
Paclitaxel—A Valuable Tool for Inducing Visceral Pain in Preclinical Testing?


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Treatments
2.2. Tests for the Evaluation of Visceral Nociception
2.2.1. Scale of Abdominal Pain
2.2.2. Tactile Hypersensitivity
2.2.3. Thermal Hypersensitivity
2.3. Statistical Analysis
3. Results
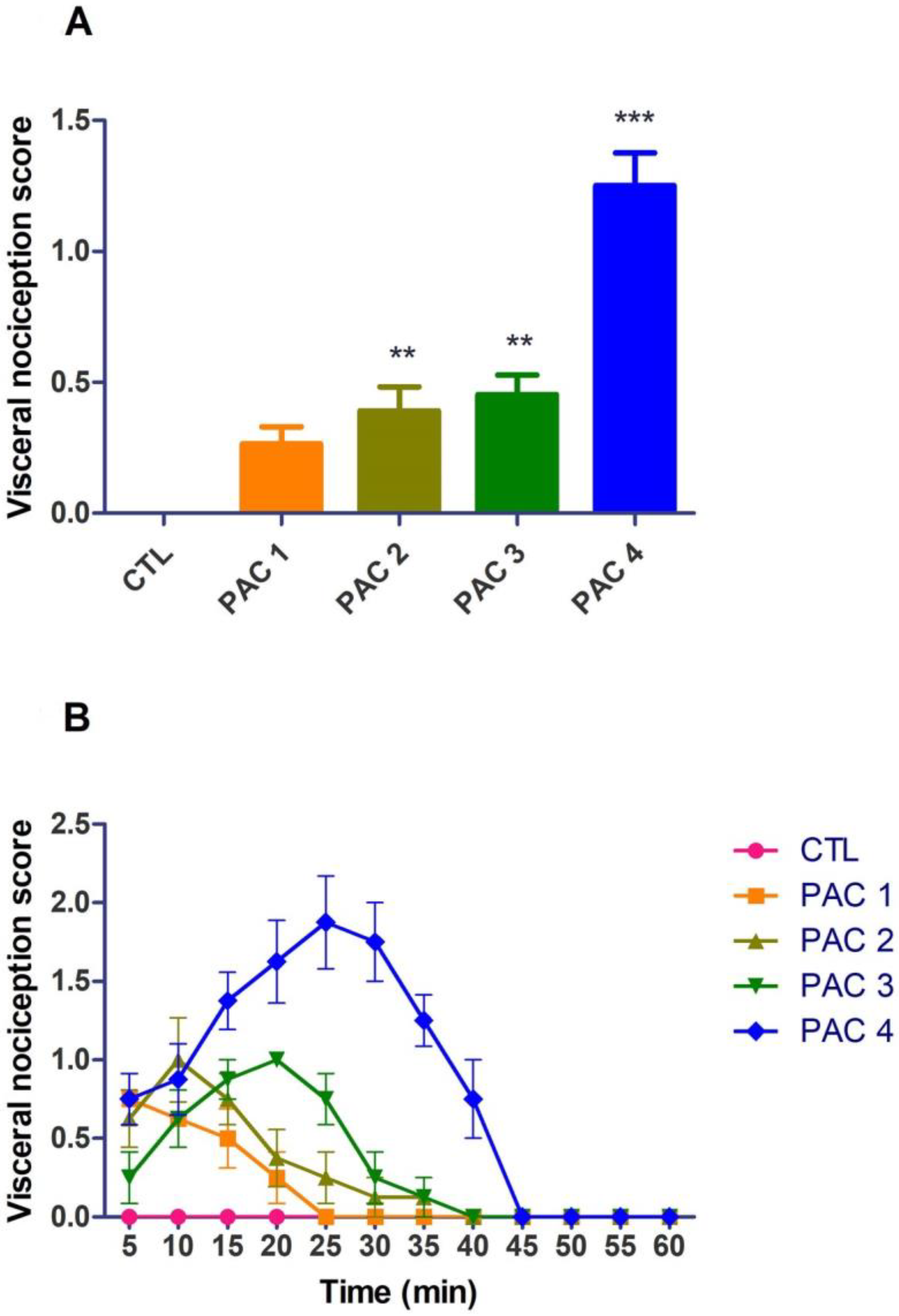
3.1. Assessment of Visceral Pain Using the Scale of Abdominal Pain
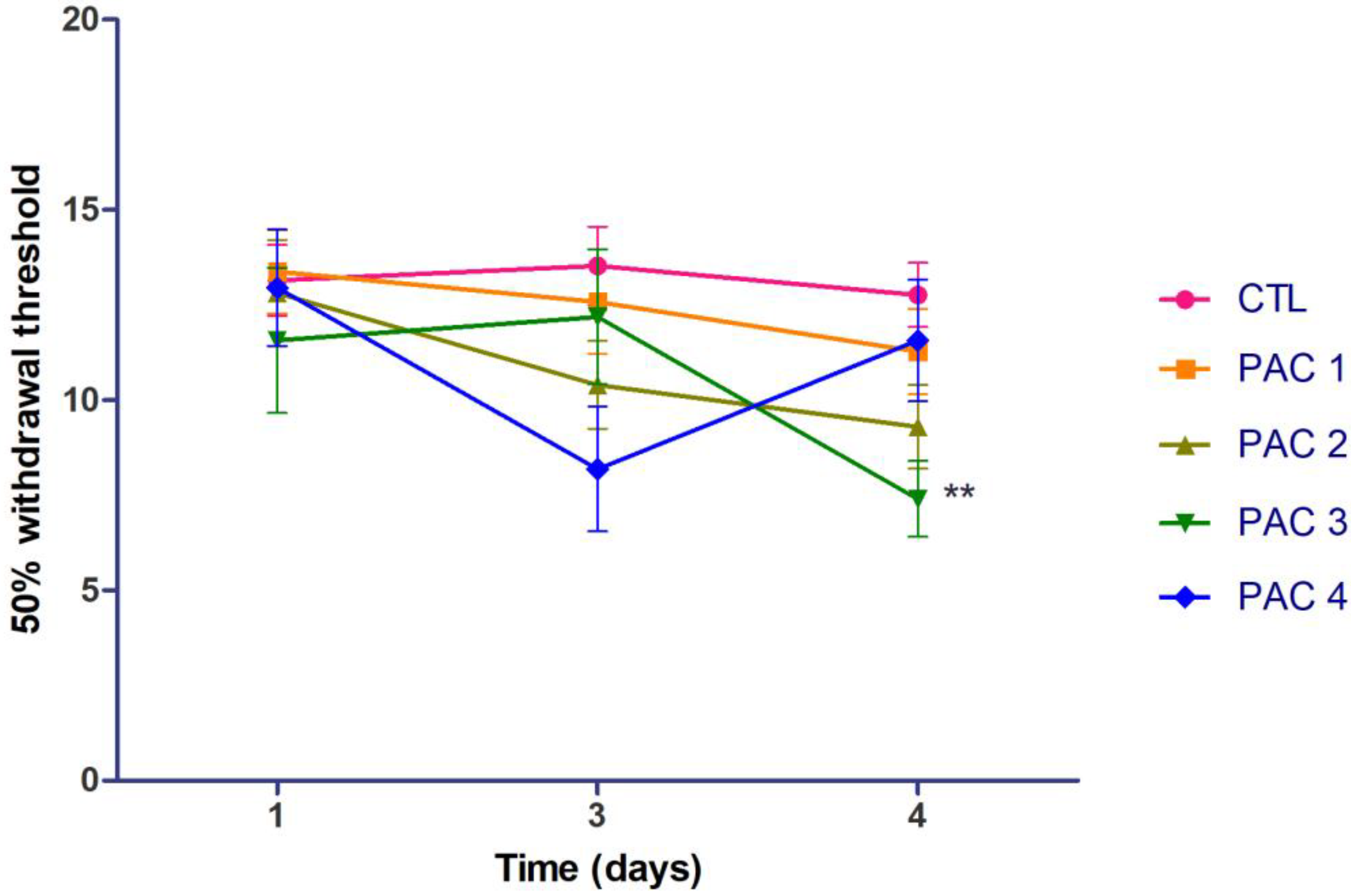
3.2. Tactile Hypersensitivity
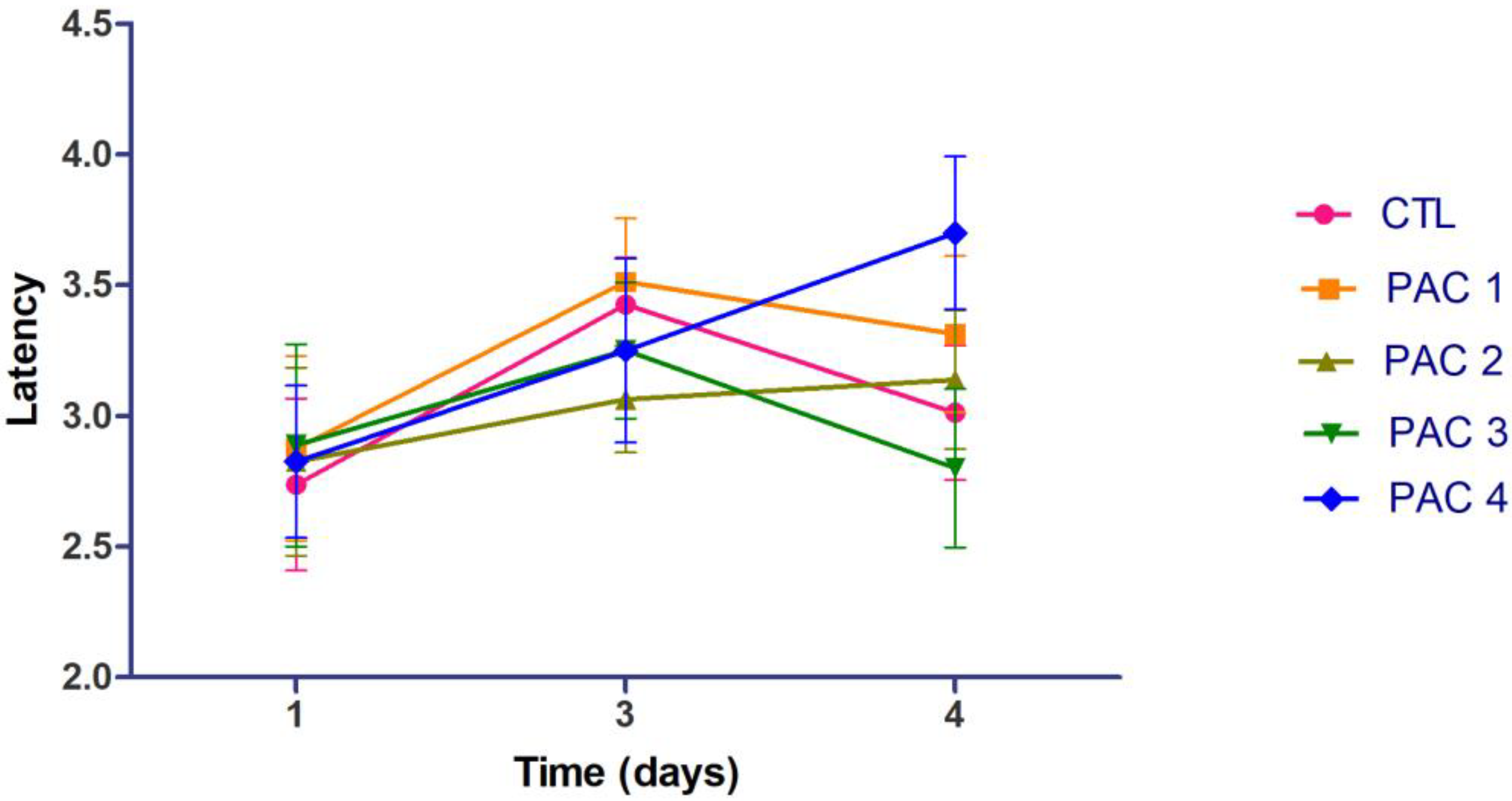
3.3. Thermal Hypersensitivity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collett, B. Visceral Pain: The Importance of Pain Management Services. Br. J. Pain 2013, 7, 6–7. [Google Scholar] [CrossRef] [Green Version]
- Al-Chaer, E.D.; Traub, R.J. Biological Basis of Visceral Pain: Recent Developments. Pain 2002, 96, 221–225. [Google Scholar] [CrossRef]
- Cervero, F.; Laird, J.M.A. Visceral Pain. Lancet 1999, 353, 2145–2148. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.C.; Greenwood-Van Meerveld, B. The Pharmacology of Visceral Pain, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Volume 75, ISBN 9780128038833. [Google Scholar]
- Pacheco-Carroza, E.A. Visceral Pain, Mechanisms, and Implications in Musculoskeletal Clinical Practice. Med. Hypotheses 2021, 153, 110624. [Google Scholar] [CrossRef]
- Sikandar, S.; Dickenson, A.H. Visceral Pain: The Ins and Outs, the Ups and Downs. Curr. Opin. Support. Palliat. Care 2012, 6, 17–26. [Google Scholar] [CrossRef]
- Clarke, G.; Quigley, E.M.M.; Cryan, J.F.; Dinan, T.G. Irritable Bowel Syndrome: Towards Biomarker Identification. Trends Mol. Med. 2009, 15, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Pusceddu, M.M.; Gareau, M.G. Visceral Pain: Gut Microbiota, a New Hope? J. Biomed. Sci. 2018, 25, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynch, M.E.; Craig, K.D.; Peng, P.W. Visceral pain. In Clinical Pain Management: A Practical Guide, 2nd ed.; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2022; pp. 355–365. [Google Scholar] [CrossRef]
