
Asymptomatic Hypoxemia as a Characteristic Symptom of Coronavirus Disease: A Narrative Review of Its Pathophysiology


Abstract
:1. Introduction
2. Hypoxia and Hypoxemia
3. Hypoxemia in COVID-19 Patients
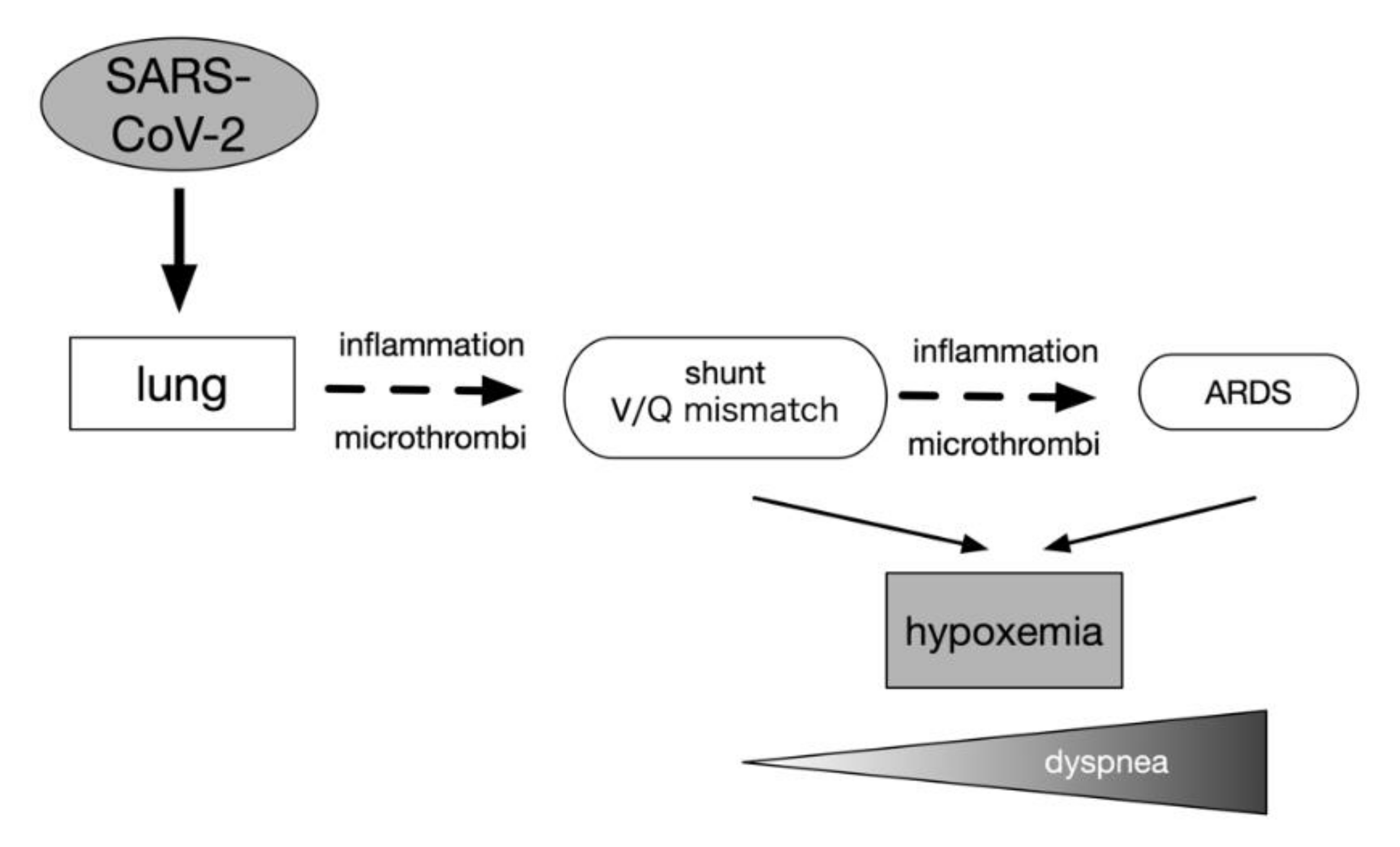
3.1. Mechanisms of Hypoxemia
3.2. Changes in the Oxygen Dissociation Curve
3.3. Accuracy and Limitations of Pulse Oximeter
4. Dyspnea
4.1. Chemoreceptors of Arterial Oxygen Tension
4.2. Information Transmission and Processing from Peripheral Receptors to the Central Receptors
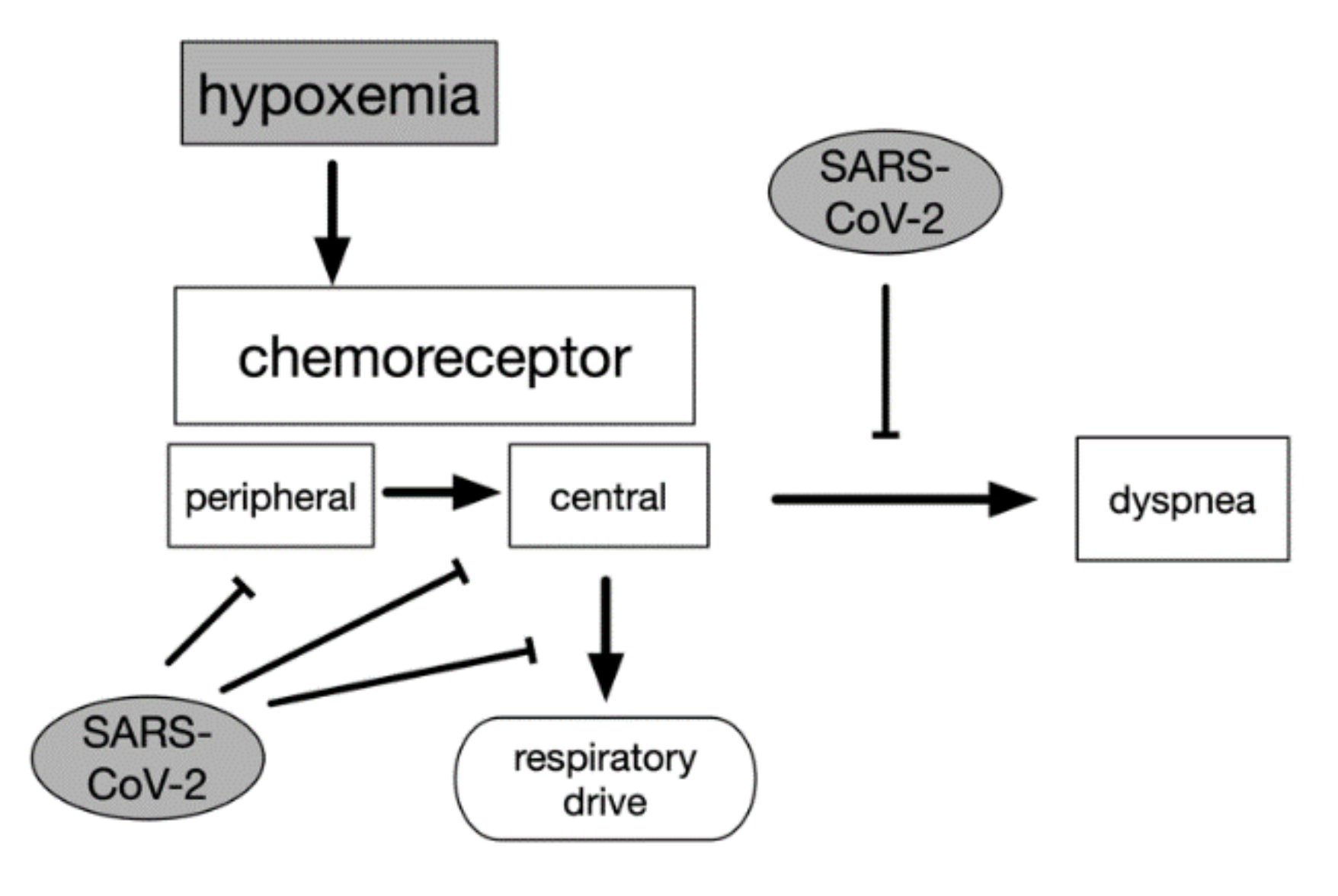
4.3. Pathogenesis of Dyspnea
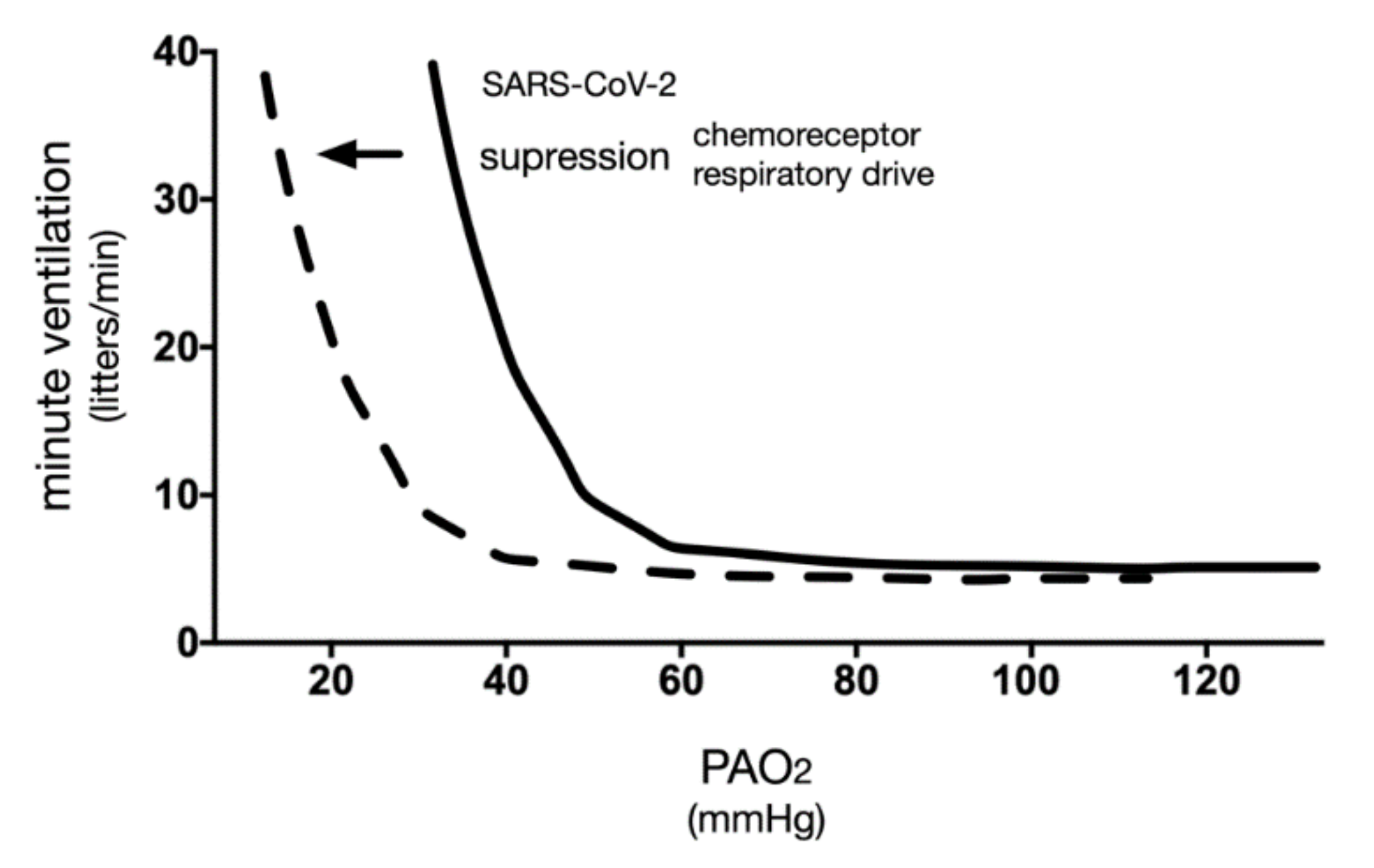
4.4. Relationship between Partial Pressure of Arterial Blood Oxygen and Respiratory Response
