

Cognitive Predictors of Posttraumatic Stress in Children 6 Months after Paediatric Intensive Care Unit Admission

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Setting
2.2. Measures
2.2.1. Premorbid and Trauma Characteristics
2.2.2. PTSS and PTSD
2.2.3. Cognitive Variables
Peri-Trauma Affect
Peri-Trauma Cognitive Processing
Acute Trauma Memory
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Demographics
3.2. Predictors of PTSS at 6 Months
3.3. Predictors of PTSD-AA
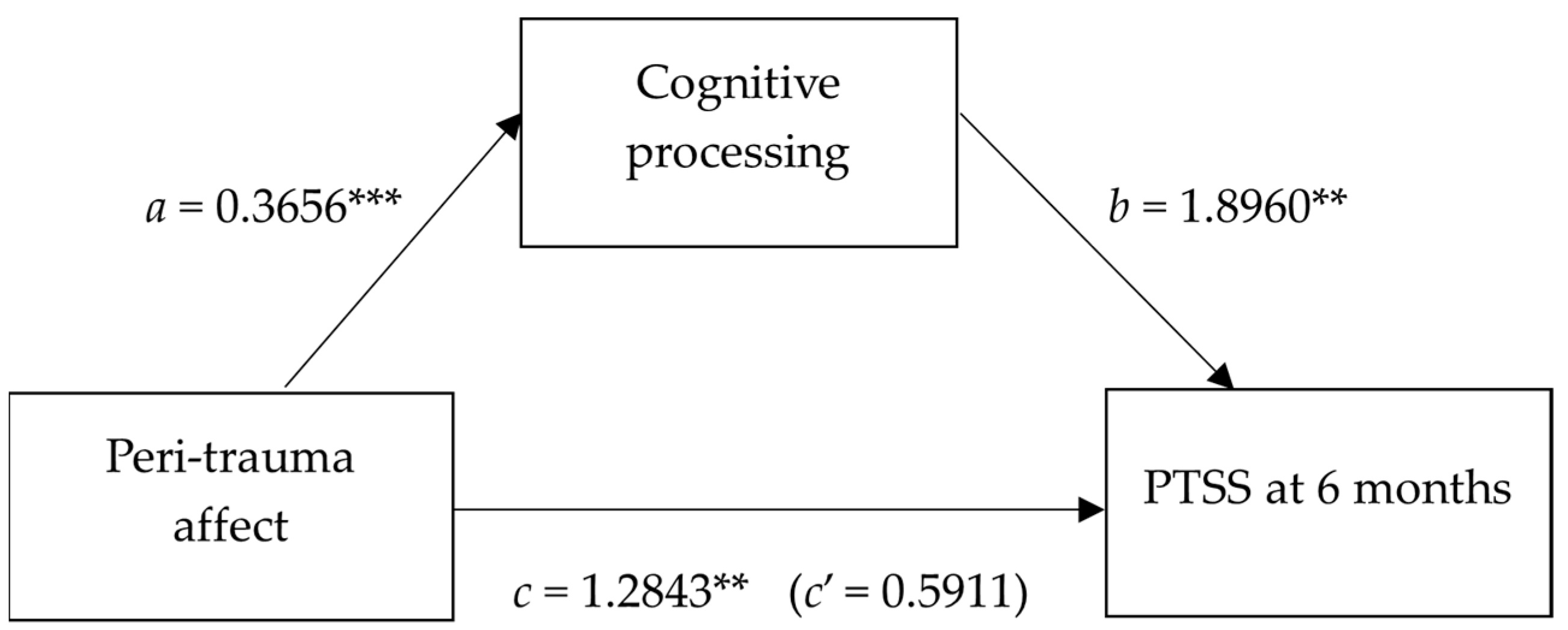
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian and New Zealand Paediatric Intensive Care Registry. ANZICS Centre for Outcome and Resource Evaluation 2020 Report Melbourne, Australia. 2020. Available online: https://www.anzics.com.au/australian-and-new-zealand-paediatric-intensive-care-registry-anzpicr/ (accessed on 22 March 2023).
