
Comparison of the Basic Reproduction Numbers for COVID-19 through Four Waves of the Pandemic in Vietnam
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
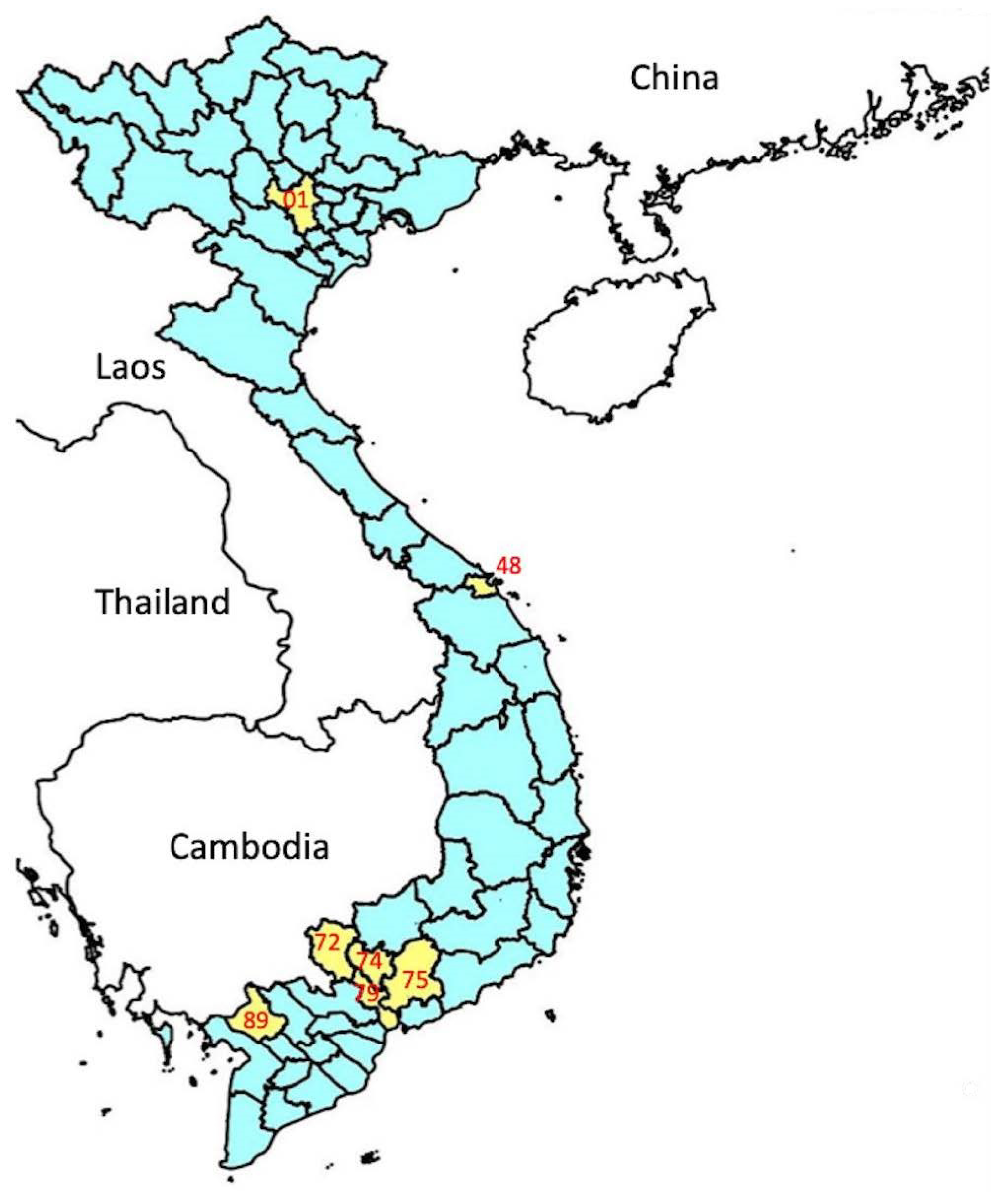
2.1. Study Area
2.2. Data Collection
2.3. Calculation of the Basic Reproduction Number (R0)
2.4. Calculation of Minimal Vaccination Coverage for COVID-19
2.5. Data Analysis
3. Results
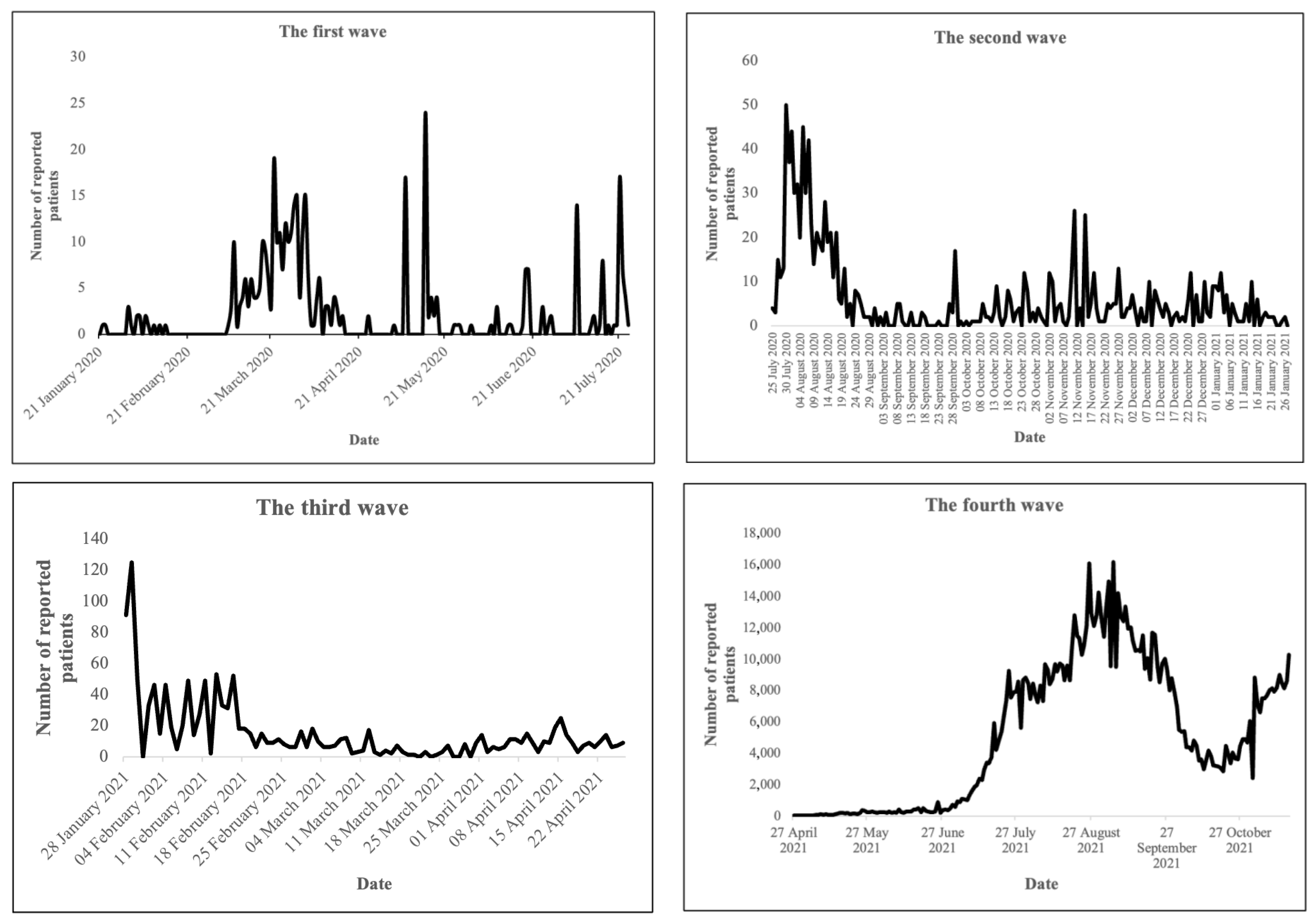
3.1. R0 Values of COVID-19 at the National Level from the First Three Waves of the Pandemic in Vietnam
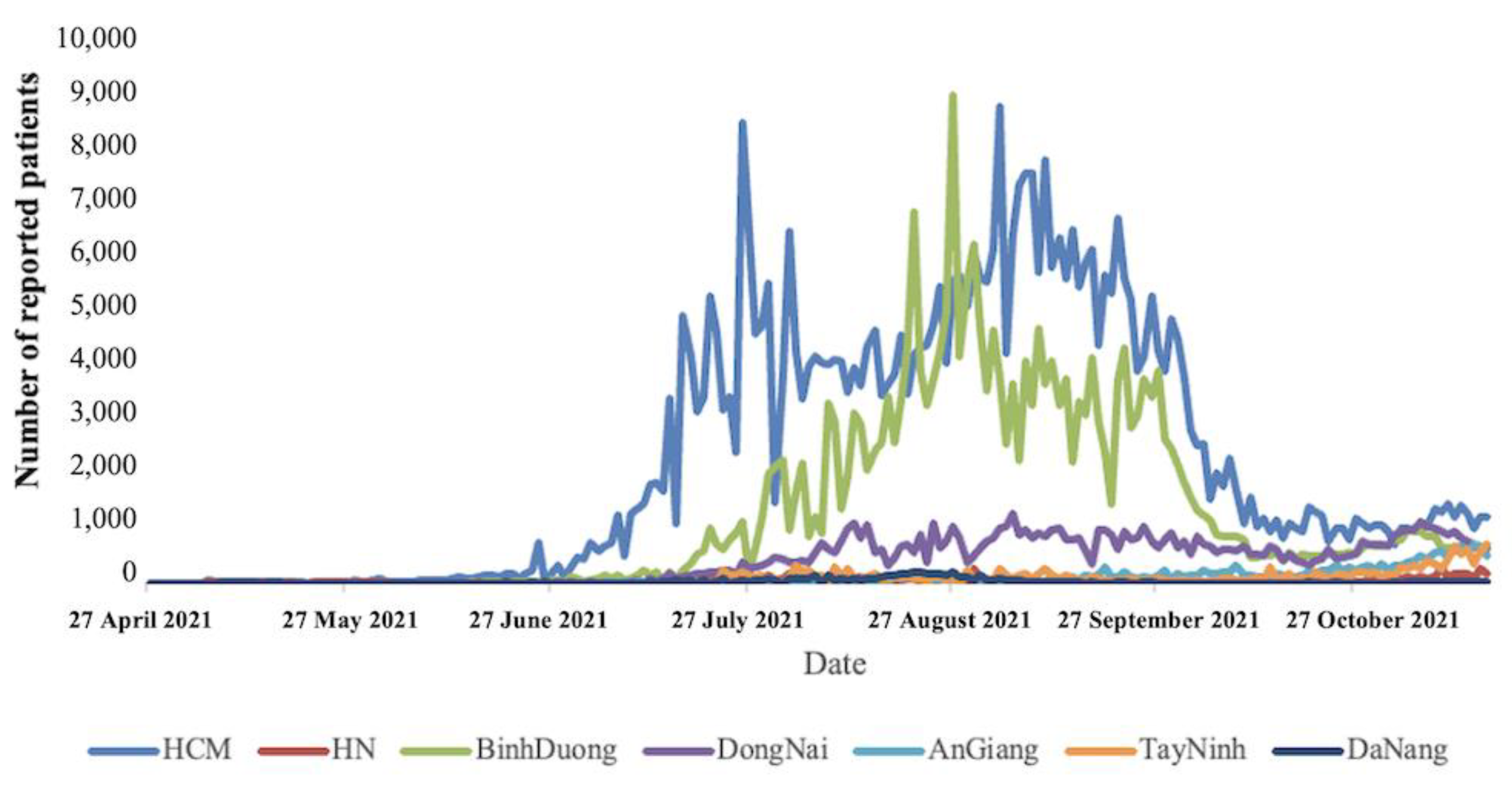
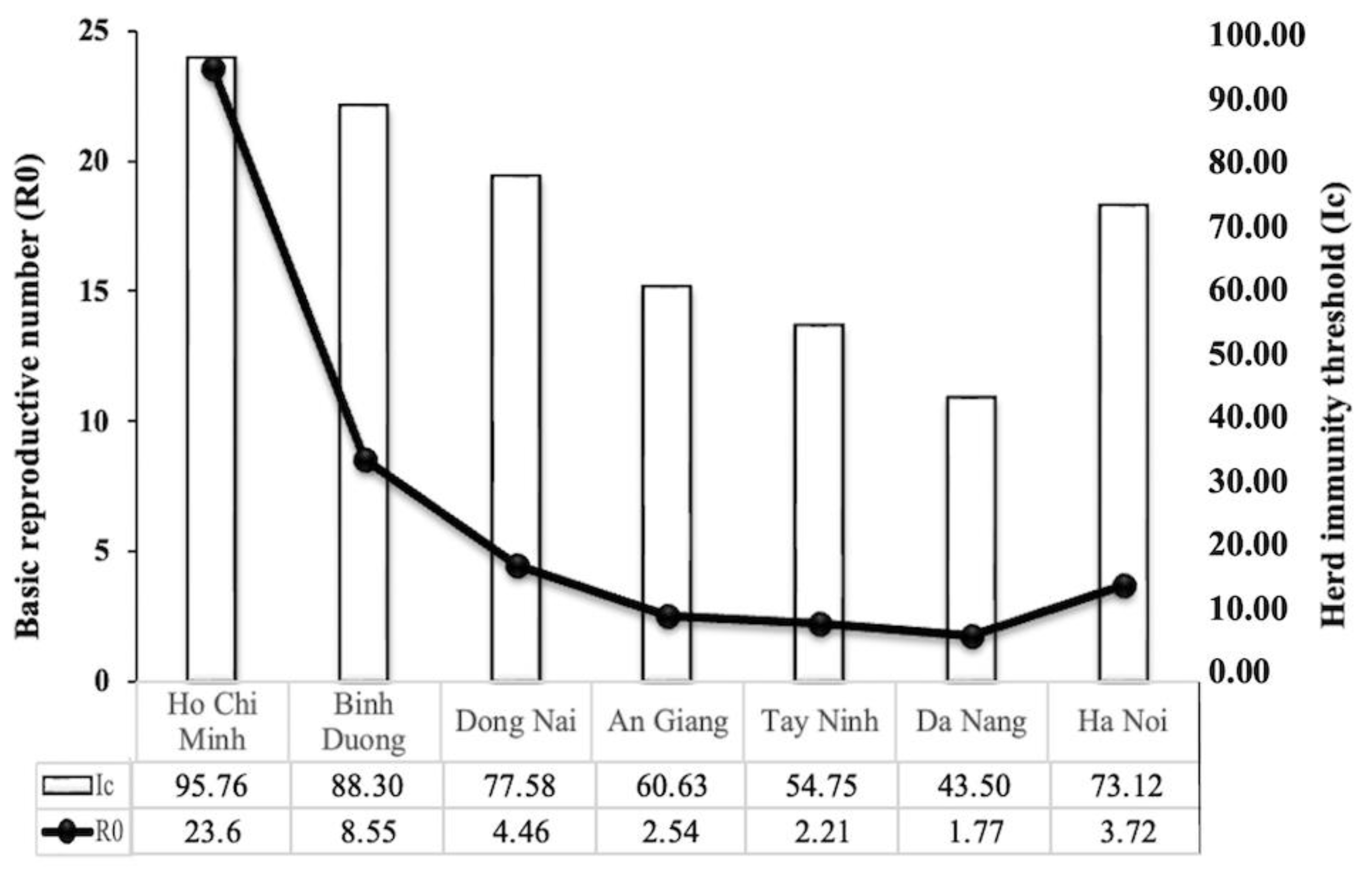
3.2. R0 Values of COVID-19 at the Province Level in Some Locations from the Fourth Wave of the Pandemic in Vietnam
3.3. Minimal Vaccination Coverage for COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abd Elaziz, M.; Dahou, A.; Alsaleh, N.A.; Elsheikh, A.H.; Saba, A.I.; Ahmadein, M. Boosting COVID-19 Image Classification Using MobileNetV3 and Aquila Optimizer Algorithm. Entropy 2021, 23, 1383. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, A.H.; Saba, A.I.; Panchal, H.; Shanmugan, S.; Alsaleh, N.A.; Ahmadein, M. Artificial Intelligence for Forecasting the Prevalence of COVID-19 Pandemic: An Overview. Healthcare 2021, 9, 1614. [Google Scholar] [CrossRef] [PubMed]
- Achaiah, N.C.; Subbarajasetty, S.B.; Shetty, R.M. R0 and Re of COVID-19: Can We Predict When the Pandemic Outbreak will be Contained? Indian J. Crit. Care Med. 2020, 24, 1125–1127. [Google Scholar] [CrossRef] [PubMed]
