
Bempedoic Acid and Statins in Lipid-Lowering Strategy: Which Came First, the Egg or the Chicken?
 ,
,
Abstract
:1. Introduction
2. Bempedoic Acid: Biochemical and Pharmacological Features
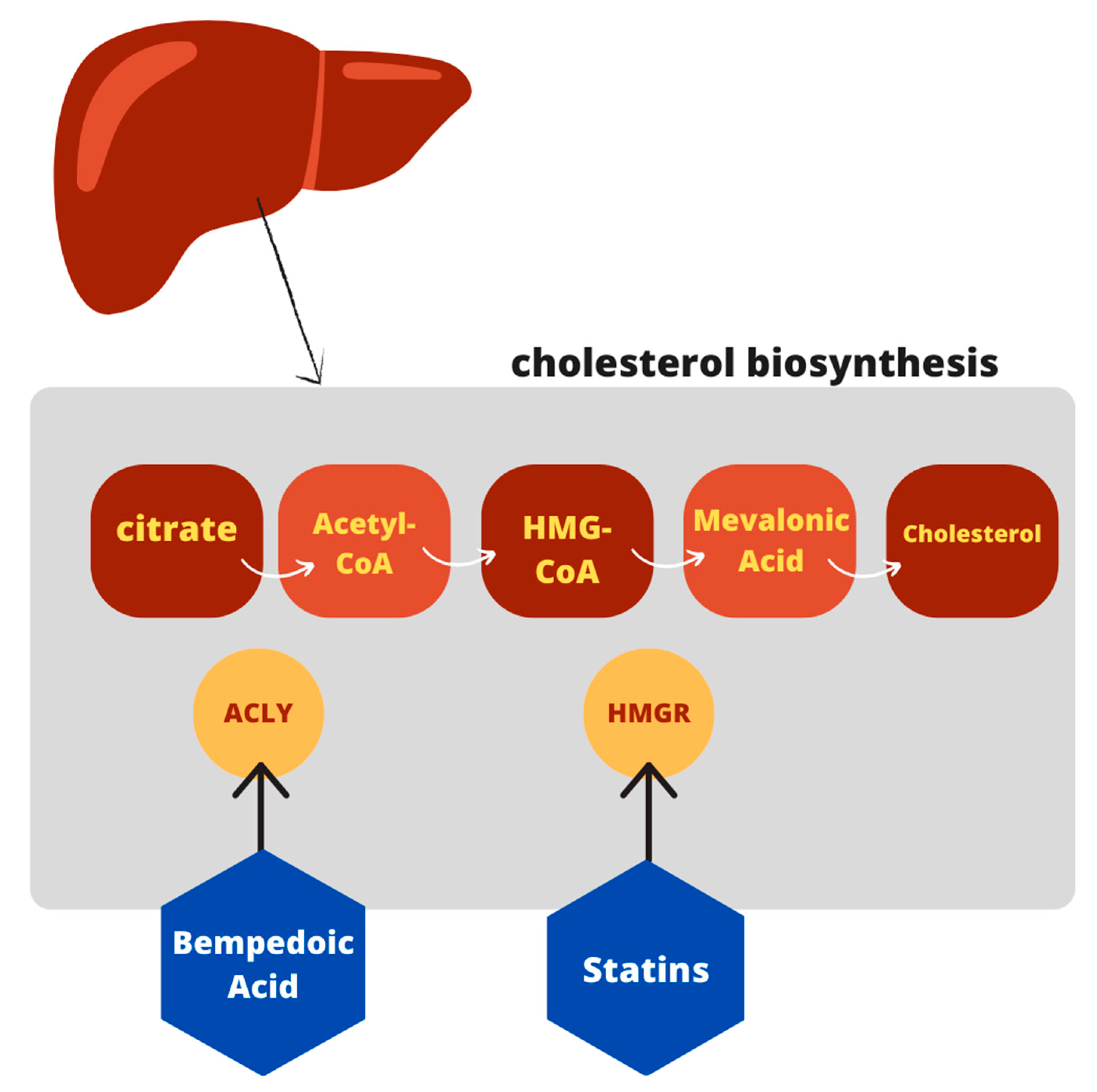
2.1. Cholesterol Biosynthesis: The Upstream Effect
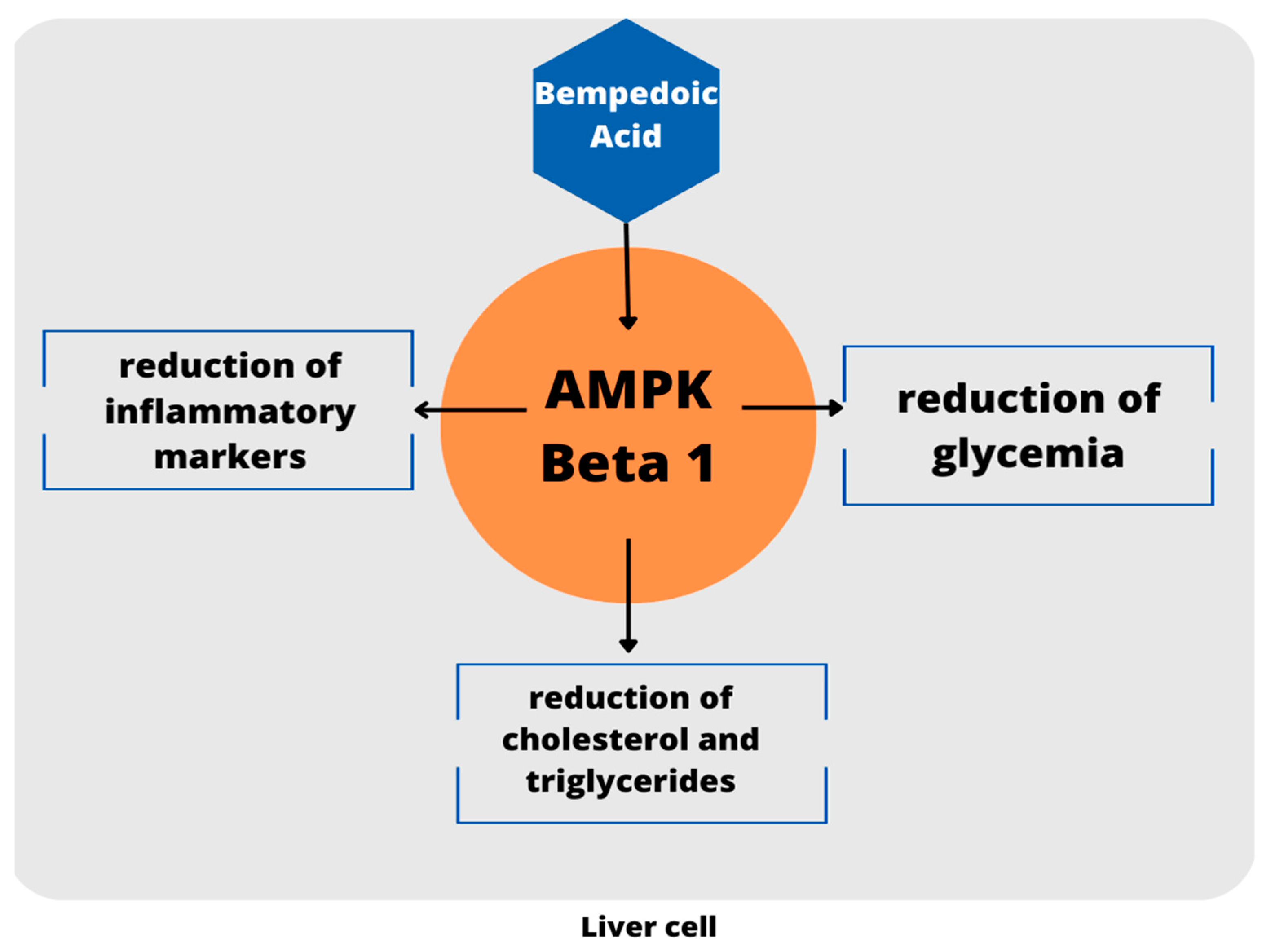
2.2. Alternative Biochemical Pathway beyond Cholesterol Synthesis
2.3. Pharmacological Properties
3. Preclinical Evidence: Optimal Dosage, Pleiotropic Effects and Promising Safety Profile
4. The CLEAR Program: Exploring the Role in Clinical Practice
4.1. Bempedoic Acid in Statin Intolerant Patients: The CLEAR Tranquility and CLEAR Serenity Trials
4.2. Patients on Maximal Lipid-Lowering Therapy: The CLEAR Harmony, CLEAR Wisdom, and FDC Trials
4.3. First Evidence on Cardiovascular Events: The CLEAR Outcomes Trial
5. Discussion
6. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silverman, M.G.; Ference, B.A.; Im, K.; Wiviott, S.D.; Giugliano, R.P.; Grundy, S.M.; Braunwald, E.; Sabatine, M.S. Association Between Lowering LDL-C and Cardiovascular Risk Reduction among Different Therapeutic Interventions: A Systematic Review and Meta-analysis. JAMA 2016, 316, 1289–1297. [Google Scholar] [CrossRef] [Green Version]
- Abdullah, S.M.; Defina, L.F.; Leonard, D.; Barlow, C.E.; Radford, N.B.; Willis, B.L.; Rohatgi, A.; McGuire, D.K.; de Lemos, J.A.; Grundy, S.M.; et al. Long-Term Association of Low-Density Lipoprotein Cholesterol with Cardiovascular Mortality in Individuals at Low 10-Year Risk of Atherosclerotic Cardiovascular Disease. Circulation 2018, 138, 2315–2325. [Google Scholar] [CrossRef]
- Cannon, C.P. Low-Density Lipoprotein Cholesterol: Lower Is Totally Better. J. Am. Coll. Cardiol. 2020, 75, 2119–2121. [Google Scholar] [CrossRef] [PubMed]
- Packard, C.; Chapman, M.J.; Sibartie, M.; Laufs, U.; Masana, L. Intensive low-density lipoprotein cholesterol lowering in cardiovascular disease prevention: Opportunities and challenges. Heart 2021, 107, 1369–1375. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [Green Version]
- Dyrbus, K.; Gasior, M.; Penson, P.E.; Banach, M. Extreme cardiovascular risk-do we need a new risk category? Eur. Heart J. 2022, 43, 1784–1786. [Google Scholar] [CrossRef]
