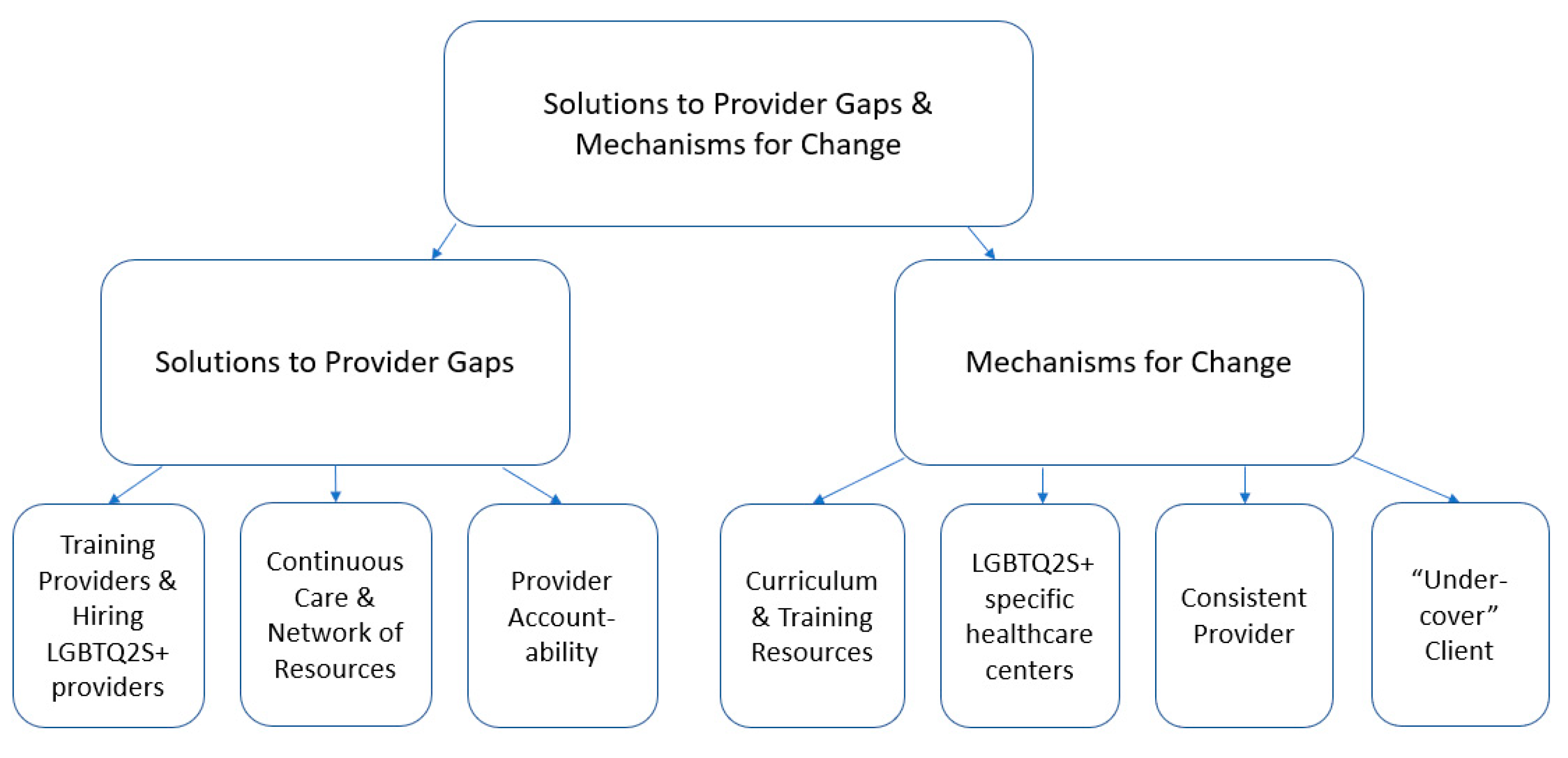
The following results highlight participant ideas for solutions to the identified provider gaps, as well as mechanisms for change. For a visual representation of these themes, see Figure 3. Youth represented their ideas visually and in writing using Miro, and the Miro board was then analyzed by the research team for themes. Young people in this study identified three solutions they believed would improve the cultural safety of LGBTQ2S+ youth when seeking MH services: training providers on LGBTQ2S+ issues and identities and hiring LGBTQ2S+ providers, ensuring patients experience continuous care and creating an extensive network of culturally safe resources, and holding providers accountable for upholding culturally safe services for LGBTQ2S+ individuals. These ideas were represented in Miro, as seen in Figure 4. They also described four mechanisms for change, including changing the curriculum and training resources for service providers, opening an LGBTQ2S+ specific healthcare center, introducing a provider at intake that stays with a patient throughout their care journey, and implementing “undercover-patient style” assessments to evaluate providers.
