
Symptoms Predicting SARS-CoV-2 Test Results in Resident Physicians and Fellows in New York City

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Mount Sinai Employee COVID-19 Testing and Assessment of SARS-CoV-2 Infection
2.3. Assessment of Symptoms
2.4. Assessment of Sociodemographic and Occupational Factors
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Symptoms Associated with SARS-CoV-2 Test Result
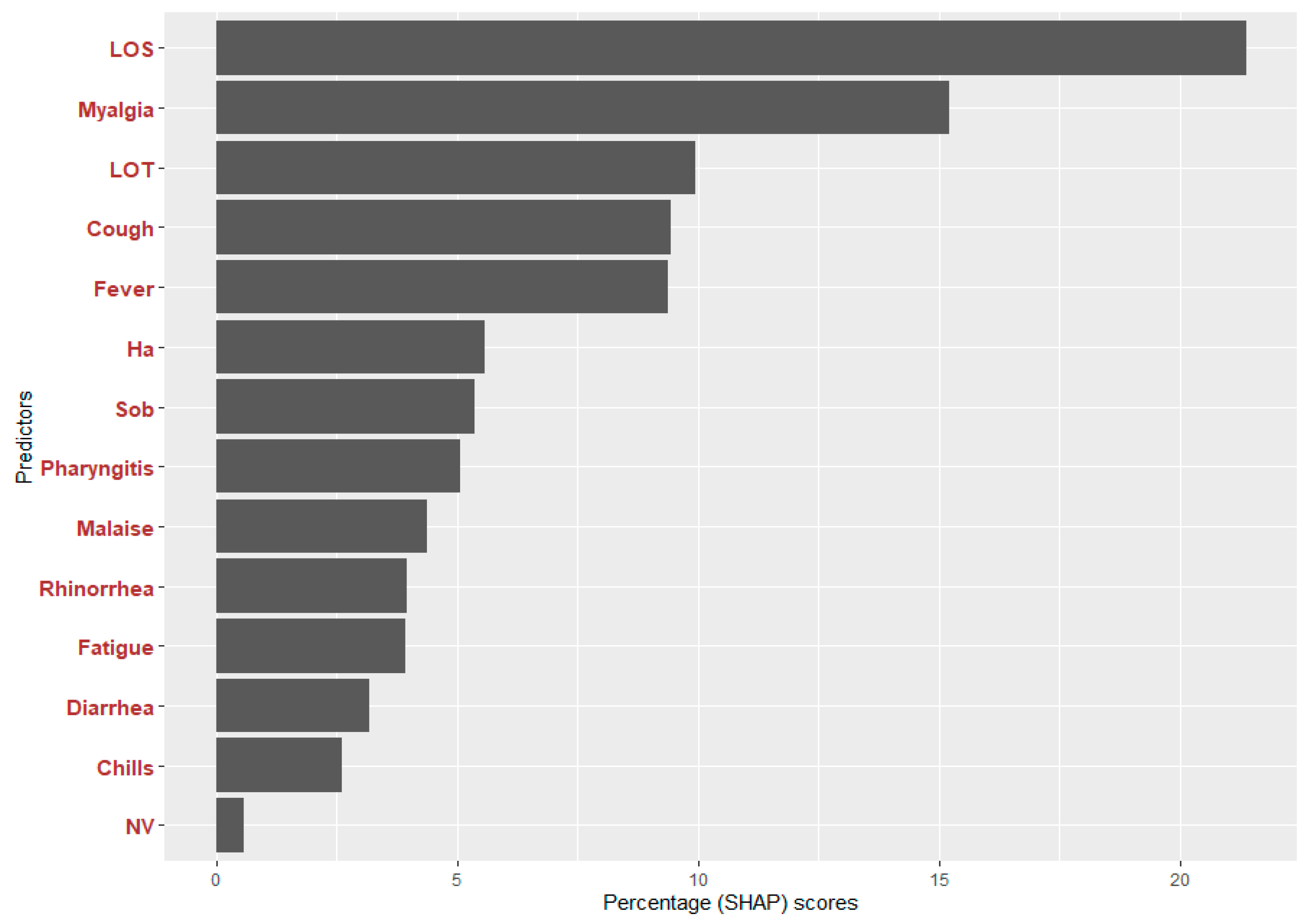
3.3. Symptoms Predicting a Positive SARS-CoV-2 Test Result in the XGBoost Model
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC Confirms First Case of Coronavirus in the United States. 2020. Available online: https://www.cbsnews.com/news/coronavirus-centers-for-disease-control-first-case-united-states/ (accessed on 26 October 2021).