- Collins, R.; Reith, C.; Emberson, J.; Armitage, J.; Baigent, C.; Blackwell, L.; Blumenthal, R.; Danesh, J.; Smith, G.D.; DeMets, D.; et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet 2016, 388, 2532–2561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwaki, Y.; Lee, W.; Sugiyama, Y. Comparative and quantitative assessment on statin efficacy and safety: Insights into inter-statin and inter-individual variability via dose- and exposure-response relationships. Expert Opin. Drug Metab. Toxicol. 2019, 15, 897–911. [Google Scholar] [CrossRef]
- Ward, N.C.; Watts, G.F.; Eckel, R.H. Statin Toxicity. Circ. Res. 2019, 124, 328–350. [Google Scholar] [CrossRef] [PubMed]
- Birtcher, K. When compliance is an issue-how to enhance statin adherence and address adverse effects. Curr. Atheroscler. Rep. 2015, 17, 471. [Google Scholar] [CrossRef]
- Abdul-Rahman, T.; Bukhari, S.M.A.; Herrera, E.C.; Awuah, W.A.; Lawrence, J.; de Andrade, H.; Patel, N.; Shah, R.; Shaikh, R.; Capriles, C.A.A.; et al. Lipid Lowering Therapy: An Era Beyond Statins. Curr. Probl. Cardiol. 2022, 47, 101342. [Google Scholar] [CrossRef] [PubMed]
- Ciccarelli, G.; D’Elia, S.; De Paulis, M.; Golino, P.; Cimmino, G. Lipid Target in Very High-Risk Cardiovascular Patients: Lesson from PCSK9 Monoclonal Antibodies. Diseases 2018, 6, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azari, S.; Rezapour, A.; Omidi, N.; Alipour, V.; Behzadifar, M.; Safari, H.; Tajdini, M.; Bragazzi, N.L. Cost-effectiveness analysis of PCSK9 inhibitors in cardiovascular diseases: A systematic review. Heart Fail. Rev. 2020, 25, 1077–1088. [Google Scholar] [CrossRef]
- Smith, W.; Cheng-Lai, A.; Nawarskas, J. Bempedoic Acid: A New Avenue for the Treatment of Dyslipidemia. Cardiol. Rev. 2021, 29, 274–280. [Google Scholar] [CrossRef]
- Masana Marin, L.; Plana Gil, N. Bempedoic acid. Mechanism of action and pharmacokinetic and pharmacodynamic properties. Clin. Investig. Arterioscler. 2021, 33, 53–57. [Google Scholar] [CrossRef]
- Di Minno, A.; Lupoli, R.; Calcaterra, I.; Poggio, P.; Forte, F.; Spadarella, G.; Ambrosino, P.; Iannuzzo, G.; Di Minno, M.N.D. Efficacy and Safety of Bempedoic Acid in Patients with Hypercholesterolemia: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2020, 9, e016262. [Google Scholar] [CrossRef]
- Ruscica, M.; Banach, M.; Sahebkar, A.; Corsini, A.; Sirtori, C.R. ETC-1002 (Bempedoic acid) for the management of hyperlipidemia: From preclinical studies to phase 3 trials. Expert Opin. Pharmacother. 2019, 20, 791–803. [Google Scholar] [CrossRef]
- Pinkosky, S.L.; Newton, R.S.; Day, E.A.; Ford, R.J.; Lhotak, S.; Austin, R.C.; Birch, C.M.; Smith, B.K.; Filippov, S.; Groot, P.H.E.; et al. Liver-specific ATP-citrate lyase inhibition by bempedoic acid decreases LDL-C and attenuates atherosclerosis. Nat. Commun. 2016, 7, 13457. [Google Scholar] [CrossRef] [Green Version]
