
Efficacy and Safety of Brazilian Green Propolis in Biochemically Recurrent Prostate Cancer after Radical Prostatectomy: A Single-Arm Phase II Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethics Statement
2.2. Patient Population
2.3. Summary of the Study and the Collected Data
2.4. Primary and Secondary Endpoints
2.5. Immunohistochemistry
2.6. Statistical Design and Analyses
3. Results
3.1. Baseline Characteristics of the Patients
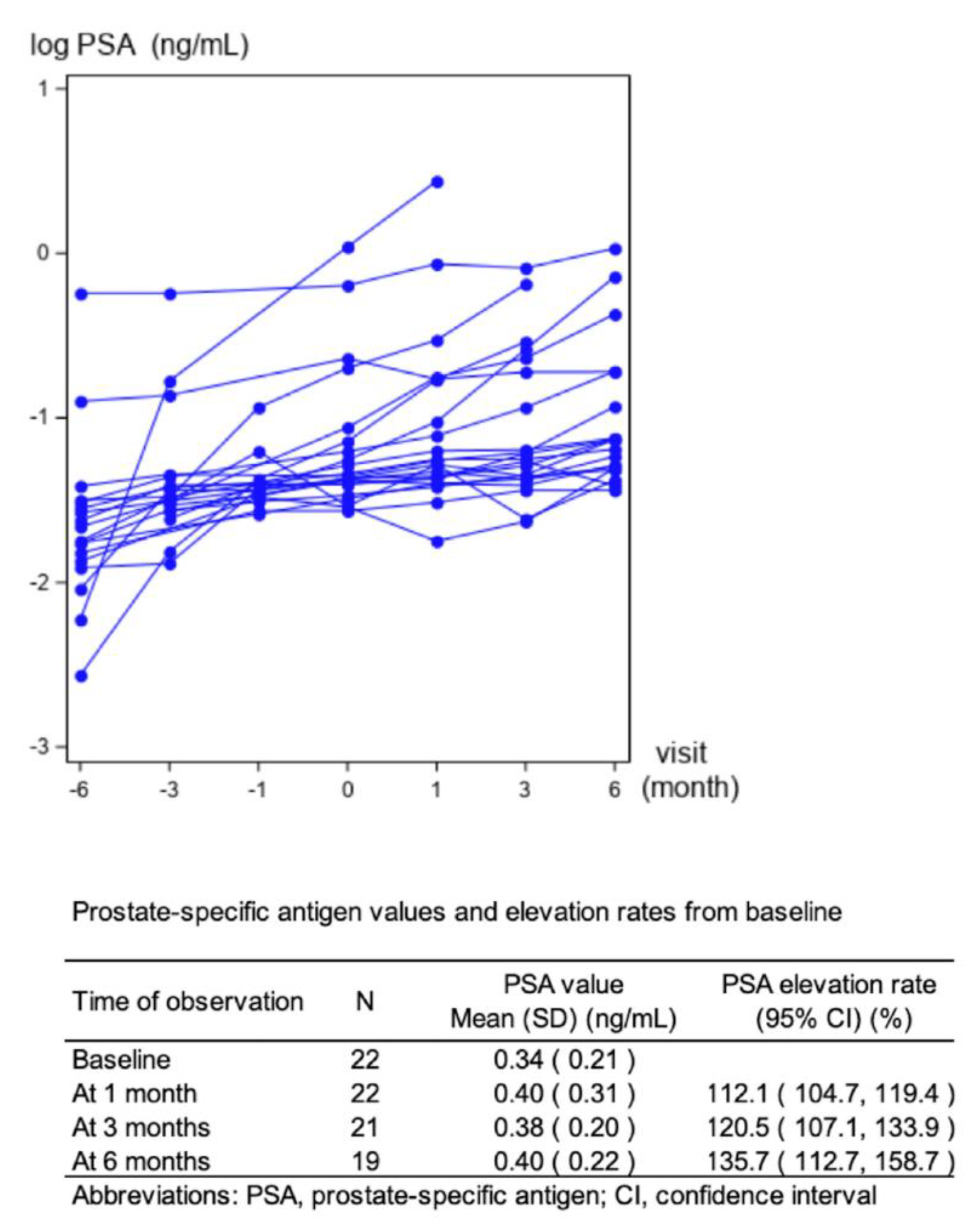
3.2. Therapeutic Effect of Brazilian Green Propolis
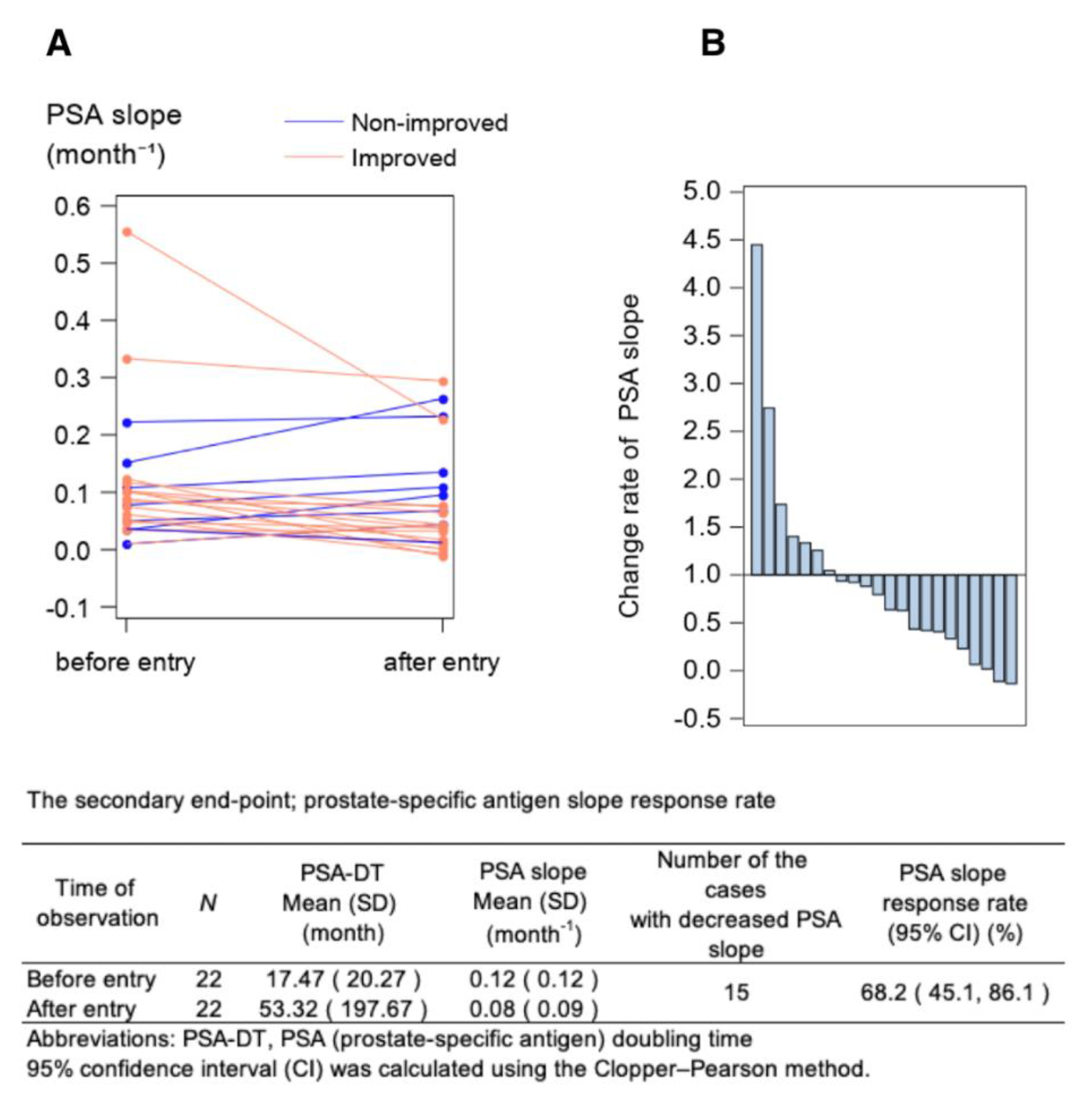
3.3. Impacts on the PSA Slope
3.4. Characteristics of the Two Groups: PSA Slope Ratio < 1 Group and PSA Slope Ratio ≥ 1 Group
3.5. Alteration of Testosterone Values
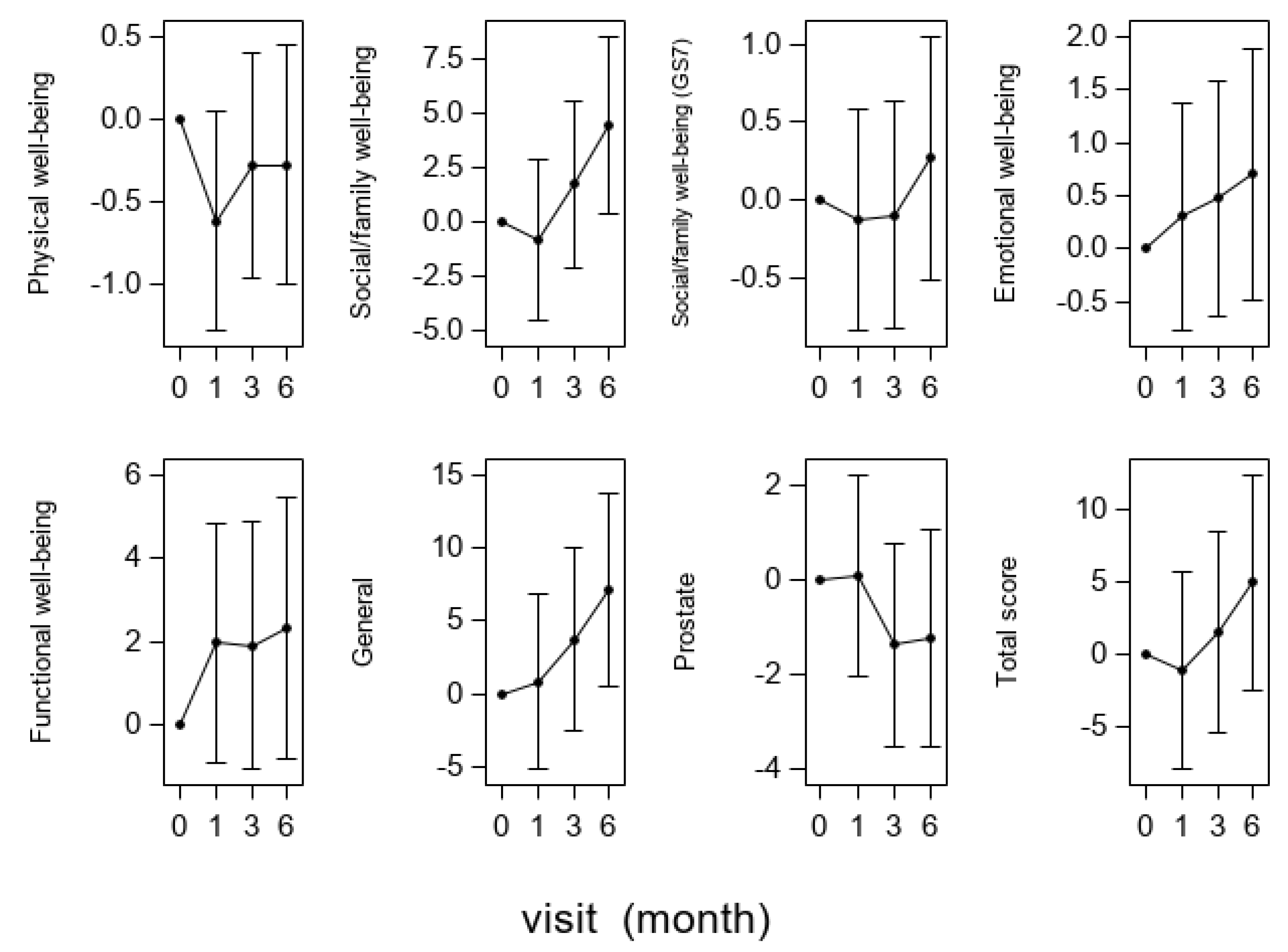
3.6. Effect on PRO
3.7. Safety Profiles of Brazilian Green Propolis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AKR1C3 | Aldo-keto reductase 1C3 |
| AR | Androgen receptor |
| BCR | Biochemical recurrence |
| CAM | Complementary and alternative medicine |
| CI | Confidence interval |
| ERG | Ets-Related Gene |
| FACT-P | Functional Assessment of Cancer Therapy-Prostate |
| PCa | Prostate cancer |
| PG | prostaglandin |
| pGS | Pathological Gleason score |
| PRO | Patient-Reported Outcomes |
| PSA | Prostate-specific antigen |
| PSA-DT | PSA doubling time |
| QOL | Quality of life |
| RP | Radical prostatectomy |
| SR | Salvage radiation |
References
- Djavan, B.; Moul, J.W.; Zlotta, A.; Remzi, M.; Ravery, V. PSA progression following radical prostatectomy and radiation therapy: New standards in the new Millennium. Eur. Urol. 2003, 43, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Simmons, M.N.; Stephenson, A.J.; Klein, E.A. Natural history of biochemical recurrence after radical prostatectomy: Risk assessment for secondary therapy. Eur. Urol. 2007, 51, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Yokomizo, A.; Wakabayashi, M.; Satoh, T.; Hashine, K.; Inoue, T.; Fujimoto, K.; Egawa, S.; Habuchi, T.; Kawashima, K.; Ishizuka, O.; et al. Salvage Radiotherapy Versus Hormone Therapy for Prostate-specific Antigen Failure After Radical Prostatectomy: A Randomised, Multicentre, Open-label, Phase 3 Trial (JCOG0401). Eur. Urol. 2020, 77, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Parker, C.C.; Clarke, N.W.; Cook, A.D.; Kynaston, H.G.; Petersen, P.M.; Catton, C.; Cross, W.; Logue, J.; Parulekar, W.; Payne, H.; et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomised, controlled phase 3 trial. Lancet 2020, 396, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Sargos, P.; Chabaud, S.; Latorzeff, I.; Magné, N.; Benyoucef, A.; Supiot, S.; Pasquier, D.; Abdiche, M.S.; Gilliot, O.; Graff-Cailleaud, P.; et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localised prostate cancer after radical prostatectomy (GETUG-AFU 17): A randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1341–1352. [Google Scholar] [CrossRef]
