
HIV Prevalence among Injury Patients Compared to Other High-Risk Groups in Tanzania
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Prospective Cohort Study
2.1.1. Setting
2.1.2. Procedures
2.1.3. Descriptive Statistics and Variables
2.2. Systematic Review
2.2.1. Eligibility Criteria
2.2.2. Information Sources and Search
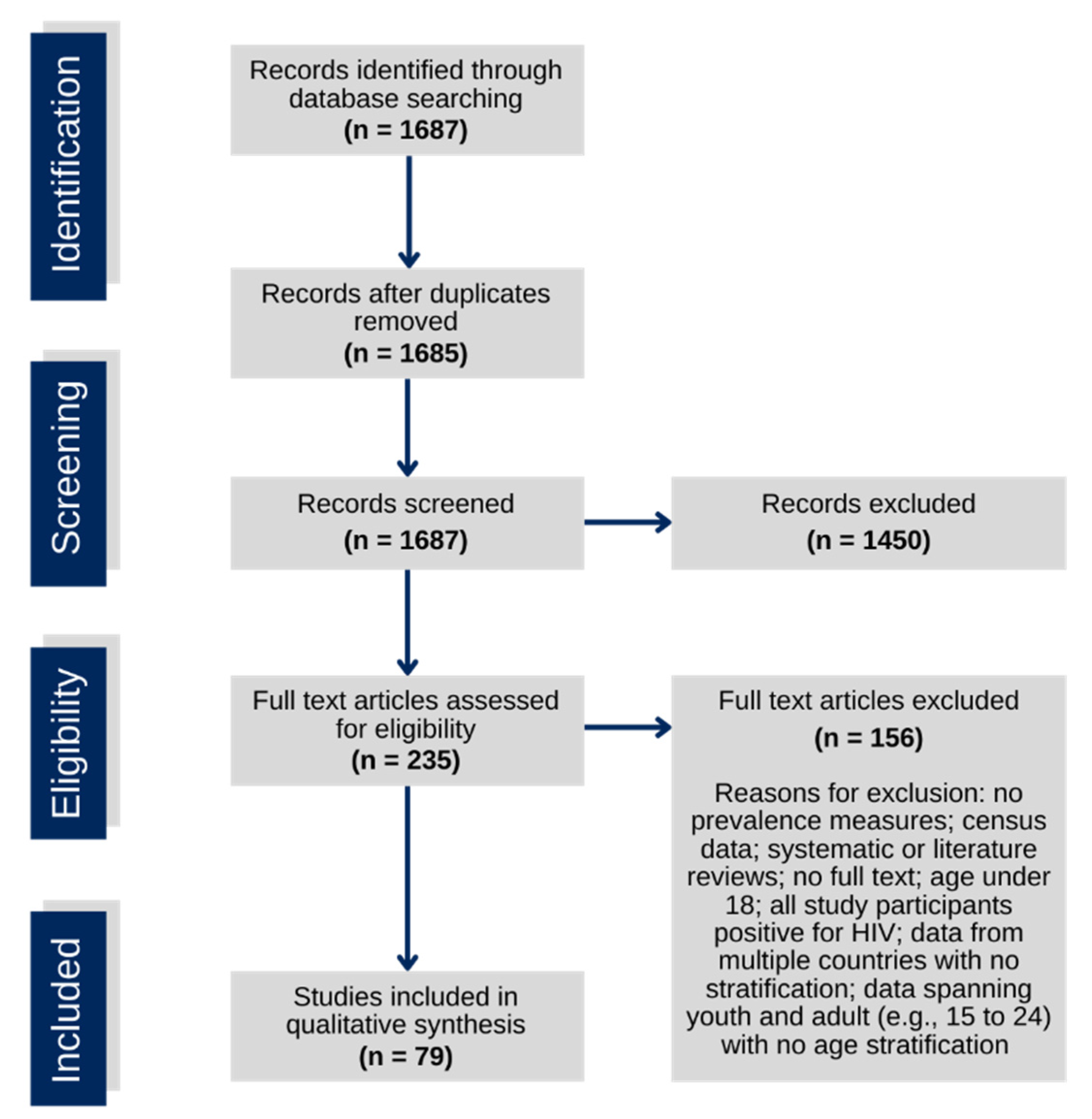
2.2.3. Study Selection
2.2.4. Quality of Included Studies
2.2.5. Data Extraction
2.2.6. Data Analysis
3. Results
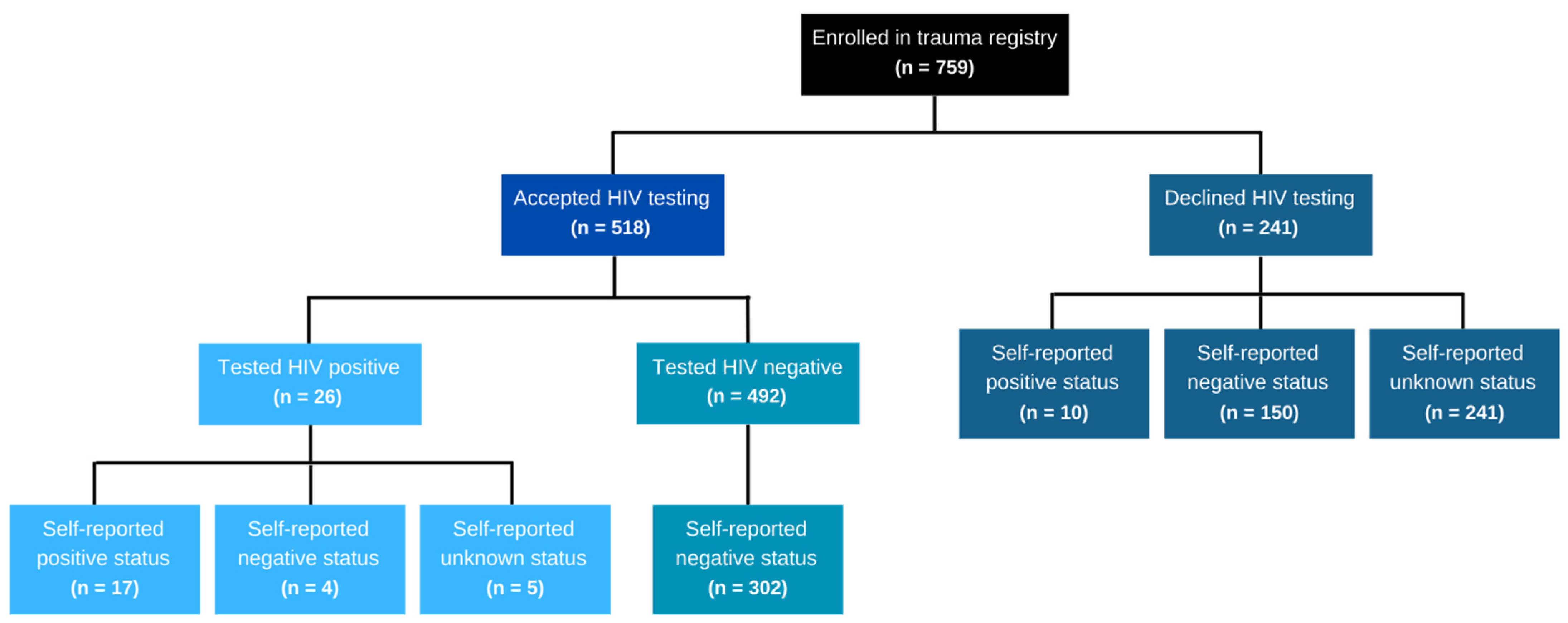
3.1. Prospective Cohort Study
3.2. Systematic Review
3.2.1. Study Characteristics
3.2.2. Narrative Summary of Results
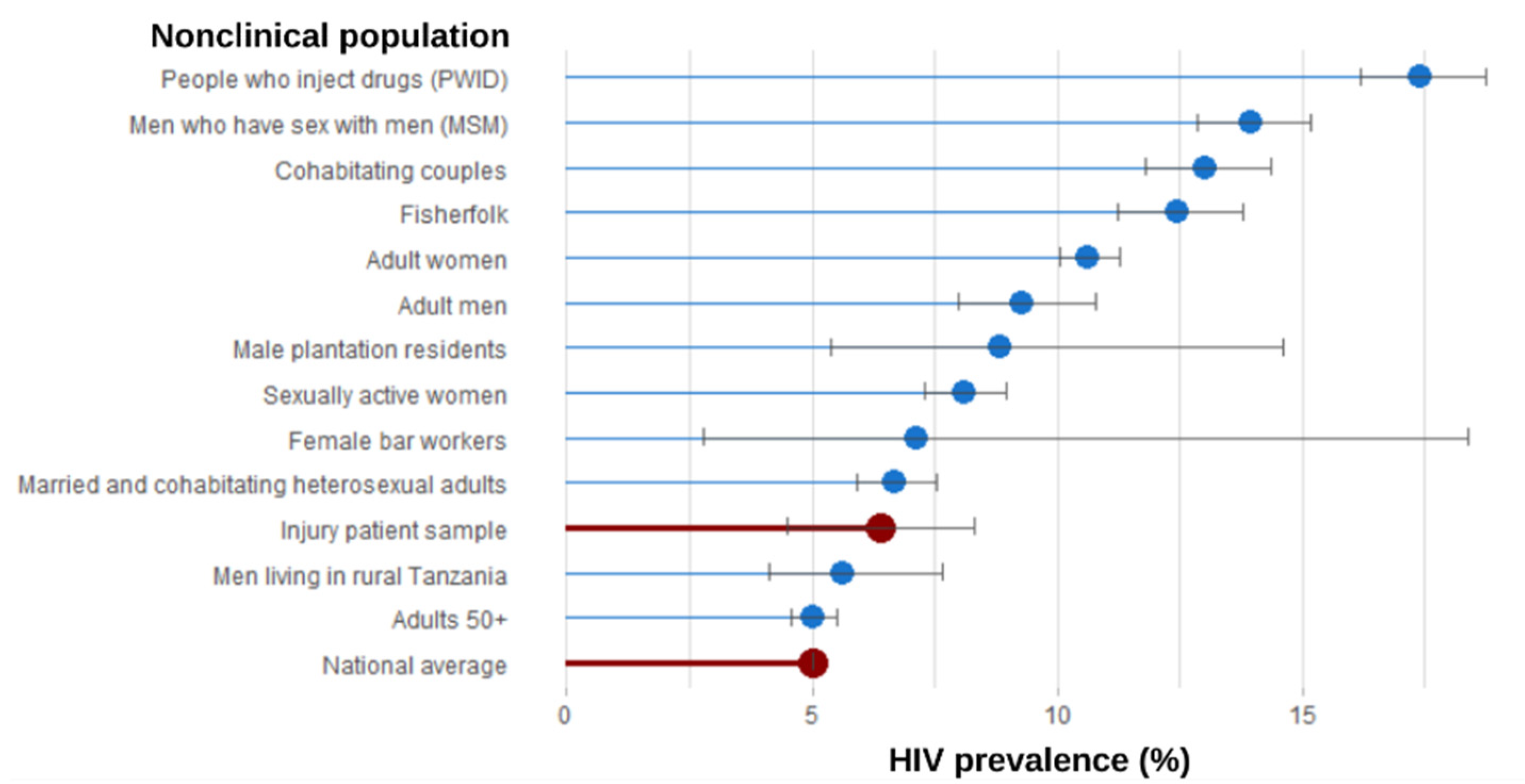
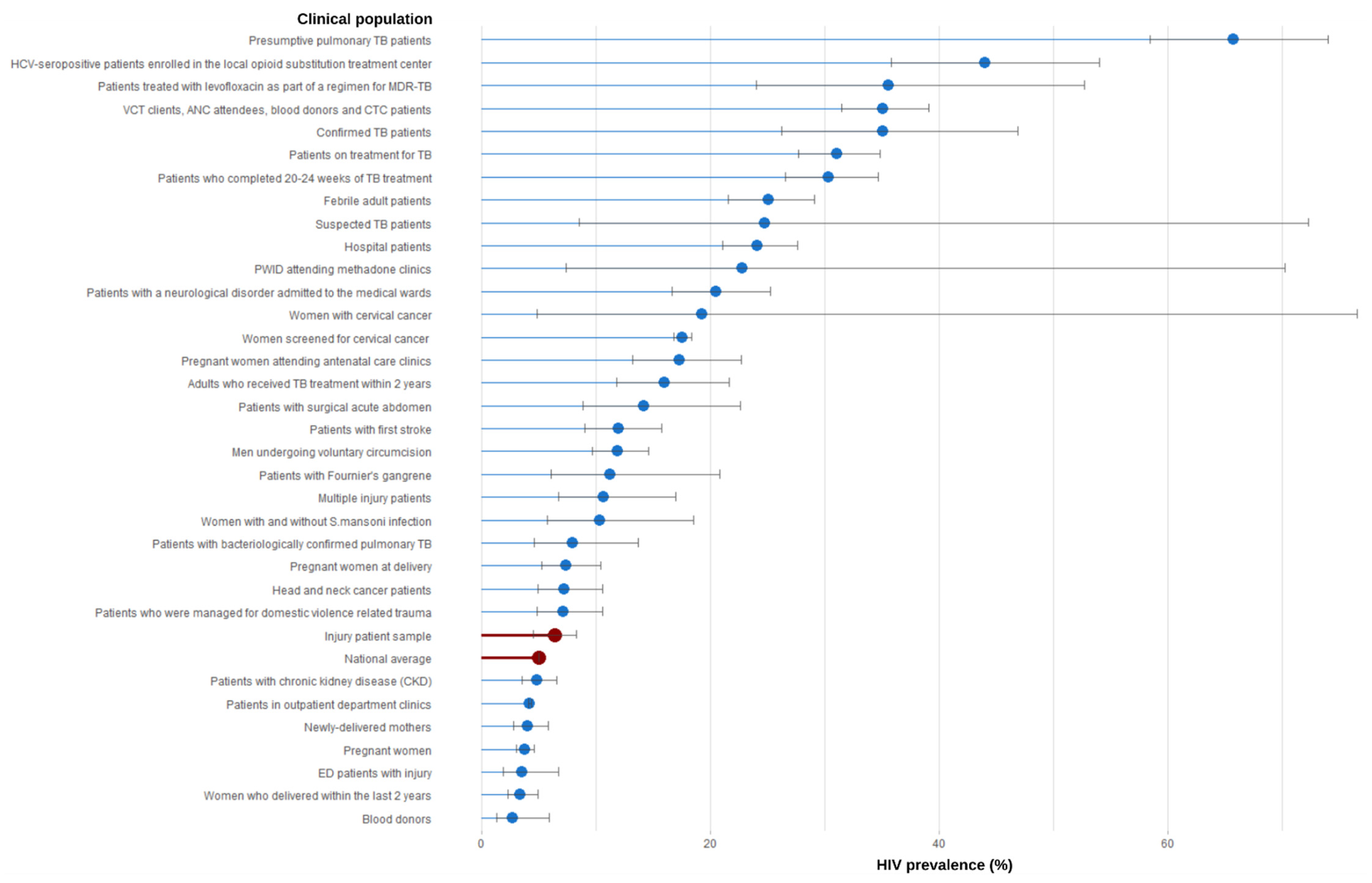
3.3. Comparison of Findings
4. Discussion
5. Limitations
5.1. Prospective Cohort Study
5.2. Systematic Review
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HIV | Human immunodeficiency virus |
| AIDS | Acquired immunodeficiency syndrome |
| ED | Emergency department |
| KCMC | Kilimanjaro Christian Medical Center |
| UNAIDS | Joint United Nations Program on HIV/AIDS |
| LMIC | Low- and middle-income country |
| PITC | Provider-initiated HIV testing and counseling services |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RTI | Road traffic injury |
| KTS II | Kampala Trauma Score II |
| CASP | Critical Appraisal Skills Program |
| TB | Tuberculosis |
| MSM | Men who have sex with men |
| WHO | World Health Organization |
| PWID | Persons who inject drugs |
| ANC | Antenatal care |
| MDR-TB | Multi-drug-resistant TB |
| HCV | Hepatitis C virus |
| VCT | Voluntary testing and counseling |
| CTC | Muhimbii—Care and Treatment Center |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PubMed | ||
|---|---|---|
| Set | Search terms | Results |
| #1 | “HIV Infections” [Mesh] OR “HIV” [Mesh] OR “HIV Long-Term Survivors” [Mesh] OR “HIV Testing” [Mesh] OR “HIV Seroprevalence” [Mesh] OR HIV [tiab] OR AIDS [tiab] OR “Human immunodeficiency virus” [tiab] OR “acquired immunodeficiency syndrome” [tiab] | 474,722 |
| #2 | prevalence [Mesh] OR Incidence [Mesh] OR prevalence [tiab] OR prevalent [tiab] OR incidence [tiab] OR statistics and numerical data [sh] OR epidemiology [sh] OR statistics [tiab] OR rate [tiab] OR rates [tiab] OR population [tiab] OR seroprevalence [tiab] OR epidemiology [tiab] | 7,186,324 |
| #3 | “Tanzania” [Mesh] OR Tanzania [all fields] OR Kilimanjaro [all fields] OR Moshi [all fields] OR Tanzanian [all fields] OR Kili [all fields] | 21,480 |
