
miR-148b as a Potential Biomarker for IgA Nephropathy

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participant Selection
2.2. Study Population Description
2.3. Sample Collection for the microRNA Experiment
2.4. microRNA Quantification
2.5. Histopathological Analysis
2.6. Statistical Analysis
3. Results
3.1. Correlation Analysis
3.2. Logistic Regression Model
3.3. GFR Remission in Follow Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wyatt, R.; Julian, B. IgA nephropathy. N. Engl. J. Med. 2013, 368, 2402–2414. [Google Scholar] [CrossRef]
- Tumlin, J.A.; Madaio, M.P.; Hennigar, R. Idiopathic IgA nephropathy: Pathogenesis, histopathology, and therapeutic options. Clin. J. Am. Soc. Nephrol. 2007, 2, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.F.S.; Roberts, I.S.D. Histologic Classification of IgA Nephropathy: Past, Present, and Future. Semin. Nephrol. 2018, 38, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Jarrick, S.; Lundberg, S.; Welander, A.; Carrero, J.J.; Höijer, J.; Bottai, M.; Ludvigsson, J.F. Mortality in IgA Nephropathy : A Nationwide Population-Based Cohort Study. J. Am. Soc. Nephrol. 2019, 30, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Novak, J.; Barratt, J.; Julian, B.A.; Renfrow. Aberrant Glycosylation of the IgA1 Molecule in IgA Nephropathy. Semin Nephrol. 2018, 38, 461–476. [Google Scholar] [CrossRef]
- Barbour, S.J.; Cattran, D.C.; Kim, S.J.; Levin, A.; Wald, R.; Hladunewich, M.A.; Reich, H.N. Individuals of Pacific Asian origin with IgA nephropathy have an increased risk of progression to end-stage renal disease. Kidney Int. 2013, 84, 1017–1024. [Google Scholar] [CrossRef]
- Zhu, X.; Li, H.; Liu, Y.; You, J.; Qu, Z.; Yuan, S.; Peng, Y.; Liu, F.; Liu, H. Tubular atrophy/interstitial fibrosis scores of Oxford classification combined with proteinuria level at biopsy provides earlier risk prediction in lgA nephropathy. Sci. Rep. 2017, 24, 1100. [Google Scholar] [CrossRef] [PubMed]
- Schena, F.P.; Nistor, I. Epidemiology of IgA Nephropathy: A Global Perspective. Semin. Nephrol. 2018, 38, 435–442. [Google Scholar] [CrossRef]
- Tomino, Y. Diagnosis and treatment of patients with IgA nephropathy in Japan. Kidney Res. Clin. Pract. 2016, 35, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Trimarchi, H.; Barratt, J.; Cattran, D.C.; Cook, H.T.; Coppo, R.; Haas, M.; Liu, Z.H.; Roberts, I.S.; Yuzawa, Y.; Zhang, H.; et al. Oxford Classification of IgA nephropathy 2016: An update from the IgA Nephropathy Classification Working Group. Kidney Int. 2017, 91, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- Barbour, S.J.; Espino-Hernandez, G.; Reich, H.N.; Coppo, R.; Roberts, I.S.; Feehally, J.; Herzenberg, A.M.; Cattran, D.C.; Bavbek, N.; Cook, T.; et al. The MEST score provides earlier risk prediction in lgA nephropathy. Kidney Int. 2016, 89, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.C.; Haas, M.; Reich, H.N. IgA nephropathy. Clin. J. Am. Soc. Nephrol. 2017, 12, 677–686. [Google Scholar] [CrossRef]
- Bartel, D.P. MicroRNAs: Genomics, Biogenesis, Mechanism, and Function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Selvaskandan, H.; Pawluczyk, I.; Barratt, J. MicroRNAs: A new avenue to understand, investigate and treat immunoglobulin A nephropathy? Clin. Kidney J. 2018, 11, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Sallustio, F.; Cox, S.N.; Pesce, F.; Schena, F.P. Abnormal miR-148b Expression Promotes Aberrant Glycosylation of IgA1 in IgA Nephropathy. J. Am. Soc. Nephrol. 2012, 23, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.C.; Li, P.K.T. MicroRNAs in IgA nephropathy. Nat. Rev. Nephrol. 2014, 10, 249–256. [Google Scholar] [CrossRef]
- Serino, G.; Sallustio, F.; Curci, C.; Cox, S.N.; Pesce, F.; De Palma, G.; Schena, F.P. Role of let-7b in the regulation of N-acetylgalactosaminyltransferase 2 in IgA nephropathy. Nephrol. Dial. Transplant. 2015, 30, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Pesce, F.; Sallustio, F.; De Palma, G.; Cox, S.N.; Curci, C.; Zaza, G.; Lai, K.N.; Leung, J.C.; Tang, S.C.; et al. In a retrospective international study, circulating MIR-148b and let-7b were found to be serum markers for detecting primary IgA nephropathy. Kidney Int. 2016, 89, 683–692. [Google Scholar] [CrossRef]
- Placzek, W.J.; Yanagawa, H.; Makita, Y.; Renfrow, M.B.; Julian, B.A.; Rizk, D.V.; Suzuki, Y.; Novak, J.; Suzuki, H. Serum galactose deficient IgA1 and IgG autoantibodies correlate in patients with IgA nephropathy. PLoS ONE 2018, 13, e0190967. [Google Scholar] [CrossRef]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, 753–779. [Google Scholar] [CrossRef]
- Kumar, S.; Priscilla, C.; Parameswaran, S.; Shewade, G.D.; Charan, G.A.; Ganesh, N.R. Mean expression value normalized and absolute quantified miR-21 found to be a potential diagnostic and prognostic marker for IgA nephropathy. Indian J. Sci. Technol. 2020, 13, 1078–1088. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R. Multimodel Inference: Understanding AIC and BIC in Model Selection. Sociol. Methods Res. 2004, 33, 261–304. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-Project.Org/ (accessed on 2 November 2022).