5. COVID-19 and Asymptomatic Hypoxemia
5.1. Possible Neuroinvasion by SARS-CoV-2
5.2. Anosmia or Absence of the Sense of Smell
5.3. Inflammatory Responses
6. Is Asymptomatic Hypoxemia a “Paradoxical” Phenomenon?
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 Variants—Clinical, Public Health, and Vaccine Implications. N. Engl. J. Med. 2021, 384, 1866–1868. [Google Scholar] [CrossRef] [PubMed]
- Oran, D.P.; Topol, E.J. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic: A Systematic Review. Ann. Intern. Med. 2021, 174, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Tan, R.Q.; Li, W.T.V.; Shum, W.Z.; Chu, S.C.; Li, H.L.; Shea, Y.F.; Chung, T.W. A systematic review and meta-analysis protocol examining the clinical characteristics and epidemiological features of olfactory dysfunction (OD) in coronavirus disease 2019 (COVID-19). Syst. Rev. 2021, 10, 73. [Google Scholar] [CrossRef]
- National Center for Global Health and Medicine. COVID-19 Registry Japan (COVIREGI-JP). Available online: https://covid-registry.ncgm.go.jp/ (accessed on 28 December 2021).
- Dhont, S.; Derom, E.; Van Braeckel, E.; Depuydt, P.; Lambrecht, B.N. The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respir. Res. 2020, 21, 198. [Google Scholar] [CrossRef]
- Couzin-Frankel, J. The mystery of the pandemic’s ‘happy hypoxia’. Science 2020, 368, 455–456. [Google Scholar] [CrossRef]
- Wadman, M.; Couzin-Frankel, J.; Kaiser, J.; Matacic, C. A rampage through the body. Science 2020, 368, 356–360. [Google Scholar] [CrossRef]
- Clinical Practice Guide Review Committee. Guideline of the Treatment of New Coronavirus Infections (COVID-19), 5th ed. Available online: https://www.mhlw.go.jp/content/000785013.pdf (accessed on 28 December 2021).
- Hasell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Roser, M.; Ritchie, H. A cross-country database of COVID-19 testing. Sci. Data 2020, 7, 345. [Google Scholar] [CrossRef]
- @dajhiroki. Available online: https://twitter.com/dajhiroki/status/1348896174497955840?s=21 (accessed on 28 December 2021).