- Molus, L.; Kansal, A. Visceral Pain. Anaesth. Intensive Care Med. 2022, 23, 535–539. [Google Scholar] [CrossRef]
- Gebhart, G.F. Pathobiology of Visceral Pain: Molecular Mechanisms and Therapeutic Implications. IV. Visceral Afferent Contributions to the Pathobiology of Visceral Pain. Am. J. Physiol.-Gastrointest. Liver Physiol. 2000, 278, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Hungin, A.P.S.; Whorwell, P.J.; Tack, J.; Mearin, F. The Prevalence, Patterns and Impact of Irritable Bowel Syndrome: An International Survey of 40 000 Subjects. Aliment. Pharmacol. Ther. 2003, 17, 643–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wie, C.; Ghanavatian, S.; Pew, S.; Kim, A.; Strand, N.; Freeman, J.; Maita, M.; Covington, S.; Maloney, J. Interventional Treatment Modalities for Chronic Abdominal and Pelvic Visceral Pain. Curr. Pain Headache Rep. 2022, 26, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Grundy, L.; Erickson, A.; Brierley, S.M. Visceral Pain. Annu. Rev. Physiol. 2019, 81, 261–284. [Google Scholar] [CrossRef]
- Ahlbeck, K. Opioids: A Two-Faced Janus. Curr. Med. Res. Opin. 2011, 27, 439–448. [Google Scholar] [CrossRef]
- Olesen, A.E.; Farmer, A.D.; Olesen, S.S.; Aziz, Q.; Drewes, A.M. Management of Chronic Visceral Pain. Pain Manag. 2016, 6, 469–486. [Google Scholar] [CrossRef] [PubMed]
- Micó, J.A.; Ardid, D.; Berrocoso, E.; Eschalier, A. Antidepressants and Pain. Trends Pharmacol. Sci. 2006, 27, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Stepanovíc-Petrovíc, R.M.; Tomíc, M.A.; Vučkovíc, S.M.; Paranos, S.; Ugrešíc, N.D.; Prostran, M.Š.; Milovanovíc, S.; Boškovíc, B. The Antinociceptive Effects of Anticonvulsants in a Mouse Visceral Pain Model. Anesth. Analg. 2008, 106, 1897–1903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meymandi, M.S.; Sepehri, G. Gabapentin Action and Interaction on the Antinociceptive Effect of Morphine on Visceral Pain in Mice. Eur. J. Anaesthesiol. 2008, 25, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Lambarth, A.; Zarate-Lopez, N.; Fayaz, A. Oral and Parenteral Anti-Neuropathic Agents for the Management of Pain and Discomfort in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. Neurogastroenterol. Motil. 2022, 34, e14289. [Google Scholar] [CrossRef]
