
A Preliminary Scoping Review of Trauma Recovery Pathways among Refugees in the United States


Abstract
:1. Introduction
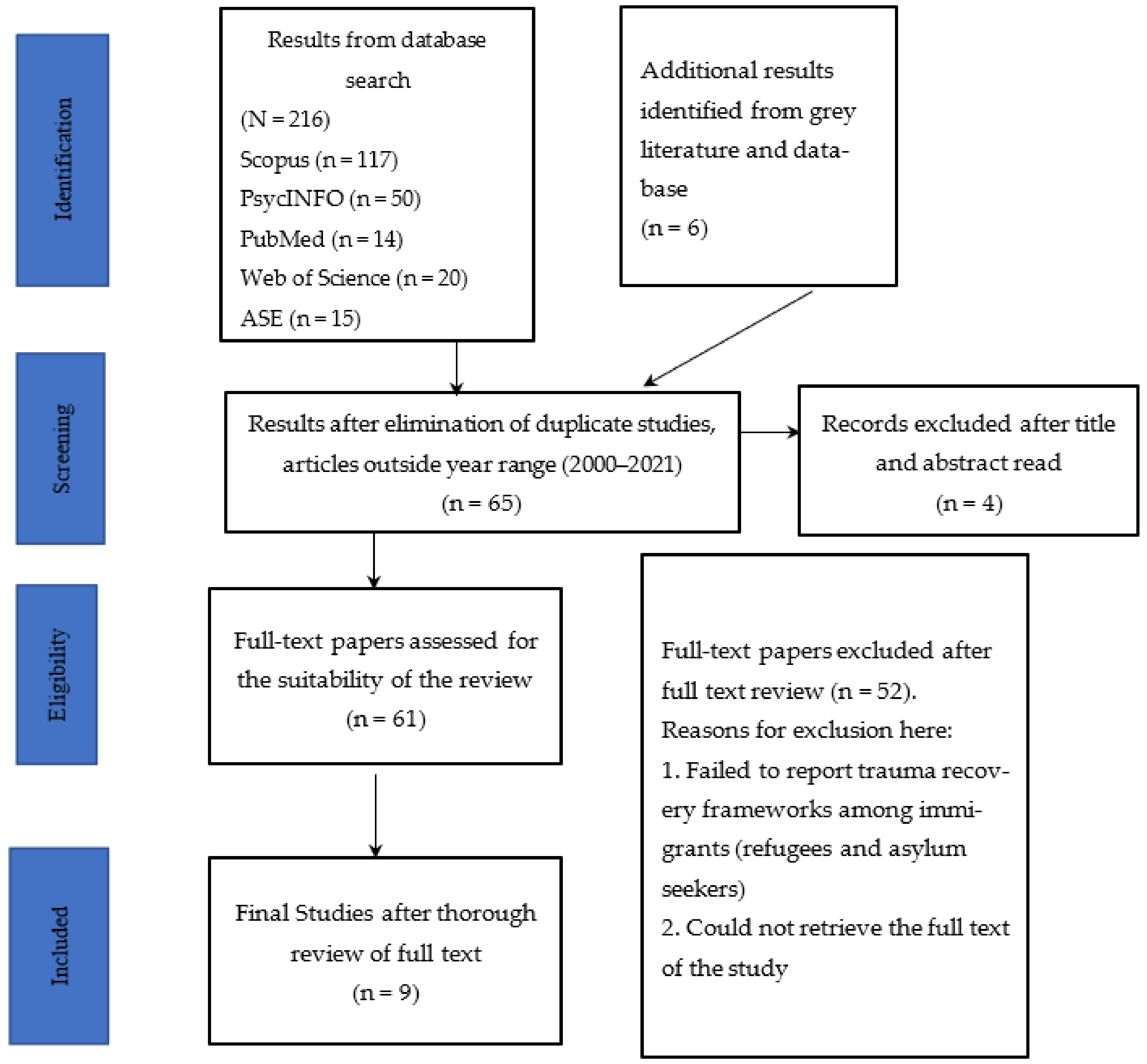
2. Review Method
Methodological Description of Included Studies
3. Results
3.1. Summary of Findings and Discussion
3.2. Macro-Level Structural Intervention—Preventing Re-Traumatization
3.3. Culturally Sensitive Therapeutic Intervention
3.4. Diagnosis and Therapy
4. Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNHCR. Global Trends 2016. 2017. Available online: http://www.unhcr.org/5943e8a34.pdf (accessed on 30 September 2022).
