
Does Blast Mild Traumatic Brain Injury Have an Impact on PTSD Severity? A Systematic Review and Meta-Analysis



1
Institute of Inflammation and Ageing, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK
2
Centre for Trauma Sciences Research, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK
*
Author to whom correspondence should be addressed.
Trauma Care 2023, 3(1), 9-21; https://doi.org/10.3390/traumacare3010002
Submission received: 7 October 2022
/
Revised: 28 December 2022
/
Accepted: 29 December 2022
/
Published: 8 January 2023
Abstract
:Blast mild traumatic brain injury (mTBI) is a unique injury in the military population and post-traumatic stress disorder (PTSD) is shown to be linked with it. The main purpose of the systematic review was to understand the impact of blast mTBI on PTSD symptom severity. We systematically searched Pubmed, Web of Science, Embase (Ovid), APAPsycINFO (Ovid) and Medline (R) and In-Process, In-Data-Review and Other Non-Indexed Citations (Ovid). Data extraction and quality assessment was completed using the AXIS tool. Statistical analysis was undertaken to determine differences between blast mTBI and the control group (no blast and no TBI in military personnel) and a meta-analysis using the random effects model was used to calculate between-study heterogeneity and variance through I2 and Tau2, respectively. Additionally, the likelihood of PTSD, analysed using the average PTSD Checklist (PCL) score, was also determined based. Statistically higher PCL scores were found in the blast mTBI group compared to control groups, but high heterogeneity was found between the studies (p < 0.001, I2 = 84%, Tau2 = 0.44). Furthermore, all studies reported that blast mTBI had probable PTSD, but this was not the case for the control group. Blast mTBI appears to impact on PTSD symptom severity and the likelihood of developing PTSD, which healthcare professionals need to be aware of. The high heterogeneity present in the studies means that caution must be exercised when interpreting the data from this study. However, future studies require more well-defined, high-quality studies to answer the question of how blast mTBI affects PTSD symptom severity.
1. Introduction
Military personnel are considerably more at risk of injury compared with civilians especially those deployed to areas of conflict such as Afghanistan, Iraq and Ukraine. A traumatic brain injury (TBI) is an acquired brain injury where a force is applied to the brain causing reversible or irreversible damage to white matter structures. Mild, moderate and severe are the three classifications of TBI with mild being the most common form. A mild TBI (mTBI) can be diagnosed by a loss of consciousness for less than 30 min, suffering post-traumatic amnesia for less than 24 h and a Glasgow Coma scale score between 13–15 [1]. In the military environment, mTBI has been dubbed the signature wound of war, where 82.3% of service members suffering with TBI were classified with mTBI [2,3]. The high prevalence of mTBI in the military community suggests a population demographic which could benefit from further investigation especially with the variety of causative injury mechanisms [4].
Direct contact blast can cause a plethora of injury presentations to the military personnel such as burns from explosions, shrapnel from explosive devices or debris contributing to penetrating and blunt trauma and force from the blast wave. Even when not in direct contact with a blast, overpressure can still cause considerable trauma to the body and brain. The effects of blasts on the brain vary but factors that normally influence TBI are blast energy, distance from explosion, body position and the protection worn [5]. Blast TBI occurs due to the differences in tissue density in the head, resulting in an acoustic impedance mismatch as the blast wave passes through the head to cause mechanical disruption to the tissue [6]. One model of blast TBI showed this impedance to create a change in intracranial pressure forming cavitations and penetrations in the brain tissue, causing damage to brain structures [7]. Therefore, with indirect contact to the blast there is still risk of military personnel developing mTBI from a blast. This unique injury mechanism can cause many physical (e.g., fatigue, seizures), cognitive (e.g., concentration) and psychological problems developing as a consequence of mTBI which healthcare professionals have to manage.
The military environment is a highly stressful and traumatic setting for veterans, especially when deployed to warzones due to the variety of psychological and physical trauma one may experience or observe compared to the civilian environment [8]. A survey identified that 75% of U.S. veterans and active service members experienced post-traumatic stress disorder (PTSD) in the year 2021 [9]. This shows psychological impairments to be a huge concern for healthcare practitioners dealing with the military population. Psychological impairments such as anxiety disorders and depression following mTBI are also common. U.S. military personnel were shown to have a rate of 47.8% PTSD diagnosis and a rate of 34% depression diagnosis following mTBI, indicating the high comorbidity PTSD plays within mTBI [10].
Blast related mTBI results in elevated rates of psychiatric diagnosis compared to those who experienced mTBI through other means [11]. This is supported by a systematic review that identified PTSD to be the highest comorbidity to blast mTBI further highlighting the relationship between PTSD and blast mTBI [12]. Blast mTBI appears to impact psychological impairments (e.g., PTSD) more in military personnel than the general population suffering mTBI, potentially due to the higher stress levels and traumatic environments accompanied with blasts that military personnel experience. Further to this, blasts could increase PTSD severity due to the stressful environment that ensues and thus prompting investigation into blast mTBI’s effect on PTSD severity. The PTSD Checklist (PCL), PCL-5 (or DSM-5) is a 20 item self-report measure that enables the measurement of PTSD symptom severity and has a pooled positive predictive value of 72% [13]. PCL for DSM-IV which has been updated by DSM-V has three versions of the PCL are: PCL-M for stressful military experiences, PCL-C for general stressful experiences and PCL-S (most similar to DSM-V) for specific events and evidence shows that evaluation and comparison of PTSD through PCL can be achieved regardless of the version in military population [14,15].