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Kopecki, D. New York City Confirms First Coronavirus Case. CNBC. Available online: https://www.cnbc.com/2020/03/01/first-coronavirus-case-confirmed-in-new-york-city.html (accessed on 2 March 2021).
- At Novel Coronavirus Briefing, Governor Cuomo Declares State of Emergency to Contain Spread of Virus. 2020. Available online: https://www.governor.ny.gov/news/novel-coronavirus-briefing-governor-cuomo-declares-state-emergency-contain-spread-virus (accessed on 26 October 2021).
- Pawloski, K.R.; Kolod, B.; Khan, R.F.; Midya, V.; Chen, T.; Oduwole, A.; Camins, B.; Colicino, E.; Leitman, I.M.; Nabeel, I.; et al. Factors Associated with SARS-CoV-2 Infection in Physician Trainees in New York City during the First COVID-19 Wave. Int. J. Environ. Res. Public Health 2021, 18, 5274. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Hegde, S.; LaFiura, C.; Raghavan, M.; Sun, N.; Cheng, S.; Rebholz, C.M.; Seidelmann, S.B. Access to personal protective equipment in exposed healthcare workers and COVID-19 illness, severity, symptoms and duration: A population-based case-control study in six countries. BMJ Glob. Health 2021, 6, e004611. [Google Scholar] [CrossRef]
- CDCMMWR. Characteristics of Health Care Personnel with COVID-19—United States, February 12–April 9, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 477. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- Rossman, H.; Keshet, A.; Shilo, S.; Gavrieli, A.; Bauman, T.; Cohen, O.; Shelly, E.; Balicer, R.; Geiger, B.; Dor, Y.; et al. A framework for identifying regional outbreak and spread of COVID-19 from one-minute population-wide surveys. Nat. Med. 2020, 26, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Ramírez Varela, A.; Moreno López, S.; Contreras-Arrieta, S.; Tamayo-Cabeza, G.; Restrepo-Restrepo, S.; Sarmiento-Barbieri, I.; Caballero-Díaz, Y.; Jorge Hernandez-Florez, L.; Mario González, J.; Salas-Zapata, L.; et al. Prediction of SARS-COV-2 infection with a symptoms-based model to aid public health decision making in Latin America and other low and middle income settings. Prev. Med. Rep. 2022, 27, 101798. [Google Scholar] [CrossRef] [PubMed]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020, 20, 1401–1408. [Google Scholar] [CrossRef]
- Gholami, M.; Fawad, I.; Shadan, S.; Rowaiee, R.; Ghanem, H.; Hassan Khamis, A.; Ho, S.B. COVID-19 and healthcare workers: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 104, 335–346. [Google Scholar] [CrossRef]
- Baker, J.M.; Nelson, K.N.; Overton, E.; Lopman, B.A.; Lash, T.L.; Photakis, M.; Jacob, J.T.; Roback, J.D.; Fridkin, S.K.; Steinberg, J.P. Quantification of Occupational and Community Risk Factors for SARS-CoV-2 Seropositivity Among Health Care Workers in a Large U.S. Health Care System. Ann. Intern. Med. 2021, 174, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Dzinamarira, T.; Murewanhema, G.; Mhango, M.; Iradukunda, P.G.; Chitungo, I.; Mashora, M.; Makanda, P.; Atwine, J.; Chimene, M.; Mbunge, E.; et al. COVID-19 Prevalence among Healthcare Workers. A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 19, 146. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, H.A.S.; Asif, H.M. Early Detection and Assessment of Covid-19. Front. Med. 2020, 7, 311. [Google Scholar] [CrossRef]
- Bastiani, L.; Fortunato, L.; Pieroni, S.; Bianchi, F.; Adorni, F.; Prinelli, F.; Giacomelli, A.; Pagani, G.; Maggi, S.; Trevisan, C.; et al. Rapid COVID-19 Screening Based on Self-Reported Symptoms: Psychometric Assessment and Validation of the EPICOVID19 Short Diagnostic Scale. J. Med. Internet Res. 2021, 23, e23897. [Google Scholar] [CrossRef]
- Marcus, G.M.; Olgin, J.E.; Peyser, N.D.; Vittinghoff, E.; Yang, V.; Joyce, S.; Avram, R.; Tison, G.H.; Wen, D.; Butcher, X.; et al. Predictors of incident viral symptoms ascertained in the era of COVID-19. PLoS ONE 2021, 16, e0253120. [Google Scholar] [CrossRef]
- Kennedy, B.; Fitipaldi, H.; Hammar, U.; Maziarz, M.; Tsereteli, N.; Oskolkov, N.; Varotsis, G.; Franks, C.A.; Nguyen, D.; Spiliopoulos, L.; et al. App-based COVID-19 syndromic surveillance and prediction of hospital admissions in COVID Symptom Study Sweden. Nat. Commun. 2022, 13, 2110. [Google Scholar] [CrossRef]
- Center for Devices and Radiological Health. EUA Authorized Serology Test Performance. U.S. Food and Drug Administration. 2020. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/eua-authorized-serology-test-performance (accessed on 26 July 2022).
