
The Efficacy of Honey Compared to Silver Sulfadiazine for Burn Wound Dressing in Superficial and Partial Thickness Burns—A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias
2.6. Statistical Analysis
3. Results
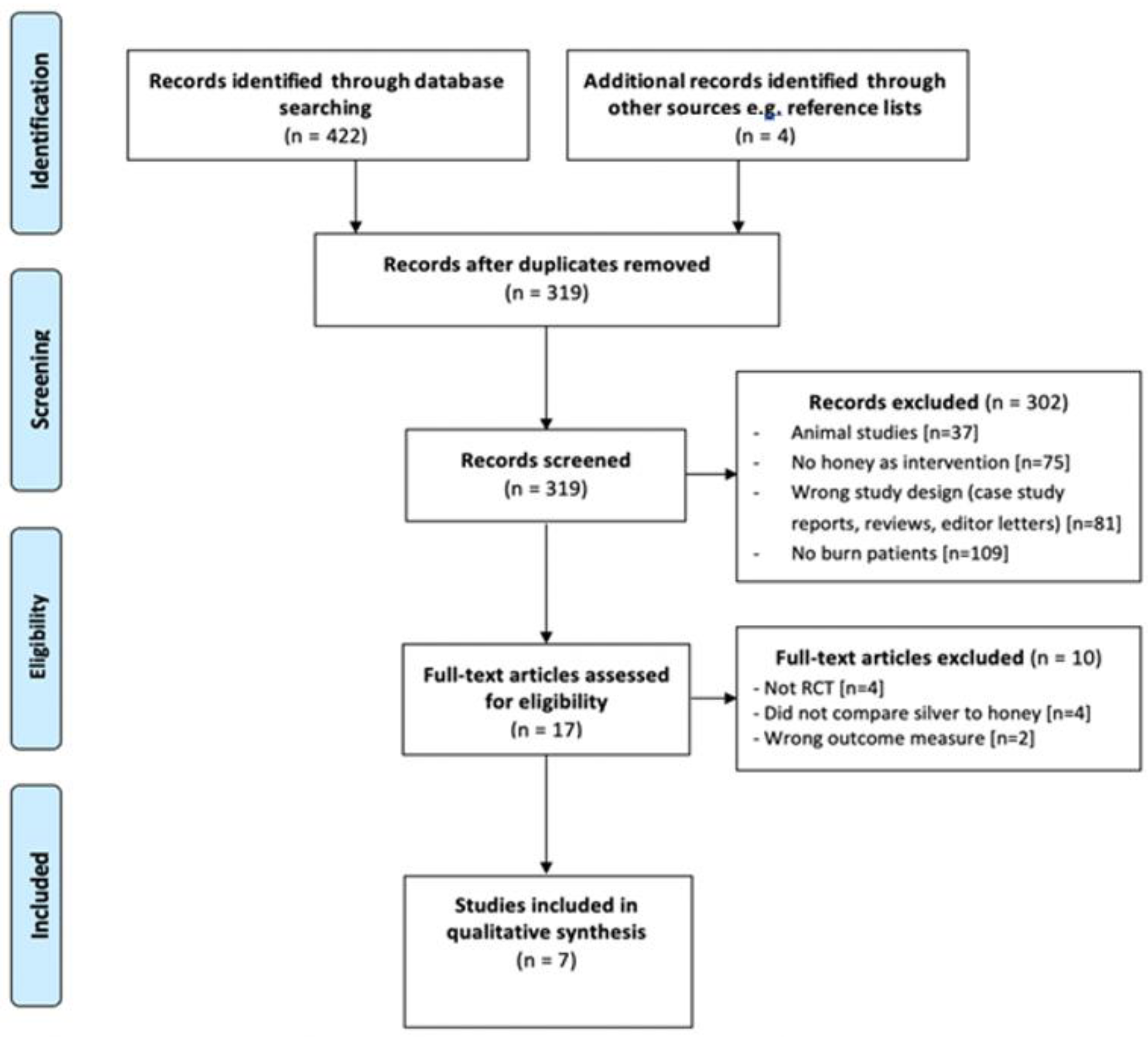
3.1. Study Selection
3.2. Study Characteristics
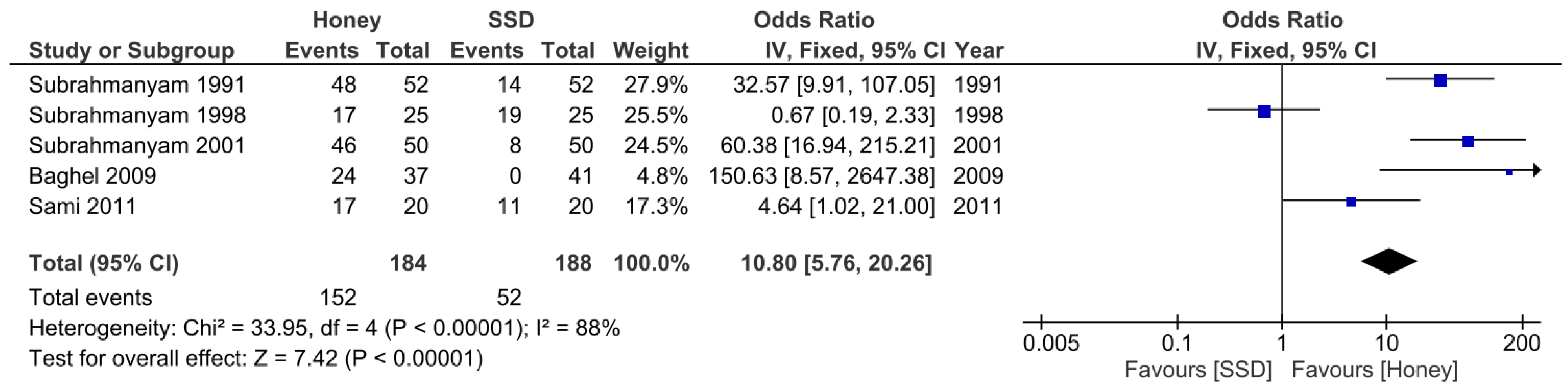
3.3. Results of Individual Studies—Primary Outcomes
3.4. Results of Individual Studies—Secondary Outcome
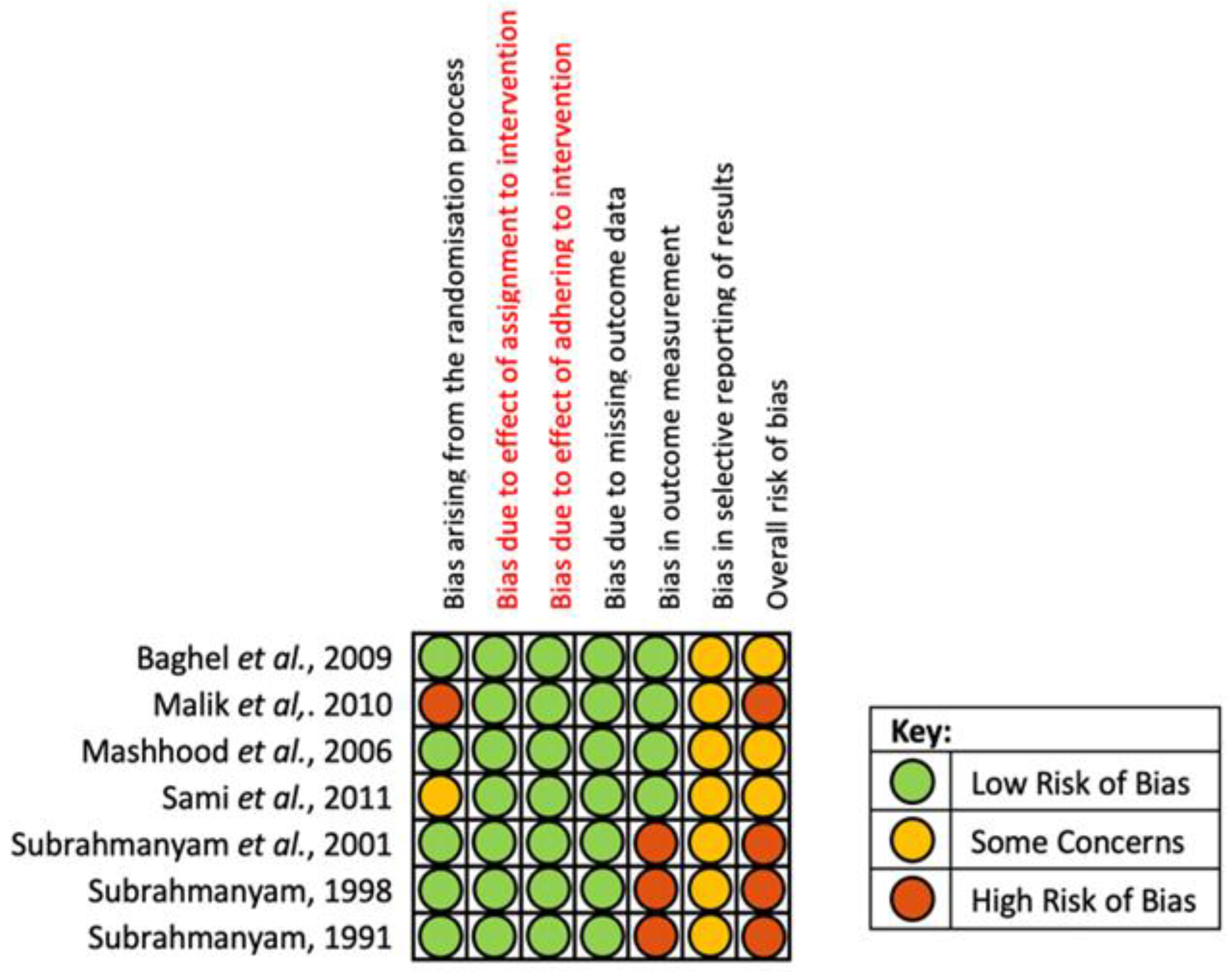
3.5. Risk of Bias in Studies
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tolles, J. Emergency department management of patients with thermal burns. Emerg. Med. Pract. 2018, 20, 1–24. [Google Scholar]
- WHO Burns Information Facts Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/burns (accessed on 15 July 2022).
- Toussaint, J.; Singer, A.J. The evaluation and management of thermal injuries: 2014 update. Clin. Exp. Emerg. Med. 2014, 1, 8–18. [Google Scholar] [CrossRef]
- NHS National Burn Care Referral Guidance. Available online: https://www.britishburnassociation.org/wp-content/uploads/2018/02/National-Burn-Care-Referral-Guidance-2012.pdf (accessed on 14 July 2022).
- Osuka, A.; Ogura, H.; Ueyama, M.; Shimazu, T.; Lederer, J.A. Immune response to traumatic injury: Harmony and discordance of immune system homeostasis. Acute Med. Surg. 2014, 1, 63–69. [Google Scholar] [CrossRef]
- Dvorak, J.E.; Ladhani, H.A.; Claridge, J.A. Review of Sepsis in Burn Patients in 2020. Surg. Infect. (Larchmt) 2021, 22, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Rech, M.A.; Mosier, M.J.; McConkey, K.; Zelisko, S.; Netzer, G.; Kovacs, E.J.; Afshar, M. Outcomes in burn-injured patients who develop sepsis. J. Burn Care Res. 2019, 40, 269–273. [Google Scholar] [CrossRef]
- Spronk, I.; Van Loey, N.E.E.; van der Vlies, C.H.; Haagsma, J.A.; Polinder, S.; van Baar, M.E. Activity Impairment, Work Status, and Work Productivity Loss in Adults 5–7 Years After Burn Injuries. J. Burn Care Res. 2022, 43, 256–262. [Google Scholar] [CrossRef]
- AbdelWahab, M.E.; Sadaka, M.S.; Elbana, E.A.; Hendy, A.A. Evaluation of prognostic factors affecting length of stay in hospital and mortality rates in acute burn patients. Ann. Burns Fire Disasters 2018, 31, 83–88. [Google Scholar] [PubMed]
