
External Validation of the ImAgeS Risk Score for Mortality in Hospitalized Kidney Transplant Recipients with COVID-19: A Retrospective Observational Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Ethical and Institutional Considerations
2.3. ImAgeS Risk Score and Data Collection
2.4. Data Collection
2.5. Aims and Outcomes
2.6. Statistical Analysis
3. Results
3.1. Exploratory Analysis
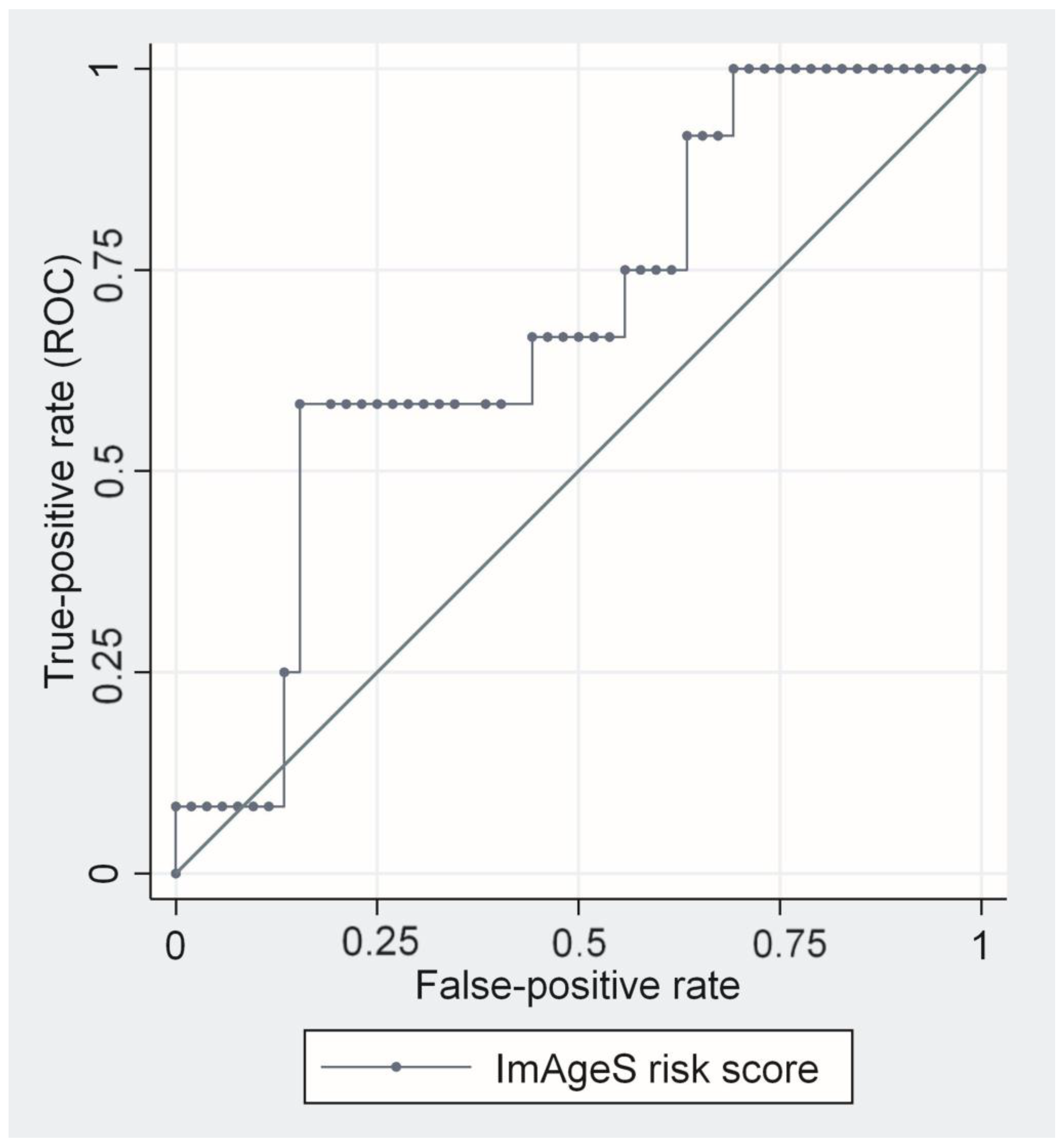
3.2. ImAgeS Risk Score and 30-Day Mortality
3.3. Calibration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Udomkarnjananun, S.; Kerr, S.J.; Townamchai, N.; Susantitaphong, P.; Tulvatana, W.; Praditpornsilpa, K.; Eiam-Ong, S.; Avihingsanon, Y. Mortality risk factors of COVID-19 infection in kidney transplantation recipients: A systematic review and meta-analysis of cohorts and clinical registries. Sci. Rep. 2021, 11, 20073. [Google Scholar] [CrossRef]
- Modelli de Andrade, L.G.; de Sandes-Freitas, T.V.; Requião-Moura, L.R.; Viana, L.A.; Cristelli, M.P.; Garcia, V.D.; Alcântara, A.L.C.; Esmeraldo, R.D.M.; Filho, M.A.; Pacheco-Silva, A.; et al. Development and validation of a simple web-based tool for early prediction of COVID-19-associated death in kidney transplant recipients. Am. J. Transplant. 2022, 22, 610–625. [Google Scholar] [CrossRef]
- Raja, M.A.; Mendoza, M.A.; Villavicencio, A.; Anjan, S.; Reynolds, J.M.; Kittipibul, V.; Fernandez, A.; Guerra, G.; Camargo, J.F.; Simkins, J.; et al. COVID-19 in solid organ transplant recipients: A systematic review and meta-analysis of current literature. Transplant. Rev. 2021, 35, 100588. [Google Scholar] [CrossRef]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef] [PubMed]