The main aim of this paper was to understand the impact of blast mTBI on PTSD symptom severity, achieved through a systematic review and meta-analysis of relevant literature and by comparing PCL scores of blast mTBI groups with no history of blast or TBI groups in military populations. The intention of this study was to increase psychological awareness, in the form of PTSD symptom severity understanding, of healthcare clinicians to aid management decisions when dealing with blast mTBI military personnel as comorbid TBI and PTSD patients normally have worse clinical outcomes [16]. Secondly, by using the discovered paper’s average PCL score, the likelihood of having PTSD was also observed to ascertain PTSD prevalence amongst blast mTBI veterans.
2. Materials and Methods
2.1. Literature Search
The search strategy recommended by the Preferred Reporting Items for systematic reviews and Meta-Analyses (PRISMA) statement [17] was utilised for the creation of this systematic review. The databases that were used to conduct the search were: Pubmed, Web of Science, Embase (Ovid), APAPsycINFO (Ovid) and Medline (R) and In-Process, In-Data-Review and Other Non-Indexed Citations (Ovid), where searches were conducted on the 20th of July 2022. These databases were viewed to be the optimal search database with APAPychinfo providing specialized psychiatric content relevant to PTSD [18]. The search terms were used with Boolean operators and consisted of (“PTSD” OR “post-traumatic stress disorder”) AND (“TBI” OR “traumatic brain injury”) AND “military” AND “blast” AND “adult” were applied to each database. The terms were applied to all fields to enable a wider range of articles to be identified. Furthermore, a screen of article’s references was also performed.
2.2. Inclusion and Exclusion Criteria
The studies were included if: it was in English, contained PCL outcome measure for PTSD, participants had blast mTBI, veterans or service members as participants, article published within the last 10 years, observational study, included a comparison group who experienced no lifetime blast or TBI. Studies were excluded based on the criteria of being a systematic review, conference papers, letters, case reports, only abstracts contained, unable to access the full article, not in English, article older than 10 years. Articles were excluded if participants were animals, civilians, diagnosed with neuropsychiatric disorders other than PTSD (e.g., Parkinson’s, stroke, schizophrenia as this could affect results), a known PTSD diagnosis pre-study (as including this could skew results and analysis or this review), penetrating head injury, if comparison control group had experienced lifetime TBI or blast, individuals aged 18 years old or younger, diagnosis of moderate or severe TBI and blast mTBI not diagnosed via healthcare professional. Finally, articles were excluded if there was no mention of PCL measure, treatment intervention involved and no cross-sectional analysis of PCL at start of study.
2.3. Data Collection
Articles found in the literature search were exported to Microsoft Excel where they were compiled and underwent screening. The title and abstracts were screened by two authors independently (Z.A. and R.B.) and any differences were resolved via discussion. Appropriate studies were then passed for a full text review in which eligible articles in line with the exclusion and inclusion criteria were derived.
2.4. Data Extraction
The following data were extracted from eligible articles: study design; number of participants; participant groupings, PCL version used; PCL mean and standard deviation for blast mTBI group and the control group; p values to determine significance between blast mTBI group and control; average time since most recent blast (if available) and average number of blast exposure (if available). Furthermore, helpful information involving study limitations was also extracted to enable a better understanding of the study.
2.5. Quality Assessment
Due to all the studies included being cross-sectional, the appraisal tool for cross-sectional studies (AXIS) was the critical appraisal tool used to assess the quality of the studies [19]. The tool was used to answer questions about the eligible article to then draw conclusion of the quality of the article through the overall score of “good”, “fair” or “poor”. Review of articles was done by one author (R.B). The AXIS tool allowed subjective outcome deduction enhancing flexibility in the judgement of articles as it was not a numerical scale [20].
2.6. Statistical Analysis
The mean and standard deviation PCL scores of blast mTBI and control group (no blast and no TBI) of each paper were gathered and analyzed in SPSS (IBM, Chicago, IL, USA). An unpaired t-test was used to compare means to identify statistical significance which was set to p < 0.05. A random effects model was utilized for meta-analysis to incorporate heterogeneity and calculated between study heterogeneity and variance through I2 and Tau2, respectively. Overall effect size was calculated by Cohens d, and summary effect sizes of each paper were presented. Egger’s intercept test was used to assess publication bias. Additionally, the means of the control and blast mTBI group were utilized to determine the likelihood of PTSD based on the average PCL score. A PCL score of 50 and above was considered PTSD positive for military personnel based on U.S. Department of Veterans Affair [21]. Probable PTSD was indicated with a cut off score of 34 which is considered optimum for probable PTSD diagnosis and indicates a 77.7% PTSD prevalence within the population [22]. Graphical data were displayed as forest plots created by SPSS. Due to the low number of studies, subgroup and meta-analysis were not conducted in recommendation of Cochrane [23].
