
Molecular Identification of Blastocystis hominis Isolates in Patients with Autoimmune Diseases
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Settings
2.2. Data and Sample Collection
2.3. Laboratory Investigations
2.4. Blastocystis Hominis Stool PCR
2.5. Data Processing and Statistical Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Badparva, E.; Kheirandish, F. Blastocystis hominis: A pathogenic parasite. Arch. Clin. Infect. Dis. 2020, 15, 1–6. [Google Scholar] [CrossRef]
- Alfellani, M.A.; Stensvold, C.R.; Vidal-Lapiedra, A.; Onuoha, E.S.; FagbenroBeyioku, A.F.; Clark, C.G. Variable geographic distribution of Blastocystis subtypes and its potential implications. Acta Trop. 2013, 126, 11–18. [Google Scholar] [CrossRef]
- Suresh, K.; Venilla, G.D.; Tan, T.C.; Rohela, M. In vivo encystation of Blastocystis hominis. Parasitol. Res. 2009, 104, 1373–1380. [Google Scholar] [CrossRef]
- Leelayoova, S.; Siripattanapipong, S.; Thathaisong, U.; Naaglor, T.; Taamasri, P.; Piyaraj, P.; Mungthin, M. Drinking water: A possible source of Blastocystis spp. subtype 1 infection in schoolchildren of a rural community in central Thailand. Am. J. Trop. Med. Hyg. 2008, 79, 401–406. [Google Scholar] [CrossRef]
- Mohammed, A.; Derya, T.; Alison, S.; Christine, A.; Hisao, Y.; Rune, S.; Graham, C. Genetic Diversity of Blastocystis in Livestock and Zoo Animals. Protist 2013, 164, 497–509. [Google Scholar]
- Tan, K.S. New insights on classification, identification, and clinical relevance of Blastocystis spp. Clin. Microbiol. Rev. 2008, 21, 639–665. [Google Scholar] [CrossRef]
- Stensvold, C.R.; Clark, C.G. Pre-empting Pandora’s Box: Blastocystis Subtypes Revisited. Trends Parasitol. 2020, 36, 229–232. [Google Scholar] [CrossRef]
- El Safadi, D.; Gaayeb, L.; Meloni, D.; Cian, A.; Poirier, P.; Wawrzyniak, I.; Delbac, F.; Dabboussi, F.; Delhaes, L.; Seck, M.; et al. Children of Senegal River Basin show the highest prevalence of Blastocystis sp. ever observed worldwide. BMC Infect. Dis. 2014, 14, 164. [Google Scholar] [CrossRef]
- Scanlan, P.D.; Stensvold, C.R.; Cotter, P.D. Development and application of a Blastocystis subtype-specific PCR assay reveals that mixed-subtype infections are common in a healthy human population. Appl. Environ. Microbiol. 2015, 81, 4071–4076. [Google Scholar] [CrossRef]
- Bart, A.; Wentink-Bonnema, E.; Gilis, H.; Verhaar, N.; Wassenaar, C.J.; van Vugt, M.; Goorhuis, A.; Van Gool, T. Diagnosis and subtype analysis of Blastocystis sp. in 442 patients in a hospital setting in the Netherlands. BMC Infect. Dis. 2013, 13, 389. [Google Scholar] [CrossRef]
- El Safadi, D.; Cian, A.; Nourrisson, C.; Pereira, B.; Morelle, C.; Bastien, P.; Bellanger, A.P.; Botterel, F.; Candolfi, E.; Desoubeaux, G.; et al. Prevalence, risk factors for infection and subtyspe distribution of the intestinal parasite Blastocystis sp. from a large-scale multi-center study in France. BMC Infect. Dis. 2016, 16, 451. [Google Scholar] [CrossRef]
- Tan, K.S.W.; Mirza, H.; Teo, J.D.W.; Wu, B.; MacAry, P.A. Current views on the clinical relevance of Blastocystis spp. Curr. Infect. Dis. Rep. 2010, 12, 28–35. [Google Scholar] [CrossRef]
- Ajjampur, S.S.R.; Tan, K.S.W. Pathogenic mechanisms in Blastocystis spp.– Interpreting results from in vitro and in vivo studies. Parasitol. Int. 2016, 65 Pt B, 772–779. [Google Scholar] [CrossRef]
- Andersen, L.O.; Stensvold, C.R. Blastocystis in health and disease: Are we moving from a clinical to a public health perspective? J. Clin. Microbiol. 2016, 54, 524–528. [Google Scholar] [CrossRef]
- Poirier, P.; Wawrzyniak, I.; Vivarès, C.P.; Delbac, F.; El Alaoui, H. New insights into Blastocystis spp.: A potential link with irritable bowel syndrome. PLoS Pathog. 2012, 8, e1002545. [Google Scholar] [CrossRef]
- Lepczynska, M.; Chen, W.C.; Dzika, E. Mysterious chronic urticarial caused by Blastocystis spp.? Int. J. Dermatol. 2016, 55, 259–266. [Google Scholar] [CrossRef]
- Noel, C.; Dufernez, F.; Gerbod, D.; Edgcomb, V.P.; Delgado-Viscogliosi, P.; Ho, L.C.; Singh, M.; Wintjens, R.; Sogin, M.L.; Capron, M.; et al. Molecular phylogenies of Blastocystis isolates from different hosts: Implications for genetic diversity, identification of species, and zoonosis. J. Clin. Microbiol. 2005, 43, 348–355. [Google Scholar] [CrossRef]