- Covid-19 Diagnostics in Context-Harvard University. 2020. Available online: https://csb.mgh.harvard.edu/covid (accessed on 26 July 2022).
- Chen, T.; Guestrin, C. XGBoost: A scalable tree boosting system. arXiv 2022, arXiv:1603.02754. [Google Scholar]
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.I. From local explanations to global understanding with explainable AI for trees. Nat. Mach. Intell. 2020, 2, 56–67. [Google Scholar] [CrossRef]
- Azeli, Y.; Fernández, A.; Capriles, F.; Rojewski, W.; Lopez-Madrid, V.; Sabaté-Lissner, D.; Serrano, R.M.; Rey-Reñones, C.; Civit, M.; Casellas, J.; et al. A machine learning COVID-19 mass screening based on symptoms and a simple olfactory test. Sci. Rep. 2022, 12, 15622. [Google Scholar] [CrossRef]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19. Cochrane Database Syst. Rev. 2022, 5, CD013665. [Google Scholar] [CrossRef]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Health-Care Workers: A Living Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Savoy, M.; Kopp, B.; Chaouch, A.; Cohidon, C.; Gouveia, A.; Lombardo, P.; Maeder, M.; Payot, S.; Perdrix, J.; Schwarz, J.; et al. Diagnostic performance of individual symptoms to predict SARS-COV-2 RT-PCR positivity and symptom persistence among suspects presenting in primary care during the first wave of covid-19. Infect. Dis. Rep. 2023, 15, 112–124. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | All Participants (n = 328) | By SARS-CoV-2 Status | p-Value | |
|---|---|---|---|---|
| Negative Test Result (n = 262) | Positive Test Result (n = 66) | |||
| Symptoms | ||||
| Cough, n (%) | ||||
| No | 238 (73) | 208 (87) | 30 (13) | <0.001 |
| Yes | 90 (27) | 54 (60) | 36 (40) | |
| Chills, n (%) | ||||
| No | 276 (84) | 241 (87) | 35 (13) | <0.001 |
| Yes | 52 (16) | 21 (40) | 31 (60) | |
| Fever, n (%) | ||||
| No | 269 (82) | 239 (89) | 30 (11) | <0.001 |
| Yes | 59 (18) | 23 (39) | 36 (61) | |
| Fatigue, n (%) | ||||
| No | 220 (67) | 202 (92) | 18 (8) | <0.001 |
| Yes | 108 (33) | 60 (56) | 48 (44) | |
| Myalgia, n (%) | ||||
| No | 250 (76) | 228 (91) | 22 (9) | <0.001 |
| Yes | 78 (24) | 34 (44) | 44 (56) | |
| Headache, n (%) | ||||
| No | 256 (78) | 219 (86) | 37 (14) | <0.001 |
| Yes | 72 (22) | 43 (60) | 29 (40) | |
| Shortness of breath, n (%) | ||||
| No | 284 (87) | 236 (83) | 48 (17) | <0.001 |
| Yes | 44 (13) | 26 (59) | 18 (41) | |
| Sore throat, n (%) | ||||
| No | 257 (78) | 210 (82) | 47 (18) | 0.13 |
| Yes | 71 (22) | 52 (73) | 19 (27) | |
| Diarrhea, n (%) | ||||
| No | 291 (89) | 238 (82) | 53 (18) | 0.02 |
| Yes | 37 (11) | 24 (65) | 13 (35) | |
| Nausea/vomiting, n (%) | ||||
| No | 316 (96) | 256 (81) | 60 (19) | 0.02 |
| Yes | 12 (4) | 6 (50) | 6 (50) | |
| Loss of sense of smell, n (%) | ||||
| No | 283 (86) | 257 (91) | 26 (9) | <0.001 |
| Yes | 45 (14) | 5 (11) | 40 (89) | |
| Loss of sense of taste, n (%) | ||||
| No | 291 (89) | 257 (88) | 34 (12) | <0.001 |
| Yes | 37 (11) | 5 (14) | 32 (86) | |
| Malaise, n (%) | ||||
