
Heterotopic Ossification after a Prolonged Course of COVID-19: A Case Report and Review of the Literature

 , and
, and
Abstract
:1. Introduction
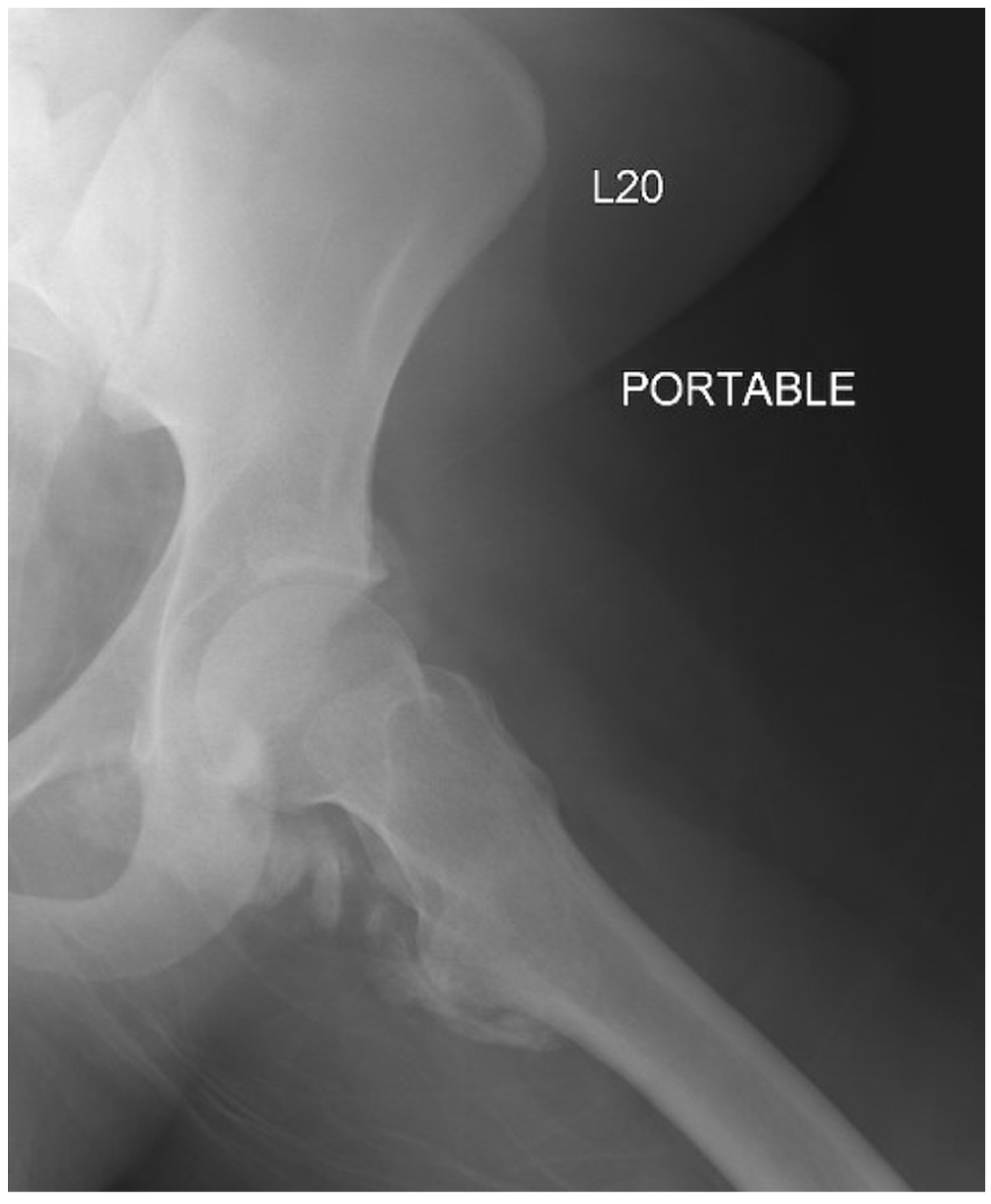
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meyers, C.; Lisiecki, J.; Miller, S. Heterotopic Ossification: A Comprehensive Review. JBMR Plus 2019, 3, e10172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, C.; Haustrate, M.A.; Nisolle, J.F.; Deltombe, T. Heterotopic ossification in COVID-19: A series of 4 cases. Ann. Phys. Rehabil. Med. 2020, 63, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, K.; Loder, S.; Agarwal, S. Heterotopic Ossification: Basic-Science Principles and Clinical Correlates. J. Bone Jt. Surg. Am. 2015, 97, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Grgurevic, L.; Novak, R.; Hrkac, S.; Salai, G.; Grazio, S. Post-COVID-19 exacerbation of fibrodysplasia ossificans progressiva with multiple flare-ups and extensive heterotopic ossification in a 45-year-old female patient. Rheumatol. Int. 2021, 41, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- de l’Escalopier, N.; Mathieu, L.; Duret, C.; Banzet, S.; Genet, F.; Salga, M. Re: “High prevalence of heterotopic ossification in critically ill patients with severe COVID-19” by Stoira et al. Clin. Microbiol. Infect. 2021, 27, 1051–1052. [Google Scholar] [CrossRef] [PubMed]
- DeBaun, M.R.; Ziino, C.; LaPrade, C.; Pun, S.; Avedian, R.S.; Bellino, M.J. An anatomic classification for heterotopic ossification about the hip. J. Orthop. 2020, 21, 228–231. [Google Scholar] [CrossRef]
- Jensen, L.L.; Halar, E.; Little, J.W.; Brooke, M.M. Neurogenic heterotopic ossification. Am. J. Phys. Med. 1987, 66, 351–363. [Google Scholar]
- Clements, N.C.; Jr Camilli, A.E. Heterotopic Ossification Complicating Critical Illness. CHEST 1993, 104, 1526–1528. [Google Scholar] [CrossRef] [Green Version]
- Christakou, A.; Alimatiri, M.; Kouvarakos, A. Heterotopic ossification in critical ill patients: A review. Int. J. Physiother. Res. 2013, 1, 188–195. [Google Scholar]
- McCarthy, E.F.; Sundaram, M. Heterotopic ossification: A review. Skelet. Radiol. 2005, 34, 609–619. [Google Scholar] [CrossRef]
- Aziz, A.; Choudhari, R.; Alexander, A.J.; Allam, E. Heterotopic ossification post COVID-19: Report of two cases. Radiol Case Rep. 2021, 16, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.F. Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Front Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, T.; Zhang, J.; Yang, Y. The role of interleukin-6 in monitoring severe case of coronavirus disease 2019. EMBO Mol. Med. 2020, 12, e12421. [Google Scholar] [CrossRef]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- Cholok, D.; Chung, M.T.; Ranganathan, K. Heterotopic ossification and the elucidation of pathologic differentiation. Bone 2018, 109, 12–21. [Google Scholar] [CrossRef]
- Liu, J.; Luther, L.; Dwivedi, S.; Evans, A.R. Long-term Orthopedic Manifestations of COVID-19: Heterotopic Ossification and Digital Necrosis. R. I. Med. J. 2022, 105, 31–35. [Google Scholar]
