1. Introduction
Electronic cigarettes (e-cigs) increased in popularity and usage between 2013 and 2019 amongst youth in Canada, something which is also consistent with data from the United States [
1]. In the Canadian setting, Irvine et al. [
2] used cross-sectional data from the COMPASS study and found that male adolescents had a greater prevalence of e-cig use (40%) compared with female adolescents (31.3%). Chen et al. [
3] found that the mean age for e-cig initiation in the United States was 17.5 years of age. Considering the global context, Sreeramareddy et al. [
4] studied the prevalence of youth e-cig use from 75 countries using data from the Global Youth Tobacco Surveys. Ever use of e-cigs varied greatly in 54 countries, ranging from 2.3% in Cambodia all the way to 55.1% in Italy [
4]. Further, when considering current use of e-cigs in 54 countries, it ranged from 1.2% in Togo up to 35.1% in Guam [
4]. Interestingly, in seven of the 54 countries, approximately a third to half of the youth had reported everyday use of e-cigs [
4], which represents a significant proportion of the youth population.
One of the possible reasons these products have gained so much popularity among young people, is due to the clever ways in which they are marketed [
5]. These products are often made available in a variety of flavours, such as mint or chocolate, and these flavours may potentially mask the harms these products can cause. Unfortunately, some may even go as far as promoting e-cig use as being beneficial for one’s health [
6]. Therefore, given the attractive ways e-cigs are marketed and the misinformation perpetuated about e-cigs, it is clear that young people may not be able to fully understand the significant and lasting harm that e-cig use can cause to their developing bodies and minds.
Furthermore, it appears that e-cig usage may disproportionately impact youth from low socioeconomic backgrounds. Specifically, Cambron and Thackeray [
7] found that youth residing in communities with high levels of poverty were at a significantly higher risk of e-cig use. On the other hand, living in a household with high levels of education appears to be a protective factor against e-cig use [
7]. It is very likely that our society’s most vulnerable youth are at the highest risk for e-cig use.
It is clear that e-cigs can have an impact on multiple biopsychosocial domains for youth. In terms of the biological domain, e-cig use can lead to physiological changes, which may increase the risk of experiencing adverse cardiovascular events [
8]. Additionally, e-cig users may show evidence of the presence of carcinogens with a known association with bladder cancer in their urine [
9], as well as increased levels of pulmonary disease biomarkers [
8]. In the acute setting and considering the timing of the COVID-19 pandemic, it can be quite challenging to distinguish between active COVID-19 infection and symptoms associated with the use of e-cigs or vaping products that are themselves associated with lung injury [
10]. In terms of the psychosocial domain, Javed et al.’s [
11] scoping review found that e-cig use was associated with depression, suicidal intention, and suicidal attempts.
In addition, the use of e-cigs is often considered as a gateway to combustible cigarette use [
12]. Martinelli et al. [
13] assessed whether e-cigs had such a gateway effect that might lead to subsequent combustible cigarette use for youth. It was found that non-smoking youth who used e-cigs were at a higher risk of subsequent combustible cigarette initiation [
13]. Interestingly, Martinelli et al.’s [
13] findings point to a likely bidirectional relationship associating e-cig use with combustible cigarette use and vice versa.
Considering strategies that have been previously implemented, evidence from the global literature demonstrates that policies that restrict the use of e-cigs are effective in reducing the prevalence of current use of e-cigs among youth [
4]. Specifically, youth in countries with the most stringent e-cig regulations have a lower odds ratio of 0.6 of being current e-cig users compared with countries with no regulatory policies [
4]. This highlights the power that public policy has over youth e-cig use. Considering a global context in regulation policy approaches to e-cigarette use, Kennedy et al. [
14] assessed the diverse range in methods used by 68 countries, of which 25 have banned the sale of e-cigarettes. In the countries that do permit the sale of e-cigarettes the most common regulatory approaches include minimum age-of-purchase policies and the banning of their use in indoor public places, while 35 countries restricted or banned the promotion or advertising of e-cigs. Other observed polices enacted involve taxation, requirement of health warning labels, regulation of ingredients and flavouring and the regulation of manufacturing standards of e-cigs marketed as medicine [
14]. In terms of other programs, Graham et al. [
15] assessed the effectiveness of an e-cig text message-based cessation program among youth through a randomized control trial. A statistically significant 24.1% post-randomization abstinence rate at seven months post randomization was found [
15]. This highlights the impact that interactive text messages can have on supporting youth e-cig users achieve cessation. Some of the limitations of current efforts to curb youth e-cig use include the need to deal with a great deal of misinformation on e-cigs on social media platforms that are accessed by youth [
16] and combating the attractiveness of flavoured e-cigs [
17]. Another challenge in supporting e-cig cessation for youth is that there is a lack of international guidelines to manage e-cig cessation [
18]. This further re-iterates the importance for continued research on e-cigs and how to support young people who use e-cigs to achieve cessation.