- Hirota, K. Basic Biology of Hypoxic Responses Mediated by the Transcription Factor HIFs and its Implication for Medicine. Biomedicines 2020, 8, 32. [Google Scholar] [CrossRef] [Green Version]
- Hirota, K. Hypoxia-dependent signaling in perioperative and critical care medicine. J. Anesth. 2021, 35, 741–756. [Google Scholar] [CrossRef]
- Bateman, N.T.; Leach, R.M. ABC of oxygen. Acute oxygen therapy. BMJ 1998, 317, 798–801. [Google Scholar] [CrossRef]
- Evans, T.W.; Smithies, M. ABC of intensive care: Organ dysfunction. BMJ 1999, 318, 1606–1609. [Google Scholar] [CrossRef]
- Jouffroy, R.; Jost, D.; Prunet, B. Prehospital pulse oximetry: A red flag for early detection of silent hypoxemia in COVID-19 patients. Crit. Care 2020, 24, 313. [Google Scholar] [CrossRef]
- Quaresima, V.; Ferrari, M. COVID-19: Efficacy of prehospital pulse oximetry for early detection of silent hypoxemia. Crit. Care 2020, 24, 501. [Google Scholar] [CrossRef]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensive Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef]
- Archer, S.L.; Sharp, W.W.; Weir, E.K. Differentiating COVID-19 Pneumonia from Acute Respiratory Distress Syndrome and High Altitude Pulmonary Edema: Therapeutic Implications. Circulation 2020, 142, 101–104. [Google Scholar] [CrossRef]
- Lang, M.; Som, A.; Mendoza, D.P.; Flores, E.J.; Reid, N.; Carey, D.; Li, M.D.; Witkin, A.; Rodriguez-Lopez, J.M.; Shepard, J.O.; et al. Hypoxaemia related to COVID-19: Vascular and perfusion abnormalities on dual-energy CT. Lancet Infect. Dis 2020, 20, 1365–1366. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Y.; Zhang, C.; Huang, F.; Wang, F.; Yuan, J.; Wang, Z.; Li, J.; Li, J.; Feng, C.; et al. Clinical and biochemical indexes from 2019-nCoV infected patients linked to viral loads and lung injury. Sci. China Life Sci. 2020, 63, 364–374. [Google Scholar] [CrossRef] [Green Version]
- Tay, M.Z.; Poh, C.M.; Renia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Jia, H.P.; Look, D.C.; Shi, L.; Hickey, M.; Pewe, L.; Netland, J.; Farzan, M.; Wohlford-Lenane, C.; Perlman, S.; McCray, P.B., Jr. ACE2 receptor expression and severe acute respiratory syndrome coronavirus infection depend on differentiation of human airway epithelia. J. Virol. 2005, 79, 14614–14621. [Google Scholar] [CrossRef] [Green Version]
- Ostergaard, L. SARS CoV-2 related microvascular damage and symptoms during and after COVID-19: Consequences of capillary transit-time changes, tissue hypoxia and inflammation. Physiol. Rep. 2021, 9, e14726. [Google Scholar] [CrossRef]
- Campbell, C.M.; Kahwash, R. Will Complement Inhibition Be the New Target in Treating COVID-19-Related Systemic Thrombosis? Circulation 2020, 141, 1739–1741. [Google Scholar] [CrossRef] [Green Version]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef] [PubMed]
- Boning, D.; Kuebler, W.M.; Bloch, W. The oxygen dissociation curve of blood in COVID-19. Am. J. Physiol. Lung Cell Mol. Physiol. 2021, 321, L349–L357. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, C.; Steinlechner, B.; Gruber, E.; Simon, P.; Wollenek, G. The oxygen dissociation curve: Quantifying the shift. Perfusion 2004, 19, 141–144. [Google Scholar] [CrossRef]
- Nitzan, M.; Nitzan, I.; Arieli, Y. The Various Oximetric Techniques Used for the Evaluation of Blood Oxygenation. Sensors 2020, 20, 4844. [Google Scholar] [CrossRef]
- Louie, A.; Feiner, J.R.; Bickler, P.E.; Rhodes, L.; Bernstein, M.; Lucero, J. Four Types of Pulse Oximeters Accurately Detect Hypoxia during Low Perfusion and Motion. Anesthesiology 2018, 128, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Bickler, P.E.; Feiner, J.R.; Severinghaus, J.W. Effects of skin pigmentation on pulse oximeter accuracy at low saturation. Anesthesiology 2005, 102, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Sjoding, M.W.; Dickson, R.P.; Iwashyna, T.J.; Gay, S.E.; Valley, T.S. Racial Bias in Pulse Oximetry Measurement. N. Engl. J. Med. 2020, 383, 2477–2478. [Google Scholar] [CrossRef] [PubMed]
- Pulse Oximeter Accuracy and Limitations: FDA Safety Communication. Available online: https://www.fda.gov/medical-devices/safety-communications/pulse-oximeter-accuracy-and-limitations-fda-safety-communication (accessed on 6 February 2021).