- Dow, B.L.; Kenardy, J.; Le Brocque, R.; Long, D. Brief Report: The utility of the Children’s Revised Impact of Event Scale in screening for Posttraumatic Stress Disorder in children following admission to Intensive Care. J. Trauma. Stress 2012, 25, 602–605. [Google Scholar] [CrossRef]
- Landolt, M.A.; Buehlmann, C.; Maag, T.; Schiestl, C. Brief Report: Quality of life is impaired in pediatric burn survivors with posttraumatic stress disorder. J. Pediatr. Psychol. 2009, 34, 14–21. [Google Scholar] [CrossRef]
- Seng, J.S.; Graham-Bermann, S.A.; Clark, C.R.; McCarthy, A.M.; Ronis, D.L. Posttraumatic stress disorder and physical comorbidity among female children and adolescents: Results from service-use data. Pediatrics 2005, 116, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Zatzick, D.F.; Jurkovich, G.J.; Fan, M.Y.; Grossman, D.; Russo, J.; Katon, W.; Rivara, F.P. Association between posttraumatic stress and depressive symptoms and functional outcomes in adolescents followed up longitudinally after injury hospitalization. Arch. Pediatr. Adolesc. Med. 2008, 162, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Shears, D.; Nadel, S.; Gledhill, J.; Garralda, M.E. Short-term psychiatric adjustment of children and their parents following meningoccal disease. Pediatr. Crit. Care Med. 2005, 6, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Colville, G.; Kerry, S.; Pierce, C. Children’s factual and delusional memories of Intensive Care. Am. J. Respir. Crit. Care Med. 2008, 177, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Bronner, M.B.; Knoester, H.; Bos, A.P.; Last, B.F.; Grootenhuis, M.A. Follow-up after paediatric intensive care treatment: Parental posttraumatic stress. Acta Paediatr. 2008, 97, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Rees, G.; Gledhill, J.; Garralda, M.E.; Nadel, S. Psychiatric outcome following paediatric intensive care unit (PICU) admission: A cohort study. Intensive Care Med. 2004, 30, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Dow, B.; Kenardy, J.; Long, D.; Le Brocque, R. Children’s post-traumatic stress and the role of memory following admission to intensive care: A review. Clin. Psychol. 2012, 16, 1–14. [Google Scholar] [CrossRef]
- Rennick, J.E.; Johnston, C.C.; Dougherty, G.; Platt, R.; Ritchie, J.A. Children’s psychological responses after critical illness and exposure to invasive technology. J. Dev. Behav. Pediatr. JDBP 2002, 23, 133–144. [Google Scholar] [CrossRef]
- Ehlers, A.; Clark, D.M. A cognitive model of posttraumatic stress disorder. Behav. Res. Ther. 2000, 38, 319–345. [Google Scholar] [CrossRef]
- Marsac, M.L.; Kassam-Adams, N.; Delahanty, D.L.; Widaman, K.; Barakat, L.P. Posttraumatic stress following acute medical trauma in children: A proposed model of bio-psycho-social processes during the peri-trauma period. Clin. Child Fam. Psychol. Rev. 2014, 17, 399–411. [Google Scholar] [CrossRef]
- Meiser-Stedman, R. Towards a cognitive-behavioral model of PTSD in children and adolescents. Clin. Child Fam. Psychol. Rev. 2002, 5, 217–232. [Google Scholar] [CrossRef] [PubMed]
- Kassam-Adams, N.; Winston, F. Predicting Child PTSD: The relationship between Acute Stress Disorder and PTSD in injured children. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Meiser-Stedman, R.; Dalgleish, T.; Smith, P.; Yule, W.; Glucksman, E. Diagnostic, demographic, memory quality, and cognitive variables associated with acute stress disorder in children and adolescents. J. Abnorm. Psychol. 2007, 116, 65–79. [Google Scholar] [CrossRef]