- Kneebone, A.; Fraser-Browne, C.; Duchesne, G.M.; Fisher, R.; Frydenberg, M.; Herschtal, A.; Williams, S.G.; Brown, C.; Delprado, W.; Haworth, A.; et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020, 21, 1331–1340. [Google Scholar] [CrossRef]
- Pfister, D.; Bolla, M.; Briganti, A.; Carroll, P.; Cozzarini, C.; Joniau, S.; van Poppel, H.; Roach, M.; Stephenson, A.; Wiegel, T.; et al. Early salvage radiotherapy following radical prostatectomy. Eur. Urol. 2014, 65, 1034–1043. [Google Scholar] [CrossRef]
- Van den Bergh, R.C.; van Casteren, N.J.; van den Broeck, T.; Fordyce, E.R.; Gietzmann, W.K.; Stewart, F.; MacLennan, S.; Dabestani, S.; Bellmunt, J.; Bolla, M.; et al. Role of Hormonal Treatment in Prostate Cancer Patients with Nonmetastatic Disease Recurrence After Local Curative Treatment: A Systematic Review. Eur. Urol. 2016, 69, 802–820. [Google Scholar] [CrossRef]
- Harris, P.E.; Cooper, K.L.; Relton, C.; Thomas, K.J. Prevalence of complementary and alternative medicine (CAM) use by the general population: A systematic review and update. Int. J. Clin. Pract. 2012, 66, 924–939. [Google Scholar] [CrossRef]
- Rhee, T.G.; Pawloski, P.A.; Parsons, H.M. Health-related quality of life among US adults with cancer: Potential roles of complementary and alternative medicine for health promotion and well-being. Psychooncology 2019, 28, 896–902. [Google Scholar] [CrossRef]
- Cornara, L.; Biagi, M.; Xiao, J.; Burlando, B. Therapeutic Properties of Bioactive Compounds from Different Honeybee Products. Front. Pharmacol. 2017, 8, 412. [Google Scholar] [CrossRef] [Green Version]
- Burdock, G.A. Review of the biological properties and toxicity of bee propolis (propolis). Food Chem. Toxicol. 1998, 36, 347–363. [Google Scholar] [CrossRef]
- Khalil, M.L. Biological activity of bee propolis in health and disease. Asian Pac. J. Cancer Prev. 2006, 7, 22–31. [Google Scholar]
- Messerli, S.M.; Ahn, M.R.; Kunimasa, K.; Yanagihara, M.; Tatefuji, T.; Hashimoto, K.; Mautner, V.; Uto, Y.; Hori, H.; Kumazawa, S.; et al. Artepillin C (ARC) in Brazilian green propolis selectively blocks oncogenic PAK1 signaling and suppresses the growth of NF tumors in mice. Phytother. Res. 2009, 23, 423–427. [Google Scholar] [CrossRef]
- Akao, Y.; Maruyama, H.; Matsumoto, K.; Ohguchi, K.; Nishizawa, K.; Sakamoto, T.; Araki, Y.; Mishima, S.; Nozawa, Y. Cell growth inhibitory effect of cinnamic acid derivatives from propolis on human tumor cell lines. Biol. Pharm. Bull. 2003, 26, 1057–1059. [Google Scholar] [CrossRef] [Green Version]