- Watkins, P.A. Very-long-chain acyl-CoA synthetases. J. Biol. Chem. 2008, 283, 1773–1777. [Google Scholar] [CrossRef] [Green Version]
- Ruscica, M.; Sirtori, C.R.; Carugo, S.; Banach, M.; Corsini, A. Bempedoic Acid: For Whom and When. Curr. Atheroscler. Rep. 2022, 24, 791–801. [Google Scholar] [CrossRef]
- Feng, X.; Zhang, L.; Xu, S.; Shen, A.Z. ATP-citrate lyase (ACLY) in lipid metabolism and atherosclerosis: An updated review. Prog. Lipid Res. 2020, 77, 101006. [Google Scholar] [CrossRef]
- Oniciu, D.C.; Myers, J.L. Bempedoic Acid and the Fraudulent Fatty Acid Family: The Gold Rush to Cardiovascular Therapies in the New Millennium. Org. Process Res. Dev. 2021, 25, 365–372. [Google Scholar] [CrossRef]
- Velazquez, A.M.; Bentanachs, R.; Sala-Vila, A.; Lazaro, I.; Rodriguez-Morato, J.; Sanchez, R.M.; Laguna, J.C.; Roglans, N.; Alegret, M. KHK, PNPLA3 and PPAR as Novel Targets for the Anti-Steatotic Action of Bempedoic Acid. Biomedicines 2022, 10, 1517. [Google Scholar] [CrossRef]
- Paton, D.M. Bempedoic acid. ATP-citrate lyase inhibitor, AMPK activator, Treatment of hypercholesterolemia. Drugs Future 2017, 42, 201. [Google Scholar] [CrossRef]
- Ballantyne, C.M.; Davidson, M.H.; Macdougall, D.E.; Bays, H.E.; Dicarlo, L.A.; Rosenberg, N.L.; Margulies, J.; Newton, R.S. Efficacy and safety of a novel dual modulator of adenosine triphosphate-citrate lyase and adenosine monophosphate-activated protein kinase in patients with hypercholesterolemia: Results of a multicenter, randomized, double-blind, placebo-controlled, parallel-group trial. J. Am. Coll. Cardiol. 2013, 62, 1154–1162. [Google Scholar] [CrossRef] [Green Version]
- Pinkosky, S.L.; Filippov, S.; Srivastava, R.A.; Hanselman, J.C.; Bradshaw, C.D.; Hurley, T.R.; Cramer, C.T.; Spahr, M.A.; Brant, A.F.; Houghton, J.L.; et al. AMP-activated protein kinase and ATP-citrate lyase are two distinct molecular targets for ETC-1002, a novel small molecule regulator of lipid and carbohydrate metabolism. J. Lipid Res. 2013, 54, 134–151. [Google Scholar] [CrossRef] [Green Version]
- Mackenzie, P.I.; Miners, J.O.; McKinnon, R.A. Polymorphisms in UDP glucuronosyltransferase genes: Functional consequences and clinical relevance. Clin. Chem. Lab. Med. 2000, 38, 889–892. [Google Scholar] [CrossRef]