| #4 | #1 AND #2 AND #3 | 2788 |
| #5 | #4 AND (“2015/01/01” [Date Publication]: “3000” [Date Publication]) | 1155 |
| Embase | ||
| Set | Search terms | Results |
| #1 | ‘Human immunodeficiency virus infection’/exp OR ‘Human immunodeficiency virus’/exp OR ‘Human immunodeficiency virus infected patient’/exp OR ‘HIV test’/exp OR ‘Human immunodeficiency virus prevalence’/exp OR HIV: ab, ti OR AIDS: ab, ti OR “Human immunodeficiency virus”: ab, ti OR “acquired immunodeficiency syndrome”: ab, ti | 647,800 |
| #2 | ‘prevalence’/exp OR ‘incidence’/exp OR ‘human immunodeficiency virus infection’/exp/dm_ep OR prevalence: ab, ti OR prevalent: ab, ti OR incidence: ab, ti OR statistics: ab, ti OR rate: ab, ti OR rates: ab, ti OR population: ab, ti OR seroprevalence: ab, ti OR epidemiology: ab, ti | 7,903,764 |
| #3 | ‘Tanzania’/exp OR Tanzania: ab, ti, ca or Kilimanjaro: ab, ti, ca or Moshi: ab, ti, ca OR Tanzanian: ab, ti, ca OR Kili: ab, ti, ca | 22,246 |
| #4 | #1 AND #2 AND #3 | 2519 |
| #5 | #4 AND [2015-2022]/py | 1073 |
| Scopus | ||
| Set | Search terms | Results |
| #1 | TITLE-ABS-KEY (HIV OR AIDS OR “Human immunodeficiency virus” OR “acquired immunodeficiency syndrome”) | 684,566 |
| #2 | TITLE-ABS-KEY (prevalence OR prevalent OR incidence OR statistics OR rate OR rates OR population OR seroprevalence OR epidemiology) | 13,234,711 |
| #3 | TITLE-ABS-KEY (Tanzania OR Kilimanjaro OR Moshi OR Tanzanian OR Kili) OR AFFILCOUNTRY (Tanzania) OR AFFILCITY (Moshi) | 49,412 |
| #4 | #1 AND #2 AND #3 | 3012 |
| #5 | #4 AND 2015–present | 1240 |
| African Index Medicus | ||
| Set | Search terms | Results |
| #1 | (HIV OR AIDS OR “Human immunodeficiency virus” OR “acquired immunodeficiency syndrome”) AND (prevalence OR prevalent OR incidence OR statistics OR rate OR rates OR population OR seroprevalence OR epidemiology) AND (Tanzania OR Kilimanjaro OR Moshi OR Tanzanian OR Kili); 2015-2022 | 2 |
Appendix B
- Was the research question or objective in this paper clearly stated?
- Did the authors use an appropriate method to answer their question?
- Was the study population clearly specified and defined?
- Were the cases recruited in an acceptable way?
- Were all subjects selected or recruited from the same or similar populations (including the same time period)?
- Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants?
- Was a sample size justification, power description, or variance and effect estimates provided?
- Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?