Ultimately, given the rise in e-cig use among youth, the inequitable impact that e-cig use has on youth from lower socioeconomic backgrounds, the complex biopsychosocial challenges associated with e-cig use and the gateway effect associated with e-cig use, it is necessary to develop additional strategies to communicate the risks of e-cig use with youth. It is important to acknowledge that we, as a society, have achieved significant milestones in reducing combustible tobacco use in the 21st century. For example, since 2007, the global population that has benefited from at least a single cost-effective tobacco control policy has quadrupled in number [
19]. Moreover, 65% of the global population currently benefits from at least one of the World Health Organization’s (WHO) six WHO MPOWER strategies, which are considered highly essential and effective tobacco control strategies [
19]. Unfortunately, despite all of the progress that has been made, the increase in youth e-cig use threatens to reverse the substantial progress made through anti-tobacco initiatives [
20]. This paper provides an overview of a five factor model to communicate the risks of e-cig use with youth. This five-factor model was built considering some of the strengths and limitations of current approaches to address youth e-cig use.
2. The Five Factor Model
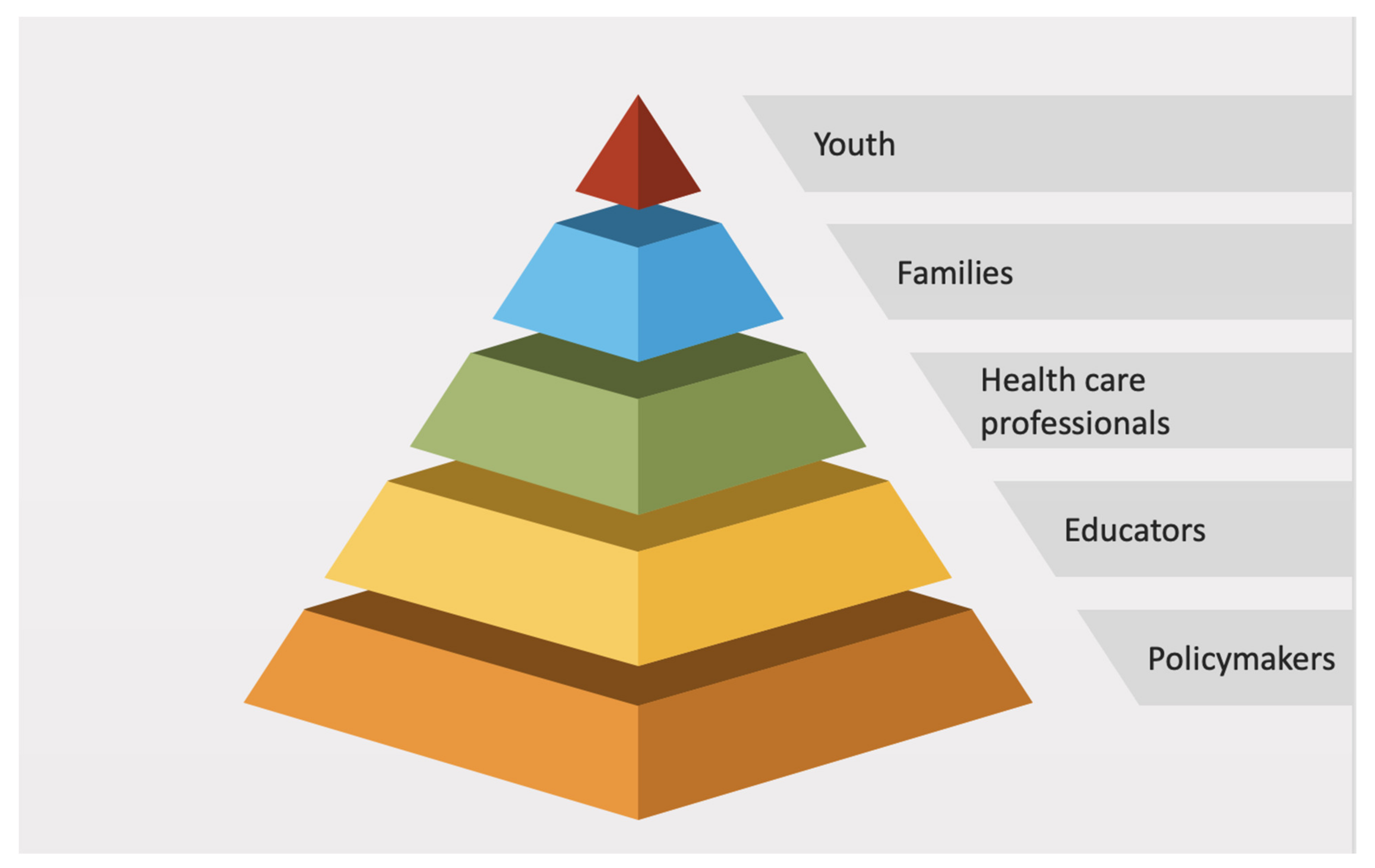
We propose a five factor model that aims to provide support to stakeholders involved in promoting information on e-cig use and its biopsychosocial impacts, including policymakers, educators, health care professionals, families and youth.