- Biolo, G.; Vinci, P.; Mangogna, A.; Landolfo, M.; Schincariol, P.; Fiotti, N.; Mearelli, F.; Di Girolamo, F.G. Mechanism of action and therapeutic use of bempedoic acid in atherosclerosis and metabolic syndrome. Front. Cardiovasc. Med. 2022, 9. [Google Scholar] [CrossRef]
- Jadhav, S.B.; Crass, R.L.; Chapel, S.; Kerschnitzki, M.; Sasiela, W.J.; Emery, M.G.; Amore, B.M.; Barrett, P.H.R.; Watts, G.F.; Catapano, A.L. Pharmacodynamic effect of bempedoic acid and statin combinations: Predictions from a dose-response model. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 578–586. [Google Scholar] [CrossRef]
- Lalwani, N.D.; Hanselman, J.C.; MacDougall, D.E.; Sterling, L.R.; Cramer, C.T. Complementary low-density lipoprotein-cholesterol lowering and pharmacokinetics of adding bempedoic acid (ETC-1002) to high-dose atorvastatin background therapy in hypercholesterolemic patients: A randomized placebo-controlled trial. J. Clin. Lipidol. 2019, 13, 568–579. [Google Scholar] [CrossRef]
- Sato, M.; Mamada, H.; Anzai, N.; Shirasaka, Y.; Nakanishi, T.; Tamai, I. Renal secretion of uric acid by organic anion transporter 2 (OAT2/SLC22A7) in human. Biol. Pharm. Bull. 2010, 33, 498–503. [Google Scholar] [CrossRef] [Green Version]
- Ray, K.K.; Bakris, G.L.; Banach, M.; Catapano, A.; Duell, P.B.; Mancini, G.B.J.; Bloedon, L.; Feng, A.; Gotto Jr, A.M. Effect of bempedoic acid on uric acid and gout in 3621 patients with hypercholesterolemia: Pooled analyses from phase 3 trials. Eur. Heart J. 2020, 41, ehaa946-3001. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Pontremoli, R.; Fogacci, F.; Viazzi, F.; Borghi, C. Effect of Bempedoic Acid on Serum Uric Acid and Related Outcomes: A Systematic Review and Meta-analysis of the available Phase 2 and Phase 3 Clinical Studies. Drug Saf. 2020, 43, 727–736. [Google Scholar] [CrossRef]
- Ballantyne, C.M.; Bays, H.; Catapano, A.L.; Goldberg, A.; Ray, K.K.; Saseen, J.J. Role of Bempedoic Acid in Clinical Practice. Cardiovasc. Drugs Ther. 2021, 35, 853–864. [Google Scholar] [CrossRef]
- Gutierrez, M.J.; Rosenberg, N.L.; Macdougall, D.E.; Hanselman, J.C.; Margulies, J.R.; Strange, P.; Milad, M.A.; McBride, S.J.; Newton, R.S. Efficacy and safety of ETC-1002, a novel investigational low-density lipoprotein-cholesterol-lowering therapy for the treatment of patients with hypercholesterolemia and type 2 diabetes mellitus. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Thompson, P.D.; Rubino, J.; Janik, M.J.; MacDougall, D.E.; McBride, S.J.; Margulies, J.R.; Newton, R.S. Use of ETC-1002 to treat hypercholesterolemia in patients with statin intolerance. J. Clin. Lipidol. 