Appendix C
| Population Group | Study | Quality Rating (#/8) | Outcome Type |
|---|---|---|---|
| Clinical Populations | |||
| Pregnant women | Gamell, 2017 [43] | 7 | primary |
| Konje, 2018 [53] | 7 | primary | |
| Chibwe, 2019 [83] | 8 | secondary | |
| Ng’wamkai, 2019 [67] | 8 | primary | |
| Pregnant women attending antenatal care clinics (ANC) | Manyahi, 2017 [58] | 8 | primary |
| Pregnant women at delivery | Lawi, 2015 [54] | 8 | primary |
| Women who delivered within the last 2 years | Adinan, 2019 [36] | 8 | primary |
| Newly delivered mothers | Nungu, 2019 [71] | 8 | primary |
| Women screened for cervical cancer | Chambuso, 2016 [39] | 7 | primary |
| Mchome, 2020 [84] | 7 | secondary | |
| Chinn, 2021 [85] | 8 | secondary | |
| Katanga, 2021 [86] | 7 | secondary | |
| Women with cervical cancer | Lovgren, 2016 [56] | 7 | primary |
| Khamis, 2021 [87] | 7 | secondary | |
| Men undergoing voluntary circumcision | Bazant, 2016 [88] | 8 | secondary |
| Febrile adult patients | Boillat-Blanco, 2018 [89] | 7 | secondary |
| Patients with Fournier’s gangrene | Chalya, 2015 [90] | 7 | secondary |
| Patients who were managed for domestic-violence-related trauma | Chalya, 2015 [91] | 7 | secondary |
| Hospital patients | Kilale, 2016 [92] | 7 | secondary |
| Patients in outpatient department clinics | Cham, 2019 [35] | 7 | primary |
| Multiple injury patients | Issa, 2018 [93] | 8 | secondary |
| ED patients with injury | Hyuha, 2021 [45] | 8 | primary |
| Confirmed TB patients | Denti, 2015 [79] | 8 | secondary |
| Gunda, 2017 [44] | 7 | primary | |
| Friis, 2018 [42] | 7 | primary | |
| Kidenya, 2018 [80] | 7 | secondary | |
| Mhimbira, 2019 [81] | 7 | secondary | |
| Patients on treatment for TB | Munseri, 2019 [94] | 8 | secondary |
| Suspected TB patients | Hoza, 2016 [95] | 7 | secondary |
| Reither, 2015 [96] | 7 | secondary | |
| Presumptive pulmonary TB patients | Mhimbira, 2015 [77] | 7 | secondary |
| Patients with bacteriologically confirmed pulmonary TB | Senkoro, 2016 [97] | 8 | secondary |
| Patients who completed 20–24 weeks of TB treatment | Manji, 2016 [98] | 7 | secondary |
| Patients treated with levofloxacin as part of MDR-TB regimen | Mohamed, 2021 [34] | 7 | secondary |
| Adults who received TB treatment within 2 years | Mpagama, 2021 [99] | 8 | secondary |
| Head and neck cancer patients | Gilyoma, 2015 [100] | 7 | secondary |
| PWID attending methadone clinics | Lambdin, 2017 [101] | 7 | secondary |
| Kilonzo, 2021 [52] | 7 | primary | |
| HCV-seropositive patients enrolled in the local opioid substitution treatment center | Mohamed, 2017 [102] | 7 | secondary |
| Patients with a neurological disorder admitted to the medical ward | Laizer, 2019 [103] | 7 | secondary |
| Blood donors | Lidenge, 2020 [104] | 7 | secondary |
| Mremi, 2021 [82] | 7 | secondary | |
| Patients with first stroke | Matuja, 2020 [105] | 7 | secondary |
| Patients with chronic kidney disease (CKD) | Meremo, 2018 [106] | 7 | secondary |
| Women with and without S. mansoni infection | Mishra, 2019 [107] | 7 | secondary |
| Patients with surgical acute abdomen | Sravanam, 2018 [74] | 7 | primary |
| VCT clients, ANC attendees, blood Donors, and CTC patients | Urio, 2015 [76] | 7 | primary |
| Nonclinical populations | |||
| Cohabiting couples | Ngilangwa, 2015 [68] | 7 | primary |
| Married and cohabitating heterosexual adults | Mtenga, 2015 [64] | 7 | primary |
| Adults over 50 | Senkoro, 2016 [78] | 8 | secondary |
| Mtowa, 2017 [65] | 7 | primary | |
| Swai, 2017 [75] | 7 | primary | |
| Muiruri, 2019 [66] | 7 | primary | |
| Adult women | Faber, 2017 [41] | 7 | primary |
| Hjort, 2019 [109] | 8 | secondary | |
| Baldur-Felskov, 2019 [110] | 7 | secondary | |
| Mchome, 2021 [60] | 7 | primary | |
| Sexually active women | Safari, 2019 [111] | 7 | secondary |
| Female bar workers | Barnhart, 2019 [38] | 7 | primary |
| Adult men | Norris, 2017 [69] | 7 | primary |
| Olesen, 2017 [112] | 7 | secondary | |
| Men living in rural Tanzania | Downs, 2017 [40] | 7 | primary |
| Men who have sex with men (MSM) | Ahaneku, 2016 [37] | 8 | primary |
| Ishungisa, 2020 [46] | 8 | primary | |
| Khatib, 2017 [51] | 7 | primary | |
| Mmbaga, 2017 [63] | 8 | primary | |
| Mmbaga, 2020 [113] | 8 | primary | |
| Mizinduko, 2020 [61] | 8 | primary | |
| Male plantation residents | Norris 2017 [70] | 7 | primary |
| Fisherfolk | Kapesa, 2018 [47] | 8 | primary |
| Kapiga, 2021 [48] | 7 | primary | |
| Panga, 2021 [72] | 8 | primary | |
| People who inject drugs (PWID) | Matiko, 2015 [59] | 8 | primary |
| Khatib, 2017 [50] | 7 | primary | |
| Mmbaga, 2017 [62] | 8 | primary | |
| Leyna, 2019 [55] | 8 | primary | |
| Kawambwa, 2020 [49] | 8 | primary | |
| Minja, 2021 [108] | 8 | secondary | |
References
- UNAIDS. 90–90–90: An Ambitious Treatment Target to Help End the AIDS Epidemic; Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland, 2014. [Google Scholar]
- UNAIDS. Global AIDS Strategy 2021–2026—End Inequalities. End AIDS; Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland, 2020. [Google Scholar]
- Global Statistics, HIV.gov. Available online: https://www.hiv.gov/hiv-basics/overview/data-and-trends/global-statistics (accessed on 30 October 2020).
- Giguère, K.; Eaton, J.W.; Marsh, K.; Johnson, L.F.; Johnson, C.C.; Ehui, E.; Jahn, A.; Wanyeki, I.; Mbofana, F.; Bakiono, F.; et al. Trends in knowledge of HIV status and efficiency of HIV testing services in sub-Saharan Africa, 2000–2020: A modelling study using survey and HIV testing programme data. Lancet HIV 2021, 8, e284–e293. [Google Scholar] [CrossRef]
- Adolescent and Young Adult Health. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions (accessed on 28 June 2022).
- United Republic of Tanzania, UNAIDS. Available online: https://www.unaids.org/en/regionscountries/countries/unitedrepublicoftanzania (accessed on 5 November 2020).
- GHO, By category, Prevalence of HIV Among Adults Aged 15 to 49—Estimates by WHO Region. Available online: https://apps.who.int/gho/data/view.main.22500WHOREG?lang=en (accessed on 23 October 2020).
- Ogendi, J.O.K.; Ayisi, J.G. Causes of injuries resulting in a visit to the emergency department of a Provincial General Hospital, Nyanza, western Kenya. Afr. Health Sci. 2011, 11, 255–261. [Google Scholar] [PubMed]
- Bundu, I.; Lowsby, R.; Vandy, H.P.; Kamara, S.P.; Jalloh, A.M.; Scott, C.O.S.; Beynon, F. The burden of trauma presenting to the government referral hospital in Freetown, Sierra Leone: An observational study. Afr. J. Emerg. Med. 2019, 9, S9–S13. [Google Scholar] [CrossRef] [PubMed]
- Sawe, H.R.; Mfinanga, J.A.; Mbaya, K.R.; Koka, P.M.; Kilindimo, S.S.; Runyon, M.S.; Mwafongo, V.G.; Wallis, L.A.; Reynolds, T.A. Trauma burden in Tanzania: A one-day survey of all district and regional public hospitals. BMC Emerg. Med. 2017, 17, 30. [Google Scholar] [CrossRef] [PubMed]
- Mortality Caused by Road Traffic Injury (per 100,000 Population)—Tanzania, Data. Available online: https://data.worldbank.org/indicator/SH.STA.TRAF.P5?locations=TZ (accessed on 29 September 2021).
- Mwandri, M.; Hardcastle, T.C.; Sawe, H.; Sakita, F.; Mfinanga, J.; Urassa, S.; Mremi, A.; Mboma, L.N.; Bashaka, P. Trauma burden, patient demographics and care-process in major hospitals in Tanzania: A needs assessment for improving healthcare resource management. Afr. J. Emerg. Med. 2020, 10, 111–117. [Google Scholar] [CrossRef]
- Samji, H.; Zhang, W.; Eyawo, O.; Jabbari, S.; Colley, G.; Tanner, Z.; Hull, M.; Montaner, J.S.G.; Hogg, R.S.; COAST Study Team. Rates and predictors of injury in a population-based cohort of people living with HIV. AIDS 2017, 31, 295–304. [Google Scholar] [CrossRef]
- National AIDS Control Programme. Guidelines for HIV Testing and Counselling in Clinical Settings; United Republic of Tanzania Ministry of Health and Social Welfare: Dodoma, Tanzania, 2007. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef]
- PRISMA. 2021. “PRISMA.” Prisma-Statement.org. Available online: https://prisma-statement.org/ (accessed on 7 September 2022).
- Kilimanjaro Christian Medical Centre (KCMC), VECD Global Health Fellowship. Available online: https://www.vumc.org/vecd/kilimanjaro-christian-medical-centre-kcmc (accessed on 29 June 2022).
- Staton, C.A.; Msilanga, D.; Kiwango, G.; Vissoci, J.R.; de Andrade, L.; Lester, R.; Hocker, M.; Gerardo, C.J.; Mvungi, M. A prospective registry evaluating the epidemiology and clinical care of traumatic brain injury patients presenting to a regional referral hospital in Moshi, Tanzania: Challenges and the way forward. Int. J. Inj. Contr. Saf. Promot. 2017, 24, 69–77. [Google Scholar] [CrossRef]
- Casey, E.R.; Muro, F.; Thielman, N.M.; Maya, E.; Ossmann, E.W.; Hocker, M.B.; Gerardo, C.J. Analysis of traumatic injuries presenting to a referral hospital emergency department in Moshi, Tanzania. Int. J. Emerg. Med. 2012, 5, 28. [Google Scholar] [CrossRef]
- National Bureau of Statistics—The Tanzania HIV Impact Survey 2016–2017 (THIS)—Final Report. Available online: https://www.nbs.go.tz/index.php/en/census-surveys/health-statistics/hiv-and-malaria-survey/382-the-tanzania-hiv-impact-survey-2016-2017-this-final-report (accessed on 5 November 2020).