- Yaylaci, F.T. Trauma and resilient functioning among Syrian refugee children. Dev. Psychopathol. 2018, 30, 1923–1936. [Google Scholar] [CrossRef]
- Schick, M.; Morina, N.; Mistridis, P.; Schnyder, U.; Bryant, R.A.; Nickerson, A. Changes in Post-migration Living Difficulties Predict Treatment Outcome in Traumatized Refugees. Front. Psychiatry 2018, 9, 476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickerson, A. Pathways to recovery: Psychological mechanisms underlying refugee mental health. In Mental Health of Refugee and Conflict-Affected Populations; Springer: Cham, Swizerland, 2018; pp. 91–109. [Google Scholar] [CrossRef]
- Oren-Schwartz, R.; Aizik-Reebs, A.; Yuval, K.; Hadash, Y.; Bernstein, A. Effect of mindfulness-based trauma recovery for refugees on shame and guilt in trauma recovery among African asylum-seekers. Emotion 2022. [Google Scholar] [CrossRef]
- Kartal, D.; Alkemade, N.; Kiropoulos, L. Trauma and mental health in resettled refugees: Mediating effect of host language acquisition on posttraumatic stress disorder, depressive and anxiety symptoms. Transcult. Psychiatry 2019, 56, 3–23. [Google Scholar] [CrossRef]
- Bhui, K. A Refugee Rose of competencies and capabilities for mental healthcare of refugees. BJPsych Open 2022, 8, e45. [Google Scholar] [CrossRef]
- Lampa, E.; Sarkadi, A.; Warner, G. Implementation and Maintenance of a Community-Based Intervention for Refugee Youth Reporting Symptoms of Post-Traumatic Stress: Lessons from Successful Sites. Int. J. Environ. Res. Public Health 2021, 18, 43. [Google Scholar] [CrossRef]
- Kashyap, S.; Keegan, D.; Liddell, B.J.; Thomson, T.; Nickerson, A. An Interaction Model of Environmental and Psychological Factors Influencing Refugee Mental Health. J. Trauma. Stress 2021, 34, 257–266. [Google Scholar] [CrossRef]
- Biswas, T.; Thomas, H.J.; Scott, J.G.; Munir, K.; Baxter, J.; Huda, M.M.; Renzaho, A.M.N.; Cross, D.; Ahmed, H.U.; Mahumud, R.A.; et al. Variation in the prevalence of different forms of bullying victimisation among adolescents and their associations with family, peer and school connectedness: A population-based study in 40 lower and middle income to high-income countries (LMIC-HICs). J. Child Adolescent Trauma 2022, 15, 1029–1039. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.; Berthold, S.M.; Critelli, F.M. Refugees and Asylum Seekers. In Trauma and Human Rights: Integrating Approaches to Address Human Suffering; Butler, L.D., Critelli, F.M., Carello, J., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 221–240. [Google Scholar] [CrossRef]
- Umer, M.; Elliot, D.L. Being Hopeful: Exploring the Dynamics of Post-traumatic Growth and Hope in Refugees. J. Refug. Stud. 2021, 34, 953–975. [Google Scholar] [CrossRef]
- Boettcher, V.S.; Nowak, A.C.; Neuner, F. Mental health service utilization and perceived barriers to treatment among adult refugees in Germany. Eur. J. Psychotraumatol. 2021, 12, 1910407. [Google Scholar] [CrossRef]
- Nilsson, H.; Saboonchi, F.; Gustavsson, C.; Malm, A.; Gottvall, M. Trauma-afflicted refugees’ experiences of participating in physical activity and exercise treatment: A qualitative study based on focus group discussions. Eur. J. Psychotraumatology 2019, 10, 1699327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abooali, S. Exploring the somatic dimension for sport-based interventions: A refugee’s autoethnography. Sport Soc. 2022, 25, 506–522. [Google Scholar] [CrossRef]
- Van Haumeder, A.; Ghafoori, B.; Retailleau, J. Psychological adaptation and posttraumatic stress disorder among Syrian refugees in Germany: A mixed-methods study investigating environmental factors. Eur. J. Psychotraumatol. 2019, 10, 1686801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferriss, S.S.; Forrest-Bank, S.S. Perspectives of Somali Refugees on Post-traumatic Growth after Resettlement. J. Refug. Stud. 2018, 31, 626–646. [Google Scholar] [CrossRef]
- Schlaudt, V.A.; Bosson, R.; Williams, M.T.; German, B.; Hooper, L.M.; Frazier, V.; Carrico, R.; Ramirez, J. Traumatic experiences and mental health risk for refugees. Int. J. Environ. Res. Public Health 2020, 17, 1943. [Google Scholar] [CrossRef] [Green Version]
- Koutra, K.; Burns, C.; Sinko, L.; Kita, S.; Bilgin, H.; Arnault, D.S. Trauma Recovery Rubric: A Mixed-Method Analysis of Trauma Recovery Pathways in Four Countries. Int. J. Environ. Res. Public Health 2022, 19, 10310. [Google Scholar] [CrossRef]