- Davis, M.P. Drug Management of Visceral Pain: Concepts from Basic Research. Pain Res. Treat. 2012, 2012, 265605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Pérez, C.A. Visceral Pain: The Neurophysiological Mechanism. Geotech. Geol. Earthq. Eng. 2016, 16, 129–145. [Google Scholar] [CrossRef]
- Regmi, B.; Shah, M.K. Possible Implications of Animal Models for the Assessment of Visceral Pain. Anim. Model. Exp. Med. 2020, 3, 215–228. [Google Scholar] [CrossRef]
- Johnson, A.C.; Farmer, A.D.; Ness, T.J.; Greenwood-Van Meerveld, B. Critical Evaluation of Animal Models of Visceral Pain for Therapeutics Development: A Focus on Irritable Bowel Syndrome. Neurogastroenterol. Motil. 2020, 32, e13776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staahl, C.; Drewes, A.M. Experimental Human Pain Models: A Review of Standardised Methods for Preclinical Testing of Analgesics. Basic Clin. Pharmacol. Toxicol. 2004, 95, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Le Bars, D.; Gozariu, M.; Cadden, S.W. Animal Models of Nociception. Pharmacol. Rev. 2001, 53, 597–652. [Google Scholar] [CrossRef] [PubMed]
- Pearl, J.; Stander, H.; McKean, D.B. Effects of Analgesics and Other Drugs on Mice in Phenylquinone and Rotarod Tests. J. Pharmacol. Exp. Ther. 1969, 167, 9–13. [Google Scholar] [PubMed]
- Bernabeu, E.; Cagel, M.; Lagomarsino, E.; Moretton, M.; Chiappetta, D.A. Paclitaxel: What Has Been Done and the Challenges Remain Ahead. Int. J. Pharm. 2017, 526, 474–495. [Google Scholar] [CrossRef]