3.2.1. Training Providers and Hiring LGBTQ2S+ Providers
The young people in this study identified a need for provider training in LGBTQ2S+ issues and identities. The purpose of this training would be for providers to have a better understanding of the LGBTQ2S+ experience. This would prevent providers from needing to rely on service users for education in LGBTQ2+ issues and identities, and reduce the amount of unintended harm caused by uneducated providers. Ultimately, this training would improve the effectiveness of MH services for LGBTQ2S+ youth.
Similarly, hiring more providers who are members of the LGBTQ2S+ community would also offer some diversity to MH services, reducing the need for youth to explain experiences that heterosexual or cisgendered providers may not understand in the same way and allow those with lived experience to effectively assist LGBTQ2S+ youth seeking service.
3.2.2. Continuous Care and Network of Resources
Young people in this study identified that service users need to experience a more continuous form of care in order to develop a consistent and trusting relationship with their service provider. This consistent provider relationship would make it easier to for participants to disclose information and prevent them from needing to re-explain their experiences and identities.
Furthermore, young people in this study suggested LGBTQ2S+ patients would benefit greatly from a central resource that lists all available culturally safe MH resources in Ontario, so they could understand what services are available to them and select services that best suit their needs.
3.2.3. Accountability
Young people in this study felt that improvements would only be effective if MH services and service providers were held accountable for upholding their proposed ideas for a culturally safe environment. Without methods to ensure suggested changes are upheld, young people in this tidy felt it was likely that the current MH system will remain cisnormative and heteronormative, and that they would continue to experience barriers to MH care.
3.3. Mechanisms of Change
3.3.1. Updating Provider Training
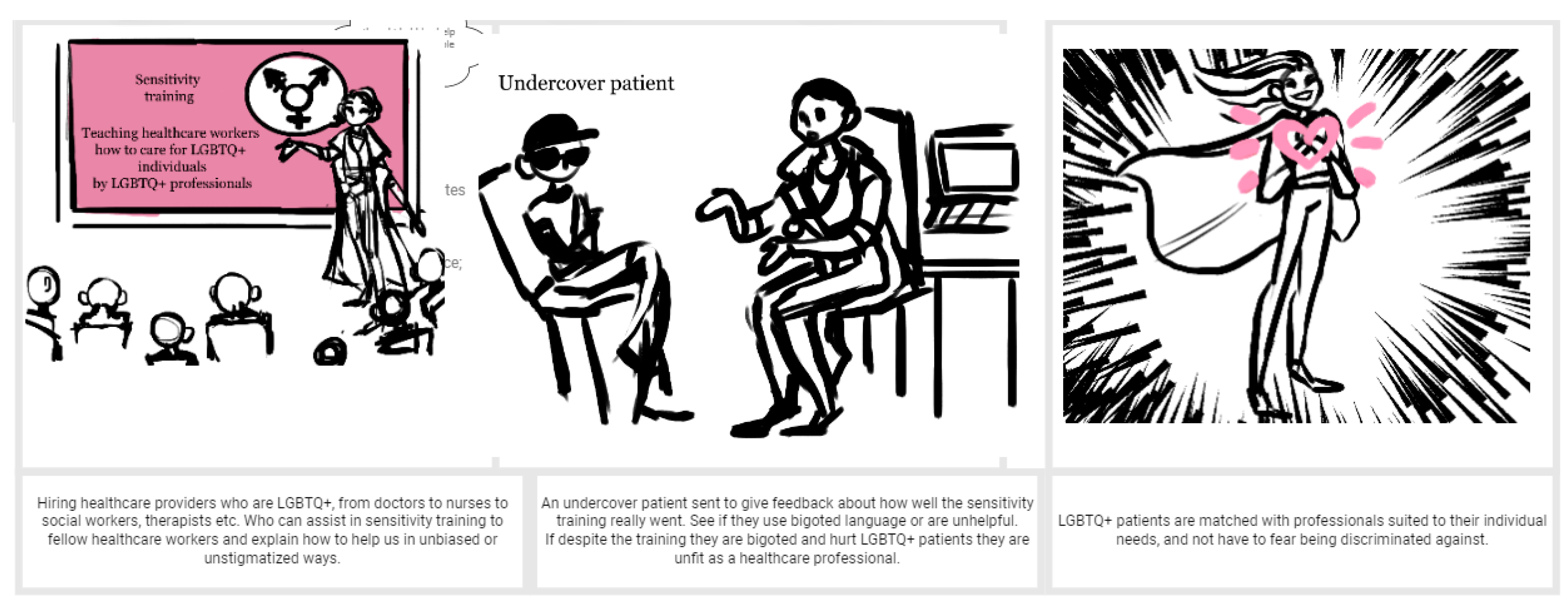
Young people in this study identified that changing the curriculum and training resources for providers should involve reviewing and conducting research involving LGBTQ2S+ youth surrounding various identities, shared experiences of sexual minorities, as well as methods of care that are most effective for the community. Then, such research should be implemented into the curriculum of all MH providers to ensure that they can competently serve LGBTQ2S+ youth. The impact of this training is demonstrated in Figure 5.