- Endo, S.; Matsunaga, T.; Kanamori, A.; Otsuji, Y.; Nagai, H.; Sundaram, K.; El-Kabbani, O.; Toyooka, N.; Ohta, S.; Hara, A. Selective inhibition of human type-5 17β-hydroxysteroid dehydrogenase (AKR1C3) by baccharin, a component of Brazilian propolis. J. Nat. Prod. 2012, 75, 716–721. [Google Scholar] [CrossRef]
- Penning, T.M. Aldo-Keto Reductase (AKR) 1C3 inhibitors: A patent review. Expert Opin. Ther. Pat. 2017, 27, 1329–1340. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Teramoto, Y.; Shibuya, S.; Goto, T.; Okasho, K.; Mizuno, K.; Uegaki, M.; Yoshikawa, T.; Akamatsu, S.; Kobayashi, T.; et al. Consecutive Prostate Cancer Specimens Revealed Increased Aldo–Keto Reductase Family 1 Member C3 Expression with Progression to Castration-Resistant Prostate Cancer. J. Clin. Med. 2019, 8, 601. [Google Scholar] [CrossRef] [Green Version]
- Mishima, S.; Inoh, Y.; Narita, Y.; Ohta, S.; Sakamoto, T.; Araki, Y.; Suzuki, K.M.; Akao, Y.; Nozawa, Y. Identification of caffeoylquinic acid derivatives from Brazilian propolis as constituents involved in induction of granulocytic differentiation of HL-60 cells. Bioorganic Med. Chem. 2005, 13, 5814–5818. [Google Scholar] [CrossRef]
- DCTD; NCI; NIH; DHHS; Cancer Therapy Evaluation Program. Common Toxicity Criteria, Version 2.0; CTEP: Bethesda, MD, USA, 1999. [Google Scholar]
- Esper, P.; Mo, F.; Chodak, G.; Sinner, M.; Cella, D.; Pienta, K.J. Measuring quality of life in men with prostate cancer using the functional assessment of cancer therapy-prostate instrument. Urology 1997, 50, 920–928. [Google Scholar] [CrossRef]
- DCTD; NCI; NIH; DHHS; Cancer Therapy Evaluation Program. Common Toxicity Criteria for Adverse Events, Version 3.0; CTEP: Bethesda, MD, USA, 2006. [Google Scholar]
- Bubley, G.J.; Carducci, M.; Dahut, W.; Dawson, N.; Daliani, D.; Eisenberger, M.; Figg, W.D.; Freidlin, B.; Halabi, S.; Hudes, G.; et al. Eligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: Recommendations from the Prostate-Specific Antigen Working Group. J. Clin. Oncol. 1999, 17, 3461–3467. [Google Scholar] [CrossRef] [PubMed]
- Pound, C.R.; Partin, A.W.; Eisenberger, M.A.; Chan, D.W.; Pearson, J.D.; Walsh, P.C. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999, 281, 1591–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allred, D.C.; Harvey, J.M.; Berardo, M.; Clark, G.M. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod. Pathol. 1998, 11, 155–168. [Google Scholar] [PubMed]
