1. Introduction
Evusheld is a combination injection of tixagevimab and cilgavimab for pre-exposure COVID-19 prophylaxis in adults and adolescents aged 12 years and older. Furthermore, it is indicated for the treatment of adults and adolescents (aged 12 years and older) with COVID-19, who do not require supplemental oxygen and who are at increased risk of progressing to severe COVID-19. In March 2022, the Medicines and Healthcare Products Regulatory Agency (MHRA) authorized its use in immunocompromised individuals where vaccination is minimally effective or not recommended [
1]. Despite early UK approval, the drug was not made available to patients on the National Health Service (NHS) owing to a combination of reasons, and only since October 2022 has Evusheld been available in the UK private sector. The drug still has no agreement for NHS use and NICE (National Institute of Health and Clinical Excellence) review is still ongoing, with particular focus on the true efficacy of the drug against the current COVID-19 variants and final appraisal expected in April 2023 [
2,
3]. Until now, efficacy analysis of Evusheld has focused on reduced risk of COVID-19 infection and subsequent hospitalization and physical health outcome, and the results for immunocompromised patients have been encouraging [
4]. However, anecdotal reports suggest there are additional psychological benefits from Evusheld prophylaxis, particularly in specific immunosuppressed patient groups, although objective supporting data are lacking. Other research has identified poor psychological health consequences arising from the COVID-19 pandemic, with several studies focusing on immunocompromised groups including previous or current cancer patients, but to our knowledge, no studies have specifically addressed potential psychological benefits of using a pre-exposure prophylaxis intervention in a high-risk patient group and seeing whether this improved objective measures of psychological health [
5,
6,
7,
8]. In this study, we created a questionnaire to assess four well-established psychological health parameters in blood cancer patients who did or did not receive Evusheld to assess whether Evusheld treatment improved their psychological health. To give a reference point, we have compared the outcomes of Evusheld-treated patients with a matched control group of blood cancer patients who did not receive Evusheld.
2. Materials and Methods
Our online questionnaire used 35 questions drawn from four established psychological health parameters (EQ5D-3L quality of life (QoL) score, DSM5 Agoraphobia score, Duke’s Social Support Index (DSSI) and the hospital anxiety and depression score (HADS)) to compare psychological wellbeing of patients in the 3-weeks pre- and 3-weeks post-Evusheld and control patients who did not receive Evusheld [
9,
10,
11,
12]. EQ5D-3L is a widely used tool in healthcare economics. It is a descriptive system for health-related QoL states in adults consisting of five dimensions (mobility/self-care/usual activities/pain and discomfort/anxiety and depression) each of which has three severity levels that are described by statements appropriate to that dimension. Patients and controls self-scored in each dimension. In addition, patients and controls self-scored a value between 0–100 to describe their current overall health-related QoL. The DSM5 Agoraphobia score is widely used as a tool to assess fear and anxiety relating to a range of day-to-day interactions an individual might have with their social and physical environment. Scores are self-assessed in 10 separate domains, each scored from 0–4, and a mean score across 10 domains was calculated for each study patient. An individual can therefore score from 0 to 40, with higher scores indicating greater severity of agoraphobia. The grouped data were then compared using paired t-tests, and individual domains were compared using chi-squared analysis. The DSSI is widely used to assess the provision of and satisfaction with social support and is typically assessed in multiple domains. We modified this score to quantify social and work interactions outside of the home environment in three domains: the number of interactions with someone the patient does not live with, the number of times the house was left to go to a social event, and the number of times the house was left to go to a work event. Scores were assessed on a 0–7 scale for the time period 3 weeks prior to the point of assessment. Patients could therefore score 0–14 if they were not working, or 0–21 if working. Grouped scores were assessed as a percentage of total points and were compared using chi-squared tests. The HADS score is used to self-report anxiety on a four-point scale across 14 domains and is a NICE-approved tool to assess anxiety and depression. We used the standard HADS questions but modified the 0–3 score to ask whether each parameter was worse/the same/a little improved/significantly improved post-Evusheld treatment. This gave a total score of 0–42 for each patient, with scores > 14 correlating with improvement in anxiety/depression after Evusheld treatment. The quantifiable difference in HADS score post-Evusheld was expressed as a percentage increase or decrease.