3.3.2. LGBTQ2S+ Specific Healthcare Centre
Young people in this study also suggested opening an LGBTQ2S+ specific healthcare center. Having access to these centers would ensure that LGBTQ2S+ service seekers could go to one spot where providers would be trained to understand and accommodate their unique needs. This would allow LGBTQ2S+ youth to feel comfortable, accepted, and understood, ultimately creating a culturally safe environment that would serve LGBTQ2S+ youth effectively.
3.3.3. Consistent Provider Model
Study participants suggested that, to ensure continuity of care, patients would benefit from having access to a person who is responsible for staying with a patient from their intake into the MH system all the way to the end of their journey, regardless of what that trajectory looks like. This would allow the patient to feel more comfortable navigating the MH system and provide them with more continuous care.
3.3.4. Provider Evaluation
Finally, in order to ensure providers are held accountable for upholding this proposed culturally safe environment, study participants suggested an ‘undercover boss’ style assessment in which someone would assume the role of an LGBTQ2S+ youth patient, meet with a provider, and evaluate the provider’s ability to care for a patient while they do not know that they are being assessed. This way, provider competency could be assessed without providing harm to actual service users. Figure 5 demonstrates the role of the “undercover patient” in creating culturally safe care in a graphic created by participants.
4. Discussion
Our findings show that LGBTQ2S+ youth experienced significant barriers to accessing MH care during the COVID-19 pandemic and beyond. While study participants described positive characteristics of the current MH climate for LGBTQ2S+ individuals, many gaps within the system were highlighted. LGBTQ2S+ specific programs exist; however, current services lack accessibility and diversity. Healthcare that is not tailored to the unique needs of LGBTQ2+ youth can be perceived as impersonal and ineffective and can ultimately discourage youth from attempting to seek services. Moreover, programs are not useful if youth cannot access them, or must wait for prolonged periods of time to receive care.
Current training and education do not adequately prepare MH providers to assist LGBTQ2S+ youth effectively. This can create issues for service-seeking youth when providers do not know about LGBTQ2S+ specific identities or issues and are thus unable to create culturally safe environments or effectively address their needs. Young people in this study attest that provider ignorance can be retraumatizing, as youth may have to explain their situation many times, or may feel as though they are teaching their MH provider about certain terms, identities, or even the complexities of various issues through the lens of an LGBTQ2S+ individual. Finally, the participants of our study described experiences with MH providers who displayed a bias towards LGBTQ2S+ youth, resulting in ineffectual services, and discouraging youth from seeking help from MH services at all.
These findings align with previous research which has addressed the lack of availability of culturally safe MH services. Qualitative studies addressing LGBTQ2S+ MH service seekers have revealed that availability, accessibility, acceptability, and quality of MH services were common issues that LGBTQ2S+ service users face when seeking healthcare, and that these issues cause LGBTQ2S+ individuals to delay or avoid seeking care [8]. The barriers described by young people in our study also align with existing research demonstrating that LGBTQ2S+ youth experience discrimination not only within healthcare but within their broader communities as well, and that this discrimination results in higher rates of mental health concerns and barriers to access [2,3,4,5,6,7].