Figure 1 showcases this model.
We have organized the five factor model into the shape of a pyramid representing the reciprocal impact each stakeholder has on one another, and the support required from one for another to function. We have placed policy makers at the bottom of the pyramid because appropriate and evidence-based policies provide the foundation upon which school staff and health care professionals, for example, can base youth-oriented advice and information. Families then can take a step further and personalize this information for their unique socioeconomic and cultural context. Lastly, youth are at the top of the pyramid because not only will the stakeholders under them provide them with the necessary and appropriate information related to e-cig use and its related harms, but their personal views and values also influence their decisions and outcomes on e-cig use.
2.1. Policymakers
In terms of policymakers, it is necessary to develop and implement robust policies that limit the access youth have to e-cigs. Ruokolainen et al. [
21] found that flavoured e-cigs were discerned as a reason for e-cig use. Given that flavoured e-cigs are quite attractive to young people, bans on the sale of flavoured e-cigs can be a meaningful goal for policymakers to enact. The Canadian province of Nova Scotia has implemented a regional ban on the sale of flavoured e-cigs [
22,
23]. Notably, this policy is based on evidence surrounding context-specific data on youth e-cig use and related data were drawn upon to create and implement it [
22]. It is important to acknowledge that, at this point in time, there does not exist any data that have studied the impacts of this policy and subsequent youth e-cig use patterns. Considering national-level policies in the global context, Finland implemented a ban of the sale of flavoured e-cigs in 2016 [
21]. Population-based evaluation of this policy change has shown that there has not been an increase in e-cig use following the flavour ban. However, an important challenge to note was that the ban was not 100% effective in limiting access to flavours as some people were still able to use flavoured e-cigs [
21]. Ruokolainen et al., [
21] suggest one of the ways people still access flavoured e-cigs is through online shopping. Hence, public policies should be cognizant to restrict the sale and importation of flavoured e-cigs within their borders. National-level policies may have inherent benefits over regional-level policies because jurisdictional areas are significantly more well-defined when they encompass an entire country, compared with smaller areas that are governed by regional policies. Given the challenges of enforcing flavour bans or related policies that seek to reduce the access that youth have to e-cigs [
21], having a single nationwide policy has the potential to reduce the enforcement confusion that can be associated with a patchwork of different regional policies. It must be acknowledged that creating national policies can be challenging, as setting up and coordinating a national enforcement structure may require a great deal of effort, taking longer to implement and gather feedback compared with policies that are implemented at a regional level.
Policies surrounding the advertisement of e-cigs can be implemented to prevent the industry from specifically targeting youth in its marketing materials. For example, the American Centers for Disease Control and Prevention (CDC) [
24] state that approximately 70% of students aged 11 to 17 years old have been exposed to e-cig promotional products through retail stores, social media, written media, and digital media [
24]. The e-cig industry invests a great deal of financial resources in marketing their products [
24,
25]. Ozga et al. [
25] assessed the marketing expenditures of the e-cig industry in the United States from 2016 to 2021, finding that expenditures on e-cig marketing peaked in 2018 and 2019, and then began to dramatically decline from early 2020 until July 2021 [
25]. The sharp decline in marketing expenditure in the early portion of 2020 was related to the implementation of the Tobacco 21 federal policy, which increased the legal age to purchase tobacco products (including e-cigs), and the e-cig industry was notified of the Food and Drug Administration’s (FDA) intention to prioritize discretionary enforcement of authority over flavoured e-cig products that were not tobacco or menthol flavoured [
25]. E-cig advertisements have a cross association with an increase in traditional cigarette consumption as well, thus there is more incentive to heavily regulate marketing materials [
26]. Moreover, the CDC [
24] suggests that successful policies can limit advertisement avenues and content and thereby decrease youth enticement. Taxation is a negative incentive to reduce affordability and hence the accessibility of e-cigarettes to deter consumption. Abouk et al. [
27] found that, in states in the US that have enacted the electronic nicotine delivery system (ENDS) tax, generally higher taxation was found to be effective in the reduction of use and initiation amongst youth. However, caution must be employed when using taxation practices, as substitution to cigarette and tobacco-based products increased [
27].