Patients in the experimental group were selected for the study if they had an underlying diagnosis of blood cancer, had received Evusheld and had consented to be approached by email from the cancer center. Not all Evusheld patients had received systemic anti-cancer therapy (SACT), as a number of patients had early-stage blood cancers that were on an initial observation program (e.g., early-stage chronic lymphocytic leukemia). A group of blood cancer patients who did not receive Evusheld but had been treated in the Genesis Care (GC) private clinic with SACT within the preceding 6 months was selected as a control group and were sent a similar questionnaire. This control group was well-matched in terms of demographics, socio-economic grouping, and underlying disease, as they were also blood cancer patients. However, the control group patients had all received SACT in the preceding 6 months and were therefore a potentially more immunosuppressed group of patients than the Evusheld group. The study was approved by GC and all patients had consented to email contact. Questionnaire replies were anonymized, and free-text comments were invited. Non-Evusheld patients had an additional three questions to establish why they had not received Evusheld.
3. Results
In total, 29/40 Evusheld patients and 54/100 control patients responded to the questionnaire. With three Evusheld patients, the drug was paid for by the insurance company/employer, but for 37/40 the drug was self-funded. For the control patients, 44% were aware of Evusheld but chose not to have the drug, with cost being the majority reason cited. The majority of control patients (56%) were not aware of Evusheld, primarily because they had not discussed the drug with their managing hematologist. Analysis of EQ5D data (