- Domjanović, J.; Škopinić, T.D.; Radić, J.; Luketin, M.; Jeličić, I.; Matetic, A. Performance of Derived Laboratory Biomarkers with Regard to 30-Day Mortality in Kidney Transplant Recipients with COVID-19. Life 2022, 12, 2068. [Google Scholar] [CrossRef] [PubMed]
- Domjanović, J.; Matetic, A.; Kramarić, D.B.; Škopinić, T.D.; Škaro, D.B.; Delić, N.; Runjić, F.; Jeličić, I. Association of the novel CROW-65 risk score and mortality in hospitalized kidney transplant recipients with COVID-19: A retrospective observational study. Wien. Klin. Wochenschr. 2022, 134, 842–849. [Google Scholar] [CrossRef]
- Kremer, D.; Pieters, T.T.; Verhaar, M.C.; Berger, S.P.; Bakker, S.J.L.; van Zuilen, A.D.; Joles, J.A.; Vernooij, R.W.; van Balkom, B.W. A systematic review and meta-analysis of COVID-19 in kidney transplant recipients: Lessons to be learned. Am. J. Transplant. 2021, 21, 3936–3945. [Google Scholar] [CrossRef]
- Caillard, S.; Chavarot, N.; Francois, H.; Matignon, M.; Greze, C.; Kamar, N.; Gatault, P.; Thaunat, O.; Legris, T.; Frimat, L.; et al. Is COVID-19 infection more severe in kidney transplant recipients? Am. J. Transplant. 2021, 21, 1295–1303. [Google Scholar] [CrossRef]
- Mahalingasivam, V.; Craik, A.; Tomlinson, L.A.; Ge, L.; Hou, L.; Wang, Q.; Yang, K.; Fogarty, D.G.; Keenan, C. A Systematic Review of COVID-19 and Kidney Transplantation. Kidney Int. Rep. 2021, 6, 24–45. [Google Scholar] [CrossRef]
- COVID-19 in Solid Organ Transplant Recipients: Initial Report from the US Epicenter—Pereira—2020—American Journal of Transplantation—Wiley Online Library n.d. Available online: https://onlinelibrary.wiley.com/doi/10.1111/ajt.15941 (accessed on 10 May 2022).