- Alhajj, M.; Farhana, A. Enzyme linked immunosorbent assay. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Manoochehry, S.; Vafabin, M.; Bitaraf, S.; Amiri, A. A Comparison between the Ability of Revised Trauma Score and Kampala Trauma Score in Predicting Mortality; a Meta-Analysis. Arch. Acad. Emerg. Med. 2019, 7, e6. [Google Scholar] [PubMed]
- Rosenkrantz, L.; Schuurman, N.; Hameed, M.S.; Boniface, R.; Lett, R. The Kampala Trauma Score: A 20-year track record. J. Trauma Acute Care Surg. 2022, 92, e132–e138. [Google Scholar] [CrossRef] [PubMed]
- Kobusingye, O.C.; Lett, R.R. Hospital-based trauma registries in Uganda. J. Trauma 2000, 48, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Gender, Elderly, and Children (MoHCDGEC) [Dar es Salaam], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), [Dar es Salaam], Office of Chief Government Statistician (OCGS) [Zanzibar] & ICF [Rockville, Maryland]. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) Report 2015-16. (2016). MoHCDGEC, MoH, NBS, OCGS, and ICF: Dar es Salaam, Tanzania. Available online: https://dhsprogram.com/publications/publication-fr321-dhs-final-reports.cfm (accessed on 7 September 2022).
- Covidence—Better Systematic Review Management. Available online: https://www.covidence.org/ (accessed on 29 June 2022).
- Study Quality Assessment Tools, NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 30 October 2020).
- CASP CHECKLISTS-CASP-Critical Appraisal Skills Programme. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 5 November 2020).
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 30 June 2022).
- Mohamed, S.; Mvungi, H.C.; Sariko, M.; Rao, P.; Mbelele, P.; Jongedijk, E.M.; van Winkel, C.A.J.; Touw, D.J.; Stroup, S.; Alffenaar, J.-W.C.; et al. Levofloxacin pharmacokinetics in saliva as measured by a mobile microvolume UV spectrophotometer among people treated for rifampicin-resistant TB in Tanzania. J. Antimicrob. Chemother. 2021, 76, 1547–1552. [Google Scholar] [CrossRef]
- Cham, H.J.; MacKellar, D.; Maruyama, H.; Rwabiyago, O.E.; Msumi, O.; Steiner, C.; Kundi, G.; Weber, R.; Byrd, J.; Suraratdecha, C.; et al. Methods, outcomes, and costs of a 2.5 year comprehensive facility-and community-based HIV testing intervention in Bukoba Municipal Council, Tanzania, 2014–2017. PLoS ONE 2019, 14, e0215654. [Google Scholar] [CrossRef]
- Adinan, J.; Adamou, B.; Amour, C.; Shayo, A.; Kidayi, P.L.; Msuya, L. Feasibility of home-based HIV counselling and testing and linking to HIV services among women delivering at home in Geita, Tanzania: A household longitudinal survey. BMC Public Health 2019, 19, 1758. [Google Scholar] [CrossRef]
- Ahaneku, H.; Ross, M.W.; Nyoni, J.E.; Selwyn, B.; Troisi, C.; Mbwambo, J.; Adeboye, A.; McCurdy, S. Depression and HIV risk among men who have sex with men in Tanzania. AIDS Care 2016, 28 (Suppl. 1), 140–147. [Google Scholar] [CrossRef] [Green Version]
- Barnhart, D.A.; Harling, G.; Muya, A.; Ortblad, K.F.; Mashasi, I.; Dambach, P.; Ulenga, N.; Mboggo, E.; Oldenburg, C.E.; Bärnighausen, T.W.; et al. Structural, interpersonal, psychosocial, and behavioral risk factors for HIV acquisition among female bar workers in Dar es Salaam, Tanzania. AIDS Care 2019, 31, 1096–1105. [Google Scholar] [CrossRef] [PubMed]
- Chambuso, R.S.; Shadrack, S.; Lidenge, S.J.; Mwakibete, N.; Medeiros, R.M. Influence of HIV/AIDS on cervical cancer: A retrospective study from tanzania. J. Glob. Oncol. 2017, 3, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Downs, J.A.; de Dood, C.J.; Dee, H.E.; McGeehan, M.; Khan, H.; Marenga, A.; Adel, P.E.; Faustine, E.; Issarow, B.; Kisanga, E.F.; et al. Schistosomiasis and human immunodeficiency virus in men in tanzania. Am. J. Trop. Med. Hyg. 2017, 96, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Faber, M.T.; Munk, C.; Mwaiselage, J.; Dartell, M.; Kahesa, C.; Iftner, T.; Rasch, V.; Kjaer, S.K. Risk factors for HIV positivity among more than 3400 Tanzanian women. Women Health 2017, 57, 650–664. [Google Scholar] [CrossRef]
- Friis, H.; Range, N.S.; Changalucha, J.; PrayGod, G.; Jeremiah, K.; Faurholt-Jepsen, D.; Krarup, H.B.; Andersen, A.B.; Kæstel, P.; Filteau, S. HIV, TB, inflammation and other correlates of serum phosphate: A cross-sectional study. Clin. Nutr. ESPEN 2018, 27, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Gamell, A.; Luwanda, L.B.; Kalinjuma, A.V.; Samson, L.; Ntamatungiro, A.J.; Weisser, M.; Gingo, W.; Tanner, M.; Hatz, C.; Letang, E.; et al. Prevention of mother-to-child transmission of HIV Option B+ cascade in rural Tanzania: The One Stop Clinic model. PLoS ONE 2017, 12, e0181096. [Google Scholar] [CrossRef]
- Gunda, D.W.; Nkandala, I.; Kavishe, G.A.; Kilonzo, S.B.; Kabangila, R.; Mpondo, B.C. Prevalence and Risk Factors of Delayed Sputum Conversion among Patients Treated for Smear Positive PTB in Northwestern Rural Tanzania: A Retrospective Cohort Study. J. Trop. Med. 2017, 2017, 5352906. [Google Scholar] [CrossRef]
- Hyuha, G.M.; Sawe, H.R.; Kilindimo, S.; Mussa, R.Y.; Gulamhussein, M.A.; Rwegoshora, S.S.; Shayo, F.; Mdundo, W.; Mfinanga, J.A.; Weber, E.J. Feasibility and efficacy of text messaging to promote care among trauma patients screened for HIV at an urban emergency department in Tanzania. Int. J. Emerg. Med. 2021, 14, 72. [Google Scholar] [CrossRef]
- Alexander Ishungisa, M.; Moen, K.; Leyna, G.; Makyao, N.; Ramadhan, A.; Lange, T.; Meyrowitsch, D.W.; Mizinduko, M.; Likindikoki, S.; Leshabari, M.; et al. HIV prevalence among men who have sex with men following the implementation of the HIV preventive guideline in Tanzania: Respondent-driven sampling survey. BMJ Open 2020, 10, e036460. [Google Scholar] [CrossRef]
- Kapesa, A.; Basinda, N.; Nyanza, E.C.; Mushi, M.F.; Jahanpour, O.; Ngallaba, S.E. Prevalence of HIV infection and uptake of HIV/AIDS services among fisherfolk in landing Islands of Lake Victoria, north western Tanzania. BMC Health Serv. Res. 2018, 18, 980. [Google Scholar] [CrossRef]
- Kapiga, S.; Hansen, C.H.; Downs, J.A.; Sichalwe, S.; Hashim, R.; Mngara, J.; van Dam, G.J.; Corstjens, P.L.A.M.; Kingery, J.R.; Peck, R.N.; et al. The burden of HIV, syphilis and schistosome infection and associated factors among adults in the fishing communities in northwestern Tanzania. Trop. Med. Int. Health 2021, 26, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Kawambwa, R.H.; Majigo, M.V.; Mohamed, A.A.; Matee, M.I. High prevalence of human immunodeficiency virus, hepatitis B and C viral infections among people who inject drugs: A potential stumbling block in the control of HIV and viral hepatitis in Tanzania. BMC Public Health 2020, 20, 177. [Google Scholar] [CrossRef]
- Khatib, A.; Matiko, E.; Khalid, F.; Welty, S.; Ali, A.; Othman, A.; Haji, S.; Dahoma, M.; Rutherford, G. HIV and hepatitis B and C co-infection among people who inject drugs in Zanzibar. BMC Public Health 2017, 17, 917. [Google Scholar] [CrossRef] [PubMed]
- Khatib, A.; Haji, S.; Khamis, M.; Said, C.; Khalid, F.; Dahoma, M.; Ali, A.; Othman, A.; Welty, S.; McFarland, W. Reproducibility of Respondent-Driven Sampling (RDS) in Repeat Surveys of Men Who have Sex with Men, Unguja, Zanzibar. AIDS Behav. 2017, 21, 2180–2187. [Google Scholar] [CrossRef] [PubMed]
- Kilonzo, S.B.; Gunda, D.W.; Majinge, D.C.; Jaka, H.; Manyiri, P.M.; Kalokola, F.; Mtui, G.; Shao, E.R.; Bakshi, F.A.; Stephano, A. Seroprevalence of hepatitis B virus infection, anti-HCV antibodies and HIV and knowledge among people who use drugs attending methadone therapy clinic in Tanzania; a cross-sectional study. BMC Infect. Dis. 2021, 21, 699. [Google Scholar] [CrossRef]
- Konje, E.T.; Magoma, M.T.N.; Hatfield, J.; Kuhn, S.; Sauve, R.S.; Dewey, D.M. Missed opportunities in antenatal care for improving the health of pregnant women and newborns in Geita district, Northwest Tanzania. BMC Pregnancy Childbirth 2018, 18, 394. [Google Scholar] [CrossRef]
- Lawi, J.D.T.; Mirambo, M.M.; Magoma, M.; Mushi, M.F.; Jaka, H.M.; Gumodoka, B.; Mshana, S.E. Sero-conversion rate of Syphilis and HIV among pregnant women attending antenatal clinic in Tanzania: A need for re-screening at delivery. BMC Pregnancy Childbirth 2015, 15, 3. [Google Scholar] [CrossRef]
- Leyna, G.H.; Makyao, N.; Mwijage, A.; Ramadhan, A.; Likindikoki, S.; Mizinduko, M.; Leshabari, M.T.; Moen, K.; Mmbaga, E.J. HIV/HCV co-infection and associated risk factors among injecting drug users in Dar es Salaam, Tanzania: Potential for HCV elimination. Harm Reduct. J. 2019, 16, 68. [Google Scholar] [CrossRef]
- Lovgren, K.; Soliman, A.S.; Ngoma, T.; Kahesa, C.; Meza, J. Characteristics and geographic distribution of HIV-positive women diagnosed with cervical cancer in Dar es Salaam, Tanzania. Int. J. STD AIDS 2016, 27, 1049–1056. [Google Scholar] [CrossRef]