- Ross, E.; Crijns, T.J.; Ring, D.; Coopwood, B. Social factors and injury characteristics associated with the development of perceived injury stigma among burn survivors. Burns 2021, 47, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Guest, J.F.; Fuller, G.W.; Edwards, J. Cohort study evaluating management of burns in the community in clinical practice in the UK: Costs and outcomes. BMJ Open. 2020, 10, e035345. [Google Scholar] [CrossRef] [Green Version]
- Pankhurst, S.; Pochkhanawala, T. Wound care. In Burn Trauma Management and Nursing Care, 2nd ed.; Bosworth-Bousfield, C., Ed.; Whurr Publishers: Chicester, UK, 2002; pp. 81–108. [Google Scholar]
- Selig, H.F.; Lumenta, D.B.; Giretzlehner, M.; Jeschke, M.G.; Upton, D.; Kamolz, L.P. The properties of an “ideal” burn wound dressing--what do we need in daily clinical practice? Results of a worldwide online survey among burn care specialists. Burns 2012, 38, 960–966. [Google Scholar] [CrossRef]
- Carta, T.; Gawaziuk, J.P.; Diaz-Abele, J.; Liu, S.; Jeschke, M.; Logsetty, S. Properties of an ideal burn dressing: A survey of burn survivors and front-line burn healthcare providers. Burns 2019, 45, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.; Tanideh, N.; Kohanteb, J.; Ghodrati, Z.; Mehrabani, D.; Yarmohammadi, H. Comparison between Alpha and silver sulfadiazine ointments in treatment of Pseudomonas infections in 3rd degree burns. Int. J. Surg. 2007, 5, 23–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, A.; Dissemond, J.; Kim, S.; Willy, C.; Mayer, D.; Papke, R.; Tuchmann, F.; Assadian, O. Consensus on wound antisepsis: Update 2018. Skin Pharmacol. Physiol. 2018, 31, 28–58. [Google Scholar] [CrossRef] [PubMed]
- Qian, L.W.; Fourcaudot, A.B.; Leung, K.P. Silver sulfadiazine retards wound healing and increases hypertrophic scarring in a rabbit ear excisional wound model. J. Burn Care Res. 2017, 38, e418–e422. [Google Scholar] [CrossRef] [PubMed]
- Poon, V.K.; Burd, A. In vitro cytotoxity of silver: Implication for clinical wound care. Burns 2004, 30, 140–147. [Google Scholar] [CrossRef]
- Mandal, M.D.; Mandal, S. Honey: Its medicinal property and antibacterial activity. Asian Pac. J. Trop. Biomed. 2011, 1, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Cooper, R.A.; Halas, E.; Molan, P.C. The efficacy of honey in inhibiting strains of Pseudomonas aeruginosa from infected burns. J. Burn Care Rehabil. 2002, 23, 366–370. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- PROSPERO International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 17 July 2022).