- Fleming, T.R. One-sample multiple testing procedure for phase II clinical trials. Biometrics 1982, 38, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Meijer, D.; Ettema, R.H.; van Leeuwen, P.J.; van der Kwast, T.H.; van der Poel, H.G.; Donswijk, M.L.; Oprea-Lager, D.E.; Bekers, E.M.; Vis, A.N. The prognostic value of lymph node staging with prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography (PET/CT) and extended pelvic lymph node dissection in node-positive patients with prostate cancer. BJU Int. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Claps, F.; Ramírez-Backhaus, M.; Mir Maresma, M.C.; Gómez-Ferrer, Á.; Mascarós, J.M.; Marenco, J.; Collado Serra, A.; Casanova Ramón-Borja, J.; Calatrava Fons, A.; Trombetta, C.; et al. Indocyanine green guidance improves the efficiency of extended pelvic lymph node dissection during laparoscopic radical prostatectomy. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2021, 28, 566–572. [Google Scholar] [CrossRef]
- Claps, F.; de Pablos-Rodríguez, P.; Gómez-Ferrer, Á.; Mascarós, J.M.; Marenco, J.; Collado Serra, A.; Casanova Ramón-Borja, J.; Calatrava Fons, A.; Trombetta, C.; Rubio-Briones, J.; et al. Free-indocyanine green-guided pelvic lymph node dissection during radical prostatectomy. Urol. Oncol. 2022, 40, 489.e19–489.e26. [Google Scholar] [CrossRef]
- Van den Broeck, T.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; Cumberbatch, M.; Tilki, D.; De Santis, M.; Fanti, S.; Fossati, N.; Gillessen, S.; et al. Biochemical Recurrence in Prostate Cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur. Urol. Focus 2020, 6, 231–234. [Google Scholar] [CrossRef]
- Tilki, D.; Preisser, F.; Graefen, M.; Huland, H.; Pompe, R.S. External Validation of the European Association of Urology Biochemical Recurrence Risk Groups to Predict Metastasis and Mortality After Radical Prostatectomy in a European Cohort. Eur. Urol. 2019, 75, 896–900. [Google Scholar] [CrossRef]
- Trock, B.J.; Han, M.; Freedland, S.J.; Humphreys, E.B.; DeWeese, T.L.; Partin, A.W.; Walsh, P.C. Prostate cancer-specific survival following salvage radiotherapy vs observation in men with biochemical recurrence after radical prostatectomy. JAMA 2008, 299, 2760–2769. [Google Scholar] [CrossRef] [Green Version]
- Reese, A.C.; Fradet, V.; Whitson, J.M.; Davis, C.B.; Carroll, P.R. Poor agreement of prostate specific antigen doubling times calculated using ultrasensitive versus standard prostate specific antigen values: Important impact on risk assessment. J. Urol. 2011, 186, 2228–2232. [Google Scholar] [CrossRef]
- Laajala, T.D.; Seikkula, H.; Seyednasrollah, F.; Mirtti, T.; Boström, P.J.; Elo, L.L. Longitudinal modeling of ultrasensitive and traditional prostate-specific antigen and prediction of biochemical recurrence after radical prostatectomy. Sci. Rep. 2016, 6, 36161. [Google Scholar] [CrossRef] [Green Version]