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. ACC/AHA/AAPA/ABC/ ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Hypertension 2018, 71, 351–358. [Google Scholar] [CrossRef]
- Kouri, N.M.; Stangou, M.; Lioulios, G.; Mitsoglou, Z.; Serino, G.; Chiurlia, S.; Cox, S.N.; Stropou, P.; Schena, F.P.; Papagianni, A. Serum Levels of miR-148b and Let-7b at Diagnosis May Have Important Impact in the Response to Treatment and Long-Term Outcome in IgA Nephropathy. J. Clin. Med. 2021, 10, 1987. [Google Scholar] [CrossRef]
- Alkhateeb, D.M.; Altamemi, I.A. Altamemi Circulating Microrna (148b And 150) As Potential Biomarker in IgA Nephropathy and Lupus Nephritis. Ann. RSCB 2021, 25, 6294–6309. [Google Scholar]
- Coppo, R.; D’Arrigo, G.; Tripepi, G.; Russo, M.L.; Roberts, I.S.; Bellur, S.; Cattran, D.; Cook, T.H.; Feehally, J.; Tesar, V.; et al. Is there long-term value of pathology scoring in immunoglobulin A nephropathy? A validation study of the Oxford Classification for IgA Nephropathy (VALIGA) update. Nephrol. Dial. Transplant. 2020, 35, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Maixnerova, D.; Tesar, V. Emerging Modes of Treatment of IgA Nephropathy. Int. J. Mol. Sci. 2020, 21, 9064. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predictive | miR-148b Copy Number | p | let-7b Copy Number | p |
|---|---|---|---|---|
| Parameters | Median (IQR) | Median (IQR) | ||
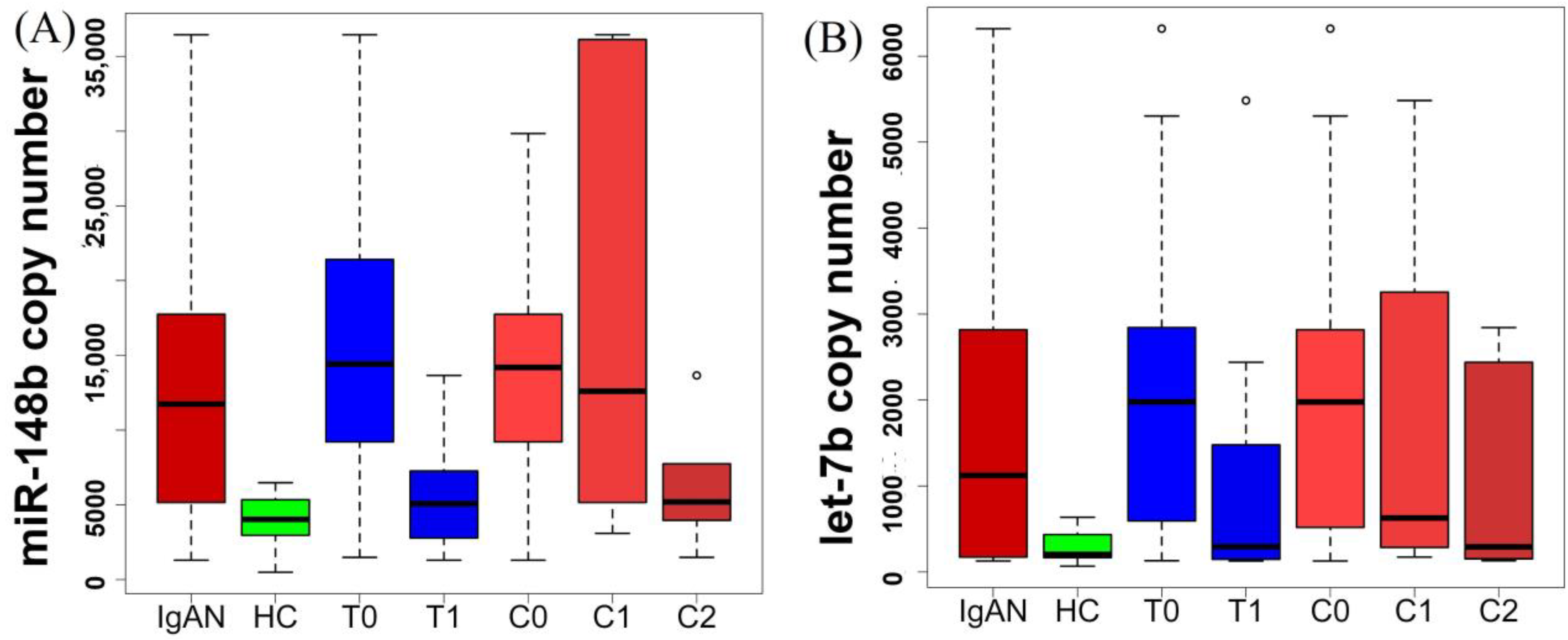
| IgAN | 11,742 (5224–17,694) | 0.0002 | 1124 (202–2808) | 0.0065 |
| HC | 4032 (2970–5342) | 205 (167–435) | ||
| M0 | 7222 (3323–11,742) | 0.2661 | 174 (152–862) | 0.0624 |
| M1 | 13,973 (6104–18,083) | 1990 (468–2900) | ||
| E0 | 10,699 (5159–18,415) | 0.8716 | 1967 (519–2818) | 0.1558 |
| E1 | 12,784 (7745–17,146) | 154 (150–166) | ||
| S0 | 17,146 (7745–25,410) | 0.0313 | 707 (174–2712) | 0.5165 |