Supplementary Table S1) showed that Evusheld did not impact ‘mobility’, ‘self-care’, or ‘pain/discomfort’ scores, and patient and control groups scored at similar levels. Evusheld did, however, improve the ‘usual activities’ and ‘anxiety/depression’ scores of EQ5D, with 48.3% of patients reporting some level of problem completing usual activities pre-Evusheld, decreasing to 18.5% post-Evusheld (
p = 0.02). The control group reported 21.8%. Similarly, pre-Evusheld, 55.2% of patients suffered from some level of anxiety/depression, decreasing to 32.1% post-Evusheld (
p = 0.03) (control = 34.5%). Additionally, the EQ5D mean measure of global health increased from 68.5% to 75.5% following Evusheld treatment (
p = 0.03) (control = 75.7%). Overall, therefore, Evusheld treatment was associated with a statistically significant benefit in three of five EQ5D dimensions using chi-squared analysis and an improved global health score using a paired t-test. Of note, after Evusheld treatment, all EQ5D scores were highly similar to the baseline scores of the non-Evusheld control group using chi-squared analysis.
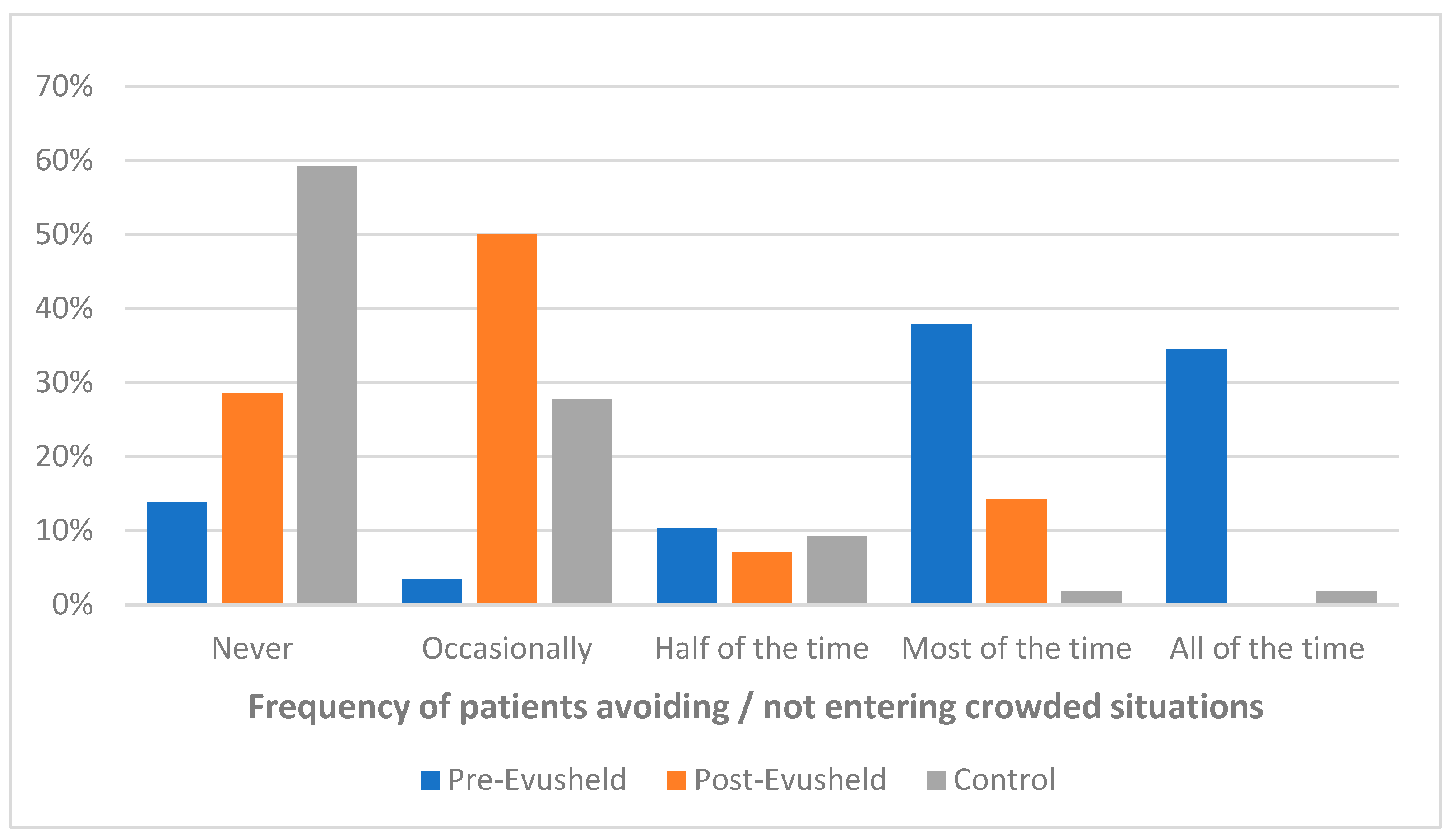
Evusheld also showed improvements in the DSM5 agoraphobia score (
Supplementary Table S2), reducing the mean score from 15.7/40 pre-Evusheld to 5.1/40 post-Evusheld (
p < 0.001). The post-Evusheld DSM5 score was statistically equivalent to the control non-Evusheld patient score of 3.7/40. The most notable change for Evusheld patients was with the parameter of willingness to enter crowded situations. Before Evusheld, 72.5% of patients avoided crowded situations all or most of the time. This decreased to 14.3% after Evusheld (
p < 0.001). Interestingly, this was one parameter that remained statistically different from control patients (control = 3.7%;
p < 0.05;
Figure 1) suggesting that even though Evusheld improved the willingness to enter crowded situations, the Evusheld patients remained more concerned about this key marker of social interaction compared with control patients.