- Manning, H.L.; Schwartzstein, R.M. Pathophysiology of dyspnea. N. Engl. J. Med. 1995, 333, 1547–1553. [Google Scholar] [CrossRef]
- Nishino, T. Dyspnoea: Underlying mechanisms and treatment. Br. J. Anaesth. 2011, 106, 463–474. [Google Scholar] [CrossRef] [Green Version]
- Simon, P.M.; Schwartzstein, R.M.; Weiss, J.W.; Fencl, V.; Teghtsoonian, M.; Weinberger, S.E. Distinguishable types of dyspnea in patients with shortness of breath. Am. Rev. Respir. Dis. 1990, 142, 1009–1014. [Google Scholar] [CrossRef]
- Simon, P.M.; Schwartzstein, R.M.; Weiss, J.W.; Lahive, K.; Fencl, V.; Teghtsoonian, M.; Weinberger, S.E. Distinguishable sensations of breathlessness induced in normal volunteers. Am. Rev. Respir. Dis. 1989, 140, 1021–1027. [Google Scholar] [CrossRef]
- Campbell, E.J.; Howell, J.B. The sensation of breathlessness. Br. Med. Bull. 1963, 19, 36–40. [Google Scholar] [CrossRef]
- Nishino, T.; Yashiro, E.; Yogo, H.; Isono, S.; Shinozuka, N.; Ishikawa, T. Comparison of pain and dyspnea perceptual responses in healthy subjects. Pain 2010, 148, 426–430. [Google Scholar] [CrossRef]
- Caretta, A.; Mucignat-Caretta, C. Are Multiple Chemosensory Systems Accountable for COVID-19 Outcome? J. Clin. Med. 2021, 10, 5601. [Google Scholar] [CrossRef]
- Alayash, A.I. The Impact of COVID-19 Infection on Oxygen Homeostasis: A Molecular Perspective. Front. Physiol. 2021, 12, 711976. [Google Scholar] [CrossRef]
- Iannaccone, G.; Scacciavillani, R.; Del Buono, M.G.; Camilli, M.; Ronco, C.; Lavie, C.J.; Abbate, A.; Crea, F.; Massetti, M.; Aspromonte, N. Weathering the Cytokine Storm in COVID-19: Therapeutic Implications. Cardiorenal Med. 2020, 10, 277–287. [Google Scholar] [CrossRef]
- Berger, A.J.; Mitchell, R.A.; Severinghaus, J.W. Regulation of respiration (third of three parts). N. Engl. J. Med. 1977, 297, 194–201. [Google Scholar] [CrossRef]
- Kaufman, M.P.; Iwamoto, G.A.; Ashton, J.H.; Cassidy, S.S. Responses to inflation of vagal afferents with endings in the lung of dogs. Circ. Res. 1982, 51, 525–531. [Google Scholar] [CrossRef] [Green Version]
- Coleridge, J.C.; Coleridge, H.M. Afferent vagal C fibre innervation of the lungs and airways and its functional significance. Rev. Physiol. Biochem. Pharmacol. 1984, 99, 1–110. [Google Scholar] [CrossRef]
- Gandevia, S.C.; Macefield, G. Projection of low-threshold afferents from human intercostal muscles to the cerebral cortex. Respir. Physiol. 1989, 77, 203–214. [Google Scholar] [CrossRef]
- American Thoracic Society. Dyspnea. Mechanisms, assessment, and management: A consensus statement. American Thoracic Society. Am. J. Respir. Crit. Care Med. 1999, 159, 321–340. [Google Scholar] [CrossRef]
- Fukushi, I.; Pokorski, M.; Okada, Y. Mechanisms underlying the sensation of dyspnea. Respir. Investig. 2021, 59, 66–80. [Google Scholar] [CrossRef]
- Parshall, M.B.; Schwartzstein, R.M.; Adams, L.; Banzett, R.B.; Manning, H.L.; Bourbeau, J.; Calverley, P.M.; Gift, A.G.; Harver, A.; Lareau, S.C.; et al. An official American Thoracic Society statement: Update on the mechanisms, assessment, and management of dyspnea. Am. J. Respir. Crit. Care Med. 2012, 185, 435–452. [Google Scholar] [CrossRef] [Green Version]