- Stoira, E.; Elzi, L.; Puligheddu, C.; Garibaldi, R.; Voinea, C.; Chiesa, A.F.; Collaborators. High prevalence of heterotopic ossification in critically ill patients with severe COVID-19. Clin. Microbiol. Infect. 2021, 27, 1049–1050. [Google Scholar] [CrossRef]
- Barbato, M.; D’Angelo, E.; Di Loreto, G. Adherence to routine use of pharmacological prophylaxis of heterotopic ossification after total hip arthroplasty: Results from an Italian multicenter, prospective, observational survey. J. Orthop. Traumatol. 2012, 13, 63–67. [Google Scholar] [CrossRef] [Green Version]
- Anglen, J.O.; Moore, K.D. Prevention of Heterotopic Bone Formation After Acetabular Fracture Fixation by Single-Dose Radiation Therapy: A Preliminary Report. J. Orthop. Trauma. 1996, 10, 258–263. [Google Scholar] [CrossRef]
- Geller, J.S.; Allegra, P.R.; Seldon, C.S. Primary Versus Secondary Radiotherapy for Heterotopic Ossification Prevention About the Elbow. J. Orthop. Trauma. 2022, 36, e56–e61. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R.W.; Mehta, S.; Aubut, J.L. A systematic review of the therapeutic interventions for heterotopic ossification after spinal cord injury. Spinal. Cord. 2010, 48, 512–521. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Stage | Description |
|---|---|
| I | Bone islands within the soft tissues |
| II | Bone spurs from the pelvis or proximal end of the femur, with at least 1 cm between opposing bone surfaces |
| III | Bone spurs from the pelvis and/or proximal end of femur, with <1 cm between opposing bone surfaces |
| IV | Apparent bone ankylosis of the hip |
| Patient | Age | Gender | LOS (Days) | Mechanical Ventilation (Days) | Comorbidities | HO Location | Laterality |
|---|---|---|---|---|---|---|---|
| 1 | 64 | Male | - | 26 | HTN, Afib | Hip | Bilateral |
| 2 | 73 | Male | - | 27 | HTN, COPD | Hip | Left |
| 3 | 74 | Male | - | 30 | HTN, COPD | Hip | Left |
| 4 | 39 | Male | - | 28 | Schizophrenia, Bipolar, Etoh abuse | Shoulder | Bilateral |
| 5 | 51 | Female | 47 | - | HTN, T2DM | Shoulder | Bilateral |
| 6 | 43 | Female | 33 | - | HTN | Shoulder | Right |
| 7 | 45 | Female | 0 | 0 | FOP | Neck | Left |
| 8 | 23 | Female | 81 | - | Postpartum | Knee | Left |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milner, J.E.; Schwartz, E.C.; Geller, J.S.; Constantinescu, D.; Allegra, P.R.; Trapana, J.E.; Vilella, F.E. Heterotopic Ossification after a Prolonged Course of COVID-19: A Case Report and Review of the Literature. Trauma Care 2022, 2, 550-555. https://doi.org/10.3390/traumacare2040045
Milner JE, Schwartz EC, Geller JS, Constantinescu D, Allegra PR, Trapana JE, Vilella FE. Heterotopic Ossification after a Prolonged Course of COVID-19: A Case Report and Review of the Literature. Trauma Care. 2022; 2(4):550-555. https://doi.org/10.3390/traumacare2040045
Chicago/Turabian StyleMilner, Jacob E., Ean C. Schwartz, Joseph S. Geller, David Constantinescu, Paul R. Allegra, Justin E. Trapana, and Fernando E. Vilella. 2022. "Heterotopic Ossification after a Prolonged Course of COVID-19: A Case Report and Review of the Literature" Trauma Care 2, no. 4: 550-555. https://doi.org/10.3390/traumacare2040045