- Delamater, P.L.; Street, E.J.; Leslie, T.F.; Yang, Y.T.; Jacobsen, K.H. Complexity of the Basic Reproduction Number (R0). Emerg. Infect. Dis. 2019, 25, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (R0) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef]
- Dietz, K. The estimation of the basic reproduction number for infectious diseases. Stat. Methods Med. Res. 1993, 2, 23–41. [Google Scholar] [CrossRef]
- Maiese, A.; Baronti, A.; Manetti, A.C.; Di Paolo, M.; Turillazzi, E.; Frati, P.; Fineschi, V. Death after the Administration of COVID-19 Vaccines Approved by EMA: Has a Causal Relationship Been Demonstrated? Vaccines 2022, 10, 308. [Google Scholar] [CrossRef]
- Elsheikh, A.H.; Saba, A.I.; Elaziz, M.A.; Lu, S.; Shanmugan, S.; Muthuramalingam, T.; Kumar, R.; Mosleh, A.O.; Essa, F.A.; Shehabeldeen, T.A. Deep learning-based forecasting model for COVID-19 outbreak in Saudi Arabia. Process Saf. Environ. Prot. 2021, 149, 223–233. [Google Scholar] [CrossRef]
- Saba, A.I.; Elsheikh, A.H. Forecasting the prevalence of COVID-19 outbreak in Egypt using nonlinear autoregressive artificial neural networks. Process Saf. Environ. Prot. 2020, 141, 1–8. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Zhang, C.; Huang, S.; Zheng, F.; Dai, Y. Controversial treatments: An updated understanding of the coronavirus disease 2019. J. Med. Virol. 2020, 92, 1441–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dharmaratne, S.; Sudaraka, S.; Abeyagunawardena, I.; Manchanayake, K.; Kothalawala, M.; Gunathunga, W. Estimation of the basic reproduction number (R0) for the novel coronavirus disease in Sri Lanka. Virol. J. 2020, 17, 144. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Diao, M.; Yu, W.; Pei, L.; Lin, Z.; Chen, D. Estimation of the reproductive number of novel coronavirus (COVID-19) and the probable outbreak size on the Diamond Princess cruise ship: A data-driven analysis. Int. J. Infect. Dis. 2020, 93, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Li, M.; Lv, G.; Lu, Z.K. Monitoring transmissibility and mortality of COVID-19 in Europe. Int. J. Infect. Dis. 2020, 95, 311–315. [Google Scholar] [CrossRef]
- Xu, C.; Dong, Y.; Yu, X.; Wang, H.; Tsamlag, L.; Zhang, S.; Chang, R.; Wang, Z.; Yu, Y.; Long, R.; et al. Estimation of reproduction numbers of COVID-19 in typical countries and epidemic trends under different prevention and control scenarios. Front. Med. 2020, 14, 613–622. [Google Scholar] [CrossRef]
- Locatelli, I.; Trächsel, B.; Rousson, V. Estimating the basic reproduction number for COVID-19 in Western Europe. PLoS ONE 2021, 16, e0248731. [Google Scholar] [CrossRef]
- Viceconte, G.; Petrosillo, N. COVID-19 R0: Magic number or conundrum? Infect. Dis. Rep. 2020, 12, 8516. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, taaa021. [Google Scholar] [CrossRef] [Green Version]
- Ke, R.; Romero-Severson, E.; Sanche, S.; Hengartner, N. Estimating the reproductive number R0 of SARS-CoV-2 in the United States and eight European countries and implications for vaccination. J. Theor. Biol. 2021, 517, 110621. [Google Scholar] [CrossRef]
