
Exploring Mindful Self-Care as a Potential Mediator between Compassion Satisfaction and Compassion Fatigue among Student Services Professionals


Abstract
:1. Introduction
2. Materials and Methods
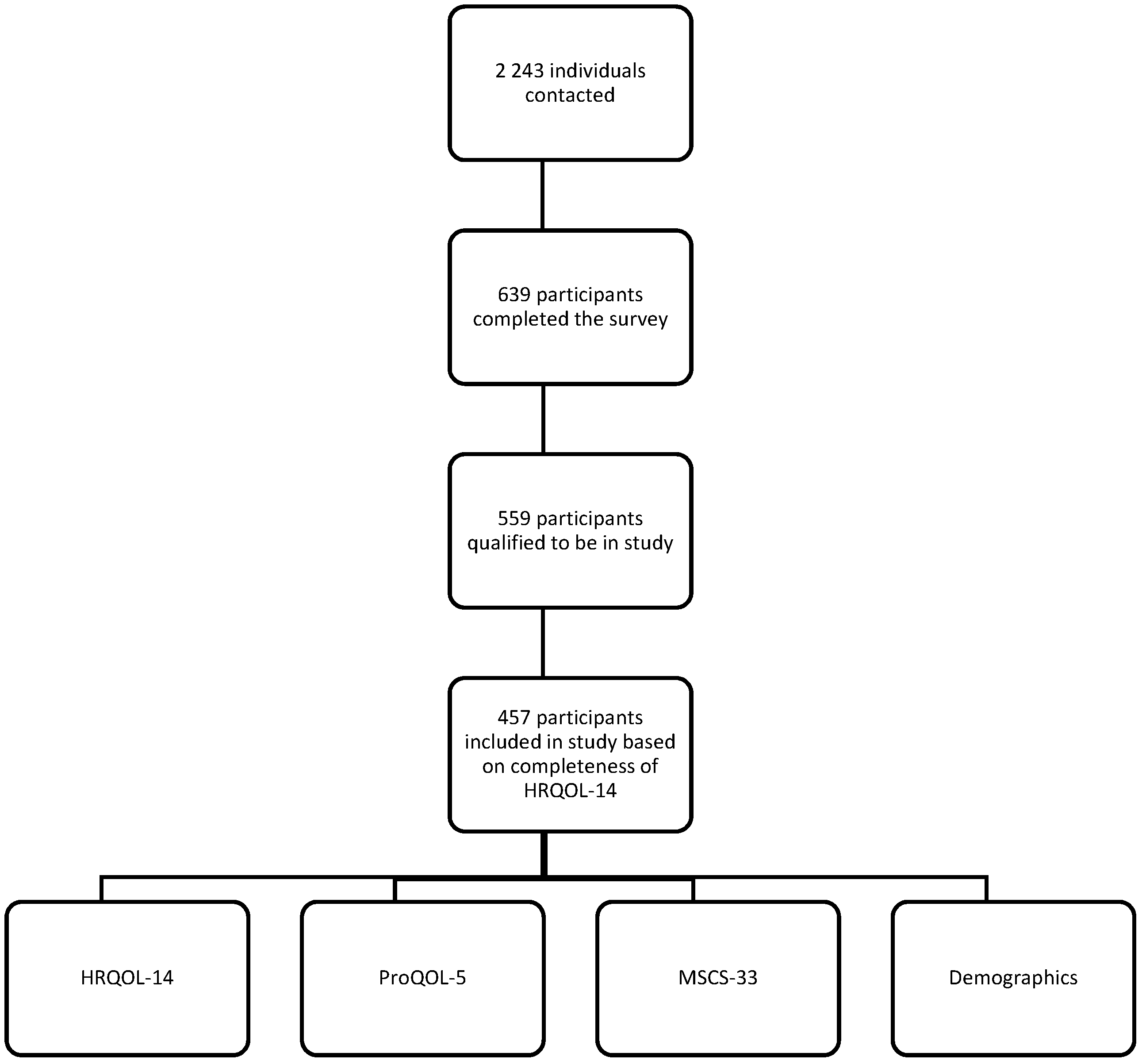
2.1. Participants
2.2. Materials
2.2.1. Compassion Satisfaction and Compassion Fatigue
2.2.2. Mindful Self-Care
2.2.3. Health-Related Quality of Life
2.2.4. Demographic and Role Variables
2.3. Data Collection
2.4. Data Analysis
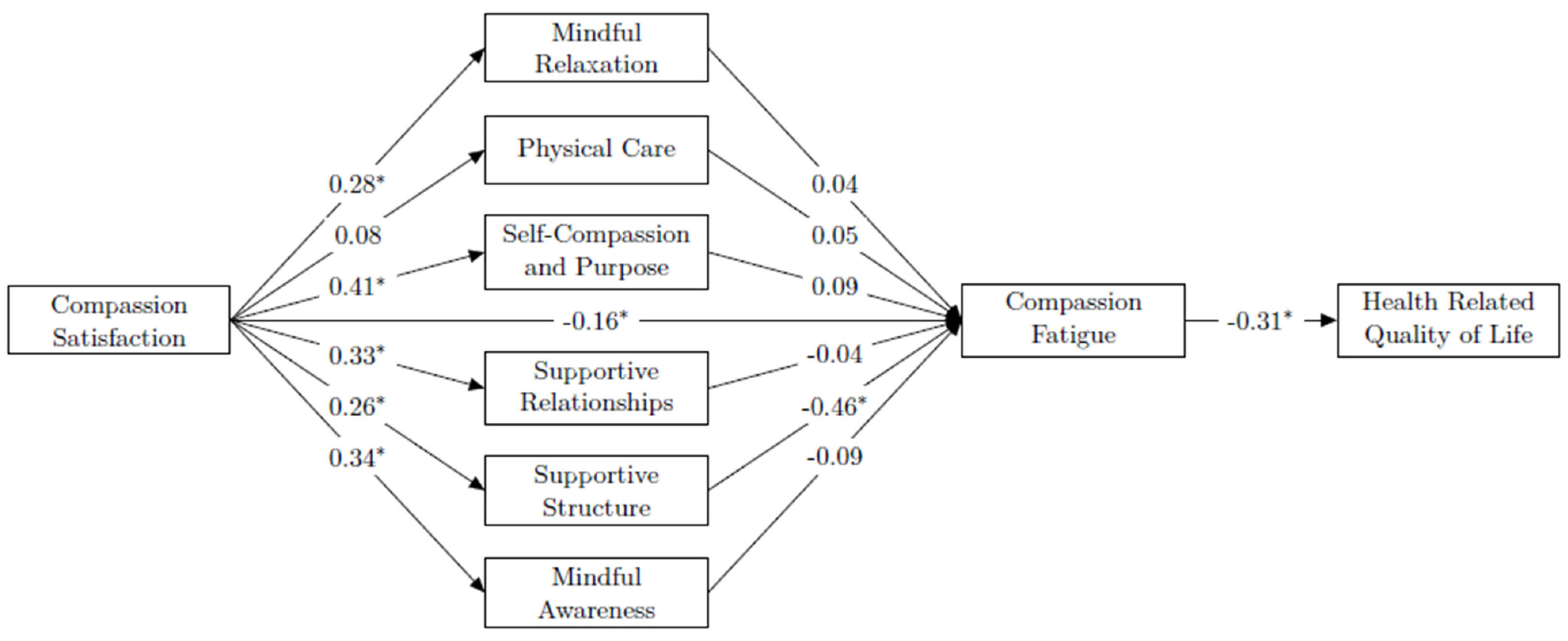
Measurement of the Hypothesized Model
3. Results
3.1. Descriptive Analyses
3.2. Model Estimation
3.2.1. Model 1
3.2.2. Model 2
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Read, J.P.; Ouimette, P.; White, J.; Colder, C.; Farrow, S. Rates of DSM-IV-TR Trauma Exposure and Posttraumatic Stress Disorder Among Newly Matriculated College Students. Psychol. Trauma 2011, 3, 148–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson Preston, P.; Peterson, H.; Sanchez, D.; Corral Carlos, A.; Reed, A. Serving students takes a toll: Self-care, health, and professional quality of life. J. Stud. Aff. Res. Pract. 2021, 58, 163–178. [Google Scholar] [CrossRef]
- Burke, M.G.; Dye, L.; Hughey, A.W. Teaching Mindfulness for the Self-Care and Well-Being of Student Affairs Professionals. Coll. Stud. Aff. J. 2016, 34, 93–107. [Google Scholar] [CrossRef] [Green Version]
- Singer, T.; Klimecki, O.M. Empathy and compassion. Curr. Biol. 2014, 24, R875–R878. [Google Scholar] [CrossRef] [Green Version]
- Pronk, N.P.; Katz, A.S.; Gallagher, J.; Austin, E.; Mullen, D.; Lowry, M.; Kottke, T.E. Adherence to optimal lifestyle behaviors is related to emotional health indicators among employees. Popul. Health Manag. 2011, 14, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Stamm, B.H. The Concise ProQOL Manual. Available online: https://programs.caringsafely.org/wp-content/uploads/2018/01/ProQOL_Concise_2ndEd_12-2010.pdf (accessed on 1 May 2020).
- Stoewen, D.L. Moving from compassion fatigue to compassion resilience Part 2: Understanding compassion fatigue. Can. Vet. J. 2019, 60, 1004–1006. [Google Scholar] [PubMed]
- Figley, C.R. Compassion Fatigue: Secondary Traumatic Stress Disorders from Treating the Traumatized; Routledge, Taylor & Francis Group: Philadelphia, PA, USA, 1995. [Google Scholar]