3. Results
3.1. Study Selection
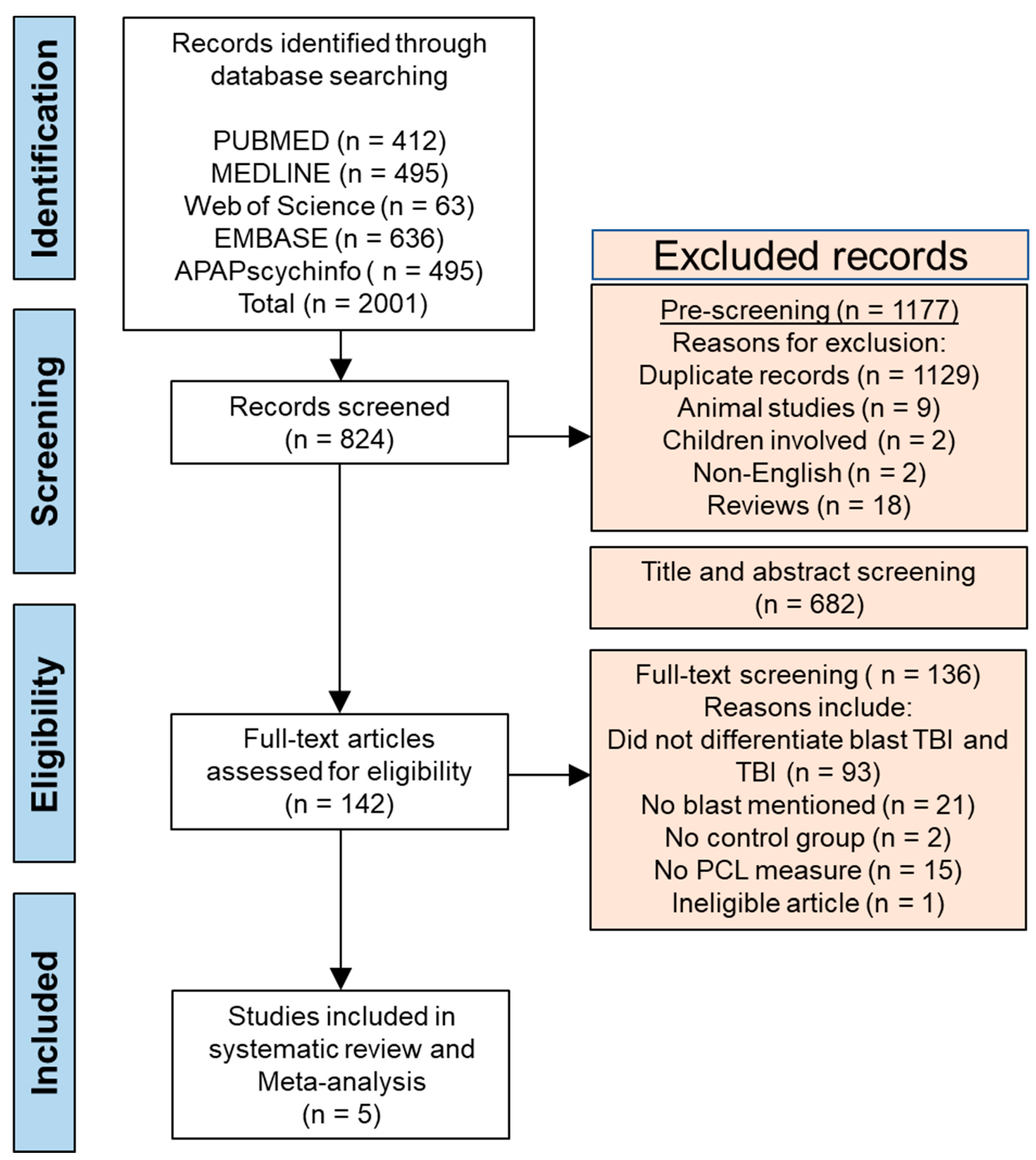
After conducting a search and following the PRISMA method, a total of 2001 articles were found across the 5 databases (Figure 1). Following this 1129 articles were removed due to being duplicates, 17 articles were removed as the full text article was not available, 18 removed for being reviews, 9 involving animal studies, two articles involving child participants and a further two for articles for not being written in English. This overall left 824 articles to be screened by title and abstract and after screening for eligibility, 142 articles were screened for the full text. Following full text screen six studies were remained (reason for exclusion described in Figure 1). Out of the six, one study appeared to be eligible when reviewing the participants [24]; however, they referenced the full procedure and participants inclusion and exclusion via referencing a previous study [25] which made it be deemed ineligible. This was because the control group were only screened for blast exposure and TBI during their deployment but may have suffered TBI pre- or post-deployments, thus excluded from review due to lack of clarity on whether pre- or post-deployment Blast or TBI status. No additional study was deemed eligible after screening the references of the five eligible studies, leaving a total of five studies for review and meta-analysis.
3.2. Study Characteristics
All five studies were observational cross-sectional studies, containing a blast mTBI group as the measure group and the control group experiencing no history of blasts or lifetime TBI [26,27,28,29,30]. Three studies used the PCL-M [28,29,30], and two studies used the PCL-C as the measure for PTSD symptom severity [26,27]. There were different methods used to diagnose blast mTBI. Three studies screened the medical records prior to conducting the interview [26,28,29]. The remaining two studies reported no screening of medical records [26,28]. However, all mTBI diagnosis was achieved through semi-structured interviews. Table 1 outlines the study characteristics.
3.3. Quality Assessment
Table 1 provides information on quality assessment and risk of bias outcome based on the AXIS tool. When performing quality assessment using the AXIS tool, four articles were given an overall score of fair [26,28,29,30]. This was given due to the sampling methods coupled with the small sample size which had potential to introduce bias and reduce generalizability. The remaining study was given a score of good based on the AXIS tool [27].
3.4. Participant Information
There were a variety of participant backgrounds from the eligible articles. One study included US military personnel from the National Intrepid Center of Excellence where patients from this population needed to show at least 6 months of post-concussion symptoms and TBI history [27]; two studies included operation enduring freedom (OEF)/operation Iraqi freedom (OIF)/operation new dawn (OND) military personnel participants who were deployed to Afghanistan or Iraq [26,28]; one study involved military participants returning from service [29] and one study involved participants seeking healthcare from Veterans Affair Puget Sound for veterans who had been deployed to Afghanistan or Iraq [30]. With regard to specific military population two papers included participants that were service members [27,29], two studies included participants that were veterans [28,30] and one paper included both service members and veterans [26]. To note, Yeh et al. [27] comparative control were health care military beneficiaries that were active duty and not deployed. Furthermore, three studies appeared to describe convenience sampling for obtaining participants [27,28,29] with the remaining two not elucidating sampling methods [26,29].