- Alves, R.C.; Fernandes, R.P.; Eloy, J.O.; Salgado, H.R.N.; Chorilli, M. Characteristics, Properties and Analytical Methods of Paclitaxel: A Review. Crit. Rev. Anal. Chem. 2018, 48, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.H.; Mao, J.W.; Tan, X.L. Research Progress on the Source, Production, and Anti-Cancer Mechanisms of Paclitaxel. Chin. J. Nat. Med. 2020, 18, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Armat, M.; Bakhshaiesh, T.O.; Sabzichi, M.; Shanehbandi, D.; Sharifi, S.; Molavi, O.; Mohammadian, J.; Hejazi, M.S.; Samadi, N. The Role of Six1 Signaling in Paclitaxel-Dependent Apoptosis in MCF-7 Cell Line. Bosn. J. Basic Med. Sci. 2016, 16, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampan, N.C.; Madondo, M.T.; McNally, O.M.; Quinn, M.; Plebanski, M. Paclitaxel and Its Evolving Role in the Management of Ovarian Cancer. Biomed Res. Int. 2015, 2015, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Mahayri, Z.N.; AlAhmad, M.M.; Ali, B.R. Current Opinion on the Pharmacogenomics of Paclitaxel-Induced Toxicity. Expert Opin. Drug Metab. Toxicol. 2021, 17, 785–801. [Google Scholar] [CrossRef]
- Klein, I.; Lehmann, H.C. Pathomechanisms of Paclitaxel-Induced Peripheral Neuropathy. Toxics 2021, 9, 229. [Google Scholar] [CrossRef] [PubMed]
- Goode, D.J.; Whitaker, E.E.; Mecum, N.E. Ovariectomy Increases Paclitaxel-Induced Mechanical Hypersensitivity and Reduces Anti-Inflammatory CD4+ T Cells in the Dorsal Root Ganglion of Female Mice. J. Neuroimmunol. 2022, 367, 577878. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, C.L.; Maddocks-Christianson, K.; Wolf, S.L.; Rao, R.D.; Dyck, P.J.B.; Mantyh, P.; Dyck, P.J. The Paclitaxel Acute Pain Syndrome: Sensitization of Nociceptors as the Putative Mechanism. Cancer J. 2007, 13, 399–403. [Google Scholar] [CrossRef]
- Reeves, B.N.; Dakhil, S.R.; Sloan, J.A.; Wolf, S.L.; Burger, K.N.; Kamal, A.; Le-Lindqwister, N.A.; Soori, G.S.; Jaslowski, A.J.; Kelaghan, J.; et al. Further Data Supporting That Paclitaxel-Associated Acute Pain Syndrome Is Associated with Development of Peripheral Neuropathy: North Central Cancer Treatment Group Trial N08C1. Cancer 2012, 118, 5171–5178. [Google Scholar] [CrossRef]
- Zhou, Q.; Price, D.D.; Caudle, R.M.; Nicholas Verne, G. Visceral and Somatic Hypersensitivity in a Subset of Rats Following TNBS-Induced Colitis. Pain 2008, 134, 9–15. [Google Scholar] [CrossRef]