- Pinchera, B.; Spirito, L.; Ferreri, L.; Rocca, R.L.; Celentano, G.; Buonomo, A.R.; Foggia, M.; Scotto, R.; Federico, S.; Gentile, I.; et al. SARS-CoV-2 in Kidney Transplant Patients: A Real-Life Experience. Front. Med. 2022, 9, 864865. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Finelli, C.; Parisi, S. The clinical impact of COVID-19 epidemic in the hematologic setting. Adv. Biol. Regul. 2020, 77, 100742. [Google Scholar] [CrossRef] [PubMed]
- Garbo, R.; Valent, F.; Gigli, G.L.; Valente, M. Pre-Existing Lymphopenia Increases the Risk of Hospitalization and Death after SARS-CoV-2 Infection. Infect. Dis. Rep. 2022, 14, 20–25. [Google Scholar] [CrossRef]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Deng, Y.; Weng, Z.; Yang, L. Lymphopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A systemic review and meta-analysis. Int. J. Infect. Dis. 2020, 96, 131–135. [Google Scholar] [CrossRef]
- Kılınç Toker, A.; Çelik, İ.; Toker, İ.; Eren, E. Quick COVID-19 Severity Index, CURB-65 and Quick SOFA Scores Comparison in Predicting Mortality and Risk Factors of COVID-19 Patients. Arch. Iran. Med. 2022, 25, 443–449. [Google Scholar] [CrossRef]
- Raj, K.; Mahajan, P.; Watts, A.; Aedma, S.; Jose, J.A.; Pillai, K.J.; Rizkalla, A.; Sharma, S.; Upadhyay, R.; Dhobale, S.; et al. Independent Predictors of Mortality in COVID-19 Myocardial Injury: The Role of Troponin Levels, GRACE Score, SOFA Score, and TIMI Score. Cureus 2022, 14, e32082. [Google Scholar] [CrossRef]
- Yang, Z.; Hu, Q.; Huang, F.; Xiong, S.; Sun, Y. The prognostic value of the SOFA score in patients with COVID-19: A retrospective, observational study. Medicine 2021, 100, e26900. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Burdick, H.; Lam, C.; Mataraso, S.; Siefkas, A.; Braden, G.; Dellinger, R.P.; McCoy, A.; Vincent, J.-L.; Green-Saxena, A.; Barnes, G.; et al. Prediction of respiratory decompensation in COVID-19 patients using machine learning: The READY trial. Comput. Biol. Med. 2020, 124, 103949. [Google Scholar] [CrossRef] [PubMed]
- Ena, J.; Segura-Heras, J.V.; Fonseca-Aizpuru, E.M.; López-Reboiro, M.L.; Gracia-Gutiérrez, A.; Martín-Oterino, J.A.; Diez-Canseco, A.M.-U.; Pérez-García, C.; Ramos-Rincón, J.; Gómez-Huelgas, R. Derivation and validation of a risk score for admission to the Intensive Care Unit in patients with COVID-19. Rev. Clin. Esp. 2022, 222, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bennouar, S.; Bachir Cherif, A.; Kessira, A.; Bennouar, D.-E.; Abdi, S. Development and validation of a laboratory risk score for the early prediction of COVID-19 severity and in-hospital mortality. Intensiv. Crit. Care Nurs. 2021, 64, 103012. [Google Scholar] [CrossRef]
- Peruzzo, M.B.; Requião-Moura, L.; Nakamura, M.R.; Viana, L.; Cristelli, M.; Tedesco-Silva, H.; Medina-Pestana, J. Predictive ability of severity scores and outcomes for mortality in kidney transplant recipients with coronavirus disease 2019 admitted to the intensive care unit: Results from a Brazilian single-center cohort study. J. Bras. Nefrol. 2022, 44, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Li, R.; Liu, S. Immunoregulation with mTOR inhibitors to prevent COVID-19 severity: A novel intervention strategy beyond vaccines and specific antiviral medicines. J. Med. Virol. 2020, 92, 1495–1500. [Google Scholar] [CrossRef]
- Basile, M.S.; Cavalli, E.; McCubrey, J.; Hernández-Bello, J.; Muñoz-Valle, J.F.; Fagone, P.; Nicoletti, F. The PI3K/Akt/mTOR pathway: A potential pharmacological target in COVID-19. Drug Discov. Today 2022, 27, 848–856. [Google Scholar] [CrossRef]