3.5. Blast Study Characteristics
Of the studies that reported number of blasts the means ranged from 2.6 blasts [27] to 38.4 blasts for participants [28]. Of the studies that reported the time since participant’s most recent blast, means ranged from 103 days [29] to 6.4 years [28]. Table 2 summarizes the information regarding blast information.
3.6. Results Regarding PTSD
All studies reported means of the PCL for the blast mTBI and control groups. PCL means ranged from 35.29–52.10 and 20.7–31.64 for the blast mTBI and control groups, respectively. The highest PCL score of 52.10 was reported by Pagulayan et al. [28] for the blast mTBI group and the lowest, 35.29, was reported by Tate et al. [29]. For control groups the highest PCL score was reported by Tate et al. [29] and the lowest score was reported by Petrie et al. [30]. Only one study reported no significant difference between the blast mTBI PCL score and control group PCL score [29], however the PCL symptom severity score was still higher than that of the control, with the remaining four reporting significant differences between groups [26,27,28,30].
Of the studies that were statistically significant two studies had a p value < 0.001 [28,30] and the other two had a p value < 0.0001 [26,27]. Determining the likelihood of PTSD utilizing the PCL score, two papers [26,27] indicated a PTSD positive score based on the mean PCL score of the blast mTBI being above 50 and the remaining three [26,29,30] indicating probable PTSD with a mean PCL score greater than 34. None of the studies had a control group mean PCL greater than 34 to indicate probable PTSD. All this information is summarized in Table 1.
3.7. Meta-Analysis
Summary of meta-analysis results displayed in Table 3. Unpaired t-test between blast mTBI and control group mean PCL scores showed statistical significance, p < 0.001. Random effects model was used to calculate between study heterogeneity and between study variance with I2 = 84% and Tau2 = 0.44, respectively. Egger’s intercept was 0.134 and since p > 0.1, it was not significant thus publication bias is unlikely. Summary effect sizes for each study are displayed in Figure 2 as forest plots and the overall effect size was 1.622 (Cohen’s D > 0.8) thus large effect indicating practical significance.
4. Discussion
This article aimed to investigate the effect blast mTBI on PTSD symptom severity and observe the likelihood of developing PTSD from blast mTBI in the format of a systematic review and meta-analysis. Overall, the difference in mean PCL score of the blast mTBI and control groups was seen to be statistically significant (p < 0.001) with a large effect size indicating practical significance. Further to this, all blast mTBI groups appeared to have probable PTSD or greater, based on average PCL score which was not observed in control groups. However, the high heterogeneity (I2 = 84%) adds caution in results interpretation and conclusion derivation.
Regardless, there appeared to be some effect between the PTSD symptom severity and the presence of blast mTBI in military personnel. Mild TBI has been associated with the disturbance of the frontal subcortical neurocircuitry which is involved in emotion regulation, thus leading to elevated emotional responsivity after trauma and has been shown to reduce the threshold for PTSD [15]. Due to a reduced threshold for PTSD, sufferers of blast mTBI can experience increased PTSD symptom severity compared to those who do not suffer TBI. Additionally, repetitive blast exposure has been shown to increase PTSD symptoms in rats via the increase in anxiety and fear [31]. This implies that fear and anxiety could be what is exacerbated by the blast mTBI but of course this has yet to be shown in humans. Moreover, the four domains of PTSD are: intrusive memories, active avoidance, distressed emotional state, and changes in arousal and reactivity; and re-experiencing, part of intrusive memories domain, has been shown to be significantly higher in blast mTBI participants compared to controls where other domains showed no significant difference [32,33]. This provides insight as to what aspect of PTSD may be impacted by blast mTBI, potentially encouraging healthcare practitioners to focus on this aspect of patient rehabilitation in order to maximize patient recovery. However, more research is required to further investigate the domains of PTSD affected by blast mTBI to increase understanding and inform the patient management process.
Although Tate et al. [29] reported higher PTSD symptoms between the blast mTBI and control group, no significant difference of PCL was detected. It is difficult to reconcile this with other studies that showed a clear difference in PTSD but one explanation could be due to their definition of “healthy controls”. The study does not elaborate on what is meant by “healthy non-injured” participants and thus the use of the word healthy appears vague as it is not supplemented by complimentary inclusion and exclusion criteria. Although not suffering a blast mTBI, participants may have suffered other physical impairments such as amputation that affect PTSD symptom severity unknown to the reader [34]. Even though the participants are age and gender matched, combat exposure and deployment location are other variables that contribute to PTSD [35,36]. Therefore, theories of possible causes for the non-significant difference could be because the control group had more combat exposure or been deployed to more hostile locations compared to blast mTBI participants. However, this hypothesis cannot be said with confidence due to the lack of information provided in the Tate et al. study [28]. Insight to this by the provision of the extra information would provide valuable knowledge as to why this paper produced a non-significant difference, especially as it contributed to the considerable heterogeneity present in the meta-analysis. Further investigation would allow better insight on heterogeneity to increase confidence in results and understand factors that contribute to PTSD.
In terms of the likelihood of developing PTSD, results appear to suggest there to be an increased risk of PTSD diagnosis following blast mTBI, since studies reported probable PTSD or mean PCL scores of 34 and above. Veterans with confirmed TBI were identified to be over three times more likely to have PTSD diagnosis than those with no TBI and increased TBI severity also increases the risk of developing PTSD [37,38]. Fear conditioning is a proposed possible mechanism to why PTSD is likely to develop from TBI. For example, TBI in rats enhances fear learning promoted by conditioned and novel stimuli settings, due to up-regulation of excitatory NMDA receptors in the basolateral amygdala complex [39]. Therefore, regardless of whether veterans re-experience blasts or are in civilian settings, they may have heightened fear association derived from PTSD. Memory reconstruction of the event and post amnesia resolution are other possible mechanisms to explain PTSD occurrence following TBI [40]. This implies there to be a long-term effect and even if no formal diagnosis of PTSD has been made after a blast mTBI event, the possibility of its development remains. Hence, there appears to be a relationship between mTBI and comorbid PTSD due to the high likelihood of mTBI sufferers developing PTSD. Furthermore, loss of consciousness following blast mTBI has been shown to be predictive of PTSD [41]. Healthcare professionals dealing with blast mTBI patients in the military settings should not only focus on the biological aspects of management but be vigilant in the development of PTSD and incorporate psychological management when dealing with blast mTBI patients.