- Shaikh, D.H.; Baiomi, A.; Mehershahi, S.; Abbas, H.; Gongati, S.; Nayudu, S.K. Paclitaxel-Induced Bowel Perforation: A Rare Cause of Acute Abdomen. Case Rep. Gastroenterol. 2020, 14, 687–694. [Google Scholar] [CrossRef]
- Rodrigues, F.G.; Dasilva, G.; Wexner, S.D. Neutropenic Enterocolitis. World J. Gastroenterol. 2017, 23, 42. [Google Scholar] [CrossRef]
- Rossato, M.F.; Rigo, F.K.; Oliveira, S.M.; Guerra, G.P.; Silva, C.R.; Cunha, T.M.; Gomez, M.V.; Ferreira, J.; Trevisan, G. Participation of Transient Receptor Potential Vanilloid 1 in Paclitaxel-Induced Acute Visceral and Peripheral Nociception in Rodents. Eur. J. Pharmacol. 2018, 828, 42–51. [Google Scholar] [CrossRef]
- Charan, J.; Kantharia, N. How to Calculate Sample Size in Animal Studies? J. Pharmacol. Pharmacother. 2013, 4, 303–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trevisan, G.; Rossato, M.F.; Hoffmeister, C.; Oliveira, S.M.; Silva, C.R.; Matheus, F.C.; Mello, G.C.; Antunes, E.; Prediger, R.D.S.; Ferreira, J. Mechanisms Involved in Abdominal Nociception Induced by Either TRPV1 or TRPA1 Stimulation of Rat Peritoneum. Eur. J. Pharmacol. 2013, 714, 332–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavrielides, A.T.; Sukow, D.W. Experimental observations. In Unlocking Dynamical Diversity: Optical Feedback Effects on Semiconductor Lasers; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2005; pp. 81–145. [Google Scholar] [CrossRef]
- Dixon, W.J. The Up-and-Down Method for Small Samples. J. Am. Stat. Assoc. 1965, 60, 967–978. [Google Scholar] [CrossRef]
- Chaplan, S.R.; Bach, F.W.; Pogrel, J.W.; Chung, J.M.; Yaksh, T.L. Quantitative Assessment of Tactile Allodynia in the Rat Paw. J. Neurosci. Methods 1994, 53, 55–63. [Google Scholar] [CrossRef]
- Deuis, J.R.; Dvorakova, L.S.; Vetter, I. Methods Used to Evaluate Pain Behaviors in Rodents. Front. Mol. Neurosci. 2017, 10, 284. [Google Scholar] [CrossRef] [Green Version]