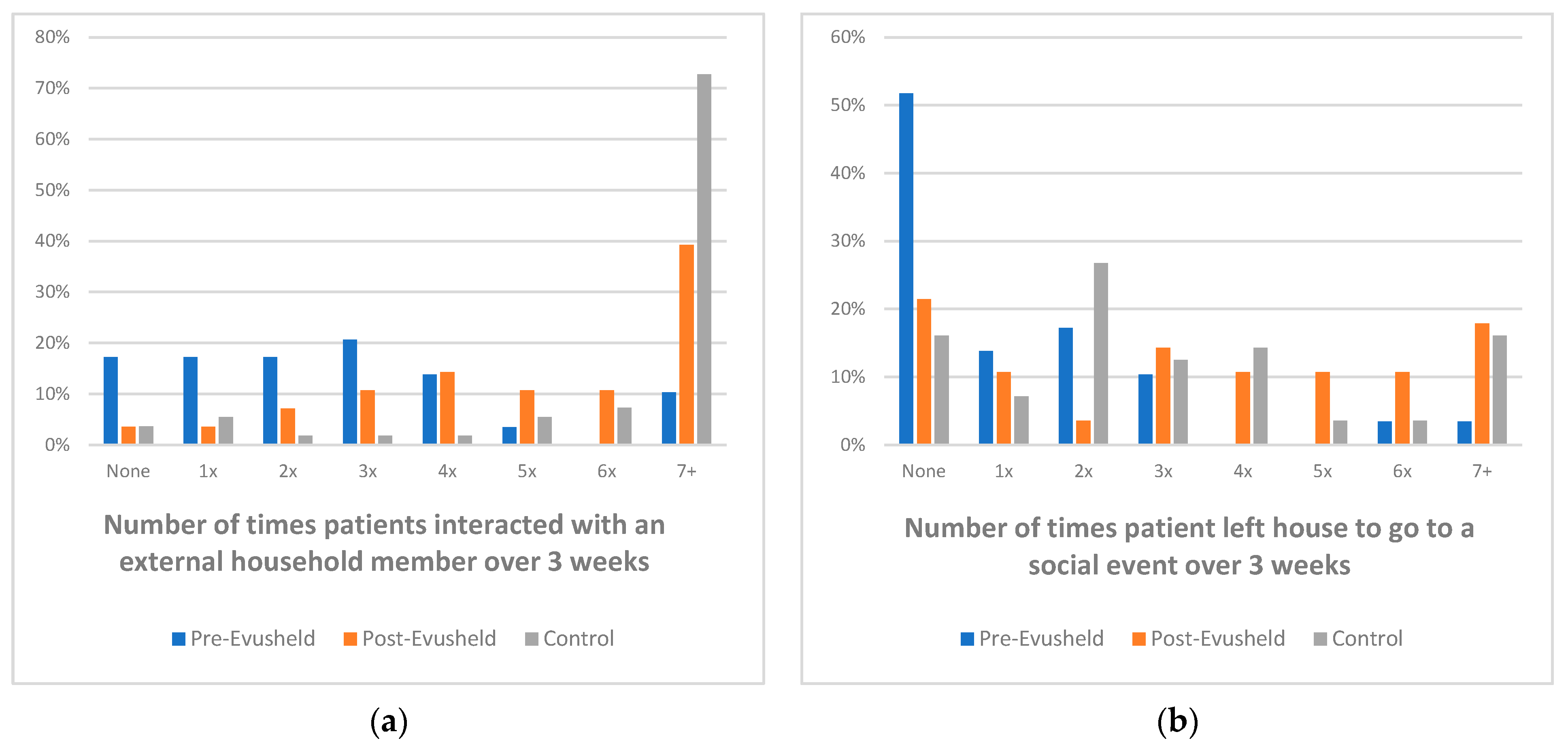
The DSSI score (
Supplementary Table S3) showed that the mean number of interactions with external household contacts (social/work) increased from 1.48 external interactions in the 3 weeks pre-Evusheld to 3.37 in the 3-weeks post-Evusheld (
p < 0.001) (control = 3.77;
Figure 2a). Indeed, in the 3-weeks pre-Evusheld, 52% of patients had no social interactions outside of their household, which reduced to 20% of patients in the 3-weeks post-Evusheld (
p = 0.002) which was statistically similar to the control group (17%;
Figure 2b). Furthermore, the average total score from the 14 HADS domains was 24.7 (a score of 14 = no change following Evusheld treatment), with 25.4% of scores ranks as “significantly improved” and 25.4% ranked as “a little improved” with Evusheld treatment (
Supplementary Table S4). The HADS domain ranked as the most improved with Evusheld was “I look forward with enjoyment to things” with 45% of patients ranking this as “significantly improved”. The HADS domain that changed the least with Evusheld treatment was “I have lost interest in my appearance” with 72% of patients reporting no difference with Evusheld treatment.