4.1. Implications and Future Considerations
This review can be used to increase healthcare clinician awareness of PTSD symptom severity and prevalence when dealing with blast mTBI patients. Sufferers of PTSD and more severe PTSD symptomology can have increased anxiety and sensitivity to treatment and possess reduced participant resilience in completing treatment, especially in rehabilitation, leading to poorer mTBI outcomes [16]. Furthermore, mental health is observed to be the main cause for disability and therefore if not appropriately managed, the psychological impairment of PTSD can lead to worse impairments such chronic pain [42,43]. This can prove harmful to military population due to the increased risk of pain, complicating management. Therefore, it is paramount that healthcare practitioners do not solely focus on biomedical management but adopt a biopsychosocial approach when dealing with military personnel as it can potentially attenuate PTSD [44]. There has been recognition to improve health care practitioner’s knowledge on mental health care to veterans, including practitioners dealing with veterans in civilian settings who have experienced blast mTBI in the past [45,46].
In a future consideration, it would be interesting to determine what factors impact on PTSD symptomology in blast alone or mTBI alone. This will enhance the understanding of contributors towards PTSD symptomology severity for healthcare awareness. Although partially alluded to, it would also be interesting to determine the domain of PTSD that is most affected by blast mTBI. Knowledge of this could help healthcare practitioners on their treatment standpoint and what to be aware of and further understand potential barriers this could cause to treatment.
4.2. Limitations
One common limitation between some of the studies was the lack of medical records used when diagnosing mTBI [26,28]. The diagnosis of blast mTBI via the interview relied heavily on the retrospective self-reported recall of events from participants following a blast. Without medical records being used in conjunction to confirm diagnosis at the time of injury, there is a risk of recall and/or response bias from participants. This is something to be aware of as these biases have been shown contribute to the decreased precision of self-reported events following mTBI and blast waves have been shown to effect memory [47,48]. Another common limitation between the studies was the small sample size. A small sample size impacts the generalizability of results generated and it reduces the study’s power of the study. Thirdly, the sampling method utilized by the studies proved to be a limitation. Convenience sampling employed by researchers may not provide representative results of PCL score in the military personnel population. This reduces the generalizability of results towards people who do not fit the population demographic, i.e., gender or race. Further to this, participants also have potential to be selected based on researcher sampling bias.
Another limitation identified was the small number of studies which were eligible for analysis following the search and screening of databases. Articles older than 10 years old were disregarded to ensure up to date articles were selected. However, due to the prevalence of wars and conflict throughout history increasing the publication date range may have proved beneficial. Therefore, setting a no publication date limitations may increase the number of studies screened in future studies. Another limitation was the considerable heterogeneity between the studies adding caution to the interpretation of results. Although high, I2 and Tau2 value should be interpreted with caution due to uncertainty of the value when there are a small number of studies [23]. Due to the small number of studies, further investigation into heterogeneity was not done because of the doubtful value it would provide [23].
Additionally, lack of consistent information provided between each study proved difficult in determining and exploring heterogeneity. Finally, another limitation was the use of PCL as the outcome measure for PTSD symptom severity instead of the Clinician-Administered PTSD Scale for DSM-5 (CAPS). CAPS is the gold standard for PTSD assessment and has been noted to have minimal measurement error occurring from the participant answering its questions [49]. Therefore, utilizing CAPS can enable higher accuracy and confidence in findings. However, PCL was opted as the measurement tool to compare due to its reported quick and easy application over CAPS and common use by clinicians [14]. This would allow ease of comparison between studies and increase the number of potential articles. Future studies could incorporate CAPS and PCL for systematic review and meta-analysis of PTSD symptom severity.
5. Conclusions
To conclude, there appears to be a relationship between blast mTBI and PTSD symptom severity, where blast mTBI increases PTSD severity. This was demonstrated through the statistical significance of PCL between blast mTBI military group and veterans who have not experienced lifetime blast or mTBI. Further to this, blast mTBI was observed to increase the likelihood of PTSD diagnosis based on PCL score. This could be due to the effect the blast wave has on the brain. Overall, this aids awareness to healthcare professionals managing blast mTBI veterans to be aware of PTSD symptoms which can affect outcomes. Increasing awareness can enable veterans who suffer TBI without official PTSD diagnosis to be treated and managed with a more biopsychosocial approach with additional psychological intervention to improve clinical outcomes. The heterogeneity present adds caution to conclusions and indicates the need to better define the blast mTBI population in future studies investigating PTSD. Further to this, determination of what has the greater effect on PTSD, the blast itself or the TBI, or understanding which domains are impaired by blast mTBI are all considerations for future research.
Author Contributions
Conceptualization, R.B. and Z.A.; methodology, R.B. and Z.A.; formal analysis, R.B. and Z.A.; investigation, R.B. and Z.A.; data curation, R.B. writing original draft preparation, R.B. and Z.A.; writing—review and editing, R.B. and Z.A.; supervision, Z.A.; project administration, Z.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study since it is a systematic review of published literature.
Informed Consent Statement
Patient consent was waived because no patients or members of the public were involved in the design, conduct of this study, or reporting of this research. research article describing a study in-volving humans should contain this statement.