- McKinnon, A.C.; Nixon, R.D.V.; Brewer, N. The influence of data-driven processing on perceptions of memory quality and intrusive symptoms in children following traumatic events. Behav. Res. Ther. 2008, 46, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, A.; Mayou, R.A.; Bryant, B. Cognitive predictors of posttraumatic stress disorder in children: Results of a prospective longitudinal study. Behav. Res. Ther. 2003, 41, 1–10. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, A.; Brewer, N.; Cameron, K.; Nixon, R.D.V. The relationship between processing style, trauma memory processes, and the development of posttraumatic stress symptoms in children and adolescents. J. Behav. Ther. Exp. Psychiatry 2017, 57, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Dow, B.L.; Kenardy, J.A.; Long, D.A.; Le Brocque, R.M. Cognitive/Affective Factors are Associated with Children’s Acute Posttraumatic Stress Following Pediatric Intensive Care. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 55–63. [Google Scholar] [CrossRef]
- Smith, P.; Perrin, S.; Dyregrov, A.; Yule, W. Principal components analysis of the Impact of Event Scale with children in war. Personal. Individ. Differ. 2003, 34, 315–322. [Google Scholar] [CrossRef]
- Giannopoulou, I.; Smith, P.; Ecker, C.; Strouthos, M.; Dikaiakou, A.; Yule, W. Factor structure of the Children’s Revised Impact of Event Scale (CRIES) with children exposed to earthquake. Personal. Individ. Differ. 2006, 40, 1027–1037. [Google Scholar] [CrossRef]
- Saigh, P.A.; Yasik, A.E.; Oberfield, R.A.; Green, B.L.; Halamandaris, P.V.; Rubenstein, H.; Nester, J.; Resko, J.; Hetz, B.; McHugh, M. The Children’s PTSD Inventory: Development and reliability. J. Trauma. Stress 2000, 13, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Yasik, A.E.; Saigh, P.A.; Oberfield, R.A.; Green, B.; Halamandaris, P.; McHugh, M. The validity of the Children’s PTSD Inventory. J. Trauma. Stress 2001, 14, 81–94. [Google Scholar] [CrossRef]
- Scheeringa, M.S.; Wright, M.J.; Hunt, J.P.; Zeanah, C.H. Factors affecting the diagnosis and prediction of PTSD symptomatology in children and adolescents. Am. J. Psychiatry 2006, 163, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Dow, B.L.; Kenardy, J.A.; Le Brocque, R.M.; Long, D.A. The Diagnosis of Posttraumatic Stress Disorder in School-Aged Children and Adolescents Following Pediatric Intensive Care Unit Admission. J. Child Adolesc. Psychopharmacol. 2013, 23, 614–619. [Google Scholar] [CrossRef]
- Jones, C.; Humphris, G.; Griffiths, R.D. Preliminary validation of the ICUM Tool: A tool for assessing memory of the intensive care experience. Clin. Intensive Care 2000, 11, 252–255. [Google Scholar]
- Meiser-Stedman, R.; Smith, P.; Yule, W.; Dalgleish, T. The Trauma Memory Quality Questionnaire: Preliminary development and validation of a measure of trauma memory characteristics for children and adolescents. Memory 2007, 15, 271–279. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Pai, A.; Heining, M. Ketamine. Continuing Education in Anaesthesia. Crit. Care Pain 2007, 7, 59–63. [Google Scholar]