- Manyahi, J.; Jullu, B.S.; Abuya, M.I.; Juma, J.; Ndayongeje, J.; Kilama, B.; Sambu, V.; Nondi, J.; Rabiel, B.; Somi, G.; et al. Prevalence of HIV and syphilis infections among pregnant women attending antenatal clinics in Tanzania, 2011. BMC Public Health 2015, 15, 501. [Google Scholar] [CrossRef] [Green Version]
- Manyahi, J.; Msigwa, Y.; Mhimbira, F.; Majigo, M. High sero-prevalence of hepatitis B virus and human immunodeficiency virus infections among pregnant women attending antenatal clinic at Temeke municipal health facilities, Dar es Salaam, Tanzania: A cross sectional study. BMC Pregnancy Childbirth 2017, 17, 109. [Google Scholar] [CrossRef]
- Matiko, E.; Khatib, A.; Khalid, F.; Welty, S.; Said, C.; Ali, A.; Othman, A.; Haji, S.; Kibona, M.; Kim, E.; et al. HIV prevalence and risk behaviors among people who inject drugs in two serial cross-sectional respondent-driven sampling surveys, Zanzibar 2007 and 2012. AIDS Behav. 2015, 19 (Suppl. 1), S36–S45. [Google Scholar] [CrossRef]
- Mchome, B.; Linde, D.S.; Manongi, R.; Waldstroem, M.; Lftner, T.; Wu, C.; Mwaisalage, J.; Rasch, V.; Kjaer, S.K. Incident detection of human papillomavirus—A prospective follow-up study among Tanzanian women with a focus on HIV status. Int. J. Infect. Dis. 2021, 110, 165–170. [Google Scholar] [CrossRef]
- Mizinduko, M.M.; Moen, K.; Likindikoki, S.; Mwijage, A.; Leyna, G.H.; Makyao, N.; Leshabari, M.T.; Ramadhan, A.; Kambi, M.B.; Meyrowitsch, D.; et al. HIV prevalence and associated risk factors among female sex workers in Dar es Salaam, Tanzania: Tracking the epidemic. Int. J. STD AIDS 2020, 31, 950–957. [Google Scholar] [CrossRef]
- Mmbaga, E.J.; Moen, K.; Makyao, N.; Leshabari, M. Prevalence and predictors of human immunodeficiency virus and selected sexually transmitted infections among people who inject drugs in dar es salaam, tanzania: A new focus to get to zero. Sex. Transm. Dis. 2017, 44, 79–84. [Google Scholar] [CrossRef]
- Mmbaga, E.J.; Moen, K.; Makyao, N.; Mpembeni, R.; Leshabari, M.T. HIV and STI s among men who have sex with men in Dodoma municipality, Tanzania: A cross-sectional study. Sex. Transm. Infect. 2017, 93, 314–319. [Google Scholar] [CrossRef]
- Mtenga, S.M.; Pfeiffer, C.; Merten, S.; Mamdani, M.; Exavery, A.; Haafkens, J.; Tanner, M.; Geubbels, E. Prevalence and social drivers of HIV among married and cohabitating heterosexual adults in south-eastern Tanzania: Analysis of adult health community cohort data. Glob. Health Action 2015, 8, 28941. [Google Scholar] [CrossRef]
- Mtowa, A.; Gerritsen, A.A.M.; Mtenga, S.; Mwangome, M.; Geubbels, E. Socio-demographic inequalities in HIV testing behaviour and HIV prevalence among older adults in rural Tanzania, 2013. AIDS Care 2017, 29, 1162–1168. [Google Scholar] [CrossRef]
- Muiruri, C.; Swai, S.J.; Ramadhani, H.O.; Knettel, B.A.; Mahande, M.J.; Msuya, S.E.; Bartlett, J.A. Individual and partner characteristics associated with HIV testing and counseling uptake among individuals 50 years or older in Tanzania. Int. J. STD AIDS 2019, 30, 1425–1431. [Google Scholar] [CrossRef]
- Ng’wamkai, G.; Msigwa, K.V.; Chengula, D.; Mgaya, F.; Chuma, C.; Msemwa, B.; Silago, V.; Majigo, M.; Mshana, S.E.; Mirambo, M.M. Treponema pallidum infection predicts sexually transmitted viral infections (hepatitis B virus, herpes simplex virus-2, and human immunodeficiency virus) among pregnant women from rural areas of Mwanza region, Tanzania. BMC Pregnancy Childbirth 2019, 19, 392. [Google Scholar] [CrossRef]
- Ngilangwa, D.P.; Ochako, R.; Mboya, B.A.; Noronha, R.H.; Mgomella, G.S. Prevalence and predictors of HIV sero-discordance among cohabiting couples tested in northern Tanzania. Pan Afr. Med. J. 2015, 22, 275. [Google Scholar] [CrossRef]
- Norris, A.H.; Loewenberg Weisband, Y.; Wiles, M.; Ickovics, J.R. Prevalence of sexually transmitted infections among Tanzanian migrants: A cross-sectional study. Int. J. STD AIDS 2017, 28, 991–1000. [Google Scholar] [CrossRef]
- Norris, A.H.; Decker, M.R.; Weisband, Y.L.; Hindin, M.J. Reciprocal physical intimate partner violence is associated with prevalent STI/HIV among male Tanzanian migrant workers: A cross-sectional study. Sex. Transm. Infect. 2017, 93, 253–258. [Google Scholar] [CrossRef]
- Nungu, S.I.; Mghamba, J.M.; Rumisha, S.F.; Semali, I.A. Uptake and determinants for HIV postpartum re-testing among mothers with prenatal negative status in Njombe region, Tanzania. BMC Infect. Dis. 2019, 19, 398. [Google Scholar] [CrossRef]
- Panga, O.D.; Joachim, A.; Samizi, F.G.; Gitige, C.G.; Moremi, N.; Simeo, J.; Mtebe, M.; Abade, A. Prevalence, recent infection and predictors of HIV infection in fishing community along the shore of Lake Victoria in Tanzania. J. Public Health 2021. [Google Scholar] [CrossRef]
- Shayo, G.; Makundi, I.; Luzzatto, L. The prevalence of human immunodeficiency and of hepatitis B viral infections is not increased in patients with sickle cell disease in Tanzania. BMC Infect. Dis. 2021, 21, 1028. [Google Scholar] [CrossRef]
- Sravanam, P.; Massenga, A.; Bugimbi, M.; Mirambo, M.M.; Chalya, P.L. HIV seroprevalence and factors affecting clinical outcomes among patients with surgical acute abdomen in selected hospitals in Mwanza, north-western in Tanzania. Tanzan. J. Health Res. 2018, 20, 4. [Google Scholar] [CrossRef]
- Swai, S.J.; Damian, D.J.; Urassa, S.; Temba, B.; Mahande, M.J.; Philemon, R.N.; Msuya, S.E. Prevalence and risk factors for HIV among people aged 50 years and older in Rombo district, Northern Tanzania. Tanzan. J. Health Res. 2017, 19, 2. [Google Scholar] [CrossRef]
- Urio, L.J.; Mohamed, M.A.; Mghamba, J.; Abade, A.; Aboud, S. Evaluation of HIV antigen/antibody combination ELISAs for diagnosis of HIV infection in Dar Es Salaam, Tanzania. Pan Afr. Med. J. 2015, 20, 196. [Google Scholar] [CrossRef]
- Mhimbira, F.A.; Bholla, M.; Sasamalo, M.; Mukurasi, W.; Hella, J.J.; Jugheli, L.; Reither, K. Detection of Mycobacterium tuberculosis by EasyNAT diagnostic kit in sputum samples from Tanzania. J. Clin. Microbiol. 2015, 53, 1342–1344. [Google Scholar] [CrossRef] [Green Version]
- Senkoro, M.; Mfinanga, S.; Egwaga, S.; Mtandu, R.; Kamara, D.V.; Basra, D.; Fundikira, L.; Kahwa, A.; Shirima, R.; Range, N.; et al. Prevalence of pulmonary tuberculosis in adult population of Tanzania: A national survey, 2012. Int. J. Tuberc. Lung Dis. 2016, 20, 1014–1021. [Google Scholar] [CrossRef]
- Denti, P.; Jeremiah, K.; Chigutsa, E.; Faurholt-Jepsen, D.; PrayGod, G.; Range, N.; Castel, S.; Wiesner, L.; Hagen, C.M.; Christiansen, M.; et al. Pharmacokinetics of isoniazid, pyrazinamide, and ethambutol in newly diagnosed pulmonary TB patients in tanzania. PLoS ONE 2015, 10, e0141002. [Google Scholar] [CrossRef]
- Kidenya, B.R.; Mshana, S.E.; Fitzgerald, D.W.; Ocheretina, O. Genotypic drug resistance using whole-genome sequencing of Mycobacterium tuberculosis clinical isolates from North-western Tanzania. Tuberculosis 2018, 109, 97–101. [Google Scholar] [CrossRef]
- Mhimbira, F.; Hiza, H.; Mbuba, E.; Hella, J.; Kamwela, L.; Sasamalo, M.; Ticlla, M.; Said, K.; Mhalu, G.; Chiryamkubi, M.; et al. Prevalence and clinical significance of respiratory viruses and bacteria detected in tuberculosis patients compared to household contact controls in Tanzania: A cohort study. Clin. Microbiol. Infect. 2019, 25, 107.e1–107.e7. [Google Scholar] [CrossRef]
- Mremi, A.; Yahaya, J.J.; Nyindo, M.; Mollel, E. Transfusion-Transmitted Infections and associated risk factors at the Northern Zone Blood Transfusion Center in Tanzania: A study of blood donors between 2017 and 2019. PLoS ONE 2021, 16, e0249061. [Google Scholar] [CrossRef]
- Chibwe, E.; Silago, V.; Kajoro, E.; Juma, M.; Mkumbo, E.; Minja, C.A.; Mujuni, F.; Mshana, S.E.; Mirambo, M.M. Antihepatitis B Surface Antigen and Hepatitis C Antibodies among Pregnant Women in an Urban Area of Mwanza City, Tanzania. J. Pregnancy 2019, 2019, 7917894. [Google Scholar] [CrossRef]
- Mchome, B.; Swai, P.; Wu, C.; Katanga, J.; Kahesa, C.; Manongi, R.; Mwaiselage, J.D.; Kjaer, S.; Rasch, V.; Linde, D.S. Comprehensive Cervical Cancer Prevention in Tanzania (CONCEPT) study: Cohort profile. BMJ Open 2020, 10, e038531. [Google Scholar] [CrossRef]
- Chinn, J.O.; Runge, A.S.; Dinicu, A.I.; Chang, J.; Maher, J.A.; Crawford, E.W.; Naaseh, A.; Cooper, E.C.; Zezoff, D.C.; White, K.M.; et al. Visual inspection with acetic acid screening for cervical cancer among women receiving anti-retroviral therapy for human immunodeficiency virus infection in northern Tanzania. J. Obstet. Gynaecol. Res. 2021, 47, 4365–4370. [Google Scholar] [CrossRef]
- Katanga, J.; Kjaer, S.K.; Manongi, R.; Pembe, A.B.; Iftner, T.; Waldstrom, M.; Mwaiselage, J.; Rasch, V. Agreement between careHPV and hybrid capture 2 in detecting high-risk HPV in women in Tanzania. Acta Obstet. Gynecol. Scand. 2021, 100, 786–793. [Google Scholar] [CrossRef]