- Magnavita, N. Work-related psychological injury is associated with metabolic syndrome components in apparently healthy workers. PLoS ONE 2015, 10, e0130944. [Google Scholar] [CrossRef] [PubMed]
- Newell, J.M.; Nelson-Gardell, D.; MacNeil, G. Clinician Responses to Client Traumas: A Chronological Review of Constructs and Terminology. Trauma Violence Abus. 2016, 17, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Lynch, R.J.; Glass, C.R. The Development of the Secondary Trauma in Student Affairs Professionals Scale (STSAP). J. Stud. Aff. Res. Pract. 2018, 56, 1–18. [Google Scholar] [CrossRef]
- Stamm, B.H. Measuring compassion satisfaction as well as fatigue: Developmental history of the compassion satisfaction and fatigue test. In Treating Compassion Fatigue; Figley, C.R., Ed.; Brunner-Routledge: New York, NY, USA, 2002; pp. 107–119. [Google Scholar]
- Raimondi, T.P. Compassion Fatigue in Higher Education: Lessons from Other Helping Fields. Change: Mag. High. Learn. 2019, 51, 52–58. [Google Scholar] [CrossRef]
- Pines, A.; Maslach, C. Characteristics of staff burnout in mental health settings. Psychiatr. Serv. 1978, 29, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Mullen, P.R.; Malone, A.; Denney, A.; Dietz, S.S. Job Stress, Burnout, Job Satisfaction, and Turnover Intention Among Student Affairs Professionals. Coll. Stud. Aff. J. 2018, 36, 94–108. [Google Scholar] [CrossRef]
- Marshall, S.M.; Gardner, M.M.; Hughes, C.; Lottery, U. Attrition from Student Affairs: Perspectives from Those Who Exited the Profession. J. Stud. Aff. Res. Pract. 2016, 53, 146–159. [Google Scholar] [CrossRef]
- Alkema, K.; Linton, J.M.; Davies, R. A study of the relationship between self-care, compassion satisfaction, compassion fatigue, and burnout among hospice professionals. J. Soc. Work. End—Life Palliat. Care 2008, 4, 101–119. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, J.M. Risk of compassion fatigue and burnout and potential for compassion satisfaction among employee assistance professionals: Protecting the workforce. Traumatology 2012, 18, 64–72. [Google Scholar] [CrossRef]
- Dasan, S.; Gohil, P.; Cornelius, V.; Taylor, C. Prevalence, causes and consequences of compassion satisfaction and compassion fatigue in emergency care: A mixed-methods study of UK NHS Consultants. Emerg. Med. J. 2015, 32, 588–594. [Google Scholar] [CrossRef] [Green Version]