- Le Brocque, R.M.; Hendrikz, J.; Kenardy, J.A. The course of posttraumatic stress in children: Examination of recovery trajectories following traumatic injury. J. Pediatr. Psychol. 2010, 35, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Trickey, D.; Siddaway, A.; Meiser-Stedman, R.; Serpell, L.; Field, A. A meta-analysis of risk factors for post-traumatic stress disorder in children and adolescents. Clin. Psychol. Rev. 2012, 32, 122–138. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, L.; Böhringer, A.; Wolf, O.T. Stress disrupts context-dependent memory. Learn. Mem. 2009, 16, 110–113. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n (%) | M (SD) |
|---|---|---|
| Age, years | 10.78 (2.65) | |
| Gender, male | 32 (58%) | |
| Family of origin, both biological parents a | 38 (69%) | |
| Participating parent’s highest level of education a | ||
| Did not complete high school | 6 (11%) | |
| Completed high school | 7 (13%) | |
| College certificate | 16 (29%) | |
| University degree | 19 (35%) | |
| Prior trauma exposure a (# of traumas) | 1.39 (1.42) | |
| Premorbid behavioural problems a | 5 (11%) | |
| Length of stay in PICU > 48 h | 12 (22%) | |
| PIM2 Risk of Mortality | 1.81 (2.55) | |
| Mechanically ventilated | 16 (29%) | |
| Reason for admission | ||
| Post-operative care | 22 (40%) | |
| Traumatic Injury | 13 (24%) | |
| Respiratory | 6 (11%) | |
| Other | 14 (25%) | |
| Admission status, elective | 21 (38%) | |
| Number of invasive procedures | 4.98 (4.98) | |
| Received therapeutic agents | ||
| Midazolam | 13 (24%) | |
| Morphine | 28 (51%) | |
| Propofol | 9 (16%) | |
| Ketamine | 13 (24%) | |
| Other patient death during admission | 5 (9%) | |
| Exposed to distressing event in PICU a | 3 (6%) | |
| Acute PTSS (>30 = elevated) | 19.87 (18.00) | |
| Peri-trauma affect | ||
| Peri-trauma fear | 21 (38%) | |
| Peri-trauma panic | 19 (35%) | |
| Peri-trauma sadness | 21 (38%) | |
| Cognitive variables | ||
| Confusion | 27 (49%) | |
| Delusional experiences | 28 (51%) | |
| Total PICU recall | 1.91 (1.09) | |
| Sensory memory quality | 23.75 (5.58) |
| Variables | PTSS at 6 Months | PTDS-AA Positive |
|---|---|---|
| Premorbid factors | ||
| Age | 0.02 | −0.05 |
| Gender | 0.08 | 0.11 |
| Prior trauma exposure a | 0.15 | −0.04 |
| Premorbid behavioural problems a | 0.23 | 0.09 |
| Trauma characteristics | ||
| Disease-related | ||
| Length of stay in PICU > 48 h | 0.02 | 0.05 |
| PIM2 Risk of death | 0.05 | 0.06 |
| Admission for traumatic injury | 0.01 | 0.02 |
| Treatment-related | ||
| Number of invasive procedures | 0.12 | 0.16 |
| Mechanically ventilated | 0.12 | 0.03 |
| Intubated | 0.08 | 0.01 |
| Therapeutic agents | ||
| Midazolam | 0.12 | 0.12 |
| Morphine | 0.22 | 0.23 |
| Propofol | 0.06 | 0.04 |
| Ketamine | 0.33 * | 0.21 |
| Environment-related | ||
| Other patient death during admission | 0.01 | 0.08 |
| Exposed to distressing event in PICU a | 0.03 | 0.05 |
| Peri-trauma affect | ||
| Peri-trauma fear | 0.28 * | 0.24 |
| Peri-trauma panic | 0.47 *** | 0.38 ** |
| Peri-trauma sadness | 0.27 * | 0.24 |
| Cognitive variables | ||
| Peri-trauma cognitive processing | ||
| Confusion | 0.45 ** | 0.33 * |
| Delusional experiences | 0.47 *** | 0.38 ** |
| Acute trauma memory | ||
| Total PICU recall | −0.13 | 0.02 |
| Sensory memory quality | 0.42 ** | 0.38 ** |