- Sterne, J.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Baghel, P.S.; Shukla, S.; Mathur, R.K.; Randa, R. A comparative study to evaluate the effect of honey dressing and silver sulfadiazene dressing on wound healing in burn patients. Indian J. Plast. Surg. 2009, 42, 176–181. [Google Scholar] [CrossRef]
- Malik, K.I.; Malik, M.A.; Aslam, A. Honey compared with silver sulphadiazine in the treatment of superficial partial-thickness burns. Int. Wound J. 2010, 7, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Mashhood, A.A.; Khan, T.A.; Sami, A.N. Honey compared with 1% silver sulfadiazine cream in the treatment of superficial and partial thickness burns. J. Pak. Assoc. Dermatol. 2006, 16, 14–19. [Google Scholar]
- Subrahmanyam, M.; Sahapure, A.G.; Nagane, N.S.; Bhagwat, V.R.; Ganu, J.V. Effects of topical application of honey on burn wound healing. Ann. Burn. Fire Disasters 2001, 15, 143–145. [Google Scholar]
- Sami, A.N.; Mehmood, N.; Qureshi, M.A.; Muhammad, A.Q.; Zeeshan, H.K.; Malik, I.A.; Khan, M. Honey Compared With Silver sulphadiazine as Burn Wound Dressing. Ann. Pak. Inst. Med. Sci. 2011, 7, 22–25. [Google Scholar]
- Subrahmanyam, M. A prospective randomised clinical and histological study of superficial burn wound healing with honey and silver sulfadiazine. Burns 1998, 24, 157–161. [Google Scholar] [CrossRef]
- Subrahmanyam, M. Topical application of honey in treatment of burns. Br. J. Surg. 1991, 78, 497–498. [Google Scholar] [CrossRef]
- Barakhbah, A.; Anisah, S.; Agil, S. Honey in the Malay tradition. Malays. J. Med. Sci. 2007, 14, 106. [Google Scholar]
- Marwat, S.K.; Khan, M.A.; Rehman, F.; Khan, K. Medicinal uses of honey (Quranic medicine) and its bee flora from Dera Ismail Khan District, KPK, Pakistan. Pak. J. Pharm. Sci. 2013, 26, 307–314. [Google Scholar] [PubMed]
- Subrahmanyam, M. Topical application of honey for burn wound treatment-an overview. Ann. Burns Fire Disasters 2007, 20, 137–139. [Google Scholar] [PubMed]
- Efem, S.E. Clinical observations on the wound healing properties of honey. Br. J. Surg. 1988, 75, 679–681. [Google Scholar] [CrossRef]
- Nagane, N.S.; Ganu, J.V.; Bhagwat, V.R.; Subramanium, M. Efficacy of topical honey therapy against silver sulphadiazine treatment in burns: A biochemical study. Indian J. Clin. Biochem. 2004, 19, 173–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bang, L.; Buntting, C.; Molan, P. The effect of dilution on the rate of hydrogen peroxide production in honey and its implications for wound healing. J. Altern. Complement. Med. 2003, 9, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandil, A. Healing effect of true floral and false nonfloral honey on medical wounds. J. Drug Res. 1987, 17, 71–75. [Google Scholar]