Subsequently, youth discussed ideas to improve the cultural safety of LGBTQ2S+ youth seeking MH services, as well as methods to ensure providers are held accountable to maintain such practices. There is a dearth of research exploring LGBTQ2S+ youth-proposed solutions and mechanisms for change to create more culturally safe MH care experiences. This study is the first of its kind to our knowledge to use a collaborative design model to create LGBTQ2S+ youth-proposed solutions to barriers to MH care.
Young people in this study proposed that MH providers receive improved training and education surrounding the treatment of LGBTQ2S+ individuals and employ more LGBTQ2S+ service providers. These suggestions aim to reduce the amount of provider bias and ignorance towards the LGBTQ2S+ community, increasing the effectiveness of care. This would create a safer and more welcoming environment for LGBTQ2S+ youth, as well as increase the diversity of LGBTQ2S+ services. This echoes existing literature which suggests that MH providers receive sensitization training and LGBTQ2S+ health-specific professional development courses to adequately prepare them to handle the unique needs to of the LGBTQ2S+ community [8].
Study participants also proposed creating an LGBTQ2S+ specific healthcare center, and the addition of an MH provider who focuses on intake and would follow the patient throughout their journey when seeking care from beginning to end. This suggestion intends to increase accessibility of care for LGBTQ2S+ patients, create a centralized resource for various forms of healthcare, and improve the continuity of care a patient would experience.
Lastly, study participants recommended the implementation of an ‘undercover patient’ style of MH provider assessment to ensure provider accountability. In this assessment, a MH professional would assume the role of a patient, make an appointment with a provider, and assess their effectiveness. This form of assessment is proposed to determine the reality of an MH service and/or provider, and to ensure that failures to maintain a culturally safe environment can be addressed.
It is important to understand our findings in the context of existing international research that has demonstrated the effectiveness of school policies, GSAs, programs for intersex youth, and training programs for providers as promising policy interventions for overcoming mental health inequities faced by LGBTQ2S+ youth [11,12,13,14,15]. This literature provides support for many of the ideas suggested by young people in this study. Our study adds to this rich body of work by confirming that many existing policy ideas align with the expressed wants and needs of LGBTQ2S+ youth, and proposing novel policy solutions, such as the undercover client proposal and increasing provider accountability.
This study is amongst the first that not only seeks to uncover the barriers that exist for LGBTQ2S+ youth, but also addresses potential interventions to create a culturally safe mental health system from the perspective of LGBTQ2S+ youth themselves. Future research should be conducted to learn more about the unique biases and barriers LGBTQ2S+ youth experience, and to explore the efficacy of novel youth-proposed interventions.
There are a few limitations to our findings. To begin, the program was limited to LGBTQ2S+ youth living in Ontario. Future studies are required to address MH provider competencies and biases in other areas in North America to develop prototypes for cultural safety and provider accountability that are suitable for the needs of different regions. Such investigations should note biases and barriers that the LGBTQ2S+ community faces on a national level in order to assist in the creation of equitable policy across multiple disciplines of healthcare.
Moreover, some participants felt they did not have enough time to elaborate on the many barriers they experienced while accessing care during our discussion. Given sufficient time and resources, future studies should allow for longer sessions, or conduct interviews one on one to ensure all participants are able to fully express their ideas. This would yield richer information from youth with lived experience. Additionally, in the discussion about barriers to healthcare, many participants discussed frustrations that reflected general issues with MH services in Ontario that have been exacerbated by the COVID-19 pandemic but were not specific to the LGBTQ2S+ community. Future research should include questions that are specifically tailored to the experience of LGBTQ2S+ youth to avoid responses that reflect general issues with MH services.
5. Conclusions
This study sought to determine the barriers and biases that LGBTQ2S+ youth experience when seeking mental health services in Ontario and Quebec, to generate solutions, and to develop methods to increase provider accountability. Several issues were brought to light, including limited LGBTQ2S+ specific services, inadequate provider training, and general provider bias. The findings from the Accountability Prototype activities generated helpful solutions to such problems, including increased provider training, hiring LGBTQ2S+ providers, and implementing ‘undercover boss’ style assessments to establish provider accountability. This information is significant in creating new policies and programs, and in informing new research with which to build a culturally safe environment for LGBTQ2S+ youth seeking mental health services.