- Khamis, S.I.; Mrema, A.S.; Katanga, J.; Lugina, E.L. Survival in cervical cancer and its predictors at ocean road cancer institute from january to december 2012. JCO Glob. Oncol. 2021, 7, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Bazant, E.; Mahler, H.; Machaku, M.; Lemwayi, R.; Kulindwa, Y.; Gisenge Lija, J.; Mpora, B.; Ochola, D.; Sarkar, S.; Williams, E.; et al. A randomized evaluation of a demand creation lottery for voluntary medical male circumcision among adults in tanzania. J. Acquir. Immune Defic. Syndr. 2016, 72 (Suppl. 4), S280–S287. [Google Scholar] [CrossRef]
- Boillat-Blanco, N.; Mbarack, Z.; Samaka, J.; Mlaganile, T.; Mamin, A.; Genton, B.; Kaiser, L.; Calandra, T.; D’Acremont, V. Prognostic value of quickSOFA as a predictor of 28-day mortality among febrile adult patients presenting to emergency departments in Dar es Salaam, Tanzania. PLoS ONE 2018, 13, e0197982. [Google Scholar] [CrossRef]
- Chalya, P.L.; Igenge, J.Z.; Mabula, J.B.; Simbila, S. Fournier’s gangrene at a tertiary health facility in northwestern Tanzania: A single centre experiences with 84 patients. BMC Res. Notes 2015, 8, 481. [Google Scholar] [CrossRef]
- Chalya, P.L.; Massinde, A.N.; Kihunrwa, A.; Kayange, N.M.; Hauli, K.A.; Kapesa, A.; Ngallaba, S.E.; Mweteni, W.; Gilyoma, J.M. Trauma admissions among victims of domestic violence at a tertiary care hospital in north-western Tanzania: An urgent call to action. Tanzan. J. Health Res. 2015, 17, 4. [Google Scholar] [CrossRef]
- Kilale, A.M.; Ngadaya, E.; Muhumuza, J.; Kagaruki, G.B.; Lema, Y.L.; Ngowi, B.J.; Mfinanga, S.G.; Hinderaker, S.G. Who has mycobacterial disease? A cross sectional study in agropastoral communities in tanzania. PLoS ONE 2016, 11, e0153711. [Google Scholar] [CrossRef]
- Issa, A.; Mbelenge, N.; Chalya, P.L.; Gilyoma, J.M. Aetiological spectrum, injury characteristics and treatment outcome of multiple injuries at a tertiary care hospital in Tanzania. Tanzan. J. Health Res. 2018, 20, 4. [Google Scholar] [CrossRef]
- Munseri, P.J.; Kimambo, H.; Pallangyo, K. Diabetes mellitus among patients attending TB clinics in Dar es Salaam: A descriptive cross-sectional study. BMC Infect. Dis. 2019, 19, 915. [Google Scholar] [CrossRef]
- Hoza, A.S.; Mfinanga, S.G.M.; Rodloff, A.C.; Moser, I.; König, B. Increased isolation of nontuberculous mycobacteria among TB suspects in Northeastern, Tanzania: Public health and diagnostic implications for control programmes. BMC Res. Notes 2016, 9, 109. [Google Scholar] [CrossRef]
- Reither, K.; Jugheli, L.; Glass, T.R.; Sasamalo, M.; Mhimbira, F.A.; Weetjens, B.J.; Cox, C.; Edwards, T.L.; Mulder, C.; Beyene, N.W.; et al. Evaluation of Giant African Pouched Rats for Detection of Pulmonary Tuberculosis in Patients from a High-Endemic Setting. PLoS ONE 2015, 10, e0135877. [Google Scholar] [CrossRef]
- Senkoro, M.; Kumar, A.M.V.; Chinnakali, P.; Mfinanga, S.G.; Egwaga, S.; Kamara, V.; van Leth, F.; Hinderaker, S.G. Population impact of factors associated with prevalent pulmonary tuberculosis in Tanzania. Int. J. Tuberc. Lung Dis. 2016, 20, 1326–1333. [Google Scholar] [CrossRef] [Green Version]
- Manji, M.; Shayo, G.; Mamuya, S.; Mpembeni, R.; Jusabani, A.; Mugusi, F. Lung functions among patients with pulmonary tuberculosis in Dar es Salaam—A cross-sectional study. BMC Pulm. Med. 2016, 16, 58. [Google Scholar] [CrossRef]
- Mpagama, S.G.; Msaji, K.S.; Kaswaga, O.; Zurba, L.J.; Mbelele, P.M.; Allwood, B.W.; Ngungwa, B.S.; Kisonga, R.M.; Lesosky, M.; Rylance, J.; et al. The burden and determinants of post-TB lung disease. Int. J. Tuberc. Lung Dis. 2021, 25, 846–853. [Google Scholar] [CrossRef]
- Gilyoma, J.M.; Rambau, P.F.; Masalu, N.; Kayange, N.M.; Chalya, P.L. Head and neck cancers: A clinico-pathological profile and management challenges in a resource-limited setting. BMC Res. Notes 2015, 8, 772. [Google Scholar] [CrossRef]
- Lambdin, B.H.; Lorvick, J.; Mbwambo, J.K.; Rwegasha, J.; Hassan, S.; Lum, P.; Kral, A.H. Prevalence and predictors of HCV among a cohort of opioid treatment patients in Dar es Salaam, Tanzania. Int. J. Drug Policy 2017, 45, 64–69. [Google Scholar] [CrossRef]
- Mohamed, Z.; Mbwambo, J.; Shimakawa, Y.; Poiteau, L.; Chevaliez, S.; Pawlotsky, J.-M.; Rwegasha, J.; Bhagani, S.; Taylor-Robinson, S.D.; Makani, J.; et al. Clinical utility of HCV core antigen detection and quantification using serum samples and dried blood spots in people who inject drugs in Dar-es-Salaam, Tanzania. J. Int. AIDS Soc. 2017, 20, 21856. [Google Scholar] [CrossRef]
- Laizer, S.; Kilonzo, K.; Urasa, S.; Maro, V.; Walker, R.; Howlett, W. Neurological disorders in a consultant hospital in Northern Tanzania. A cohort study. eNeurologicalSci 2019, 14, 101–105. [Google Scholar] [CrossRef]
- Lidenge, S.J.; Tran, T.; Tso, F.Y.; Ngowi, J.R.; Shea, D.M.; Mwaiselage, J.; Wood, C.; West, J.T. Prevalence of Kaposi’s sarcoma-associated herpesvirus and transfusion-transmissible infections in Tanzanian blood donors. Int. J. Infect. Dis. 2020, 95, 204–209. [Google Scholar] [CrossRef]
- Matuja, S.S.; Munseri, P.; Khanbhai, K. The burden and outcomes of stroke in young adults at a tertiary hospital in Tanzania: A comparison with older adults. BMC Neurol. 2020, 20, 206. [Google Scholar] [CrossRef]
- Meremo, A.J.; Masalu, M.B.; Sabi, I.; Ngilangwa, D.P.; Kapinga, J.; Tagalile, R.; Munyogwa, M.J.; Mwashambwa, M.Y. Prevalence and risk factors associated with chronic kidney disease among patients presenting at a haemodialysis unit in dodoma, tanzania. East Afr. Health Res. J. 2018, 2, 53–57. [Google Scholar] [CrossRef]
- Mishra, P.; Colombe, S.; Paul, N.; Mlingi, J.; Tosiri, I.; Aristide, C.; Gao, J.; Kashangaki, P.; Nagai, H.; Kalluvya, S.E.; et al. Insufficiency of annual praziquantel treatment to control Schistosoma mansoni infections in adult women: A longitudinal cohort study in rural Tanzania. PLoS Negl. Trop. Dis. 2019, 13, e0007844. [Google Scholar] [CrossRef]
- Hjort, L.; Lykke Møller, S.; Minja, D.; Msemo, O.; Nielsen, B.B.; Lund Christensen, D.; Theander, T.; Nielsen, K.; Larsen, L.G.; Grunnet, L.G.; et al. FOETAL for NCD-FOetal Exposure and Epidemiological Transitions: The role of Anaemia in early Life for Non-Communicable Diseases in later life: A prospective preconception study in rural Tanzania. BMJ Open 2019, 9, e024861. [Google Scholar] [CrossRef] [PubMed]
- Baldur-Felskov, B.; Mwaiselage, J.; Faber, M.T.; Kjaerem, M.; de la Cour, C.D.; Munk, C.; Kahesa, C.; Iftner, T.; Rasch, V.; Kjaer, S.K. Factors associated with a cervical high-grade lesion on cytology or a positive visual inspection with acetic acid among more than 3300 Tanzanian women. Trop. Med. Int. Health 2019, 24, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Safari, W.; Urassa, M.; Mtenga, B.; Changalucha, J.; Beard, J.; Church, K.; Zaba, B.; Todd, J. Contraceptive use and discontinuation among women in rural North-West Tanzania. Contracept. Reprod. Med. 2019, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Olesen, T.B.; Mwaiselage, J.; Iftner, T.; Kahesa, C.; Rasch, V.; Frederiksen, K.; Munk, C.; Kjaer, S.K. Risk factors for genital human papillomavirus among men in Tanzania. J. Med. Virol. 2017, 89, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Mmbaga, E.J.; Leyna, G.H.; Leshabari, M.T.; Moen, K. Early Anal Sex Experience Among Men Who Have Sex with Men in Dar Es Salaam Tanzania: Implications for HIV Prevention and Care. Arch. Sex. Behav. 2020, 49, 2045–2055. [Google Scholar] [CrossRef] [PubMed]
- Minja, L.T.; Hella, J.; Mbwambo, J.; Nyandindi, C.; Omary, U.S.; Levira, F.; Mpagama, S.; Shimwela, M.; Okuma, J.; Gagneux, S.; et al. High burden of tuberculosis infection and disease among people receiving medication-assisted treatment for substance use disorder in Tanzania. PLoS ONE 2021, 16, e0250038. [Google Scholar] [CrossRef]
- Kuendig, H.; Hasselberg, M.; Laflamme, L.; Daeppen, J.-B.; Gmel, G. Acute alcohol consumption and injury: Risk associations and attributable fractions for different injury mechanisms. J. Stud. Alcohol Drugs 2008, 69, 218–226. [Google Scholar] [CrossRef]
- Watt, K.; Purdie, D.M.; Roche, A.M.; McClure, R.J. Risk of injury from acute alcohol consumption and the influence of confounders. Addiction 2004, 99, 1262–1273. [Google Scholar] [CrossRef]
- Borges, G.; Cherpitel, C.; Mittleman, M. Risk of injury after alcohol consumption: A case-crossover study in the emergency department. Soc. Sci. Med. 2004, 58, 1191–1200. [Google Scholar] [CrossRef]
- Riuttanen, A.; Jäntti, S.J.; Mattila, V.M. Alcohol use in severely injured trauma patients. Sci. Rep. 2020, 10, 17891. [Google Scholar] [CrossRef]
- WHO. Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections 2019. Available online: https://www.who.int/hiv/strategy2016-2021/progress-report-2019/en/ (accessed on 30 October 2020).