| S1 | 6788 (4255–13,658) | 1999 (418–2958) | ||
| T0 | 14,422 (9503–20,665) | 0.003 | 1978 (612–2837) | 0.0959 |
| T1 | 5072 (3520–7027) | 296 (157–999) | ||
| C0 | 14,191 (9503–17,694) | 0.8204 | 1978 (566–2808) | 0.7785 |
| C1 | 12,602 (5566–31,703) | 628 (363–2607) | ||
| C1 | 12,602 (5566–31,703) | 0.2403 | 628 (363–2607) | 0.5025 |
| C2 | 5202 (4222–7164) | 292 (157–1934) | ||
| CKD1 | 17,449 (13,154–19,165) | 0.9333 | 1564 (602–2943) | 0.2141 |
| CKD2 | 15,965 (13,110–20,012) | 2888 (2605–3798) | ||
| CKD2 | 15,965 (13,110–20,012) | 0.9143 | 2888 (2605–3798) | 0.019 |
| CKD3 | 12,404 (8402–30,708) | 628 (279–1005) | ||
| CKD3 | 12,404 (8402–30,708) | 0.0126 | 628 (279–1005) | 0.662 |
| CKD4 | 4112 (2694–5762) | 336 (145–2946) | ||
| CKD4 | 4112 (2694–5762) | 0.4606 | 336 (145–2946) | 0.8081 |
| CKD5 | 9321 (4255–13,658) | 1999 (418–2958) |
| microRNA | Predictive Marker | ρ | p |
|---|---|---|---|
| miR-148b | S | −0.400 | 0.028 |
| T | −0.540 | 0.002 | |
| Systolic BP | −0.490 | 0.006 | |
| Diastolic BP | −0.420 | 0.019 | |
| GFR | 0.533 | 0.002 | |
| let-7b | C3 | 0.360 | 0.047 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, S.; Priscilla, C.; Parameswaran, S.; Shewade, D.G.; Viswanathan, P.; Ganesh, R.N. miR-148b as a Potential Biomarker for IgA Nephropathy. Kidney Dial. 2023, 3, 84-94. https://doi.org/10.3390/kidneydial3010008
Kumar S, Priscilla C, Parameswaran S, Shewade DG, Viswanathan P, Ganesh RN. miR-148b as a Potential Biomarker for IgA Nephropathy. Kidney and Dialysis. 2023; 3(1):84-94. https://doi.org/10.3390/kidneydial3010008
Chicago/Turabian StyleKumar, Santosh, C. Priscilla, Sreejith Parameswaran, Deepak Gopal Shewade, Pragasam Viswanathan, and Rajesh Nachiappa Ganesh. 2023. "miR-148b as a Potential Biomarker for IgA Nephropathy" Kidney and Dialysis 3, no. 1: 84-94. https://doi.org/10.3390/kidneydial3010008