- D’Amour, F.E.; Smith, D.L. A Method for Determining Loss of Pain Sensation. J. Pharmacol. Exp. Ther. 1941, 72, 74–79. [Google Scholar]
- Sugarbaker, P.H. Intraperitoneal Paclitaxel: Pharmacology, Clinical Results and Future Prospects. J. Gastrointest. Oncol. 2021, 12, S231–S239. [Google Scholar] [CrossRef] [PubMed]
- Markman, M.; Brady, M.F.; Spirtos, N.M.; Hanjani, P.; Rubin, S.C. Phase II Trial of Intraperitoneal Paclitaxel in Carcinoma of the Ovary, Tube, and Peritoneum: A Gynecologic Oncology Group Study. J. Clin. Oncol. 1998, 16, 2620–2624. [Google Scholar] [CrossRef]
- Nair, A.; Jacob, S. A Simple Practice Guide for Dose Conversion between Animals and Human. J. Basic Clin. Pharm. 2016, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Yan, X.; Maixner, D.W.; Yadav, R.; Gao, M.; Li, P.; Bartlett, M.G.; Weng, H.R. Paclitaxel Induces Acute Pain via Directly Activating Toll like Receptor 4. Mol. Pain 2015, 11, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Loprinzi, C.L.; Reeves, B.N.; Dakhil, S.R.; Sloan, J.A.; Wolf, S.L.; Burger, K.N.; Kamal, A.; Le-Lindqwister, N.A.; Soori, G.S.; Jaslowski, A.J.; et al. Natural History of Paclitaxel-Associated Acute Pain Syndrome: Prospective Cohort Study NCCTG N08C1. J. Clin. Oncol. 2011, 29, 1472–1478. [Google Scholar] [CrossRef]
- Garrison, J.A.; McCune, J.S.; Livingston, R.B.; Linden, H.M.; Gralow, J.R.; Ellis, G.K.; West, H.L. Myalgias and Arthralgias Associated with Paclitaxel: Incidence and Management. Oncology 2003, 17, 271–277. [Google Scholar] [PubMed]
- Kamata, Y.; Kambe, T.; Chiba, T.; Yamamoto, K.; Kawakami, K.; Abe, K.; Taguchi, K. Paclitaxel Induces Upregulation of Transient Receptor Potential Vanilloid 1 Expression in the Rat Spinal Cord. Int. J. Mol. Sci. 2020, 21, 4341. [Google Scholar] [CrossRef] [PubMed]
- Hara, T.; Chiba, T.; Abe, K.; Makabe, A.; Ikeno, S.; Kawakami, K.; Utsunomiya, I.; Hama, T.; Taguchi, K. Effect of Paclitaxel on Transient Receptor Potential Vanilloid 1 in Rat Dorsal Root Ganglion. Pain 2013, 154, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Adamek, P.; Zhang, H.; Tatsui, C.E.; Rhines, L.D.; Mrozkova, P.; Li, Q.; Kosturakis, A.K.; Cassidy, R.M.; Harrison, D.S.; et al. The Cancer Chemotherapeutic Paclitaxel Increases Human and Rodent Sensory Neuron Responses to TRPV1 by Activation of TLR4. J. Neurosci. 