- Nguyen, T.P.; Wong, Z.S.; Wang, L.; Thanh, T.T.; Van Nguyen, H.; Gilmour, S. Rapid impact assessments of COVID-19 control measures against the Delta variant and short-term projections of new confirmed cases in Vietnam. J. Glob. Health 2021, 11, 03118. [Google Scholar] [CrossRef]
- Van Nguyen, Q.; Cao, D.A.; Nghiem, S.H. Spread of COVID-19 and policy responses in Vietnam: An overview. Int. J. Infect. Dis. 2021, 103, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Thanh, H.N.; Van, T.N.; Thu, H.N.T.; Van, B.N.; Thanh, B.D.; Thu, H.P.T.; Kieu, A.N.T.; Viet, N.N.; Marks, G.B.; Fox, G.J.; et al. Outbreak investigation for COVID-19 in northern Vietnam. Lancet Infect. Dis. 2020, 20, 535–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Tan, L. COVID-19 control in Vietnam. Nat. Immunol. 2021, 22, 261. [Google Scholar] [CrossRef] [PubMed]
- Ha, B.T.T.; Ngoc Quang, L.; Mirzoev, T.; Tai, N.T.; Thai, P.Q.; Dinh, P.C. Combating the COVID-19 Epidemic: Experiences from Vietnam. Int. J. Environ. Res. Public Health 2020, 17, 3125. [Google Scholar] [CrossRef]
- Nguyen Thi Yen, C.; Hermoso, C.; Laguilles, E.M.; De Castro, L.E.; Camposano, S.M.; Jalmasco, N.; Cua, K.A.; Isa, M.A.; Akpan, E.F.; Ly, T.P.; et al. Vietnam’s success story against COVID-19. Public Health Pract. 2021, 2, 100132. [Google Scholar] [CrossRef]
- Quach, H.L.; Nguyen, K.C.; Hoang, N.A.; Pham, T.Q.; Tran, D.N.; Le, M.T.Q.; Do, H.T.; Vien, C.C.; Phan, L.T.; Ngu, N.D.; et al. Association of public health interventions and COVID-19 incidence in Vietnam, January to December 2020. Int. J. Infect. Dis. 2021, 110 (Suppl. 1), S28–S43. [Google Scholar] [CrossRef] [PubMed]