- Endo, S.; Hoshi, M.; Matsunaga, T.; Inoue, T.; Ichihara, K.; Ikari, A. Autophagy inhibition enhances anticancer efficacy of artepillin C, a cinnamic acid derivative in Brazilian green propolis. Biochem. Biophys. Res. Commun. 2018, 497, 437–443. [Google Scholar] [CrossRef]
- Verma, K.; Zang, T.; Gupta, N.; Penning, T.M.; Trippier, P.C. Selective AKR1C3 Inhibitors Potentiate Chemotherapeutic Activity in Multiple Acute Myeloid Leukemia (AML) Cell Lines. ACS Med. Chem. Lett. 2016, 7, 774–779. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Segawa, T.; Shiraishi, T.; Yoshida, T.; Toda, Y.; Yamada, T.; Kinukawa, N.; Kinoshita, H.; Kamoto, T.; Ogawa, O. Androgen receptor, Ki67, and p53 expression in radical prostatectomy specimens predict treatment failure in Japanese population. Urology 2005, 66, 332–337. [Google Scholar] [CrossRef]
- Cella, D.; Nichol, M.B.; Eton, D.; Nelson, J.B.; Mulani, P. Estimating clinically meaningful changes for the Functional Assessment of Cancer Therapy--Prostate: Results from a clinical trial of patients with metastatic hormone-refractory prostate cancer. Value Health 2009, 12, 124–129. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Factor | Group | N = 22 | |
|---|---|---|---|
| Age (year old) | N | 22 | |
| Mean (SD) | 71.0 (5.8) | ||
| BMI (kg/m2) | N | 22 | |
| Mean (SD) | 22.7 (2.6) | ||
| Initial PSA (ng/mL) | N | 22 | |
| Mean (SD) | 9.4 (4.9) | ||
| PSA at study entry (ng/mL) | N | 22 | |
| Mean (SD) | 0.34 (0.21) | ||
| Biopsy Gleason score | N | 22 | |
| 3 + 3 | 5 (22.7%) | ||
| 3 + 4 | 6 (27.3%) | ||
| 4 + 3 | 3 (13.6%) | ||
| 4 + 4 | 6 (27.3%) | ||
| 3 + 5 | 0 (0.0%) | ||
| 4 + 5 | 1 (4.5%) | ||
| 5 + 4 | 1 (4.5%) | ||
| Clinical T stage | N | 22 | |
| T1c | 7 (31.8%) | ||
| T2a | 10 (45.5%) | ||
| T2b | 2 (9.1%) | ||
| T2c | 3 (13.6%) | ||
| Pathological Gleason score * | N | 19 | |
| 3 + 3 | 2 (10.5%) | ||
| 3 + 4 | 10 (52.6%) | ||
| 4 + 3 | 2 (10.5%) | ||
| 4 + 4 | 3 (15.8%) | ||
| 3 + 5 | 1 (5.3%) | ||
| 4 + 5 | 0 (0.0%) | ||
| 5 + 4 | 1 (5.3%) | ||
| Pathological T stage * | N | 19 | |
| T2a | 3 (15.8%) | ||
| T2c | 8 (42.1%) | ||
| T3a | 7 (36.8%) | ||
| T3b | 1 (5.3%) | ||
| Jewett stage | N | 22 | |
| B | 22 (100.0%) | ||
| C-D2 | 0 (0.0%) | ||
| Time to biochemical recurrence after RP (year) | N | 22 | |
| Mean (SD) | 4.2 (2.4) | ||
| Time to green propolis administration after RP (year) | N | 22 | |
| Mean (SD) | 5.2 (2.7) | ||
| Performance status ** | N | 22 | |
| 0 | 22 (100.0%) | ||
| 1–4 | 0 (0.0%) | ||
| Past history | N | 22 | |
| no | 8 (36.4%) | ||
| yes | 14 (63.6%) | ||
| History of previous CAM intake | N | 22 | |
| no | 17 (77.3%) | ||
| yes | 5 (22.7%) | ||
| Blood test value | N | 22 | |
| WBC (×109/L) | Mean (SD) | 5.1 (1.4) | |
| RBC (×1012/L) | Mean (SD) | 4.4 (0.4) | |
| Hb (g/dL) | Mean (SD) | 13.9 (1.2) | |