2015, 9, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Cheeley, M.K.; Saseen, J.J.; Agarwala, A.; Ravilla, S.; Ciffone, N.; Jacobson, T.A.; Dixon, D.L.; Maki, K.C. NLA scientific statement on statin intolerance: A new definition and key considerations for ASCVD risk reduction in the statin intolerant patient. J. Clin. Lipidol. 2022, 16, 361–375. [Google Scholar] [CrossRef]
- Thompson, P.D.; MacDougall, D.E.; Newton, R.S.; Margulies, J.R.; Hanselman, J.C.; Orloff, D.G.; McKenney, J.M.; Ballantyne, C.M. Treatment with ETC-1002 alone and in combination with ezetimibe lowers LDL cholesterol in hypercholesterolemic patients with or without statin intolerance. J. Clin. Lipidol. 2016, 10, 556–567. [Google Scholar] [CrossRef] [Green Version]
- Ballantyne, C.M.; McKenney, J.M.; MacDougall, D.E.; Margulies, J.R.; Robinson, P.L.; Hanselman, J.C.; Lalwani, N.D. Effect of ETC-1002 on Serum Low-Density Lipoprotein Cholesterol in Hypercholesterolemic Patients Receiving Statin Therapy. Am. J. Cardiol. 2016, 117, 1928–1933. [Google Scholar] [CrossRef] [Green Version]
- Rubino, J.; MacDougall, D.E.; Sterling, L.R.; Hanselman, J.C.; Nicholls, S.J. Combination of bempedoic acid, ezetimibe, and atorvastatin in patients with hypercholesterolemia: A randomized clinical trial. Atherosclerosis 2021, 320, 122–128. [Google Scholar] [CrossRef]
- Rubino, J.; MacDougall, D.E.; Sterling, L.R.; Kelly, S.E.; McKenney, J.M.; Lalwani, N.D. Lipid lowering with bempedoic acid added to a proprotein convertase subtilisin/kexin type 9 inhibitor therapy: A randomized, controlled trial. J. Clin. Lipidol. 2021, 15, 593–601. [Google Scholar] [CrossRef]
- Laufs, U.; Banach, M.; Mancini, G.B.J.; Gaudet, D.; Bloedon, L.T.; Sterling, L.R.; Kelly, S.; Stroes, E.S.G. Efficacy and Safety of Bempedoic Acid in Patients with Hypercholesterolemia and Statin Intolerance. J. Am. Heart Assoc. 2019, 8, e011662. [Google Scholar] [CrossRef] [Green Version]
- Ballantyne, C.M.; Banach, M.; Mancini, G.B.J.; Lepor, N.E.; Hanselman, J.C.; Zhao, X.; Leiter, L.A. Efficacy and safety of bempedoic acid added to ezetimibe in statin-intolerant patients with hypercholesterolemia: A randomized, placebo-controlled study. Atherosclerosis 2018, 277, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Bays, H.E.; Catapano, A.L.; Lalwani, N.D.; Bloedon, L.T.; Sterling, L.R.; Robinson, P.L.; Ballantyne, C.M.; Trial, C.H. Safety