| Variables | Acute PTSS | Peri-Trauma Fear | Peri-Trauma Panic | Peri-Trauma Sadness | Confusion | Peri-Trauma Delusions | Acute Sensory Memory Quality |
|---|---|---|---|---|---|---|---|
| Ketamine | −0.062 | −0.085 | 0.046 | −0.173 | 0.139 | 0.094 | −0.052 |
| Acute PTSS | - | 0.195 | 0.368 ** | 0.213 | 0.356 ** | 0.299 * | 0.437 *** |
| Peri-trauma fear | - | - | 0.452 *** | 0.461 *** | 0.501 *** | 0.260 | 0.077 |
| Peri-trauma panic | - | - | - | 0.531 *** | 0.204 | 0.412 ** | 0.359 ** |
| Peri-trauma sadness | - | - | - | - | 0.201 | 0.485 *** | 0.314 * |
| Confusion | - | - | - | - | - | 0.345 * | 0.157 |
| Peri-trauma delusions | - | - | - | - | - | - | 0.240 |
| B | SE B | β | R2 | ∆R2 | |
|---|---|---|---|---|---|
| Step 1 | 0.21 *** | 0.21 *** | |||
| Acute PTSS | 0.13 | 0.04 | 0.46 *** | ||
| Step 2 | 0.34 *** | 0.13 ** | |||
| Acute PTSS | 0.14 | 0.03 | 0.48 *** | ||
| Ketamine | 3.04 | 0.95 | 0.36 ** | ||
| Step 3 | 0.55 *** | 0.21 *** | |||
| Acute PTSS | 0.07 | 0.03 | 0.23 * | ||
| Ketamine | 2.81 | 0.83 | 0.33 ** | ||
| Peri-trauma affect | 0.41 | 0.36 | 0.14 | ||
| Peri-trauma cognitive processing | 1.39 | 0.49 | 0.33 ** | ||
| Acute sensory memory quality | 0.16 | 0.07 | 0.24 * |
| Independent Variables | B | SE B | OR | 95% CI for OR | χ2 STEP | χ2 MODEL | Correctly Classified | Cox & Snell R2 | Negelkerke R2 |
|---|---|---|---|---|---|---|---|---|---|
| Step 1 | 5.30 * | 5.30 * | 71% | 0.10 | 0.10 | ||||
| Acute PTSS | 0.06 | 0.03 | 1.06 * | 1.01–1.11 | |||||
| Step 2 | 3.22 (*) | 8.53 * | 78% | 0.14 | 0.14 | ||||
| Acute PTSS | 0.06 | 0.03 | 1.07 * | 1.01–1.13 | |||||
| Ketamine | 1.30 | 0.73 | 3.65 (*) | 0.88–15.23 | |||||
| Step 3 | 10.31 * | 18.84 ** | 80% | 0.29 | 0.29 | ||||
| Acute PTSS | 0.02 | 0.04 | 1.02 | 0.95–1.10 | |||||
| Ketamine | 1.32 | 0.86 | 3.74 | 0.69–20.33 | |||||
| Peri-trauma affect | 0.26 | 0.35 | 1.30 | 0.65–2.58 | |||||
| Peri-trauma cognitive processing | 0.83 | 0.51 | 2.30 | 0.84–6.29 | |||||
| Acute sensory memory quality | 0.13 | 0.08 | 1.14 | 0.97–1.32 |
| Antecedent | Consequent | |||||||
|---|---|---|---|---|---|---|---|---|
| Cognitive Processing | PTSS at 6 Months | |||||||
| Coeff. | SE | p | Coeff. | SE | p | |||
| Peri-trauma affect | a | 0.3656 | 0.0844 | 0.0001 | c’ | 0.5911 | 0.4070 | 0.152 |
| Cognitive processing | - | - | - | b | 1.8960 | 0.5690 | 0.002 | |
| Constant | iM | 0.5036 | 0.1362 | <0.001 | iY | 2.4935 | 0.6327 | <0.001 |
| R2 = 0.2613 | R2 = 0.3210 | |||||||
| F (1, 53) = 18.74, p < 0.001 | F (2, 52) = 12.29, p < 0.001 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dow, B.L.; Kenardy, J.A.; Le Brocque, R.M.; Long, D.A. Cognitive Predictors of Posttraumatic Stress in Children 6 Months after Paediatric Intensive Care Unit Admission. Trauma Care 2023, 3, 82-92. https://doi.org/10.3390/traumacare3020009
Dow BL, Kenardy JA, Le Brocque RM, Long DA. Cognitive Predictors of Posttraumatic Stress in Children 6 Months after Paediatric Intensive Care Unit Admission. Trauma Care. 2023; 3(2):82-92. https://doi.org/10.3390/traumacare3020009
Chicago/Turabian StyleDow, Belinda L., Justin A. Kenardy, Robyne M. Le Brocque, and Debbie A. Long. 2023. "Cognitive Predictors of Posttraumatic Stress in Children 6 Months after Paediatric Intensive Care Unit Admission" Trauma Care 3, no. 2: 82-92. https://doi.org/10.3390/traumacare3020009