| No | 274 (84) | 241 (88) | 33 (12) | <0.001 |
| Yes | 54 (16) | 21 (39) | 33 (61) | |
| Runny nose, n (%) | ||||
| No | 266 (81) | 220 (83) | 46 (17) | 0.01 |
| Yes | 62 (19) | 42 (68) | 20 (32) | |
| Sociodemographic and Occupational Factors | ||||
| Sex, n (%) | ||||
| Female | 189 (58) | 155 (82) | 34 (18) | 0.26 |
| Male | 139 (42) | 107 (77) | 32 (23) | |
| Age, years, median (IQR) | 31 (29, 33) | 31 (29, 33) | 30 (28, 33) | 0.36 |
| Race, n (%) | ||||
| Asian | 82 (25) | 71 (87) | 11 (13) | 0.27 |
| Black | 26 (8) | 19 (73) | 7 (27) | |
| White | 202 (63) | 156 (77) | 46 (23) | |
| Other | 12 (4) | 10 (83) | 2 (17) | |
| Missing | 6 | 6 | 0 | |
| Change in usual patient population, n (%) | ||||
| No | 296 (90) | 230 (78) | 66 (22) | 0.003 |
| Yes | 32 (10) | 32 (100) | 0 (0) | |
| Medical–surgical unit, n (%) | ||||
| No | 106 (32) | 89 (84) | 17 (16) | 0.20 |
| Yes | 222 (68) | 173 (78) | 49 (22) | |
| Training specialty, n (%) | ||||
| High-risk Primary Procedural | 52 (16) | 32 (62) | 20 (38) | 0.001 |
| Primary Non-procedural | 213 (67) | 180 (85) | 33 (15) | |
| Surgery/surgical subspecialty | 53 (17) | 41 (77) | 12 (23) | |
| Missing | 10 | 9 | 1 | |
| Symptom | Unadjusted Model | Adjusted Model 2 | ||
|---|---|---|---|---|
| OR 1 | 95% CI 1 | OR 1 | 95% CI 1 | |
| cough | 2.64 | 1.50, 4.67 | 2.99 | 1.87, 4.76 |
| chills | 5.57 | 1.26, 24.56 | 5.78 | 1.05, 31.67 |
| fever | 8.15 | 3.02, 22.00 | 9.17 | 2.20, 38.26 |
| fatigue | 2.23 | 1.42, 3.49 | 2.06 | 1.46, 2.92 |
| myalgia | 3.76 | 1.09, 12.90 | 3.38 | 1.02, 11.18 |
| headache | 1.66 | 1.08, 2.57 | 1.97 | 1.27, 3.05 |
| shortness of breath | 2.43 | 1.07, 5.49 | 3.65 | 1.92, 6.94 |
| pharyngitis | 1.39 | 0.73, 2.67 | 1.39 | 0.78, 2.48 |
| diarrhea | 1.90 | 1.02, 3.52 | 2.05 | 1.01, 4.14 |
| nausea/vomiting | 4.11 | 1.31, 12.90 | 6.31 | 1.49, 26.65 |
| loss of smell | 8.70 | 8.37, 9.03 | 9.18 | 9.11, 9.25 |
| loss of taste | 8.80 | 8.71, 8.88 | 9.77 | 9.68, 9.87 |
| malaise | 6.60 | 3.65, 11.95 | 4.24 | 1.20, 14.97 |
| runny nose | 1.29 | 1.01, 1.64 | 1.54 | 1.05, 2.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, T.P.; Yao, M.; Midya, V.; Kolod, B.; Khan, R.F.; Oduwole, A.; Camins, B.; Leitman, I.M.; Nabeel, I.; Oliver, K.; et al. Symptoms Predicting SARS-CoV-2 Test Results in Resident Physicians and Fellows in New York City. COVID 2023, 3, 671-681. https://doi.org/10.3390/covid3050049
Chen TP, Yao M, Midya V, Kolod B, Khan RF, Oduwole A, Camins B, Leitman IM, Nabeel I, Oliver K, et al. Symptoms Predicting SARS-CoV-2 Test Results in Resident Physicians and Fellows in New York City. COVID. 2023; 3(5):671-681. https://doi.org/10.3390/covid3050049
Chicago/Turabian StyleChen, Tania P., Meizhen Yao, Vishal Midya, Betty Kolod, Rabeea F. Khan, Adeyemi Oduwole, Bernard Camins, I. Michael Leitman, Ismail Nabeel, Kristin Oliver, and et al. 2023. "Symptoms Predicting SARS-CoV-2 Test Results in Resident Physicians and Fellows in New York City" COVID 3, no. 5: 671-681. https://doi.org/10.3390/covid3050049