- Tobin, M.J. Basing Respiratory Management of COVID-19 on Physiological Principles. Am. J. Respir. Crit. Care Med. 2020, 201, 1319–1320. [Google Scholar] [CrossRef] [Green Version]
- Tobin, M.J. Dyspnea. Pathophysiologic basis, clinical presentation, and management. Arch. Intern. Med. 1990, 150, 1604–1613. [Google Scholar] [CrossRef]
- Weil, J.V.; Byrne-Quinn, E.; Sodal, I.E.; Friesen, W.O.; Underhill, B.; Filley, G.F.; Grover, R.F. Hypoxic ventilatory drive in normal man. J. Clin. Investig. 1970, 49, 1061–1072. [Google Scholar] [CrossRef] [Green Version]
- Moosavi, S.H.; Golestanian, E.; Binks, A.P.; Lansing, R.W.; Brown, R.; Banzett, R.B. Hypoxic and hypercapnic drives to breathe generate equivalent levels of air hunger in humans. J. Appl. Physiol. 2003, 94, 141–154. [Google Scholar] [CrossRef] [Green Version]
- Mohan, R.; Duffin, J. The effect of hypoxia on the ventilatory response to carbon dioxide in man. Respir. Physiol. 1997, 108, 101–115. [Google Scholar] [CrossRef]
- Petersson, J.; Glenny, R.W. Gas exchange and ventilation-perfusion relationships in the lung. Eur. Respir. J. 2014, 44, 1023–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bickler, P.E.; Feiner, J.R.; Lipnick, M.S.; Batchelder, P.; MacLeod, D.B.; Severinghaus, J.W. Effects of Acute, Profound Hypoxia on Healthy Humans: Implications for Safety of Tests Evaluating Pulse Oximetry or Tissue Oximetry Performance. Anesth. Analg. 2017, 124, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Singh, A.; Khan, A.A.; Gupta, V. Immune mediating molecules and pathogenesis of COVID-19-associated neurological disease. Microb. Pathog. 2021, 158, 105023. [Google Scholar] [CrossRef]
- Rogers, J.P.; Watson, C.J.; Badenoch, J.; Cross, B.; Butler, M.; Song, J.; Hafeez, D.; Morrin, H.; Rengasamy, E.R.; Thomas, L.; et al. Neurology and neuropsychiatry of COVID-19: A systematic review and meta-analysis of the early literature reveals frequent CNS manifestations and key emerging narratives. J. Neurol. Neurosurg. Psychiatry 2021, 92, 932–941. [Google Scholar] [CrossRef]
- Simonson, T.S.; Baker, T.L.; Banzett, R.B.; Bishop, T.; Dempsey, J.A.; Feldman, J.L.; Guyenet, P.G.; Hodson, E.J.; Mitchell, G.S.; Moya, E.A.; et al. Silent hypoxaemia in COVID-19 patients. J. Physiol. 2020, 599, 1057–1065. [Google Scholar] [CrossRef]
- Anoop, U.R.; Verma, K. Happy Hypoxemia in COVID-19-A Neural Hypothesis. ACS Chem. Neurosci. 2020, 11, 1865–1867. [Google Scholar] [CrossRef]
- Korompoki, E.; Gavriatopoulou, M.; Hicklen, R.S.; Ntanasis-Stathopoulos, I.; Kastritis, E.; Fotiou, D.; Stamatelopoulos, K.; Terpos, E.; Kotanidou, A.; Hagberg, C.A.; et al. Epidemiology and organ specific sequelae of post-acute COVID19: A narrative review. J. Infect. 2021, 83, 1–16. [Google Scholar] [CrossRef]