- Vilardaga, R.; Luoma, J.B.; Hayes, S.C.; Pistorello, J.; Levin, M.E.; Hildebrandt, M.J.; Kohlenberg, B.; Roget, N.A.; Bond, F. Burnout among the addiction counseling workforce: The differential roles of mindfulness and values-based processes and work-site factors. J. Subst. Abus. Treat. 2011, 40, 323–335. [Google Scholar] [CrossRef] [Green Version]
- Denyes, M.J.; Orem, D.E.; Bekel, G. SozWiss. Self-care: A foundational science. Nurs. Sci. Q. 2001, 14, 48–54. [Google Scholar] [CrossRef]
- Bercier, M.L.; Maynard, B.R. Interventions for Secondary Traumatic Stress with Mental Health Workers. Res. Soc. Work. Pract. 2014, 25, 81–89. [Google Scholar] [CrossRef]
- Bloomquist, K.R.; Wood, L.; Friedmeyer-Trainor, K.; Kim, H.-W. Self-care and Professional Quality of Life: Predictive Factors among MSW Practitioners. Adv. Soc. Work. 2016, 16, 292–311. [Google Scholar] [CrossRef]
- Bressi, S.K.; Vaden, E.R. Reconsidering Self Care. Clin. Soc. Work. J. 2016, 45, 33–38. [Google Scholar] [CrossRef]
- Butler, L.D.; Mercer, K.A.; McClain-Meeder, K.; Horne, D.M.; Dudley, M. Six domains of self-care: Attending to the whole person. J. Hum. Behav. Soc. Environ. 2019, 29, 107–124. [Google Scholar] [CrossRef]
- Newell, J.M. An Ecological Systems Framework for Professional Resilience in Social Work Practice. Soc. Work 2019, 65, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Harmon-Darrow, C.; Frey, J.J. Rethinking professional quality of life for social workers: Inclusion of ecological self-care barriers. J. Hum. Behav. Soc. Environ. 2019, 29, 11–25. [Google Scholar] [CrossRef]
- Harker, R.; Pidgeon, A.M.; Klaassen, F.; King, S. Exploring resilience and mindfulness as preventative factors for psychological distress burnout and secondary traumatic stress among human service professionals. Work 2016, 54, 631–637. [Google Scholar] [CrossRef]
- Rees, C.S.; Eley, R.; Osseiran-Moisson, R.; Francis, K.; Cusack, L.; Heritage, B.; Hegney, D. Individual and environmental determinants of burnout among nurses. J. Health Serv. Res. Policy 2019, 24, 191–200. [Google Scholar] [CrossRef]
- Cook-Cottone, C.P. Mindfulness and Yoga for Self-Regulation: A Primer for Mental Health Professionals; Springer Publishing Company: New York, NY, USA, 2015. [Google Scholar]