| PLT (×109/L) | Mean (SD) | 202.5 (41.0) | |
| LDH (U/l) | Mean (SD) | 188.8 (32.9) | |
| ALP (U/l) | Mean (SD) | 215.1 (70.0) | |
| GPT (U/l) | Mean (SD) | 24.5 (13.5) | |
| GOT (U/l) | Mean (SD) | 23.5 (7.7) | |
| Cre (mg/dL) | Mean (SD) | 0.9 (0.2) | |
| BUN (mg/dL) | Mean (SD) | 18.0 (3.3) | |
| Na (mEq/L) | Mean (SD) | 141.0 (1.6) | |
| K (mEq/L) | Mean (SD) | 4.3 (0.3) | |
| Cl (mEq/L) | Mean (SD) | 105.1 (2.3) | |
| T-COL (mg/dL) | Mean (SD) | 184.3 (20.6) | |
| TG (mg/dL) | Mean (SD) | 118.1 (64.8) | |
| Factor | PSA Slope Ratio < 1 | PSA Slope Ratio ≥ 1 | p-Value § | ||
|---|---|---|---|---|---|
| N = 15 | N = 7 | ||||
| Age (year old) | N | 15 | 7 | ||
| Mean (SD) | 69.7 (6.2) | 73.9 (3.7) | 0.12 | ||
| BMI (kg/m2) | N | 15 | 7 | ||
| Mean (SD) | 23.0 (2.5) | 22.2 (2.8) | 0.49 | ||
| Initial PSA (ng/mL) | N | 15 | 7 | ||
| Mean (SD) | 8.5 (4.8) | 11.2 (5.1) | 0.25 | ||
| PSA level at study entry (ng/mL) | N | 15 | 7 | ||
| Mean (SD) | 0.3 (0.2) | 0.4 (0.2) | 0.45 | ||
| Biopsy Gleason score | N | 15 | 7 | ||
| 3 + 3 | 5 (33.3%) | 0 (0.0%) | 0.69 §§ | ||
| 3 + 4 | 2 (13.3%) | 4 (57.1%) | |||
| 4 + 3 | 3 (20.0%) | 0 (0.0%) | |||
| 4 + 4 | 4 (26.7%) | 2 (28.6%) | |||
| 4 + 5 | 0 (0.0%) | 1 (14.3%) | |||
| 5 + 4 | 1 (6.7%) | 0 (0.0%) | |||
| Clinical T stage | N | 15 | 7 | ||
| T1c | 7 (46.7%) | 0 (0.0%) | 0.01 §§ | ||
| T2a | 7 (46.7%) | 3 (42.9%) | |||
| T2b | 0 (0.0%) | 2 (28.6%) | |||
| T2c | 1 (6.7%) | 2 (28.6%) | |||
| Pathological Gleason score * | N | 13 | 6 | ||
| 3 + 3 | 1 (7.7%) | 1 (16.7%) | 1.00 §§ | ||
| 3 + 4 | 7 (53.8%) | 3 (50.0%) | |||
| 4 + 3 | 2 (15.4%) | 0 (0.0%) | |||
| 4 + 4 | 2 (15.4%) | 1 (16.7%) | |||
| 3 + 5 | 0 (0.0%) | 1 (16.7%) | |||
| 5 + 4 | 1 (7.7%) | 0 (0.0%) | |||
| Pathological T stage * | N | 13 | 6 | ||
| T2a | 2 (15.4%) | 1 (16.7%) | 0.67 §§ | ||
| T2c | 7 (53.8%) | 1 (16.7%) | |||
| T3a | 3 (23.1%) | 4 (66.7%) | |||
| T3b | 1 (7.7%) | 0 (0.0%) | |||
| Jewett stage | N | 15 | 7 | ||
| B | 15 (100.0%) | 7 (100.0%) | - | ||
| C-D2 | 0 (0.0%) | 0 (0.0%) | |||
| Time to biochemical recurrence after RP (year) | N | 15 | 7 | ||
| Mean (SD) | 3.5 (2.0) | 5.8 (2.5) | 0.03 | ||
| Time to green propolis administration after RP (year) | N | 15 | 7 | ||
| Mean (SD) | 4.4 (2.2) | 6.9 (3.1) | 0.03 | ||
| Performance status ** | N | 15 | 7 | ||
| 0 | 15 (100.0%) | 7 (100.0%) | - | ||
| 1–4 | 0 (0.0%) | 0 (0.0%) | |||
| Past history | N | 15 | 7 | ||
| no | 6 (40.0%) | 2 (28.6%) | 1.00 | ||
| yes | 9 (60.0%) | 5 (71.4%) | |||
| History of previous CAM intake | N | 15 | 7 | ||
| no | 12 (80.0%) | 5 (71.4%) | 1.00 | ||
| yes | 3 (20.0%) | 2 (28.6%) | |||
| Immunohistochemistry * | N | 13 | 6 | ||
| AKR1C3 | Mean (SD) | 1.8 (2.6) | 4.0 (1.3) | 0.07 | |