and Efficacy of Bempedoic Acid to Reduce LDL Cholesterol. N. Engl. J. Med. 2019, 380, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.C.; Leiter, L.A.; Stroes, E.S.G.; Baum, S.J.; Hanselman, J.C.; Bloedon, L.T.; Lalwani, N.D.; Patel, P.M.; Zhao, X.; Duell, P.B. Effect of Bempedoic Acid vs Placebo Added to Maximally Tolerated Statins on Low-Density Lipoprotein Cholesterol in Patients at High Risk for Cardiovascular Disease: The CLEAR Wisdom Randomized Clinical Trial. JAMA 2019, 322, 1780–1788. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, C.M.; Laufs, U.; Ray, K.K.; Leiter, L.A.; Bays, H.E.; Goldberg, A.C.; Stroes, E.S.; MacDougall, D.; Zhao, X.; Catapano, A.L. Bempedoic acid plus ezetimibe fixed-dose combination in patients with hypercholesterolemia and high CVD risk treated with maximally tolerated statin therapy. Eur. J. Prev. Cardiol. 2020, 27, 593–603. [Google Scholar] [CrossRef] [Green Version]
- Nissen, S.E.; Lincoff, A.M.; Brennan, D.; Ray, K.K.; Mason, D.; Kastelein, J.J.P.; Thompson, P.D.; Libby, P.; Cho, L.; Plutzky, J.; et al. Bempedoic Acid and Cardiovascular Outcomes in Statin-Intolerant Patients. N. Engl. J. Med. 2023. [Google Scholar] [CrossRef]
- Atar, D.; Jukema, J.W.; Molemans, B.; Taub, P.R.; Goto, S.; Mach, F.; CerezoOlmos, C.; Underberg, J.; Keech, A.; Tokgozoglu, L.; et al. New cardiovascular prevention guidelines: How to optimally manage dyslipidaemia and cardiovascular risk in 2021 in patients needing secondary prevention? Atherosclerosis 2021, 319, 51–61. [Google Scholar] [CrossRef]
- Dai, L.; Zuo, Y.; You, Q.; Zeng, H.; Cao, S. Efficacy and safety of bempedoic acid in patients with hypercholesterolemia: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Prev. Cardiol. 2021, 28, 825–833. [Google Scholar] [CrossRef]
- Yu, D.; Liao, J.K. Emerging views of statin pleiotropy and cholesterol lowering. Cardiovasc. Res. 2021, 118, 413–423. [Google Scholar] [CrossRef]
- Proute, M.C.; Kothur, N.; Georgiou, P.; Serhiyenia, T.; Shi, W.; Kerolos, M.E.; Pradeep, R.; Akram, A.; Khan, S. The Effect of Statin Therapy on Inflammatory Biomarkers: A Systematic Review. Cureus 2021, 13, e18273. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, X.; Li, X.; Chen, H.; Hu, Y.; Zhang, X.; Tang, X.; Miao, Y.; Tian, G.; Shang, H. Statins for the Primary Prevention of Coronary Heart Disease. BioMed Res. Int. 2019, 2019, 4870350. [Google Scholar] [CrossRef] [PubMed]