- Hotchkiss, J.T. Mindful Self-Care and Secondary Traumatic Stress Mediate a Relationship between Compassion Satisfaction and Burnout Risk among Hospice Care Professionals. Am. J. Hosp. Palliat. Med. 2018, 35, 1099–1108. [Google Scholar] [CrossRef]
- Hotchkiss, J.T.; Lesher, R. Factors Predicting Burnout Among Chaplains: Compassion Satisfaction, Organizational Factors, and the Mediators of Mindful Self-Care and Secondary Traumatic Stress. J. Pastor. Care Couns. 2018, 72, 86–98. [Google Scholar] [CrossRef]
- Guthrie, V.L.; Woods, E.; Cusker, C.; Gregory, M. A Portrait of Balance: Personal and Professional Balance among Student Affairs Educators. Coll. Stud. Aff. J. 2005, 24, 110–127. [Google Scholar]
- Syed, I.U.B. Diet, physical activity, and emotional health: What works, what doesn’t, and why we need integrated solutions for total worker health. BMC Public Health 2020, 20, 152. [Google Scholar] [CrossRef] [Green Version]
- Feng, X.; Mosimah, C.I.; Sizemore, G.; Goyat, R.; Dwibedi, N. Impact of mindful self-care and perceived stress on the health-related quality of life among young-adult students in West Virginia. J. Hum. Behav. Soc. Environ. 2019, 29, 26–36. [Google Scholar] [CrossRef]
- Ullman, J.B.; Bentler, P.M. Structural Equation Modeling. In Handbook of Psychology, 2nd ed.; Tabachnick, B.G., Fidell, L.S., Eds.; Pearson: London, UK, 2012. [Google Scholar]
- Cohen, J. A Power Primer. Sychological Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Heritage, B.; Rees, C.S.; Hegney, D.G. The ProQOL-21: A revised version of the Professional Quality of Life (ProQOL) scale based on Rasch analysis. PLoS ONE 2018, 13, e0193478. [Google Scholar] [CrossRef] [PubMed]
- Cook-Cottone, C.P.; Guyker, W.M. The Development and Validation of the Mindful Self-Care Scale (MSCS): An Assessment of Practices that Support Positive Embodiment. Mindfulness 2018, 9, 161–175. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Health-related quality-of-life measures—United States, 1993. Morb. Mortal. Wkly. Rep. 1995, 44, 195–200. [Google Scholar]
- Yin, S.; Njai, R.; Barker, L.; Siegel, P.Z.; Liao, Y. Summarizing health-related quality of life (HRQOL): Development and testing of a one-factor model. Popul. Health Metr. 2016, 14, 22. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing, Version = 1.9.12. R Foundation for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 1 January 2020).