| ERG | Mean (SD) | 0.7 (1.8) | 2.2 (3.4) | 0.22 | |
| AR | Mean (SD) | 1.7 (2.0) | 4.2 (2.3) | 0.03 | |
| Blood test value | N | 15 | 7 | ||
| WBC (×109/L) | Mean (SD) | 5(1.5) | 5.3(1.2) | 0.68 | |
| RBC (×1012/L) | Mean (SD) | 4.5 (0.4) | 4.3 (0.6) | 0.52 | |
| Hb (g/dL) | Mean (SD) | 14.0 (1.1) | 13.5 (1.5) | 0.40 | |
| PLT (×109/L) | Mean (SD) | 204.2 (40.5) | 198.9(45.2) | 0.78 | |
| LDH (U/l) | Mean (SD) | 187.7 (32.0) | 191.1(37.3) | 0.82 | |
| ALP (U/l) | Mean (SD) | 219.5 (82.7) | 205.7 (32.0) | 0.68 | |
| GPT (U/l) | Mean (SD) | 26.1(15.3) | 20.9 (8.3) | 0.41 | |
| GOT (U/l) | Mean (SD) | 24.3 (8.2) | 22 (7.1) | 0.54 | |
| Cre (mg/dL) | Mean (SD) | 0.9 (0.2) | 0.8 (0.1) | 0.34 | |
| BUN (mg/dL) | Mean (SD) | 17.9 (3.5) | 18.3(3.1) | 0.79 | |
| Na (mEq/L) | Mean (SD) | 140.8 (1.7) | 141.4(1.4) | 0.41 | |
| K (mEq/L) | Mean (SD) | 4.3 (0.3) | 4.1 (0.3) | 0.21 | |
| Cl (mEq/L) | Mean (SD) | 105.2 (2.5) | 105 (1.9) | 0.85 | |
| T-COL (mg/dL) | Mean (SD) | 181.3 (20.0) | 190.7 (21.9) | 0.33 | |
| TG (mg/dL) | Mean (SD) | 119.1 (65.0) | 115.9(69.4) | 0.92 | |
| Time of Observation | N | Teststerone Level Mean (SD) (ng/dL) | N | Change Rate of Teststerone Level (95% CI) (%) | Number of the Cases with ≥20% Decreased Teststerone Level | Testosterone Response Rate (95% CI) (%) |
|---|---|---|---|---|---|---|
| Baseline | 21 | 414.12 (169.62) | ||||
| At 1 month | 21 | 439.40 (167.01) | 21 | 108.8 (99.4, 118.3) | 3 | 14.3 (3.0, 36.3) |
| At 3 months | 21 | 442.90 (173.14) | 21 | 108.7 (99.8, 117.6) | 1 | 4.8 (0.1, 23.8) |
| At 6 months | 16 | 385.53 (151.01) | 16 | 101.9 (86.1, 117.7) | 5 | 31.3 (11.0, 58.7) |
| Domain | Score Range | Time of Observation | N | Least-Squares Mean | Standard Error | Least-Squares Mean Difference from Baseline | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Total score | 0–156 | Baseline | 19 | 122.13 | 3.52 | ||||
| At 1 month | 22 | 120.99 | 3.52 | −1.14 (−8.01, 5.74) | 0.74 | ||||
| At 3 months | 20 | 123.62 | 3.58 | 1.49 (−5.50, 8.49) | 0.67 | ||||
| At 6 months | 17 | 127.07 | 3.80 | 4.94 (−2.50, 12.37) | 0.19 | ||||
| G (general) | 0-108 | Baseline | 20 | 85.02 | 2.76 | ||||
| At 1 month | 22 | 85.84 | 2.76 | 0.82 (−5.19, 6.82) | 0.79 | ||||
| At 3 months | 20 | 88.77 | 2.87 | 3.75 (−2.46, 9.96) | 0.23 | ||||
| At 6 months | 17 | 92.12 | 3.08 | 7.10 (0.49, 13.7) | 0.04 | ||||
| Physical well-being | 0–28 | Baseline | 20 | 26.60 | 0.26 | ||||
| At 1 month | 22 | 25.98 | 0.26 | −0.63 (−1.29, 0.04) | 0.07 | ||||
| At 3 months | 20 | 26.32 | 0.27 | −0.28 (−0.97, 0.41) | 0.42 | ||||
| At 6 months | 17 | 26.32 | 0.30 | −0.28 (−1.01, 0.45) | 0.44 | ||||
| Social/family well-being | 0–32 | Baseline | 20 | 19.63 | 1.58 | ||||