- Whitmore, H.A.B.; Kim, L.A. Understanding the Role of Blood Vessels in the Neurological Manifestations of COVID-19. Am. J. Pathol. 2021, 191, 1946–1954. [Google Scholar] [CrossRef]
- Melegari, G.; Rivi, V.; Zelent, G.; Nasillo, V.; De Santis, E.; Melegari, A.; Bevilacqua, C.; Zoli, M.; Meletti, S.; Barbieri, A. Mild to Severe Neurological Manifestations of COVID-19: Cases Reports. Int. J. Environ. Res. Public Health 2021, 18, 3673. [Google Scholar] [CrossRef]
- Lambermont, B.; Davenne, E.; Maclot, F.; Delvenne, P. SARS-CoV-2 in carotid body. Intensive Care Med. 2021, 47, 342–343. [Google Scholar] [CrossRef]
- Porzionato, A.; Emmi, A.; Stocco, E.; Barbon, S.; Boscolo-Berto, R.; Macchi, V.; De Caro, R. The potential role of the carotid body in COVID-19. Am. J. Physiol. Lung Cell Mol. Physiol. 2020, 319, L620–L626. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Stoyanov, G.S.; Petkova, L.; Dzhenkov, D.L.; Sapundzhiev, N.R.; Todorov, I. Gross and Histopathology of COVID-19 With First Histology Report of Olfactory Bulb Changes. Cureus 2020, 12, e11912. [Google Scholar] [CrossRef]
- Xia, L.; Bartlett, D., Jr.; Leiter, J.C. Interleukin-1beta and interleukin-6 enhance thermal prolongation of the LCR in decerebrate piglets. Respir. Physiol. Neurobiol. 2016, 230, 44–53. [Google Scholar] [CrossRef] [Green Version]
- Okuhama, A.; Ishikane, M.; Hotta, M.; Sato, L.; Akiyama, Y.; Morioka, S.; Suzuki, S.; Tajima, T.; Yamamoto, M.; Teruya, K.; et al. Clinical and radiological findings of silent hypoxia among COVID-19 patients. J. Infect. Chemother. 2021, 27, 1536–1538. [Google Scholar] [CrossRef]
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; Marder, E.P.; Raz, K.M.; El Burai Felix, S.; Tie, Y.; Fullerton, K.E. Coronavirus Disease 2019 Case Surveillance—United States, January 22–May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 759–765. [Google Scholar] [CrossRef]
- Rosas, I.O.; Brau, N.; Waters, M.; Go, R.C.; Hunter, B.D.; Bhagani, S.; Skiest, D.; Aziz, M.S.; Cooper, N.; Douglas, I.S.; et al. Tocilizumab in Hospitalized Patients with Severe Covid-19 Pneumonia. N. Engl. J. Med. 2021, 384, 1503–1516. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elements of Silent Hypoxemia |
|---|
| hypoxemia: PaO2↓, SaO2↓ |
| dyspnea (-) |
| air hunger (-) |
| breathing effort (-) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirota, K.; Mayahara, T.; Fujii, Y.; Nishi, K. Asymptomatic Hypoxemia as a Characteristic Symptom of Coronavirus Disease: A Narrative Review of Its Pathophysiology. COVID 2022, 2, 47-59. https://doi.org/10.3390/covid2010004
Hirota K, Mayahara T, Fujii Y, Nishi K. Asymptomatic Hypoxemia as a Characteristic Symptom of Coronavirus Disease: A Narrative Review of Its Pathophysiology. COVID. 2022; 2(1):47-59. https://doi.org/10.3390/covid2010004
Chicago/Turabian StyleHirota, Kiichi, Taku Mayahara, Yosuke Fujii, and Kenichiro Nishi. 2022. "Asymptomatic Hypoxemia as a Characteristic Symptom of Coronavirus Disease: A Narrative Review of Its Pathophysiology" COVID 2, no. 1: 47-59. https://doi.org/10.3390/covid2010004