Data Availability Statement
All data generated as part of this study are included in the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Malec, J.F.; Brown, A.W.; Leibson, C.L.; Flaada, J.T.; Mandrekar, J.N.; Diehl, N.N.; Perkins, P.K. The mayo classification system for traumatic brain injury severity. J. Neurotrauma 2007, 24, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Fear, D.; Phil, N.T.; Wessely, S. Shell shock and mild traumatic brain injury: A historical review. Am. J. Psychiatry 2007, 164, 1641–1645. [Google Scholar] [CrossRef] [PubMed]
- Defence Health Agency. DOD TBI Worldwide Numbers. Available online: https://health.mil/Military-Health-Topics/Centers-of-Excellence/Traumatic-Brain-Injury-Center-of-Excellence/DOD-TBI-Worldwide-Numbers (accessed on 24 August 2022).
- Wojcik, B.E.; Stein, C.R.; Bagg, K.; Humphrey, R.J.; Orosco, J. Traumatic brain injury hospitalizations of US army soldiers deployed to Afghanistan and Iraq. Am. J. Prev. Med. 2010, 38, S108–S116. [Google Scholar] [CrossRef] [PubMed]
- Bryden, D.W.; Tilghman, J.I.; Hinds, S.R. Blast-related traumatic brain injury: Current concepts and research considerations. J. Exp. Neurosci. 2019, 13, 1179069519872213. [Google Scholar] [CrossRef]
- Rosenfeld, J.V.; McFarlane, A.C.; Bragge, P.; Armonda, R.A.; Grimes, J.B.; Ling, G.S. Blast-related traumatic brain injury. Lancet Neurol. 2013, 12, 882–893. [Google Scholar] [CrossRef]
- Goeller, J.; Wardlaw, A.; Treichler, D.; O’Bruba, J.; Weiss, G. Investigation of cavitation as a possible damage mechanism in blast-induced traumatic brain injury. J. Neurotrauma 2012, 29, 1970–1981. [Google Scholar] [CrossRef]
- Van Praag, D.L.; Cnossen, M.C.; Polinder, S.; Wilson, L.; Maas, A.I. Post-traumatic stress disorder after civilian traumatic brain injury: A systematic review and meta-analysis of prevalence rates. J. Neurotrauma 2019, 36, 3220–3232. [Google Scholar] [CrossRef]
- Available online: https://www.statista.com/statistics/1202701/post-traumatic-stress-disorder-during-service-after-911-by-problem-veterans/ (accessed on 24 August 2022).
- Kennedy, J.E.; Lu, L.H.; Reid, M.W.; Leal, F.O.; Cooper, D.B. Correlates of depression in US military service members with a history of mild traumatic brain injury. Military Med. 2019, 184, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Carlson, K.F.; Nelson, D.; Orazem, R.J.; Nugent, S.; Cifu, D.X.; Sayer, N.A. Psychiatric diagnoses among Iraq and Afghanistan war veterans screened for deployment-related traumatic brain injury. J. Trauma. Stress 2010, 23, 17–24. [Google Scholar] [CrossRef]
- Phipps, H.; Mondello, S.; Wilson, A.; Dittmer, T.; Rohde, N.N.; Schroeder, P.J.; Nichols, J.; McGirt, C.; Hoffman, J.; Tanksley, K.; et al. Characteristics and impact of US military blast-related mild traumatic brain injury: A systematic review. Front. Neurol. 2020, 11, 559318. [Google Scholar] [CrossRef]
- Tiet, Q.Q.; Schutte, K.K.; Leyva, Y.E. Diagnostic accuracy of brief PTSD screening instruments in military veterans. J. Subst. Abus. Treat 2013, 45, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, K.C.; Lang, A.J.; Norman, S.B. Synthesis of the psychometric properties of the PTSD checklist (PCL) military, civilian, and specific versions. Depress. Anxiety 2011, 28, 596–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeardMann, C.A.; McMaster, H.S.; Warner, S.; Esquivel, A.P.; Porter, B.; Powell, T.M.; Tu, X.M.; Lee, W.W.; Rull, R.P.; Hoge, C.W.; et al. Comparison of posttraumatic stress disorder checklist instruments from diagnostic and statistical manual of mental disorders, vs. fifth edition in a large cohort of US military service members and veterans. JAMA Netw. Open 2021, 4, e218072. [Google Scholar] [CrossRef] [PubMed]
- Vasterling, J.J.; Jacob, S.N.; Rasmusson, A. Traumatic brain injury and posttraumatic stress disorder: Conceptual, diagnostic, and therapeutic considerations in the context of co-occurrence. J. Neuropsychiatry Clin. Neurosci. 2018, 30, 91–100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals. Internal. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.ptsd.va.gov/professional/assessment/documents/PCL_Scoring_Information.pdf (accessed on 19 August 2022).
- Murphy, D.; Ross, J.; Ashwick, R.; Armour, C.; Busuttil, W. Exploring optimum cut-off scores to screen for probable posttraumatic stress disorder within a sample of UK treatment-seeking veterans. Eur. J. Psychotraumatology 2017, 8, 1398001. [Google Scholar] [CrossRef] [Green Version]
- Cochrane. Chapter 10: Analysing Data and Undertaking Meta-Analyses. Available online: https://training.cochrane.org/handbook/current/chapter-10#_Ref180060294 (accessed on 26 August 2022).