- Elsaid, M.; Nasef, M.A.; Huy, N.T. R0 of COVID-19 and its impact on vaccination coverage: Compared with previous outbreaks. Hum. Vaccin Immunother. 2021, 17, 3850–3854. [Google Scholar] [CrossRef]
- Fine, P.; Eames, K.; Heymann, D.L. “Herd Immunity”: A Rough Guide. Clin. Infect. Dis. 2011, 52, 911–916. [Google Scholar] [CrossRef]
- Alimohamadi, Y.; Taghdir, M.; Sepandi, M. Estimate of the Basic Reproduction Number for COVID-19: A Systematic Review and Meta-analysis. J. Prev. Med. Public Health = Yebang Uihakhoe Chi 2020, 53, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Prime Minister. Directive 16 on Strict Social Distancing Measures to Prevent and Control. In COVID-19 in 16/CT-TTg; Prime Minister: London, UK, 2020. [Google Scholar]
- Le, T.T.; Vodden, K.; Wu, J.; Atiwesh, G. Policy Responses to the COVID-19 Pandemic in Vietnam. Int. J. Environ. Res. Public Health 2021, 18, 559. [Google Scholar] [CrossRef]
- Nong, V.M.; Le Thi Nguyen, Q.; Doan, T.T.; Van Do, T.; Nguyen, T.Q.; Dao, C.X.; Thi Nguyen, T.H.; Do, C.D. The second wave of COVID-19 in a tourist hotspot in Vietnam. J. Travel Med. 2021, 28, taaa174. [Google Scholar] [CrossRef]
- Van Pham, D.; Hoang, H.; Nguyen, A.V.; Nguyen, N.T.; Van Hoang, N.; Hoang, N.T. The first newborn patient with SARS-CoV-2 variant B.1.1.7 identified in Viet Nam: Treatment and care practices. West. Pac. Surveill. Response J. WPSAR 2021, 12, 77–81. [Google Scholar] [CrossRef]