- Sargeant, J.M.; O’Connor, A.M. Scoping Reviews, Systematic Reviews, and Meta-Analysis: Applications in Veterinary Medicine. Front. Veter-Sci. 2020, 7, 11. [Google Scholar] [CrossRef]
- Hilary, A.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar]
- Alessi, E.J.; Kahn, S. A framework for clinical practice with sexual and gender minority asylum seekers. Psychol. Sex. Orientat. Gend. Divers. 2017, 4, 383–391. [Google Scholar] [CrossRef]
- Endale, T.; Jean, N.S.; Birman, D. COVID-19 and refugee and immigrant youth: A community-based mental health perspective. Psychol. Trauma: Theory, Res. Pract. Policy 2020, 12, S225–S227. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, S.; Page, A.C.; Joscelyne, A. Post-migration treatment targets associated with reductions in depression and PTSD among survivors of torture seeking asylum in the USA. Psychiatry Res. 2019, 271, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Im, H.; Swan, L.E.T. Capacity Building for Refugee Mental Health in Resettlement: Implementation and Evaluation of Cross-Cultural Trauma-Informed Care Training. J. Immigr. Minor. Health 2020, 22, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.C.; Kivlighan, D.M., III. When home is gone: An application of the multicultural orientation framework to enhance clinical practice with refugees of forced migration. Prof. Psychol. Res. Pract. 2019, 50, 176–183. [Google Scholar] [CrossRef]
- Powers, A.; Woods-Jaeger, B.; Stevens, J.S.; Bradley, B.; Patel, M.B.; Joyner, A.; Smith, A.K.; Jamieson, D.J.; Kaslow, N.; Michopoulos, V. Trauma, psychiatric disorders, and treatment history among pregnant African American women. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 138–146. [Google Scholar] [CrossRef]
- Poudel-Tandukar, K.; Jacelon, C.S.; Bertone-Johnson, E.R.; Gautam, B.; Palmer, P.H.; Hollon, S.D. Coping strategies and stress among resettled Bhutanese adults in Massachusetts. Am. J. Orthopsychiatry 2020, 90, 502–509. [Google Scholar] [CrossRef]
- Im, H.; Rodriguez, C.; Grumbine, J.M. A multitier model of refugee mental health and psychosocial support in resettlement: Toward trauma-informed and culture-informed systems of care. Psychol. Serv. 2021, 18, 345. [Google Scholar] [CrossRef]
- Bailey, C.; McIntyre, E.; Arreola, A.; Venta, A. What Are We Missing? How Language Impacts Trauma Narratives. J. Child Adolesc. Trauma 2020, 13, 153–161. [Google Scholar] [CrossRef]
- Dinbabo, M.F.; Badewa, A.; Yeboah, C. Socio-Economic Inequity and Decision-Making under Uncertainty: West African Migrants’ Journey across the Mediterranean to Europe. Soc. Incl. 2021, 9, 216–225. [Google Scholar] [CrossRef]
- Bokore, N. Suffering in silence: A Canadian-Somali case study. J. Soc. Work Pract. 2013, 27, 95–113. [Google Scholar] [CrossRef]


{kind=link}
| Resource | Type of Article | Specific Methods | Age Group and Category | Location of Studies | Main Findings/Recommendations |
|---|---|---|---|---|---|
| [22] | Review | USA and Canada |
| ||
| [23] | Review | Thematic review | Youth and Families | Chicago |
|
| [24] | Quantitative | 1 Multivariable linear regressions 2 Moderated regressions | 20–70 years old | USA |
|
| [25] | Conventional content analysis; Retrospective content analysis | USA |
| ||
| [26] | Review | Narrative Review | USA and other Western industrialized countries |
| |
| [27] | Quantitative | Cross-sectional study | Pregnant women who are 18 years and above | Atlanta, GA |
|
| [28] | Quantitative | Cross-sectional study | Adults | Massachusetts |
|
| [29] | Review | Narrative Review | Virginia |
| |
| [30] | Qualitative | Interviews | Youth 16–21 years |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mbamba, C.R.; Asare, J.L.; Gyimah, C. A Preliminary Scoping Review of Trauma Recovery Pathways among Refugees in the United States. Trauma Care 2022, 2, 579-588. https://doi.org/10.3390/traumacare2040048
Mbamba CR, Asare JL, Gyimah C. A Preliminary Scoping Review of Trauma Recovery Pathways among Refugees in the United States. Trauma Care. 2022; 2(4):579-588. https://doi.org/10.3390/traumacare2040048
Chicago/Turabian StyleMbamba, Crispin Rakibu, Jennifer Litela Asare, and Clinton Gyimah. 2022. "A Preliminary Scoping Review of Trauma Recovery Pathways among Refugees in the United States" Trauma Care 2, no. 4: 579-588. https://doi.org/10.3390/traumacare2040048