2.2. Educators
Given that the vast majority of young people spend a significant amount of time in educational settings, it is necessary to incorporate education on e-cigs into the health curriculum of the classroom setting, especially during elementary and high school. These educational stages better capture students from lower socioeconomic households as compared with universities and colleges. Unfortunately, Pettigrew et al.’s [
28] study assessing the perception of Australian school staff on students’ use of e-cigs found that only 31% of school staff reported that their school had conducted e-cig prevention education in their schools. This highlights how the education system may not be providing enough information on e-cigs to youth students. Research indicates that the likelihood of initiating e-cigs increases until 18 years of age, though it is important to note that some people may initiate e-cig use as early as age seven [
3]. Chaplin et al. [
29] evaluated the effectiveness of an educational intervention explaining the risks associated with e-cig use to adolescents in high-school. They used a pre-intervention and post-intervention survey to evaluate adolescents’ change in knowledge on e-cigs. From Chaplin et al.’s [
29] study, school-based educational interventions have the potential to increase youth knowledge on the social and health risks associated with e-cig use. This is especially true if the information provided is evidence based, age-specific, and relevant [
29]. For example, research has shown that the most prevalent reason for youth to stop the use of e-cigs was the detrimental effect they had on their own or their family’s health [
29]. Incorporating this type of information in the curriculum is important to ensure youth are engaged in the conversation. In terms of age-specific education, information for elementary and middle-school youth may include pictures, stories, or roleplay while information for high school youth may include group discussions, watching movies/documentaries, or reading true stories that reflect the detrimental biopsychosocial effects of e-cig use. Relevant education means conducting needs assessments on the perception of youth on e-cig use and on their reason for use to ensure the education curriculum targets their current thoughts and ideas rather than what an adult may perceive as important. Ultimately, school-based interventions should be provided to youth in an accessible way, appropriate for their age level, and that ensures that the detrimental health risks associated with e-cig use are clearly discussed. Additionally, the implementation of school policies, such as those that do not allow e-cig use at school, in conjunction with training school staff appear to be associated with increased staff recognition of certain e-cig products [
30]. In school that had put in place e-cig policies and staff training, staff were more likely to intervene and communicate with students about stopping the use of e-cigs, in addition to reporting students who were found to have used e-cigs while at school [
30]. It is necessary that schools establish policies restricting access and use of e-cigs, so that a clear message is sent to students without any ambiguity on the part of the school staff nor the students.
Challenges associated with these strategies include creating curricular time for discussion on e-cigs in the classroom, using evidence-based research surrounding the best and most well-received communication strategies for sharing this information, and implementing teacher education or training to appropriately and correctly answer any questions that may arise during discussions.
It is important to ensure that school staff receive training on e-cigs and how to formulate conversations about e-cig use with their students. Training for teachers can be provided through continuing education seminars, such as those on professional development days.
2.3. Health Care Professionals
In terms of health care professionals that are working directly with youth, recent research has highlighted that health care professionals may have inadequate knowledge about e-cigs and may not feel comfortable discussing e-cig use with their patients [
31]. It has been reported that many health care professionals access information about e-cigs from social media and news platforms, as opposed to evidence-based platforms, such as academic journals [
31]. It is critical that health care professionals feel comfortable when discussing e-cig use with youth, especially considering that youth are exposed to a great deal of marketing [
24] and because there is a large amount of misinformation related to e-cigs that youth might be exposed to on social media [
16]. Thus, it is possible that youth patients who come to see health care professionals may have preconceived ideas on the impact that e-cigs have on their health and wellbeing. Health care professionals need sufficient knowledge on e-cigs to both address misinformation and provide evidence-based information to youth in a youth-centred way. It is necessary that health care professionals provide a clear message that there is no benefit for youth to initiate e-cig use and risk becoming dependent on nicotine. Moving forward, medical associations and guideline creating bodies should aim to provide evidence-based information on the impacts of e-cigs on youth health that is comprehensive and easily accessible. This information should be supplemented with youth-oriented communication strategies that would allow health care professionals to discuss and share the information with their patients and their families at appointments or other relevant interactions. One suggestion to implement the above two recommendations would be for health care professionals to receive dedicated training about e-cigs at all levels of education, including during professional training programs, residency, and as a part of continuing medical education [
31]. At the training level, information on e-cigs can be shared effectively through small group case-based learning sessions or large group lectures. Meanwhile, in terms of continuing medical education, research on e-cigs can be shared by experts who are involved in the care of people who use e-cigs. Other methods of communication to health care professionals may include email newsletters or academic journal social media pages which would allow for digestible evidence-based information to be readily shared. Information can be provided through platforms that health care professionals regularly check, for example, daily news updates. One challenge associated with creating communication tools for health care professionals is the question of whether to delegate the task to one appropriate medical specialist or ensuring all members of a multi-disciplinary/multi-physician care team are sharing the same information. Another challenge is the limited time that family physicians, who would likely be conducting the bulk of this conversation, have to spend with their patients [
32]. Time between health care professionals and youth is needed in order to build up rapport and have these longer, sensitive and more complex conversations.