- Bergman, A.; Yanai, J.; Weiss, J. Acceleration of wound healing by topical application of honey: An animal model. Am J Surg. 1983, 145, 374–376. [Google Scholar] [CrossRef]
- Suguna, L.; Chandrakasan, G.; Ramamoorthy, U.; Joseph, K.T. Influence of honey on biochemical and biophysical parameters of wounds in rats. J. Clin. Biochem. Nutr. 1993, 14, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Suguna, L.; Chandrakasan, G.; Joseph, K.T. Influence of honey on collagen metabolism during wound healing in rats. J. Clin. Biochem. Nutr. 1992, 13, 7–12. [Google Scholar] [CrossRef]
- Deitch, E.A.; Wheelahan, T.M.; Rose, M.P.; Clothier, J.; Cotter, J. Hypertrophic burn scars: Analysis of variables. J. Trauma. 1983, 23, 895–898. [Google Scholar] [CrossRef]
- Karim, K.; Alam, I.; Hasan, N.; Khan, A. The socio-economic factors of burn injuries in children. Burns 1975, 1, 145–148. [Google Scholar] [CrossRef]
- Atiyeh, B.S.; Gunn, S.W.A.; Hayek, S.N. State of the art in burn treatment. World J. Surg. 2005, 29, 131–148. [Google Scholar] [CrossRef]
- Atiyeh, B.S.; Gunn, S.W.A.; Hayek, S.N. Provision of essential surgery in remote and rural areas of developed as well as low- and middle-income countries. Int. J. Surg. 2010, 8, 581–585. [Google Scholar] [CrossRef] [Green Version]
- Ramakrishnan, K.M.; Jayaraman, V. Management of partial-thickness burn wounds by amniotic membrane: A cost-effective treatment in developing countries. Burns 1997, 23, S33–S36. [Google Scholar] [CrossRef]
- Ahuja, R.B.; Bhattacharya, S. Burns in the developing world and burn disasters. BMJ 2004, 329, 447–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keswani, M.H.; Vartak, A.M.; Patil, A.; Davies, J.W. Histological and bacteriological studies of burn wounds treated with boiled potato peel dressings. Burns 1990, 16, 137–143. [Google Scholar] [CrossRef]
- Starley, I.F.; Mohammed, P.; Schneider, G.; Bickler, S.W. The treatment of paediatric burns using topical papaya. Burns 1999, 25, 636–639. [Google Scholar] [CrossRef]
- The CONSORT Statement. Available online: http://www.consort-statement.org/ (accessed on 20 July 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Adult and paediatric patients with superficial or partial thickness burns | Patients with full thickness burns |
| Intervention | Honey dressing | N/A |