- Multivariate Software Inc. EQS-Structural Equation Modeling Software Software [Computer Software]. Available online: http://www.mvsoft.com (accessed on 1 May 2020).
- Yuan, K.H.; Lambert, P.L.; Fouladi, R.T. Mardia’s multivariate kurtosis with missing data. Multivar. Behav. Res. 2004, 39, 413–437. [Google Scholar] [CrossRef]
- Little, R.J.A. A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Beaujean, A.A. BaylorEdPsych: R Package for Baylor University Educational Psychology Quantitative Courses, R Package Version 0.5. Available online: http://CRAN.R-project.org/package=BaylorEdPsych (accessed on 1 May 2020).
- Awa, W.L.; Plaumann, M.; Walter, U. Burnout prevention: A review of intervention programs. Patient Educ. Couns. 2010, 78, 184–190. [Google Scholar] [CrossRef]
- Ruiz-Fernandez, M.D.; Ortega-Galan, A.M.; Fernandez-Sola, C.; Hernandez-Padilla, J.M.; Granero-Molina, J.; Ramos-Pichardo, J.D. Occupational Factors Associated with Health-Related Quality of Life in Nursing Professionals: A Multi-Centre Study. Int. J. Environ. Res. Public Health 2020, 17, 982. [Google Scholar] [CrossRef]
- Lynch, R.J. The Development and Validation of the Secondary Trauma in Resident Assistants Scale. J. Coll. Univ. Stud. Hous. 2017, 44, 10–29. [Google Scholar]
- Maslach, C. Understanding Burnout: Definitional Issues in Analyzing a Complex Phenomenon; Paine, W.S., Ed.; Sage: Beverly Hills, CA, USA, 1982. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | % | N |
|---|---|---|
| Gender Identity | 412 | |
| Male/Transgender male | 18 | 75 |
| Female/Transgender female | 78 | 232 |
| Non-Binary 1 | 2 | 10 |
| Prefer not to state | 1 | 4 |
| Race | 395 | |
| White | 53 | 210 |
| Black or African American | 9 | 35 |
| Asian | 9 | 37 |
| Other 2 | 11 | 43 |
| Multiracial | 7 | 28 |
| Prefer not to say | 11 | 42 |
| LGBTQIA+ Status 3 | 412 | |
| Yes | 25 | 102 |
| Age | 413 | |
| 18–25 | 10 | 42 |
| 26–34 | 38 | 158 |
| 35–44 | 26 | 108 |
| 45–54 | 15 | 61 |
| 55–64 | 8 | 34 |
| 65 or older | 1 | 4 |
| Prefer not to say | 1 | 6 |
| Marital Status | 412 | |
| Single, never married | 43 | 176 |
| Married or domestic partnership | 49 | 200 |
| Widowed | 7 | 29 |
| Divorced | 2 | 7 |
| Separated | 43 | 176 |
| Variable | % | N |
|---|---|---|
| Primary Role on Campus | 457 | |
| Full or part-time staff | 71 | 324 |
| Administrator | 16 | 71 |
| Full or part-time faculty 1 | 7 | 34 |
| Student | 5 | 23 |