Author Contributions
Conceptualization, M.C. and P.F.; methodology, M.C. and P.F.; formal analysis, M.S., R.T. and M.C.; investigation, M.C., P.F. and R.T.; resources, M.C.; writing—original draft preparation, M.S. and R.T.; writing—review and editing, R.T. and M.C.; supervision, M.C.; funding acquisition, M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Canadian Institute for Health Research, grant number 173073.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Board of the Centre for Addiction and Mental Health (REB # 039/2021, 13 May 2021).” for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are not publicly because participants have not provided permission for their data to be shared.
Acknowledgments
We would like to acknowledge all the facilitators, designers, and project managers who helped run our Design Charrette sessions.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A. Structured Activities and Results in Sessions 2 and 3
Appendix A.1. Brainstorming
Participants identified the short- and long-term goals of their proposed solution. Short term goals, from highest to lowest priority, included connecting LGBTQ2S+ businesses with MH providers, creating a normality for discussing sexuality and gender needs with patients, creating a safe place for disclosure, normalizing non-heteronormative discussion between patients and providers, generating more trans-specific spaces that adhere to the World Professional Association for Transgender Health (WPATH), and preventing the gatekeeping of complex MH patients.
Long-term goals, from highest to lowest priority, included conducting community-based research involving the LGBTQ2S+ community, hiring MH providers that are members of the LGBTQ2S+ community, creating a directory to specialized services for trans and non-binary individuals, and preventing the unnecessary isolation of LGBTQ2S+ patients.
General goals included increasing options for LGBTQ2S+ individuals with disabilities, discontinuing cis and heteronormative methods of training at every level, expanding MH provider training to include more LGBTQ2S+ identities, and intensifying the screening process to reduce LGBTQ2S+ prejudice among providers.
The notes gathered from the brainstorming process were then used to define the principal ideas and develop a prototype.
Appendix A.2. Idea Definition and Prototyping
In idea definition, participants stated their idea was to generate an open, ongoing, and accessible LGBTQ2S+ healthcare system, made up of educated and non-judgmental MH workers. Key features include affordability, MH providers with lived experience, LGBTQ2S+ education for MH providers, safety, trust, and an equal distribution of power. The intended outcomes of the idea include reduced bias towards LGBTQ2S+ youth seeking MH services, increased effectiveness of care, increased accessibility and diversity of services, patient safety, and lastly, for patients to feel a sense of belonging and understanding.
In the prototype playground, study participants suggested potential mechanisms that would enable their idea (identified in the idea defining session) to become a reality. This addressed solutions to problems, as well as mechanisms to assure MH providers are held accountable for upholding the solutions.
Potential solutions included creating an LGBTQ2S+ specific healthcare center, changing the educational curriculum of MH providers such that it becomes more inclusive of the LGBTQ2S+ community, introducing a Queer and Trans patient union to advocate for LGBTQ2S+ needs, and including a comprehensive list of LGBTQ2S+ identities on all patient intake forms.
Potential methods to ensure accountability included introducing ‘undercover boss’ style assessments for MH providers and introducing a Queer and Trans patient union to monitor MH providers and services and ensure that LGBTQ2S+ youth are being treated effectively.
Such ideas were subsequently used to generate a concept blueprint and storyboard.
Appendix A.3. Concept Blueprint and Storyboard
The concept blueprint addressed the functionality of the prototype in three sections, namely, Pre-engagement, Engagement, and Post-engagement, in order to simulate how a patient would experience the new proposed model of MH services.
Appendix A.3.1. Pre-Engagement
This section discusses the experiences of a patient prior to accessing the proposed prototype. Participants attested that patients are being met with unhelpful MH providers, heteronormative treatment, and are getting passed from one service to the next. This results in patients who are unable to access care, or who are receiving biased or ineffective treatment. Patients are left feeling discouraged, anxious, and as though they are not deserving of care.
Appendix A.3.2. Engagement
This section discusses the experiences of a patient during their interactions with the proposed prototype. In this model, MH services have employed more individuals with lived experiences, who have been trained using LGBTQ2S+ inclusive curricula, and are consistently tested via undercover patients to ensure provider effectiveness and accountability. LGBTQ2S+ healthcare centers have also been implemented, increasing accessibility and diversity of services for patients. This model includes an MH provider that follows a patient through their journey to ensure a continuity of care, as well as a sense of safety. In such a model, participants suggest that patients feel seen, empowered, and receive appropriate and effective care.