- Callahan, M.L.; Storzbach, D. Sensory sensitivity and posttraumatic stress disorder in blast exposed veterans with mild traumatic brain injury. Appl. Neuropsychol. Adult. 2019, 26, 365–373. [Google Scholar] [CrossRef]
- Storzbach, D.; O’Neil, M.E.; Roost, S.-M.; Kowalski, H.; Iverson, G.L.; Binder, L.M.; Fann, J.R.; Huckans, M. Comparing the neuropsychological test performance of Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans with and without blast exposure, mild traumatic brain injury, and posttraumatic stress symptoms. J. Int. Neuropsychol. Soc. 2015, 21, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troyanskaya, M.; Pastorek, N.J.; Scheibel, R.S.; Petersen, N.J.; McCulloch, K.; Wilde, E.A.; Henson, H.K.; Levin, H.S. Combat exposure, PTSD symptoms, and cognition following blast-related traumatic brain injury in OEF/OIF/OND service members and veterans. Mil. Med. 2015, 180, 285–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, P.H.; Guan Koay, C.; Wang, B.; Morissette, J.; Sham, E.; Senseney, J.; Joy, D.; Kubli, A.; Yeh, C.; Eskay, V.; et al. Compromised neurocircuitry in chronic blast-related mild traumatic brain injury. Hum. Brain Mapp. 2017, 38, 352–369. [Google Scholar] [CrossRef] [PubMed]
- Pagulayan, K.F.; Rau, H.; Madathil, R.; Werhane, M.; Millard, S.P.; Petrie, E.C.; Parmenter, B.; Peterson, S.; Sorg, S.; Hendrickson, R.; et al. Retrospective and prospective memory among OEF/OIF/OND veterans with a self-reported history of blast-related mTBI. J. Int. Neuropsychol. Soc. 2018, 24, 324–334. [Google Scholar] [CrossRef]
- Tate, D.; York, G.; Reid, M.; Cooper, D.B.; Jones, L.; Robin, D.A.; Kennedy, J.E.; Lewis, J. Preliminary findings of cortical thickness abnormalities in blast injured service members and their relationship to clinical findings. Brain Imag. Behav. 2014, 8, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Petrie, E.C.; Cross, D.J.; Yarnykh, V.L.; Richards, T.; Martin, N.M.; Pagulayan, K.; Hoff, D.; Hart, K.; Mayer, C.; Tarabochia, M.; et al. Neuroimaging, behavioral, and psychological sequelae of repetitive combined blast/impact mild traumatic brain injury in Iraq and Afghanistan war veterans. J. Neurotrauma 2014, 31, 425–436. [Google Scholar] [CrossRef] [Green Version]
- Elder, G.A.; Dorr, N.P.; De Gasperi, R.; Sosa, M.A.G.; Shaughness, M.C.; Maudlin-Jeronimo, E.; Hall, A.A.; McCarron, R.M.; Ahlers, S.T. Blast exposure induces post-traumatic stress disorder-related traits in a rat model of mild traumatic brain injury. J. Neurotrauma 2012, 29, 2564–2575. [Google Scholar] [CrossRef]
- Jorge, R.E. Posttraumatic stress disorder. Contin. Lifelong Learn. Neurol. 2015, 21, 789–805. [Google Scholar] [CrossRef]
- Kennedy, J.E.; Leal, F.O.; Lewis, J.D.; Cullen, M.A.; Amador, R.R. Posttraumatic stress symptoms in OIF/OEF service members with blast-related and non-blast-related mild TBI. NeuroRehab 2010, 26, 223–231. [Google Scholar] [CrossRef]
- Sahu, A.; Sagar, S.; Kumar, M.; Sagar, R. A study of psychiatric comorbidity after traumatic limb amputation: A neglected entity. Ind. Psychiatry J. 2017, 26, 228–292. [Google Scholar]
- Averill, L.A.; Abdallah, C.G.; Pietrzak, R.H.; Averill, C.L.; Southwick, S.M.; Krystal, J.H.; Harpaz-Rotem, I. Combat exposure severity is associated with reduced cortical thickness in combat veterans: A preliminary report. Chronic. Stress 2017, 1, 2470547017724714. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.-C.; Arkes, J.; Pilgrim, J. The effects of deployment intensity on post-traumatic stress disorder: 2002–2006. Mil. Med. 2009, 174, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dieter, J.N.I.; Engel, S.D. Traumatic brain injury and posttraumatic stress disorder: Comorbid consequences of war. Neurosci Insights 2019, 14, 1179069519892933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, M.B.; Kessler, R.C.; Heeringa, S.G.; Jain, S.; Campbell-Sills, L.; Colpe, L.J.; Fullerton, C.S.; Nock, M.K.; Sampson, N.A.; Schoenbaum, M.; et al. Prospective longitudinal evaluation of the effect of deployment-acquired traumatic brain injury on posttraumatic stress and related disorders: Results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). Am. J. Psychiatry 2015, 172, 1101–1111. [Google Scholar] [CrossRef] [Green Version]
- Reger, M.L.; Poulos, A.M.; Buen, F.; Giza, C.C.; Hovda, D.A.; Fanselow, M.S. Concussive brain injury enhances fear learning and excitatory processes in the amygdala. Biol. Psychiatry 2012, 71, 335–343. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R. Post-traumatic stress disorder vs. traumatic brain injury. Dialogues Clin. Neurosci. 2011, 13, 251–262. [Google Scholar] [CrossRef]
- Eskridge, S.L.; Macera, C.A.; Galarneau, M.R.; Holbrook, T.L.; Woodruff, S.I.; MacGregor, A.J.; Morton, D.J.; Shaffer, R.A. Influence of combat blast-related mild traumatic brain injury acute symptoms on mental health and service discharge outcomes. J. Neurotrauma 2013, 30, 1391–1397. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, J.; Liu, S.; Wang, Y.; Cui, R.; Zhang, X. The link between depression and chronic pain: Neural mechanisms in the brain. Neural. Plast. 2017, 2017, 9724371. [Google Scholar] [CrossRef] [Green Version]
- Crawford, C.; Wallerstedt, D.B.; Khorsan, R.; Clausen, S.S.; Jonas, W.B.; Walter, J.A.G. A systematic review of biopsychosocial training programs for the self-management of emotional stress: Potential applications for the military. Evid. Based Complement Altern. Med. 2013, 2013, 747694. [Google Scholar] [CrossRef] [Green Version]
- Soundy, A.; Hemmings, L.; Gardiner, L.; Rosewilliam, S.; Heneghan, N.R.; Cronin, K.; Reid, K. E-learning communication skills training for physiotherapy students: A two phased sequential mixed methods study. Patient Ed. Couns. 2021, 104, 2045–2053. [Google Scholar] [CrossRef] [PubMed]
- Busuttil, W. Understanding military-related mental illness for effective health care. Trends Urol Men’s Health 2022, 13, 11–16. [Google Scholar] [CrossRef]
- Iverson, G.L.; Lange, R.T.; Brooks, B.L.; Lynn Ashton Rennison, V. “Good old days” bias following mild traumatic brain injury. Clin. Neuropsychol. 2010, 24, 17–37. [Google Scholar] [CrossRef] [PubMed]
- Baalman, K.L.; Cotton, R.J.; Rasband, S.N.; Rasband, M.N. Blast wave exposure impairs memory and decreases axon initial segment length. J. Neurotrauma 2013, 30, 741–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM–5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow chart.