2015, 35, 13487–13500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Huang, F.; Xu, Y.; Xiang, W.; Xie, C. TRPV1 Is Involved in the Antinociceptive Effects of Resveratrol in Paclitaxel-Induced Neuropathic Pain. All Life 2021, 14, 66–74. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, F.; Zhang, S.; Mao, M.; Feng, S.; Wang, X. Participation of Transient Receptor Potential Vanilloid 1 in the Analgesic Effect of Duloxetine for Paclitaxel Induced Peripheral Neuropathic Pain. Neurosci. Lett. 2022, 773, 136512. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.W.; Cho, H.; Kwak, J.; Lee, S.Y.; Kang, C.J.; Jung, J.; Cho, S.; Min, K.H.; Suh, Y.G.; Kim, D.; et al. Direct Activation of Capsaicin Receptors by Products of Lipoxygenases: Endogenous Capsaicin-like Substances. Proc. Natl. Acad. Sci. USA 2000, 97, 6155–6160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, S.W.; Oh, U. Hot Channels in Airways: Pharmacology of the Vanilloid Receptor. Curr. Opin. Pharmacol. 2002, 2, 235–242. [Google Scholar] [CrossRef]
- Hwang, S.J.; Valtschanoff, J.G. Vanilloid Receptor VR1-Positive Afferents Are Distributed Differently at Different Levels of the Rat Lumbar Spinal Cord. Neurosci. Lett. 2003, 349, 41–44. [Google Scholar] [CrossRef]
- Gaiotte, L.B.; Carvalho Cesário, R.; Silveira, H.S.; Augusto De Morais Oliveira, D.; Cucielo, M.S.; Gorete Romagnoli, G.; Kaneno, R.; Aparecida, D.; De Campos Zuccari, P.; Reiter, R.J.; et al. Combination of Melatonin with Paclitaxel Reduces the TLR4-Mediated Inflammatory Pathway, PD-L1 Levels, and Survival of Ovarian Carcinoma Cells. Melatonin Res. 2022, 5, 34–51. [Google Scholar] [CrossRef]
- Illias, A.M.; Yu, K.J.; Hwang, S.H.; Solis, J.; Zhang, H.; Velasquez, J.F.; Cata, J.P.; Dougherty, P.M. Dorsal Root Ganglion Toll-like Receptor 4 Signaling Contributes to Oxaliplatin-Induced Peripheral Neuropathy. Pain 2022, 163, 923–935. [Google Scholar] [CrossRef]