- World Health Organization. Injuries and Violence: The Facts 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Staton, C.A.; Vissoci, J.R.N.; Toomey, N.; Abdelgadir, J.; Chou, P.; Haglund, M.; Mmbaga, B.T.; Mvungi, M.; Swahn, M. The impact of alcohol among injury patients in Moshi, Tanzania: A nested case-crossover study. BMC Public Health 2018, 18, 275. [Google Scholar] [CrossRef]
- Conserve, D.F.; Msofe, J.; Issango, J.; Tureski, K.; McCarthy, P.; Rwezahura, P.; Maboko, L.; Lwakatare, M.; Ndugulile, F.; Kamwela, J.; et al. Development, implementation, and scale up of the national furaha yangu campaign to promote HIV test and treat services uptake among men in tanzania. Am. J. Mens. Health 2022, 16, 15579883221087838. [Google Scholar] [CrossRef]
- National AIDS Control Programme (NACP). National Guidelines for the Management of HIV and AIDS. (2015). Ministry of Health and Social Welfare: Dar es Salaam, Tanzania. Available online: https://www.childrenandaids.org/sites/default/files/2017-04/Tanzania_National-HIV-Guidelines_2015.pdf (accessed on 7 September 2022).
- Hansoti, B.; Stead, D.; Parrish, A.; Reynolds, S.J.; Redd, A.D.; Whalen, M.M.; Mvandaba, N.; Quinn, T.C. HIV testing in a South African Emergency Department: A missed opportunity. PLoS ONE 2018, 13, e0193858. [Google Scholar] [CrossRef]
- Ramadhani, J.; Sawe, H.R.; Kilindimo, S.S.; Mfinanga, J.A.; Weber, E.J. Feasibility and yield of HIV screening among adult trauma patients presenting to an urban emergency department of a tertiary referral hospital in Tanzania. AIDS Res. Ther. 2019, 16, 8. [Google Scholar] [CrossRef]




| Characteristic | Total Sample (n = 759) | HIV-Positive (Both) (n = 36) | HIV-Negative (Tested) (n = 492) | HIV-Negative (Self-Report) (n = 150) | Unknown Status (n = 81) |
|---|---|---|---|---|---|
| Age Median (IQR) | 34 (26-47) | 39 (31.8–50) | 33 (26–46) | 35 (28–45) | 32 (24–49) |
| Male n (%) [missing] | 593 (78.6%) [5] | 20 (55.6%) [0] | 392 (80.2%) [3] | 117 (78.5%) [1] | 64 (80%) [1] |
| Alcohol use within 6 h of injury n (%) | 157 (20.7%) | 10 (27.8%) | 96 (19.5%) | 32 (21.3%) | 19 (23.5%) |
| Years of education Median (IQR) | 7 (7–11) | 7 (7–8.5) | 7 (7–11) | 7 (7–11) | 7 (7–11) |
| Employment | |||||
| n (%) [missing] | [3] | [0] | [2] | [0] | [1] |
| Student | 24 (3.2%) | 0 | 14 (2.8%) | 5 (3.3%) | 5 (6.2%) |
| Unemployed | 27 (3.6%) | 1 (2.8%) | 15 (3%) | 5 (3.3%) | 6 (7.4%) |
| Professional | 84 (11.1%) | 3 (8.3%) | 56 (11.4%) | 21 (14%) | 4 (4.9%) |
| Skilled employment | 117 (15.4%) | 5 (13.9%) | 78 (15.9%) | 23 (15.3%) | 11 (13.6%) |
| Self-employed | 261 (34.4%) | 17 (47.2%) | 159 (32.3%) | 54 (36%) | 31 (38.3%) |
| Farmer | 211 (27.8%) | 8 (22.2%) | 148 (30.1%) | 36 (24%) | 19 (23.5%) |
| Other | 32 (4.2%) | 2 (5.6%) | 20 (4.1%) | 6 (4%) | 4 (4.9%) |
| Prior testing n (%) | 485 (63.9%) | 31 (86.1%) | 304 (61.8%) | 150 (100%) | 0 |
| Mechanism of injury | |||||
| n (%) [missing] | [1] | [0] | [0] | [0] | [1] |
| Road traffic injury | 478 (63%) | 20 (55.6%) | 315 (64%) | 89 (59.3%) | 54 (66.7%) |
| Assault | 100 (13.2%) | 5 (13.9%) | 62 (12.6%) | 23 (15.3%) | 10 (12.3%) |
| Other | 180 (23.7%) | 11 (30.6%) | 115 (23.4%) | 38 (25.3%) | 16 (19.8%) |
| KTS II | |||||
| n (%) [missing] | [99] | [9] | [46] | [32] | [12] |
| Mild (9, 10) | 341 (44.9%) | 16 (44.4%) | 229 (46.5%) | 65 (43.3%) | 31 (38.3%) |
| Moderate (7, 8) | 307 (40.4%) | 10 (27.8%) | 211 (42.9%) | 51 (34%) | 35 (43.2%) |
| Severe (0–6) | 12 (1.6%) | 1 (2.8%) | 6 (1.2%) | 2 (1.3%) | 3 (3.7%) |
| Marital status | |||||
| n (%) [missing] | [1] | [0] | [1] | [0] | [0] |
| Single | 266 (35%) | 12 (33.3%) | 169 (34.3%) | 49 (32.7%) | 36 (44.4%) |
| Married | 404 (53.2%) | 15 (41.7%) | 268 (54.5%) | 80 (53.3%) | 41 (50.6%) |
| Partner, not married | 15 (2%) | 1 (2.8%) | 13 (2.6%) | 1 (0.7%) | 0 |
| Widow/widower | 32 (4.2%) | 3 (8.3%) | 18 (3.7%) | 9 (6%) | 2 (2.5%) |
| Separated | 41 (5.4%) | 5 (13.9%) | 23 (4.7%) | 11 (7.3%) | 2 (2.5%) |
| Tested HIV-Positive (n = 26) | Self-Reported and Tested HIV-Positive (n = 17) | Self-Reported HIV-Negative, Tested HIV-Positive (n = 4) | ||
|---|---|---|---|---|
| HIV test results from ED visit | Viral load (copies/mL) Median (IQR) | 54.5 (9.8–12,959.5) | 39 (0–141) | 7615 (39–103,364) |
| CD4 count Median (IQR) [missing] | 403 (258.5–652) [2] | 394 (267–673) | 424.5 (384–510.2) | |
| Self-reported prior HIV testing and/or treatment | On ARV n (%) [missing] | 15 (57.7%) | 13 (76.4%) [3] | 2 (50%) [1] |
| AIDS-related infections n (%) | 1 (3.8%) | 0 | 0 | |
| HIV-positive family n (%) [missing] | 7 (26.9%) | 5 (29.4%) | 1 (25%) [1] | |
| (a) | |||||||
|---|---|---|---|---|---|---|---|
| Population Group | Study | Year of Data Collection | Geographic Region | Sample Size HIV Tested | Prevalence (95% CI) | Pooled- Prevalence (95% CI) | Model Heterogeneity |
| Pregnant women | Gamell, 2017 [43] | 2014–2015 | Kilombero district | 1548 | 3.10% | 3.75% [3.05%–4.62%] | I2 = 27% τ2 = 0.0141 p = 0.25 |
| Konje, 2018 [53] | 2016–2017 | Geita district | 1426 | 3.88% | |||
| Chibwe, 2019 [83] | 2017 | Mwanza | 291 | 3.40% | |||
| Ng’wamkai, 2019 [67] | 2018 | Mwanza | 499 | 5.01% | |||
| Pregnant women attending antenatal care clinics (ANC) | Manyahi, 2017 [58] | 2014 | Temeke municipality | 249 | 17.20% | N/A | N/A |
| Pregnant women at delivery | Lawi, 2015 [54] | 2012 | Mwanza | 408 | 7.20% | N/A | N/A |
| Women who delivered within the last 2 years | Adinan, 2019 [36] | 2017 | Geita region | 767 | 3.39% | N/A | N/A |
| Newly delivered mothers | Nungu, 2019 [71] | 2015–2016 | Wanging’ombe and Njombe districts | 668 | 4.04% | N/A | N/A |
| Women screened for cervical cancer | Chambuso, 2016 [39] | unknown | Morogoro | 517 | 21.30% | 17.54% [16.77%–18.35%] | I2 = 94% τ2 = 0.1742 p < 0.01 |
| Mchome, 2020 [84] | 2015–2017 | Dar es Salaam | 4043 | 17.80% | |||
| Chinn, 2021 [85] | 2018 | Mwanza | 824 | 8.01% | |||
| Katanga, 2021 [86] | unknown | unknown | 3643 | 17.90% | |||
| Women with cervical cancer | Lovgren, 2016 [56] | 2007–2011 | Dar es Salaam | 143 | 38.46% | 19.27% [4.85%–76.58%] | I2 = 97% τ2 = 0.9622 p < 0.01 |
| Khamis, 2021 [87] | 2012 | Dar es Salaam | 202 | 9.40% | |||
| Men undergoing voluntary circumcision | Bazant, 2016 [88] | 2014–2015 | Iringa, Njombe, Tabora | 665 | 11.90% | N/A | N/A |
| Febrile adult patients | Boillat-Blanco, 2018 [89] | 2013–2014 | Dar es Salaam | 519 | 25.00% | N/A | N/A |
| Patients with Fournier’s gangrene | Chalya, 2015 [90] | 2006–2014 | Bugando | 80 | 11.30% | N/A | N/A |
| Patients who were managed for domestic-violence-related trauma | Chalya, 2015 [91] | 2009–2014 | Bugando | 324 | 7.10% | N/A | N/A |
| Hospital patients | Kilale, 2016 [92] | 2010–2012 | Arusha municipality | 664 | 24.00% | N/A | N/A |
| Patients in outpatient department clinics | Cham, 2019 [35] | 2014–2017 | Bukoba | 133695 | 4.20% | N/A | N/A |
| Multiple injury patients | Issa, 2018 [93] | 2013 | Bugando | 150 | 10.70% | N/A | N/A |
| ED patients with injury | Hyuha, 2021 [45] | 2019–2020 | Dar es Salaam | 255 | 3.50% | N/A | N/A |