| I do not fit into any of these roles. | 1 | 5 |
| Top Primary Student Service Areas | ||
| Housing and Residential Life | 12 | 56 |
| Counseling and Psychological Services | 11 | 51 |
| Academic Advising | 10 | 46 |
| No Formal Role 2 | 10 | 46 |
| Role Level for Primary Student Service Area | 413 | |
| Administrator | 10 | 42 |
| Programmatic/Service staff | 38 | 158 |
| Administrative support staff | 26 | 108 |
| Education | ||
| Associate Degree or lower 3 | 7 | 32 |
| Bachelor’s Degree | 25 | 105 |
| Master’s Degree | 54 | 225 |
| Doctoral Degree or other Professional Degree | 12 | 51 |
| Mean (S.D.) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Compassion Fatigue | 24.04 (7.31) | 1.00 | ||||||||
| 2. Compassion Satisfaction | 26.91 (5.41) | −0.31 ** | 1.00 | |||||||
| 3. Mindful Relaxation | 17.37 (4.85) | −0.20 ** | 0.30 ** | 1.00 | ||||||
| 4. Physical Care | 21.29 (5.98) | −0.16 ** | 0.09 * | 0.38 ** | 1.00 | |||||
| 5. Self-Compassion and Purpose | 19.83 (5.38) | −0.16 ** | 0.42 ** | 0.49 ** | 0.23 ** | 1.00 | ||||
| 6. Supportive Relationships | 19.38 (4.04) | −0.30 ** | 0.32 ** | 0.35 ** | 0.14 ** | 0.41 ** | 1.00 | |||
| 7. Supportive Structure | 14.27 (3.33) | −0.52 ** | 0.26 ** | 0.41 ** | 0.39 ** | 0.31 ** | 0.42 ** | 1.00 | ||
| 8. Mindful Awareness | 13.65 (3.70) | −0.33 ** | 0.34 ** | 0.38 ** | 0.33 ** | 0.60 ** | 0.37 ** | 0.54 ** | 1.00 | |
| 9. HRQOL | 10.53 (9.18) | −0.31 ** | 0.12 * | 0.13 ** | 0.05 | 0.11 * | 0.16 ** | 0.25 ** | 0.24 ** | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preston, P.J.; Sanchez, D.; Preston, K.S.J. Exploring Mindful Self-Care as a Potential Mediator between Compassion Satisfaction and Compassion Fatigue among Student Services Professionals. Trauma Care 2022, 2, 535-549. https://doi.org/10.3390/traumacare2040044
Preston PJ, Sanchez D, Preston KSJ. Exploring Mindful Self-Care as a Potential Mediator between Compassion Satisfaction and Compassion Fatigue among Student Services Professionals. Trauma Care. 2022; 2(4):535-549. https://doi.org/10.3390/traumacare2040044
Chicago/Turabian StylePreston, Portia Jackson, Delia Sanchez, and Kathleen Suzanne Johnson Preston. 2022. "Exploring Mindful Self-Care as a Potential Mediator between Compassion Satisfaction and Compassion Fatigue among Student Services Professionals" Trauma Care 2, no. 4: 535-549. https://doi.org/10.3390/traumacare2040044