Figure 2.
Forest plot showing the summary effect estimates for each paper of blast mTBI and no blast mTBI PCL score [26,27,28,29,30].


{kind=link}
{kind=link}
Table 1.
Summary of participant information and PCL scores of each paper and PTSD and quality assessment rating.
Table 1.
Summary of participant information and PCL scores of each paper and PTSD and quality assessment rating.
| Study | Method of mTBI Diagnosis | Participants | PCL Mean | Significant PCL Score | Likelihood PTSD Diagnosis of Blast mTBI Participants | Axis Score |
|---|---|---|---|---|---|---|
| Troyanskaya et al. [26] | Clinician administered Poly Trauma interview was used to collect data on pre- and post-deployment history and identify mTBI history and severity | 54 blast mTBI 43 veterans who had no blast exposure or TBI | Blast mTBI = 43.9 Control = 25.9 | p < 0.0001 | Probable PTSD | Fair |
| Yeh et al. [27] | Routine comprehensive clinical screening evaluation undertaken by medical/health-care professionals + MEDICAL RECORDS | 202 blast mTBI that were US military personnel (Service Members) 40 control active-duty Healthcare Military beneficiaries not deployed. No TBI and No blasts | Blast mTBI = 51.7 Control = 20.9 | p < 0.0001 | PTSD Positive | Good |
| Pagulayan et al. [28] | By Two clinicians (physicians or physician assistant) who were trained in mTBI and PTSD did semi structured interviews on potential TBI participants | 42 OEF/OIF/OND Veterans with a self-reported history of blast-related mTBI 19 OEF/OIF/OND era Veterans with no history of blast exposures or TBI and no current PTSD | Blast mTBI = 52.1 Control = 22.2 | p < 0.001 | PTSD Positive | Fair |
| Tate et al. [29] | Semi structured interview and record review using the veterans Affair/Department of Defence criteria had document LOC of <30 + MEDICAL RECORDS | 12 blast mTBI active-duty service personnel, no injury prior 11 healthy not injured service members | Blast mTBI = 35.29 Control = 31.64 | p = 0.47 | Probable PTSD | Fair |
| Petrie et al. [30] | Semi Structured interviews made by researchers in collaboration with 3 former senior non-commissioned officers + MEDICAL RECORDS | 34 male blast-mTBI veterans 18 non-blast veterans—No mTBI | Blast mTBI = 49.5 Control = 20.7 | p < 0.001 | Very Likely PTSD | Fair |
Notes: OEF: operation enduring freedom, OIF: operation Iraqi freedom; OND: operation new dawn.
Table 2.
Summary of blast exposure information.
| Study | Average Blast Exposure | Mean Time Since Injury Blast TBI |
|---|---|---|
| Troyanskaya et al. [26] | Undocumented | Undocumented |
| Yeh et al. [27] | 2.6 mean | 576 days |
| Pagulayan et al. [28] | Symptomatic blast exposures = 38.4 | 6.4 years |
| Tate et al. [29] | Unknown | 103 days |
| Petrie et al. [30] | 19.6 blast TBI | Unknown |
Table 3.
Summary of meta-analysis results.
| Test | Result | Interpretation |
|---|---|---|
| Significance testing | p < 0.001 | Blast mTBI has significantly difference score compared to controls |
| Heterogeneity (Random effects model) | I2 = 0.84 Tau2 = 0.44 | Considerable heterogeneity Estimate of between study variance |
| Egger’s intercept test | 0.134 (p > 0.1) | Unlikely publication bias |
| Effect size (Cohen’s D) | 1.622 (d > 0.8) | Large effect so practically significant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Borinuoluwa, R.; Ahmed, Z. Does Blast Mild Traumatic Brain Injury Have an Impact on PTSD Severity? A Systematic Review and Meta-Analysis. Trauma Care 2023, 3, 9-21. https://doi.org/10.3390/traumacare3010002
AMA Style
Borinuoluwa R, Ahmed Z. Does Blast Mild Traumatic Brain Injury Have an Impact on PTSD Severity? A Systematic Review and Meta-Analysis. Trauma Care. 2023; 3(1):9-21. https://doi.org/10.3390/traumacare3010002
Chicago/Turabian StyleBorinuoluwa, Raphael, and Zubair Ahmed. 2023. "Does Blast Mild Traumatic Brain Injury Have an Impact on PTSD Severity? A Systematic Review and Meta-Analysis" Trauma Care 3, no. 1: 9-21. https://doi.org/10.3390/traumacare3010002