- Chau, N.V.V.; Ngoc, N.M.; Nguyet, L.A.; Quang, V.M.; Ny, N.T.H.; Khoa, D.B.; Phong, N.T.; Toan, L.M.; Hong, N.T.T.; Tuyen, N.T.K.; et al. An observational study of breakthrough SARS-CoV-2 Delta variant infections among vaccinated healthcare workers in Vietnam. EClinicalMedicine 2021, 41, 101143. [Google Scholar] [CrossRef]
- Nishiura, H.; Kinoshita, R.; Mizumoto, K.; Yasuda, Y.; Nah, K. Transmission potential of Zika virus infection in the South Pacific. Int. J. Infect. Dis. 2016, 45, 95–97. [Google Scholar] [CrossRef] [Green Version]
- Nikbakht, R.; Baneshi, M.R.; Bahrampour, A. Estimation of the Basic Reproduction Number and Vaccination Coverage of Influenza in the United States (2017-18). J. Res. Health Sci. 2018, 18, e00427. [Google Scholar]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Vergnes, J.N. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2021, 384, 1577. [Google Scholar] [CrossRef]
- Knoll, M.D.; Wonodi, C. Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Francis, A.I.; Ghany, S.; Gilkes, T.; Umakanthan, S. Review of COVID-19 vaccine subtypes, efficacy and geographical distributions. Postgrad. Med. J. 2022, 98, 389–394. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outbreak Wave | Time | R0 Estimated Methods | R0 Values | 95% CI |
|---|---|---|---|---|
| 1 | 21 January 2020–24 July 2020 | EG | 1.15 | 0.99–1.31 |
| ML | 1.19 | 0.85–1.61 | ||
| 2 | 25 July 2020–27 January 2021 | EG | 3.31 | 2.72–4.00 |
| ML | 2.92 | 2.35–3.58 | ||
| 3 | 28 January 2021–26 April 2021 | EG | 1.04 | 0.28–1.42 |
| ML | 2.38 | 2.04–2.75 |
| Area | Province | Province Code | R0 Values | |||