| Confirmed TB patients | Denti, 2015 [79] | 2010–2011 | Mwanza | 100 | 50.00% | 35.06% [26.22%–46.89%] | I2 = 96% τ2 = 0.1001 p < 0.01 |
| Gunda, 2017 [44] | 2016–2017 | Sengerema district | 156 | 35.26% | |||
| Friis, 2018 [42] | 2006–2009 | Mwanza | 1605 | 41.43% | |||
| Kidenya, 2018 [80] | 2014–2015 | Mwanza | 78 | 34.60% | |||
| Mhimbira, 2019 [81] | 2013–2015 | Dar es Salaam | 794 | 21.16% | |||
| Patients on | Munseri, 2019 [94] | 2016–2017 | Dar Es Salaam | 660 | 31.12% | N/A | N/A |
| treatment for TB | |||||||
| Suspected TB patients | Hoza, 2016 [95] | 2012–2013 | Ngamiani, Muheza, Bombo, Makorora | 372 | 14.20% | 24.76% [8.48%–72.25%] | I2 = 98% τ2 = 0.5878 p < 0.01 |
| Reither, 2015 [96] | 2012 | Bagamoyo district | 480 | 42.49% | |||
| Presumptive pulmonary TB patients | Mhimbira, 2015 [77] | unknown | Bagomoyo district | 143 | 66% | N/A | N/A |
| Patients with bacteriologically confirmed pulmonary TB | Senkoro, 2016 [97] | 2011–2012 | Dar es Salaam | 151 | 7.95% | N/A | N/A |
| Patients who completed 20–24 weeks of TB treatment | Manji, 2016 [98] | 2014 | Temeke municipality | 501 | 30.30% | N/A | N/A |
| Patients treated with levofloxacin as part of MDR-TB regimen | Mohamed, 2021 [34] | 2019 | Northern Tanzania | 45 | 35.56% | N/A | N/A |
| Adults who received TB treatment within 2 years | Mpagama, 2021 [99] | unknown | Kilimanjaro | 219 | 15.98% | N/A | N/A |
| Head and neck cancer patients | Gilyoma, 2015 [100] | 2009–2013 | Mwanza | 346 | 7.20% | N/A | N/A |
| PWID attending methadone clinics | Lambdin, 2017 [101] | 2011–2013 | Dar es Salaam | 630 | 40% | 22.74% [7.36%–70.26%] | I2 = 98% τ2 = 0.6480 p < 0.01 |
| Kilonzo, 2021 [52] | 2019–2020 | Mwanza | 253 | 12.80% | |||
| HCV-seropositive patients enrolled in the local opioid substitution treatment center | Mohamed, 2017 [102] | 2015 | Dar es Salaam | 116 | 43.97% | N/A | N/A |
| Patients with a neurological disorder admitted to the medical ward | Laizer, 2019 [103] | 2007–2008 | Moshi (KCMC) | 337 | 20.50% | N/A | N/A |
| Blood donors | Lidenge, 2020 [104] | 2019 | Dar es Salaam | 504 | 4.20% | 2.73% [1.27%–5.89%] | I2 = 93% τ2 = 0.2851 p < 0.01 |
| Mremi, 2021 [82] | 2017–2019 | Kilimanjaro | 101616 | 1.90% | |||
| Patients with first stroke | Matuja, 2020 [105] | 2018–2019 | Dar es Salaam | 369 | 11.92% | N/A | N/A |
| Patients with chronic kidney disease (CKD) | Meremo, 2018 [106] | 2013–2015 | Dodoma | 792 | 4.80% | N/A | N/A |
| Women with and without S. mansoni infection | Mishra, 2019 [107] | unknown | Kisesa, Lumeji, Welamasonga, Kayenze | 97 | 10.00% | N/A | N/A |
| Patients with surgical acute abdomen | Sravanam, 2018 [74] | 2016 | Mwanza | 106 | 14.20% | N/A | N/A |
| VCT clients, ANC attendees, blood donors, and CTC patients | Urio, 2015 [76] | 2011–2012 | unknown | 596 | 35.10% | N/A | N/A |
| (b) | |||||||
| Population group | Study | Year of data collection | Geographic region | Sample size HIV tested | Prevalence (95% CI) | Pooled-prevalence (95% CI) | Model heterogeneity |
| Cohabiting couples | Ngilangwa, 2015 [68] | 2005–2007 | Kilimanjaro, Arusha | 2666 | 13.02% | N/A | N/A |
| Married and cohabitating heterosexual adults | Mtenga, 2015 [64] | 2013 | Ifakara | 3737 | 6.69% | N/A | N/A |
| Adults over 50 | Senkoro, 2016 [78] | 2011–2012 | Dar es Salaam | 6302 | 5.05% | 3.23% [1.65%–6.31%] | I2 = 89% τ2 = 0.4193 p < 0.01 |
| Mtowa, 2017 [65] | 2012–2013 | Ifakara | 1643 | 6.03% | |||
| Swai, 2017 [75] | 2015 | Rombo district | 588 | 1.70% | |||
| Muiruri, 2019 [66] | 2015 | Rombo district | 600 | 1.70% | |||
| Adult women | Faber, 2017 [41] | 2008–2009 | Dar es Salaam, Pwani, Mwanza, | 3424 | 10.19% | 8.48% [4.91%–14.67%] | I2 = 95% τ2 = 0.3037 p < 0.01 |
| and Mtwara | |||||||
| Hjort, 2019 [108] | 2014–2015 | Korogwe, Tanga | 952 | 3.57% | |||
| Baldur-Felskov, 2019 [109] | 2008–2009 | Dar es Salaam, Pwani, Mwanza, | 3339 | 10.00% | |||
| and Mtwara; | |||||||
| Mchome, 2021 [60] | 2015–2016 | Dar es Salaam and Kilimanjaro | 2253 | 13.30% | |||
| Sexually active women | Safari, 2019 [110] | 2015–2016 | Magu district | 4052 | 8.09% | N/A | N/A |
| Female bar workers | Barnhart, 2019 [38] | 2017 | Kinondoni district | 56 | 7.10% | N/A | N/A |
| Adult men | Norris, 2017 [69] | 2004 | Dar es Salaam, Pwani, Tanga, | 158 | 8.86% | 9.27% [7.98%–10.78%] | I2 = 0% τ2 = 0 p = 0.85 |
| northern Tanzania | |||||||
| Olesen, 2017 [111] | 2009 | Kilimanjaro | 1503 | 9.31% | |||
| Men living in rural Tanzania | Downs, 2017 [40] | 2014–2016 | Mwanza | 674 | 5.60% | N/A | N/A |
| Men who have sex with men (MSM) | Ahaneku, 2016 [37] | 2012–2013 | Dar es Salaam, Tanga | 176 | 25% | 14.36% [10.85%–19.01%] | I2 = 89% τ2 = 0.1115 p < 0.01 |
| Ishungisa, 2020 [46] | 2017 | Dar es Salaam | 777 | 12.30% | |||
| Khatib, 2017 [51] | 2007; 2011 | Unguja, Zanzibar | 848 | 8.72% | |||
| Mmbaga, 2017 [63] | 2015 | Dar es Salaam | 610 | 15.50% | |||
| Mmbaga, 2020 [112] | 2014 | Dodoma | 409 | 17.36% | |||
| Mizinduko, 2020 [61] | 2017 | Dar es Salaam | 777 | 12.36% | |||
| Male plantation residents | Norris 2017 [70] | 2004 | Northern Tanzania | 158 | 8.86% | N/A | N/A |
| Fisherfolk | Kapesa, 2018 [47] | 2017 | Selected Islands of Lake Victoria in Buchosa and Muleba districts | 456 | 14.00% | 12.18% [9.12%–16.27%] | I2 = 86% τ2 = 0.0561 p < 0.01 |
| Kapiga, 2021 [48] | 2015–2016 | Muleba, Sengerema, and Ukerewe along Lake Victoria | 1121 | 14.20% | |||
| Panga, 2021 [72] | 2019 | Geita and Chato | 1048 | 9.06% | |||
| districts | |||||||
| People who inject drugs (PWID) | Matiko, 2015 [59] | 2007; 2012 | Zanzibar | 907 | 16.09% | 15.82% [10.86%–23.06%] | I2 = 95% τ2 = 0.2109 p < 0.01 |
| Khatib, 2017 [50] | 2012 | Zanzibar | 408 | 11.30% | |||
| Mmbaga, 2017 [62] | 2015 | Dar es Salaam | 610 | 15.50% | |||
| Leyna, 2019 [55] | 2017 | Dar es Salaam | 611 | 8.35% | |||
| Kawambwa, 2020 [49] | 2017 | Dar es Salaam, Sinza, Kinondoni, Kimara, Tandale, Msasani, Mbagala, Kunduchi, Temeke, and Tandika suburbs | 219 | 33.80% | |||
| Minja, 2021 [113] | 2016–2017 | unknown | 897 | 18.84% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barcenas, L.K.; Tupetz, A.; Behrens, S.; Kozhumam, A.S.; Strand, E.; von Isenburg, M.; Sakasaka, P.A.; Rubach, M.P.; Vissoci, J.R.N.; Park, L.P.; et al. HIV Prevalence among Injury Patients Compared to Other High-Risk Groups in Tanzania. Trauma Care 2022, 2, 487-509. https://doi.org/10.3390/traumacare2030041
Barcenas LK, Tupetz A, Behrens S, Kozhumam AS, Strand E, von Isenburg M, Sakasaka PA, Rubach MP, Vissoci JRN, Park LP, et al. HIV Prevalence among Injury Patients Compared to Other High-Risk Groups in Tanzania. Trauma Care. 2022; 2(3):487-509. https://doi.org/10.3390/traumacare2030041
Chicago/Turabian StyleBarcenas, Loren K., Anna Tupetz, Shay Behrens, Arthi S. Kozhumam, Eleanor Strand, Megan von Isenburg, Philoteus A. Sakasaka, Matthew P. Rubach, Joao Ricardo Nickenig Vissoci, Lawrence P. Park, and et al. 2022. "HIV Prevalence among Injury Patients Compared to Other High-Risk Groups in Tanzania" Trauma Care 2, no. 3: 487-509. https://doi.org/10.3390/traumacare2030041