| Comparison | SSD cream or dressing | Other treatment modalities (e.g., early excision and grafting) |
| Outcome Measures | Primary outcomes: complete wound healing time, proportion of wounds rendered sterile, Secondary outcome: subjective pain relief | N/A |
| Study Design | Randomised controlled trials | Observational studies, animal studies, reviews, abstracts, case reports or quality improvement projects |
| Study | Location | Patient Population | Mean Age in Years (SD) | Intervention (No. of Subjects) | Control (No. of Subjects) | Duration of Study | Assessment of Complete Wound Healing and Sterility | Outcome Measures |
|---|---|---|---|---|---|---|---|---|
| Baghel et al. 2009 [24] | India | 78 patients with first and second degree burns of less than 50% TBSA | I: 34.5 C: 28.5 | Pure, unprocessed, undiluted honey dressing with sterile gauze everyday (n = 37) | SSD Cream with sterile gauze everyday (n = 41) | 2 months | Clinical observation and wound swab cultures | Wound healing time, time taken to render wounds sterile, proportion of wounds healed |
| Malik et al. 2010 [25] | Pakistan | 150 patients with partial thickness burns less than 40% on two contralateral body sites (e.g., right and left hand) | 28 (15.94) | Langnese honey twice daily (n = 150) | SSD Cream with sterile gauze everyday (n = 150) | Until burn wound fully healed | Clinical observation and wound swab culture | Wound healing time, proportion of wounds healed |
| Mashhood et al. 2006 [26] | Pakistan | 50 patients with superficial and partial thickness burns less than or equal to 15% TBSA | 27.4 | Pure, unprocessed, undiluted honey which was applied once daily with a sterile gauze (n = 25) | 1% SSD once daily (n = 25) | Until burn would healed | Clinical observation and wound swabs for bacterial density and cultures | Wound healing time, time taken to render wounds sterile, pain |
| Subrahmanyam et al. 2001 [27] | India | 100 patients with superficial thickness burns | I: 26.5 (1) C: 25.2 (2) | Undiluted, unprocessed honey dressing replaced once every 2 days (n = 50) | SSD-impregnated gauze dressing replaced every 2 days (n = 50) | Until burn wound healed | Clinical observation and wound swabs for bacterial cultures and sensitivity determinations | Wound healing time, proportion of wounds rendered sterile, subjective relief of pain |