- Tramullas, M.; Finger, B.C.; Moloney, R.D.; Golubeva, A.V.; Moloney, G.; Dinan, T.G.; Cryan, J.F. Toll-like Receptor 4 Regulates Chronic Stress-Induced Visceral Pain in Mice. Biol. Psychiatry 2014, 76, 340–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, L.F.; Yu, L.; Wang, L.M.; He, J.T.; Sun, J.L.; Wang, X.B.; Bai, Z.H.; Wang, H.; Yan, T.L.; Pei, H.H. The Toll-like Receptor 4 Antagonist TAK-242 Protects against Chronic Pancreatitis in Rats. Mol. Med. Rep. 2017, 16, 3863–3868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramullas, M.; Finger, B.C.; Dinan, T.G.; Cryan, J.F. Obesity Takes Its Toll on Visceral Pain: High-Fat Diet Induces Toll-like Receptor 4-Dependent Visceral Hypersensitivity. PLoS ONE 2016, 11, e0155367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, B.Y.; Kim, E.S.; Kim, C.H.; Kwon, J.Y.; Kim, H.K. Gender Differences in Paclitaxel-Induced Neuropathic Pain Behavior and Analgesic Response in Rats. Korean J. Anesthesiol. 2012, 62, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huynh, P.N.; Giuvelis, D.; Christensen, S.; Tucker, K.L.; McIntosh, J.M. RgIA4 Accelerates Recovery from Paclitaxel-Induced Neuropathic Pain in Rats. Mar. Drugs 2020, 18, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrei, C.; Zanfirescu, A.; Mihai, D.P.; Negreș, S. Paclitaxel—A Valuable Tool for Inducing Visceral Pain in Preclinical Testing? Int. J. Transl. Med. 2023, 3, 108-119. https://doi.org/10.3390/ijtm3010010
Andrei C, Zanfirescu A, Mihai DP, Negreș S. Paclitaxel—A Valuable Tool for Inducing Visceral Pain in Preclinical Testing? International Journal of Translational Medicine. 2023; 3(1):108-119. https://doi.org/10.3390/ijtm3010010
Chicago/Turabian StyleAndrei, Corina, Anca Zanfirescu, Dragoș Paul Mihai, and Simona Negreș. 2023. "Paclitaxel—A Valuable Tool for Inducing Visceral Pain in Preclinical Testing?" International Journal of Translational Medicine 3, no. 1: 108-119. https://doi.org/10.3390/ijtm3010010