- Safitri, N.; Alaina, M.F.; Pitaloka, D.A.E.; Abdulah, R. A Narrative Review of Statin-Induced Rhabdomyolysis: Molecular Mechanism, Risk Factors, and Management. Drug Healthc. Patient Saf. 2021, 13, 211–219. [Google Scholar] [CrossRef]
- Kohli, P.; Waters, D.D.; Nemr, R.; Arsenault, B.J.; Messig, M.; DeMicco, D.A.; Laskey, R.; Kastelein, J.J.P. Risk of new-onset diabetes and cardiovascular risk reduction from high-dose statin therapy in pre-diabetics and non-pre-diabetics: An analysis from TNT and IDEAL. J. Am. Coll. Cardiol. 2015, 65, 402–404. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Pradhan, A.; MacFadyen, J.G.; Libby, P.; Glynn, R.J. Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: An analysis from the JUPITER trial. Lancet 2012, 380, 565–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langford, H.G.; Blaufox, M.D.; Borhani, N.O.; Curb, J.D.; Molteni, A.; Schneider, K.A.; Pressel, S. Is thiazide-produced uric acid elevation harmful? Analysis of data from the Hypertension Detection and Follow-up Program. Arch. Intern. Med. 1987, 147, 645–649. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Therapy | N° of Patients | LDL-C Reduction | hs-CRP Reduction |
|---|---|---|---|---|
| Ballantyne et al., 2013 [25] | BA 40 vs. placebo BA 80 vs. placebo BA120 mg vs. placebo | 177 | BA group −17.9% −25% −26.6 −2.1% (Placebo) | BA group −21% −26% −20% −2% (Placebo) |
| Gutierrez et al., 2014 [35] | Bempedoic acid 80 mg for 2 weeks increased to 120 mg after week 2 vs. placebo for 4 weeks | 60 | BA group −42% −4% (Placebo) | BA group −41% +11% (Placebo) |
| Thompson et al., 2015 [36] | Bempedoic acid 60 mg increased to 240 mg at 2 weeks intervals vs. placebo | 56 | BA group −32% 3.3% (Placebo) | BA group −42% 0% (Placebo) |
| Thompson et al., 2016 [38] | BA 120 mg alone; BA 180 mg alone; BA 120mg + Ezetimibe 10 mg; BA 180 mg + Ezetimibe 10 mg Ezetimibe 10 mg alone | 348 | BA group −27% −30% BA + EZE group −43% −48% −21% | BA group −30% −40% BA + EZE group −38% −25% −10.5% |
| Ballantyne et al., 2016 [39] | Stable background statin therapy + BA 120 mg vs. placebo Stable background statin therapy + BA 120 mg vs. placebo | 134 | BA group −17% −24% −4% (Placebo) | BA group −21% −29% −0% (Placebo) |
| Lalwani et al., 2019 [30] | Atorvastatin 80 mg + Bempedoic acid 180 mg vs. placebo | 68 | BA group −13% +9.2% (Placebo) | BA group −34% +0.735% (Placebo) |
| Rubino, MacDougall, Sterling, Hanselman, et al., 2021 [40] | Bempedoic acid 180 mg + Atorvastatin 20 mg + Ezetimibe 10 mg vs. placebo | 63 | BA group −63.6% −3.1% (Placebo) | BA group −47.7% −2.7% (Placebo) |