| At 1 month | 22 | 18.81 | 1.58 | −0.82 (−4.51, 2.88) | 0.66 | ||||
| At 3 months | 20 | 21.37 | 1.65 | 1.75 (−2.08, 5.57) | 0.36 | ||||
| At 6 months | 17 | 24.06 | 1.78 | 4.43 (0.37, 8.48) | 0.03 | ||||
| Social/family well-being | (0–4) | Baseline | 15 | 1.05 | 0.28 | ||||
| (Answer is optional) | At 1 month | 17 | 0.92 | 0.30 | −0.13 (−0.85, 0.58) | 0.70 | |||
| At 3 months | 14 | 0.95 | 0.31 | −0.10 (−0.83, 0.63) | 0.78 | ||||
| At 6 months | 11 | 1.32 | 0.34 | 0.26 (−0.52, 1.05) | 0.50 | ||||
| Emotional well-being | 0–24 | Baseline | 20 | 18.71 | 0.46 | ||||
| At 1 month | 22 | 19.01 | 0.46 | 0.30 (−0.78, 1.38) | 0.58 | ||||
| At 3 months | 20 | 19.18 | 0.48 | 0.48 (−0.64, 1.59) | 0.40 | ||||
| At 6 months | 17 | 19.41 | 0.52 | 0.70 (−0.48, 1.88) | 0.24 | ||||
| Functional well-being | 0–28 | Baseline | 20 | 20.02 | 1.22 | ||||
| At 1 month | 22 | 21.98 | 1.22 | 1.96 (−0.92, 4.83) | 0.18 | ||||
| At 3 months | 20 | 21.91 | 1.27 | 1.89 (−1.08, 4.86) | 0.21 | ||||
| At 6 months | 17 | 22.33 | 1.38 | 2.32 (−0.84, 5.47) | 0.15 | ||||
| P (prostate) | 0–48 | Baseline | 19 | 35.74 | 1.08 | ||||
| At 1 month | 22 | 35.85 | 1.08 | 0.11 (−2.01, 2.23) | 0.92 | ||||
| At 3 months | 20 | 34.37 | 1.09 | −1.36 (−3.52, 0.79) | 0.21 | ||||
| At 6 months | 17 | 34.52 | 1.16 | −1.22 (−3.51, 1.08) | 0.29 | ||||
| Category | Grade1 | Grade2 | Grade3 | Grade4 | Total |
|---|---|---|---|---|---|
| N | N | N | N | N (%) | |
| Diarrhea | 4 | 4 (18.2) | |||
| Constipation | 1 | 1 (4.5) | |||
| Anorexia | 1 | 1 (4.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goto, T.; Kimura, H.; Yoshino, T.; Sawada, A.; Akamatsu, S.; Kobayashi, T.; Yamasaki, T.; Tazawa, S.; Fujimoto, M.; Hidaka, Y.; et al. Efficacy and Safety of Brazilian Green Propolis in Biochemically Recurrent Prostate Cancer after Radical Prostatectomy: A Single-Arm Phase II Study. Int. J. Transl. Med. 2022, 2, 618-632. https://doi.org/10.3390/ijtm2040047
Goto T, Kimura H, Yoshino T, Sawada A, Akamatsu S, Kobayashi T, Yamasaki T, Tazawa S, Fujimoto M, Hidaka Y, et al. Efficacy and Safety of Brazilian Green Propolis in Biochemically Recurrent Prostate Cancer after Radical Prostatectomy: A Single-Arm Phase II Study. International Journal of Translational Medicine. 2022; 2(4):618-632. https://doi.org/10.3390/ijtm2040047
Chicago/Turabian StyleGoto, Takayuki, Hiroko Kimura, Takayuki Yoshino, Atsuro Sawada, Shusuke Akamatsu, Takashi Kobayashi, Toshinari Yamasaki, Shigemi Tazawa, Masakazu Fujimoto, Yu Hidaka, and et al. 2022. "Efficacy and Safety of Brazilian Green Propolis in Biochemically Recurrent Prostate Cancer after Radical Prostatectomy: A Single-Arm Phase II Study" International Journal of Translational Medicine 2, no. 4: 618-632. https://doi.org/10.3390/ijtm2040047