| Sami et al. 2011 [28] | Pakistan | 50 patients with partial thickness thermal burns involving 5–40% TBSA | N/A, range = 1.5–50 | Pure unprocessed undiluted honey applied once daily (n = 25) | 1% SSD cream once daily (n = 25) | 2 months | Clinical observation of degree of epithelisation and wound swabs | Wound healing time, number of wounds rendered sterile, pain relief, cost of treatment per % burn |
| Subrahmanyam et al. 1998 [29] | India | 50 patients with superficial thermal burns involving less than 40% TBSA | I: 25.2 C: 26.4 | Pure unprocessed undiluted honey dressing replaced on alternate days (n = 25) | SSD gauze replaced daily (n = 25) | 1 month | Clinical inspection, biopsies for histological studies and wound swabs | Wound healing time, proportion of wounds rendered sterile |
| Subrahmanyam et al. 1991 [30] | India | 104 patients with superficial thermal burns less than 40% TBSA | N/A, range = 1–65 | Pure unprocessed undiluted honey dressing applied once daily (n = 52) | SSD gauze replaced daily (n = 52) | 2 months | Clinical observation and wound swabs for culture and sensitivity determinations | Wound healing time, proportion of wounds rendered sterile |
| Study | Honey Group Participants | SSD Group Participants | Honey Healing Time (Days ± SD) | SSD Healing Time (Days ± SD) | Mean Difference | p-Value |
|---|---|---|---|---|---|---|
| Baghel et al. 2009 [24] | n = 37 | n = 41 | 18.1 ± NA | 32.6 ± N/A | −14.5 | <0.05 |
| Subrahmanyam et al. 2001 [27] | n = 50 | n = 50 | 15.4 (3.2) | 17.2 (4.3) | −1.8 | <0.001 |
| Subrahmanyam et al. 1998 [29] | n = 25 | n = 25 | 4.92 (3.61) | 8.22 (8.31) | −3.3 | <0.001 |
| Subrahmanyam et al. 1991 [30] | n = 52 | n = 52 | 9.4 (2.3) | 17.2 (3.2) | −7.8 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osman, S.; Umar, H.; Hashmi, Y.; Jawaid, A.; Ahmed, Z. The Efficacy of Honey Compared to Silver Sulfadiazine for Burn Wound Dressing in Superficial and Partial Thickness Burns—A Systematic Review and Meta-Analysis. Trauma Care 2022, 2, 523-534. https://doi.org/10.3390/traumacare2040043
Osman S, Umar H, Hashmi Y, Jawaid A, Ahmed Z. The Efficacy of Honey Compared to Silver Sulfadiazine for Burn Wound Dressing in Superficial and Partial Thickness Burns—A Systematic Review and Meta-Analysis. Trauma Care. 2022; 2(4):523-534. https://doi.org/10.3390/traumacare2040043
Chicago/Turabian StyleOsman, Samatar, Hamza Umar, Yousuf Hashmi, Anam Jawaid, and Zubair Ahmed. 2022. "The Efficacy of Honey Compared to Silver Sulfadiazine for Burn Wound Dressing in Superficial and Partial Thickness Burns—A Systematic Review and Meta-Analysis" Trauma Care 2, no. 4: 523-534. https://doi.org/10.3390/traumacare2040043