|---|---|---|---|---|---|---|
| EG Method | 95% CI | ML Method | 95% CI | |||
| South | Ho Chi Minh | 79 | 22.05 | 21.86–22.24 | 23.60 | 23.33–23.86 |
| Binh Duong | 74 | 7.78 | 7.72–7.84 | 8.55 | 8.46–8.65 | |
| Dong Nai | 75 | 3.94 | 3.89–3.98 | 4.46 | 4.39–4.53 | |
| An Giang | 89 | 2.40 | 2.38–2.43 | 2.54 | 2.48–2.60 | |
| Tay Ninh | 72 | 1.78 | 1.75–1.80 | 2.21 | 2.16–2.26 | |
| Central | Da Nang | 48 | 1.73 | 1.70–1.76 | 1.77 | 1.69–1.85 |
| North | Ha Noi | 01 | 3.63 | 3.43–3.84 | 3.72 | 3.41–4.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mai, N.T.; Tran, G.T.H.; Dang, A.H.; Cao, P.T.B.; Nguyen, T.T.; Pham, H.T.L.; Vu, T.T.T.; Dong, H.V.; Huynh, L.T.M. Comparison of the Basic Reproduction Numbers for COVID-19 through Four Waves of the Pandemic in Vietnam. Int. J. Transl. Med. 2023, 3, 1-11. https://doi.org/10.3390/ijtm3010001
Mai NT, Tran GTH, Dang AH, Cao PTB, Nguyen TT, Pham HTL, Vu TTT, Dong HV, Huynh LTM. Comparison of the Basic Reproduction Numbers for COVID-19 through Four Waves of the Pandemic in Vietnam. International Journal of Translational Medicine. 2023; 3(1):1-11. https://doi.org/10.3390/ijtm3010001
Chicago/Turabian StyleMai, Ngan Thi, Giang Thi Huong Tran, Anh Huu Dang, Phuong Thi Bich Cao, Trung Thanh Nguyen, Huong Thi Lan Pham, Tra Thi Thu Vu, Hieu Van Dong, and Le Thi My Huynh. 2023. "Comparison of the Basic Reproduction Numbers for COVID-19 through Four Waves of the Pandemic in Vietnam" International Journal of Translational Medicine 3, no. 1: 1-11. https://doi.org/10.3390/ijtm3010001