- Abu-Eid, R.; Ward, F.J. Targeting the PI3K/Akt/mTOR pathway: A therapeutic strategy in COVID-19 patients. Immunol. Lett. 2021, 240, 1–8. [Google Scholar] [CrossRef]
- Henry, B.; Cheruiyot, I.; Vikse, J.; Mutua, V.; Kipkorir, V.; Benoit, J.; Plebani, M.; Bragazzi, N.; Lippi, G. Lymphopenia and neutrophilia at admission predicts severity and mortality in patients with COVID-19: A meta-analysis. Acta Biomed. 2020, 91, e2020008. [Google Scholar] [CrossRef]
- Bajpai, D.; Deb, S.; Bose, S.; Gandhi, C.P.; Modi, T.; Katyal, A.; Saxena, N.; Patil, A.; Patil, S.; Thakare, S.; et al. Clinical Course and Outcomes of COVID-19 in Kidney Transplant Recipients. Indian J. Nephrol. 2022, 32, 467–475. [Google Scholar] [CrossRef]
- Ou, M.; Zhu, J.; Ji, P.; Li, H.; Zhong, Z.; Li, B.; Pang, J.; Zhang, J.; Zheng, X. Risk factors of severe cases with COVID-19: A meta-analysis. Epidemiol. Infect. 2020, 148, e175. [Google Scholar] [CrossRef]
- Hu, J.; Wang, Y. The Clinical Characteristics and Risk Factors of Severe COVID-19. Gerontology 2021, 67, 255–266. [Google Scholar] [CrossRef]
- Figliozzi, S.; Masci, P.G.; Ahmadi, N.; Tondi, L.; Koutli, E.; Aimo, A.; Stamatelopoulos, K.; Dimopoulos, M.; Caforio, A.L.P.; Georgiopoulos, G. Predictors of adverse prognosis in COVID-19: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2020, 50, e13362. [Google Scholar] [CrossRef] [PubMed]
- Schold, J.D.; King, K.L.; Husain, S.A.; Poggio, E.D.; Buccini, L.D.; Mohan, S. COVID-19 mortality among kidney transplant candidates is strongly associated with social determinants of health. Am. J. Transplant. 2021, 21, 2563–2572. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Malcangi, G.; Ceci, S.; Patano, A.; Corriero, A.; Vimercati, L.; Azzollini, D.; Marinelli, G.; Coloccia, G.; Piras, F.; et al. Effectiveness of SARS-CoV-2 Vaccines for Short- and Long-Term Immunity: A General Overview for the Pandemic Contrast. Int. J. Mol. Sci. 2022, 23, 8485. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.-S.F.; Bemelman, F.J.; Messchendorp, A.L.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Frölke, S.C.; Geers, D.; GeurtsvanKessel, C.H.; et al. The RECOVAC Immune-response Study: The Immunogenicity, Tolerability, and Safety of COVID-19 Vaccination in Patients With Chronic Kidney Disease, on Dialysis, or Living with a Kidney Transplant. Transplantation 2022, 106, 821–834. [Google Scholar] [CrossRef] [PubMed]
- Caillard, S.; Thaunat, O. COVID-19 vaccination in kidney transplant recipients. Nat. Rev. Nephrol. 2021, 17, 785–787. [Google Scholar] [CrossRef]
- Sakuraba, A.; Luna, A.; Micic, D. A Systematic Review and Meta-Analysis of Serologic Response following Coronavirus Disease 2019 (COVID-19) Vaccination in Solid Organ Transplant Recipients. Viruses 2022, 14, 1822. [Google Scholar] [CrossRef]
- Balzanelli, M.G.; Distratis, P.; Aityan, S.K.; Amatulli, F.; Catucci, O.; Cefalo, A.; De Michele, A.; Dipalma, G.; Inchingolo, F.; Lazzaro, R.; et al. An Alternative “Trojan Horse” Hypothesis for COVID-19: Immune Deficiency of IL-10 and SARS-CoV-2 Biology. Endocr. Metab. Immune Disord. Drug Targets 2022, 22, 1–5. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Study Sample (N = 65) | Lower ImAgeS Score (N = 32) | Higher ImAgeS Score (N = 33) | p-Value * |
|---|---|---|---|---|
| Age (years) | 57 (45–66) | 50 (26–61) | 62 (51–68) | 0.001 |
| Mean blood pressure (mmHg) | 95 (91–105) | 92 (86–99) | 99 (87–107) | 0.644 |