Free-text comments from patients showed an overwhelmingly positive impact of Evusheld, with most comments highlighting improved QoL/social mobility and their belief that Evusheld should be more widely accessible (
Supplementary Table S5). Indeed, when control patients were asked why they did not have Evusheld, 42.6% said their decision was financially motivated to some extent (
Supplementary Table S6). Similarly, 26.9% of control patients stated they would have had Evusheld if it had been covered by their private health insurer or the NHS.
4. Discussion
Previous research has identified poor psychological health consequences arising from the COVID-19 pandemic, with several studies focusing on immunocompromised groups including previous or current cancer patients [
5,
6,
7,
8]. One study investigated the effect of COVID-19 vaccination on mental health and concluded that vaccination is associated with decreased distress and perceived risk of infection, hospitalization and death [
13]. Our study followed on from these findings, investigating whether pre-exposure prophylaxis with Evusheld reduces the mental health burden of COVID-19 in blood cancer patients. Using a variety of established psychological health assessment questionnaires, we were able to quantify key psychological wellbeing parameters including anxiety, depression, agoraphobia and QoL and further assess patients’ willingness to partake in social interactions. We assessed the same parameters in a relatively well-matched group of patients who did not receive Evusheld, aiming to address potential bias in the Evusheld patient group; patients suffering a greater psychological burden from the fear of COVID-19 are potentially more likely to both self-fund Evusheld and report benefit from the treatment. Accepting this limitation, our data did confirm that patients reported clearly improved QoL, agoraphobia, anxiety and depression scores following Evusheld treatment. As the average number of social interactions post-Evusheld increased 2.5-fold, this may have been a key driver in improving other measured parameters. Clearly, Evusheld patients had a higher baseline psychological burden compared with control patients, as across all parameters assessed, control patients had baseline psychological scores very similar to Evusheld patients after treatment. The one parameter which did not return to control levels after Evusheld treatment was the agoraphobia parameter of ‘willingness to enter crowded situations’. The data suggest that the patients choosing to be treated with Evusheld remain the most anxious, and despite the additional psychological gain that they derive from Evusheld they remain more cautious about entering crowded situations than their non-Evusheld counterparts. This suggests that patients who had the most to gain psychologically from Evusheld were likely those with higher baseline depression, anxiety and agoraphobia scores. Across all parameters, it appears that the control patients who either chose not to have Evusheld for a range of reasons including cost, or were not aware that Evusheld treatment was an option, had better baseline psychological health parameters than the Evusheld group. In almost every domain assessed, Evusheld treatment improved psychological health scores to match the scores of non-treated control patients. This implies that the control group may have benefited less from Evusheld, although a sizable minority of the control group indicated in free-text comments that they would have preferred Evusheld treatment if the funding was in place. Although this group had better baseline psychological scores than the Evusheld group, this does not mean that the control patients would not also have benefited from Evusheld treatment. Potentially these patients with relatively good psychological health parameters could have improved even further with Evusheld treatment.
Study Limitations
There are three key limitations with this study, namely (1) the small sample size, (2) the inevitable bias introduced by the self-funding nature of the Evusheld patients in 37/40 cases and (3) variability in the control group. Despite the sample size being small, the key observations were validated by robust statistical significance of differences when comparing pre- and post-Evusheld treatment and comparing outcomes against control patients. As the Evusheld patients chose to pay for the drug, it would be expected that these patients would have higher baseline anxiety/agoraphobia scores, and this was indeed reflected in the majority of parameters assessed compared with control patients. This does not, however, invalidate the results, as our data clearly show that highly anxious vulnerable patients can gain significant benefits in terms of psychological health and QoL from receiving a prophylactic treatment aimed at preventing COVID-19 infection. The control group is very similar but not matched exactly to the Evusheld group. From the survey results, approximately half of control patients chose not to have Evusheld based on cost/perceived benefit and around half had not discussed the option of Evusheld treatment with their managing haematologist. A post-hoc analysis of results comparing these two groups of control patients revealed minimal differences in baseline psychological health, and we felt that the study remained more robust by grouping these control patients together as per the original experimental plan.

{kind=link}
{kind=link}