Appendix A.3.3. Post-Engagement
This section describes the experience of a patient after receiving care via the proposed prototype. Following a(n) interaction(s) with a MH service/provider, participants explain that patients will be able to continue to work with their current provider, find appropriate services, and receive effective care. Providers will also conduct regular follow-ups to establish long-term support. The use of the prototype will allow patients to feel seen, understood, and comfortable. In addition, this will rebuild confidence in MH services and providers, allowing patients to feel confident to reach out again, should they require care in the future.
Study participants subsequently produced storyboard images to illustrate various scenarios of their prototype, as seen in Figure 2.
References
- Almeida, J.; Johnson, R.M.; Corliss, H.L.; Molnar, B.E.; Azrael, D. Emotional Distress Among LGBT Youth: The Influence of Perceived Discrimination Based on Sexual Orientation. J. Youth Adolesc. 2009, 38, 1001–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, A. Scrambling for access: Availability, accessibility, acceptability and quality of healthcare for lesbian, gay, bisexual and transgender people in South Africa. BMC Int. Health Hum. Rights 2017, 17, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillier, L.; Jones, T.; Monagle, M.; Overton, N.; Gahan, L.; Blackman, J.; Mitchell, A. Writing Themselves in 3: The Third National Study on the Sexual Health and Wellbeing of Same Sex Attracted and Gender Questioning Young People. 2010. Available online: https://apo.org.au/sites/default/files/resource-files/2010-11/apo-nid53195.pdf. (accessed on 21 December 2022).
- Smith, E.; Jones, T.; Ward, R.; Dixon, J.; Mitchell, A.; Hillier, L. From Blues to Rainbows: The Mental Health and Well-Being of Gender Diverse and Transgender Young People in Australia. 2014. Available online: https://www.latrobe.edu.au/__data/assets/pdf_file/0007/598804/from-blues-to-rainbows-report-sep2014.pdf (accessed on 21 December 2022).
- Kosciw, J.; Clark, C.; Truong, N.; Zongrone, A. GSLEN National School Climate Survey. 2019. Available online: https://files.eric.ed.gov/fulltext/ED608534.pdf (accessed on 21 December 2022).
- Jadva, V.; Guasp, A.; Bradlow, J.; Bower-Brown, S.; Foley, S. Predictors of Self-Harm and Suicide in LGBT Youth: The Role of Gender, Socio-Economic Status, Bullying and School Experience. J. Public Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Adelson, S.; Miller, A.M.; Johnson, K.; Reid, G. What psychiatry can do to end LGBT conversion therapy. Lancet Psychiatry 2022, 9, e40. [Google Scholar] [CrossRef] [PubMed]
- Wallach, S.; Garner, A.; Howell, S.; Adamson, T.; Baral, S.; Beyrer, C. Address Exacerbated Health Disparities and Risks to LGBTQ+ Individuals during COVID-19. Health Hum. Rights 2020, 22, 313. [Google Scholar] [PubMed]
- Curtis, M.; Ryder, D. LGBT Teens, Social Media Use & Depressive Symptoms. Think. Matters Symp. Arch. 2019. Available online: https://digitalcommons.usm.maine.edu/thinking_matters/210 (accessed on 20 December 2022).
- Salerno, J.P.; Devadas, J.; Pease, M.; Nketia, B.; Fish, J.N. Sexual and Gender Minority Stress Amid the COVID-19 Pandemic: Implications for LGBTQ Young Persons’ Mental Health and Well-Being. Public Health Rep. 2020, 135, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Jones, T. Improving Services for Transgender and Gender Variant Youth: Research, Policy and Practice for Health and Social Care Professionals; Jessica Kingsley Publishers: Philadelphia, PA, USA, 2019. [Google Scholar]
- Jones, T. Policy and Gay, Lesbian, Bisexual, Transgender and Intersex Students; Springer International Publishing: Cham, Switzerland, 2015. [Google Scholar] [CrossRef]
- Toomey, R.B.; Ryan, C.; Diaz, R.M.; Russell, S.T. High School Gay–Straight Alliances (GSAs) and Young Adult Well-Being: An Examination of GSA Presence, Participation, and Perceived Effectiveness. Appl. Dev. Sci. 2011, 15, 175–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magritte, E.; Williams, J.; Amyot, E.; Usipuik, M.; Sanders, C. Listening to Individuals with Differences in Sex Development or Intersex and Their Families: “Not Doing Surgery Does Not Mean Doing Nothing. Horm. Res. Paediatr. 2022, 94, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jadwin-Cakmak, L.; Bauermeister, J.A.; Cutler, J.M.; Loveluck, J.; Sirdenis, T.K.; Fessler, K.B.; Popoff, E.E.; Benton, A.; Pomerantz, N.F.; Atkins, S.L.; et al. The Health Access Initiative: A Training and Technical Assistance Program to Improve Health Care for Sexual and Gender Minority Youth. J. Adolesc. Health 2020, 67, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Rees, S.N.; Crowe, M.; Harris, S. The lesbian, gay, bisexual and transgender communities’ mental health care needs and experiences of mental health services: An integrative review of qualitative studies. J. Psychiatr. Ment. Health Nurs. 2021, 28, 578–589. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
Figure 1.