2.4. Families
Families play an important role in preventing youth from using e-cigs. Unfortunately, it seems that many families, specifically parents, are unaware of their children using e-cigs [
33]. A lack of awareness on the part of parents can make it quite challenging for them to support their children in regards to the use of e-cigs. Research on communication strategies between parents and adolescents on substance use, including alcohol, tobacco, and other drugs, has shown that open, credible, and two-sided communication will result in increased receptiveness by youth [
34]. Additionally, there is a need for toolkits to be made available for families to use when discussing e-cigs with their children. These toolkits should be made freely available on trusted, public health websites, such as the CDC website, so that parents can easily find them and come to know they can rely on them. Information contained within these toolkits can include signs and symptoms of e-cig use (respiratory symptoms, presence of e-cig supplies and new odours), strategies for communicating with youth on e-cigs (health and wellbeing, financial health, and addressing targeted advertising) and resources that families can access (including, but not limited to, family physicians, public health offices, quitting text lines or mobile apps) [
35]. Conversations regarding the use of tobacco between parents and children can be quite challenging [
34]. A key challenge that family members might face when discussing e-cigs with their young children is how to start the conversation. It is necessary that these tool kits also provide families with guidance on how to begin the sensitive and challenging discussion on e-cigs use. Once an available online toolkit has been created, it should then be advertised to parents through radio or TV commercials, social media sites, websites, and/or through verbal discussion.
Although parental self-disclosure of e-cig use has not been investigated, Wu and Chafee [
33] have demonstrated that youth tobacco use was lower when all family members agreed that tobacco use was not allowed throughout the home. It is also important to note that research on substance use in general [
34], and e-cig use in particular, has consistently demonstrated that enforcing ground rules is more effective than simply advising and discussing abstinence [
33]. Families can use these communication strategies to alter the information put forward by policy-makers, educators, and health care professionals to ensure it is relevant to their personal environmental, and their socioeconomic and cultural situations.
2.5. Youth
Finally, when targeting youth directly, it is important to realize that, while evidence-based academic resources on the risks of e-cig use exist, these sources may not be fully accessible to youth due to a variety of reasons [
16]. Given the plethora of misinformation available online, it is necessary for trusted sources of information to disseminate evidence-based information to youth in an accessible and easily digestible manner [
16]. We should aim to directly reach youth and communicate the potential risks of e-cig use through the social media platforms that they frequent [
16]. Furthermore, this information should be easy to understand and follow to ensure those with lower education backgrounds are also benefiting. Organizations that can take on these roles may include the social media pages of local health authorities, medical societies, and academic journals. The perception of youths changing after learning the health impacts of e-cigs (i.e., increased perceptions of risk after e-cig or vaping associated lung injury was revealed) is evidence that youth can be receptive and influenced by evidence-based information on e-cig use, although the platform of this communication must be conducive [
36]. It is necessary to acknowledge that social media posts made by these organizations will be at risk of being outnumbered and will be competing against hundreds of thousands of other messages and posts about vaping. It is therefore necessary for other innovative approaches to be taken to engage youth in an effective manner, with one suggestion being to promote youth involvement in the scientific publication process through youth advisory committees [
37]. Specifically, academic journals can aim to bring aboard youth as peer reviewers on the youth advisory committee for relevant publications, for example for studies on topics that focus on youth health and wellbeing. Youth can then share their unique perspectives during the peer review process and become an active member of the team, rather than simply a “receiver” of information [
37]. Furthermore, following publication, journals can promote key messages from these evidence-based articles on social media and share the way in which these findings are relevant to youth and can be reviewed by youth in their youth advisory committees. It is necessary to acknowledge that creating these youth advisory committees does require proper infrastructure and resources [
37]. Ultimately, this approach allows us to directly connect with youth, with the hopes of influencing their views and values surrounding e-cig use and their detrimental health impacts.


 ,
, {kind=link}