| Rubino, MacDougall, Sterling, Kelly, et al., 2021 [41] | Evolocumab 430 mg + Bempedoic acid 180 mg vs. placebo | 59 | −27.5% (BA) −3.1% (Placebo) | −34% (BA) −1.6% (Placebo) |
| Study | Therapy | N° of Patients | LDL-C Reduction | hs-CRP Reduction |
|---|---|---|---|---|
| Ballantyne et al., 2018 CLEAR Tranquility [43] | Bempedoic acid 180 mg + Ezetimibe 10 mg vs. Placebo + Ezetimibe 10 mg in addition to lipid-lowering therapy including low-dose or very low-dose statin. | 269 | −23.5% vs. + 5% | −32% vs. +2.1% |
| Laufs et al., 2019 CLEAR Serenity [42] | Bempedoic acid 180 mg vs. Placebo in addition to stable lipid-lowering therapy including low-dose or very low-dose statin. | 345 | −23.6% vs. −1.3% | −25.4% vs. +2.7% |
| Ray et al., 2019 CLEAR Harmony [44] | Bempedoic acid 180 mg vs. Placebo in addition to maximally tolerated statin therapy with or without additional lipid-lowering therapy | 2230 | −16.5% vs. +1.6% | −22.4% vs. +2.6% |
| Goldberg et al., 2019 CLEAR Wisdom [45] | Bempedoic acid 180 mg vs. Placebo in addition to tolerated statin therapy with or without additional lipid-lowering therapy | 779 | −15.1% vs. 2.4% | −18.7% vs. −9.4% |
| Ballantyne et al., 2020 [46] | BA 180 mg + EZE 10 mg BA 180 mg EZE 10 mg Placebo (in addition to maximally tolerated statin therapy) | 301 | −36.2% −17.2% −23.2% +1.8% | −35.1% −31.9% −8.2% +21.6% |
| Nissen et al., 2023 CLEAR Outcomes [47] | BA 180 mg Placebo in addition to stable lipid-lowering therapy including very low-dose statin. | 13,970 | −21.7% −0.6% (at 6th month) | −22.2% +2.4% (at 6th month) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Natale, F.; Molinari, R.; Franzese, R.; Mollo, N.; Cimmino, G. Bempedoic Acid and Statins in Lipid-Lowering Strategy: Which Came First, the Egg or the Chicken? Future Pharmacol. 2023, 3, 392-406. https://doi.org/10.3390/futurepharmacol3020024
Natale F, Molinari R, Franzese R, Mollo N, Cimmino G. Bempedoic Acid and Statins in Lipid-Lowering Strategy: Which Came First, the Egg or the Chicken? Future Pharmacology. 2023; 3(2):392-406. https://doi.org/10.3390/futurepharmacol3020024
Chicago/Turabian StyleNatale, Francesco, Riccardo Molinari, Rosa Franzese, Noemi Mollo, and Giovanni Cimmino. 2023. "Bempedoic Acid and Statins in Lipid-Lowering Strategy: Which Came First, the Egg or the Chicken?" Future Pharmacology 3, no. 2: 392-406. https://doi.org/10.3390/futurepharmacol3020024