Journey mapping describes and highlights the experience of LGBTQ2S+ youth in the current MH climate. The figure, generated by a graphic illustrator, depicts the collective experiences of LGBTQ2S+ youth participants who have accessed or tried to access mental healthcare.
Figure 1.
Journey mapping describes and highlights the experience of LGBTQ2S+ youth in the current MH climate. The figure, generated by a graphic illustrator, depicts the collective experiences of LGBTQ2S+ youth participants who have accessed or tried to access mental healthcare.

Figure 2.
Visual Summary of Themes: Provider Competencies and Gaps. Themes addressing provider competencies included anti-oppressive spaces, LGBTQ2S+ specific programs, and increased usability due to virtual appointments/telemedicine. Themes addressing provider gaps were identified as lack of LGBTQ2S+ specific services, insufficient and/or inadequate provider training, and general provider bias.
Figure 2.
Visual Summary of Themes: Provider Competencies and Gaps. Themes addressing provider competencies included anti-oppressive spaces, LGBTQ2S+ specific programs, and increased usability due to virtual appointments/telemedicine. Themes addressing provider gaps were identified as lack of LGBTQ2S+ specific services, insufficient and/or inadequate provider training, and general provider bias.

Figure 3.
Visual Summary of Themes: Solutions to Provider Gaps and Mechanisms for Change. Results highlight participant ideas for solutions to identified provider gaps, as well as mechanisms for change. Youth represented their ideas visually and in writing using Miro, and the Miro board was then analyzed by the research team for themes.
Figure 3.
Visual Summary of Themes: Solutions to Provider Gaps and Mechanisms for Change. Results highlight participant ideas for solutions to identified provider gaps, as well as mechanisms for change. Youth represented their ideas visually and in writing using Miro, and the Miro board was then analyzed by the research team for themes.

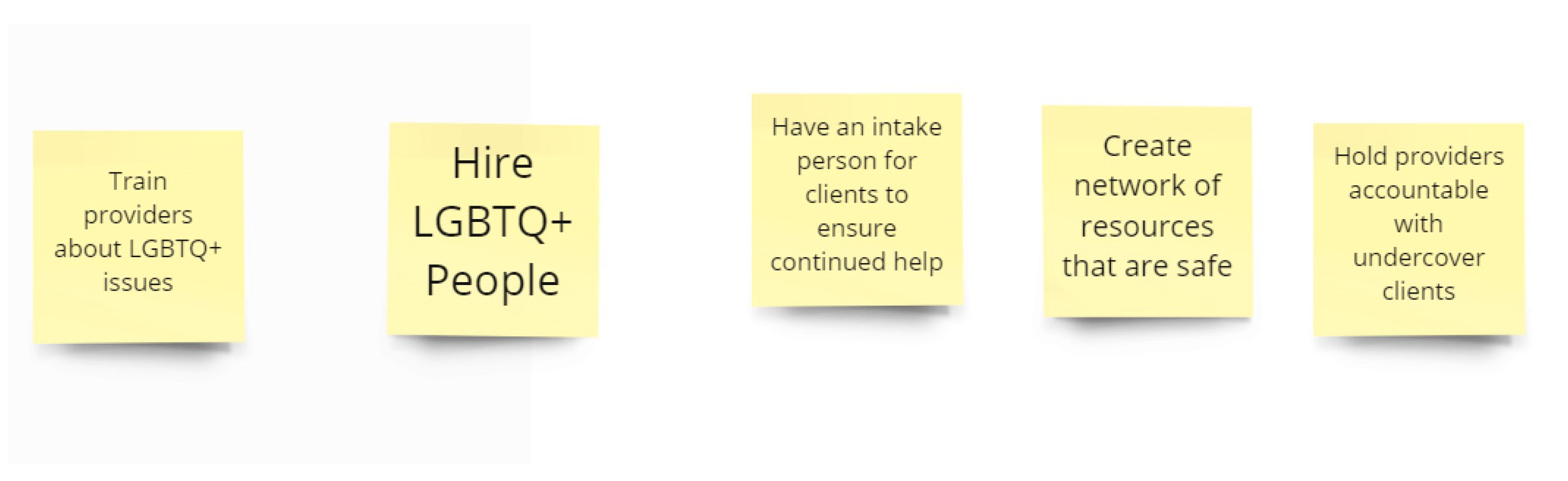
Figure 4.