| SpO2 (%) | 96 (95–96) | 96 (94–97) | 96 (91–97) | 0.587 |
| Transplant duration (years) | 8 (2–11) | 8 (1–10) | 8 (2–14) | 0.415 |
| Single vaccination dose | 3 (4.6%) | 3 (12.0%) | 0 (0.0%) | 0.080 |
| Double vaccination dose | 11 (16.9%) | 5 (18.5%) | 6 (20.7%) | 0.838 |
| Follow-up (days) | 38 (35–42) | 40 (36–43) | 38 (27–45) | 0.415 |
| Comorbidities | ||||
| Arterial hypertension | 53 (81.5%) | 28 (87.5%) | 25 (75.8%) | 0.223 |
| Diabetes mellitus | 18 (27.7%) | 7 (21.9%) | 11 (33.3%) | 0.302 |
| Chronic heart failure | 5 (7.7%) | 2 (6.3%) | 3 (9.1%) | 0.667 |
| Active smoking | 5 (7.7%) | 4 (12.5%) | 1 (3.0%) | 0.152 |
| Atrial fibrillation | 7 (10.8%) | 5 (15.6%) | 2 (6.1%) | 0.214 |
| Prior AMI | 7 (10.8%) | 2 (6.3%) | 5 (15.2%) | 0.247 |
| Prior CVI | 6 (9.2%) | 3 (9.4%) | 3 (9.1%) | 0.968 |
| PAD | 10 (15.4%) | 4 (12.5%) | 6 (18.2%) | 0.526 |
| COPD/asthma | 4 (6.2%) | 2 (6.3%) | 2 (6.1%) | 0.975 |
| Laboratory parameters | ||||
| WBC (×109/L) | 6.5 (5.3–8.9) | 5.5 (5.4–6.3) | 7.5 (4.4–9.5) | 0.728 |
| Hgb (g/L) | 128.5 (125.0–134.3) | 132.0 (125.0–134.1) | 126.0 (114.0–133.2) | 0.126 |
| Platelets (×103/L) | 240.1 (198.0–262.3) | 191.1 (180.3–245.4) | 257.0 (224.6–275.5) | 0.865 |
| CRP (mmol/L; maximal values) | 72.6 (34.8–121.8) | 72.6 (22.1–51.3) | 72.7 (47.3–122.3) | 0.639 |
| eGFR (mL/min/1.73 m2) | 44.5 (24.8–63.8) | 66.7 (20.8–77.8) | 36.0 (25.3–53.2) | 0.042 |
| D-dimers (mmol/L) | 0.8 (0.6–1.7) | 0.8 (0.4–1.3) | 0.8 (0.6–2.5) | 0.278 |
| Chronic immunosuppressive therapy | ||||
| Mycophenolate Mofetil | 58 (89.2%) | 28 (87.5%) | 30 (90.9%) | 0.658 |
| Azathioprine | 1 (1.5%) | 1 (3.1%) | 0 (0.0%) | 0.306 |
| Cyclosporine | 20 (30.8%) | 8 (25.0%) | 12 (36.4%) | 0.321 |
| Tacrolimus | 36 (55.4%) | 20 (62.5%) | 16 (48.5%) | 0.256 |
| Everolimus | 8 (12.3%) | 4 (12.5%) | 14 (12.1%) | 0.963 |
| Sirolimus | 3 (4.6%) | 1 (3.1%) | 2 (6.1%) | 0.573 |
| Prednisone | 65 (100.0%) | 32 (100.0%) | 33 (100.0%) | / |
| COVID-19 related therapy | ||||
| Convalescent plasma | 6 (9.2%) | 1 (3.1%) | 5 (15.2%) | 0.094 |
| Casirivimab/Imdevimab | 2 (3.1%) | 1 (3.1%) | 1 (3.0%) | 0.982 |
| Remdesivir | 44 (67.7%) | 20 (62.5%) | 24 (72.7%) | 0.378 |
| Oxygen therapy | 24 (36.9%) | 10 (31.3%) | 14 (42.4%) | 0.351 |
| Variables | 30-Day Post-Discharge Mortality | ||||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value * | Harrell’s C Concordance Index | Somers’ D | Hosmer-Lemeshow Test | |
| ImAgeS risk score | 1.04 (1.01–1.08) | 0.040 | 0.699 | 0.397 | 3.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domjanović, J.; Domjanović Škopinić, T.; Gamberažić Kirevski, T.; Matetic, A. External Validation of the ImAgeS Risk Score for Mortality in Hospitalized Kidney Transplant Recipients with COVID-19: A Retrospective Observational Study. BioMed 2023, 3, 207-216. https://doi.org/10.3390/biomed3020018
Domjanović J, Domjanović Škopinić T, Gamberažić Kirevski T, Matetic A. External Validation of the ImAgeS Risk Score for Mortality in Hospitalized Kidney Transplant Recipients with COVID-19: A Retrospective Observational Study. BioMed. 2023; 3(2):207-216. https://doi.org/10.3390/biomed3020018
Chicago/Turabian StyleDomjanović, Josipa, Tea Domjanović Škopinić, Tea Gamberažić Kirevski, and Andrija Matetic. 2023. "External Validation of the ImAgeS Risk Score for Mortality in Hospitalized Kidney Transplant Recipients with COVID-19: A Retrospective Observational Study" BioMed 3, no. 2: 207-216. https://doi.org/10.3390/biomed3020018