Youth-identified solutions to making healthcare safer and more accessible for LGBTQ2S+ youth. Visual representation of youth ideas on Miro during Idea Definition and Prototyping activity. Participants asked: How might we make healthcare safer and more accessible for LGBTQ2S+ youth? Final solutions are represented through these sticky notes.
Figure 4.
Youth-identified solutions to making healthcare safer and more accessible for LGBTQ2S+ youth. Visual representation of youth ideas on Miro during Idea Definition and Prototyping activity. Participants asked: How might we make healthcare safer and more accessible for LGBTQ2S+ youth? Final solutions are represented through these sticky notes.

Figure 5.
Proposed solutions and measures to ensure accountability to improve MH services and providers. This figure, created by participants, aims to demonstrate some of the changes to the current MH system proposed by the study participants. The first panel portrays the suggested increase in LGBTQ2S+ education for MH providers, the second panel illustrates an ‘undercover boss’ model of assuring provider accountability, and the third panel demonstrates positive outcomes for LGBTQ2S+ youth. Figure was generated in Miro, a cloud-based, online white-board used for the collaboration of small to mid-sized groups.
Figure 5.
Proposed solutions and measures to ensure accountability to improve MH services and providers. This figure, created by participants, aims to demonstrate some of the changes to the current MH system proposed by the study participants. The first panel portrays the suggested increase in LGBTQ2S+ education for MH providers, the second panel illustrates an ‘undercover boss’ model of assuring provider accountability, and the third panel demonstrates positive outcomes for LGBTQ2S+ youth. Figure was generated in Miro, a cloud-based, online white-board used for the collaboration of small to mid-sized groups.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Participant Demographics.
| Demographics | Percentage of Sample |
|---|---|
| Gender Identity | |
| Agender | 6% |
| Genderfluid | 9% |
| Genderqueer | 12% |
| Man | 6% |
| Non-binary | 24% |
| Trans man | 9% |
| Trans woman | 3% |
| Two-Spirit | 3% |
| Woman | 27% |
| Sexual Identity | |
| Asexual | 3% |
| Bisexual | 18% |
| Gay | 9% |
| Lesbian | 12% |
| Pansexual | 12% |
| Queer | 30% |
| Questioning | 3% |
| Straight/Heterosexual | 6% |
| Two-Spirit | 6% |
| Lived in Canada | |
| From birth | 82% |
| More than 10 years | 6% |
| 1–10 years | 12% |
| Highest level of education | |
| Some high school | 24% |
| High school diploma | 39% |
| More than high school | 33% |
| Employment Status | |
| Employee | 21% |
| Self-emp. | 6% |
| Working unpaid | 3% |
| Student | 36% |
| Long-term sick/disabled | 9% |
| Unemployed | 12% |
| Covid unemployed | 12% |
| Person Living with a Disability | |
| Yes | 55% |
| No | 45% |
| Race | |
| African Canadian/American | 3% |
| Black | 12% |
| Caribbean | 12% |
| East Asian | 3% |
| First Nations | 9% |
| Latin American | 3% |
| Métis | 6% |
| Middle Eastern | 6% |
| Multiracial/Mixed | 9% |
| South Asian | 12% |
| White | 24% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chaiton, M.; Thorburn, R.; Sutton, M.; Feng, P. LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability. Youth 2023, 3, 93-106. https://doi.org/10.3390/youth3010006
AMA Style
Chaiton M, Thorburn R, Sutton M, Feng P. LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability. Youth. 2023; 3(1):93-106. https://doi.org/10.3390/youth3010006
Chicago/Turabian StyleChaiton, Michael, Rachel Thorburn, Megan Sutton, and Patrick Feng. 2023. "LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability" Youth 3, no. 1: 93-106. https://doi.org/10.3390/youth3010006