- Chandramathi, S.; Suresh, K.; Anita, Z.; Kuppusamy, U. Elevated levels of urinary hydrogen peroxide, advanced oxidative protein product (AOPP) and malondialdehyde in humans infected with intestinal parasites. Parasitology 2009, 136, 359–363. [Google Scholar] [CrossRef]
- Dagci, H.; Ustun, S.; Taner, M.S.; Ersoz, G.; Karacasu, F.; Budak, S. Protozoon infections and intestinal permeability. Acta Trop. 2002, 81, 1–5. [Google Scholar] [CrossRef]
- Hohlfeld, R.; Dornmair, K.; Meinl, E.; Wekerle, H. The search for the target antigens of multiple sclerosis, part 1: Autoreactive CD4+T lymphocytes as pathogenic effectors and therapeutic targets. Lancet Neurol. 2016, 15, 198–209. [Google Scholar] [CrossRef]
- Kukko, M.; Virtanen, S.M.; Toivonen, A.; Simell, S.; Korhonen, S.; Ilonen, J.; Simel, O.; Knip, M. Geographical variation in risk HLA-DQB1 genotypes for type 1 diabetes and signs of beta-cell autoimmunity in a high-incidence country. Diabetes Care 2004, 27, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Marrack, P.; Kappler, J.; Kotzin, B.L. Autoimmune disease: Why and where it occurs. Nat. Med. 2001, 7, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.S.; Stroehla, B.C. The epidemiology of autoimmune diseases. Autoimmun. Rev. 2003, 2, 119–125. [Google Scholar] [CrossRef]
- Pisetsky, D.S. Systemic lupus erythematosus. A. Epidemiology, pathology and pathogenesis. In Primer on the Rheumatic Diseases, 11th ed.; Klippel, J.H., Ed.; Arthritis Foundation: Atlanta, GA, USA, 1997; pp. 246–251. [Google Scholar]
- Keshawy, M.; Alabbassy, M. Systemic Lupus Erythematosus and Irritable Bowel Syndrome: Is Blastocystis hominis the Missing Piece of the Puzzle. Suez Canal Univ. Med. J. 2018, 21, 43541. [Google Scholar] [CrossRef]
- Ernest Choy, Understanding the dynamics: Pathways involved in the pathogenesis of rheumatoid arthritis. Rheumatology 2012, 51, v3–v11. [CrossRef] [PubMed]
- Jimenez-Balderas, F.J.; Camargo-Coronel, A.; Gargia-Jaimes, J.; Zonana-Nacach, A.; Alcantara-Anguianoi, I.; Carrillo-Becerril, L.; Tapia-Romero, R.; Gonzalez, T.S.; Villalobos-Gomez, F.; Martinez-Hernandez, S.; et al. A study on parasites in Mexican rheumatic disease patients. J. Egypt. Soc. Parasitol. 2012, 42, 271–280. [Google Scholar] [CrossRef]
- M’koma, A.E. Inflammatory bowel disease: An expanding global health problem. Clinical Medicine Insights. Gastroenterology 2013, 6, S12731. [Google Scholar]
- Ellinghaus, D.; Ellinghaus, E.; Nair, R.P.; Stuart, P.E.; Esko, T.; Metspalu, A.; Debrus, S.; Raelson, J.V.; Tejasvi, T.; Belouchi, M.; et al. Combined analysis of genome-wide association studies for crohn disease and psoriasis identifies seven shared susceptibility loci. Am. J. Hum. Genet. 2012, 90, 636–647. [Google Scholar] [CrossRef]
- Ring, J.; Ruzicka, T.; Przybilla, B. (Eds.) Handbook of Atopic Eczema, 2nd ed.; Springer: Berlin, Germany; New York, NY, USA, 2006. [Google Scholar]
- Giacometti, A.; Cirioni, O.; Fiorentini, A.; Fortuna, M.; Scalise, G. Irritable bowel syndrome in patients with Blastocystis hominis infection. Eur. J. Clin. Microbiol. Infect. Dis. 1999, 18, 436–439. [Google Scholar] [CrossRef]
- Lim, M.X.; Png, C.W.; Tay, C.Y.B.; Teo, J.D.W.; Jiao, H.; Lehming, N.; Tan, K.S.W.; Zhang, Y. Differential regulation of proinflammatory cytokine expression by mitogen-activated protein kinases in macrophages in response to intestinal parasite infection. Infect. Immun. 2014, 82, 4789–4801. [Google Scholar] [CrossRef]
- Vitetta, L.; Saltzman, E.; Nikov, T.; Ibrahim, I.; Hall, S. Modulating the gut micro-environment in the treatment of intestinal parasites. J. Clin. Med. 2016, 5, 102. [Google Scholar] [CrossRef] [PubMed]
- Vielma, J.R. Blastocystosis: Epidemiological, clinical, pathogenic, diagnostic, and therapeutic spects. Invest. Clin. 2019, 60, 53–78. [Google Scholar] [CrossRef]
- McCoy, K.D.; Stoel, M.; Stettler, R.; Merky, P.; Fink, K.; Senn, B.M.; Schaer, C.; Massacand, J.; Odermatt, B.; Oettgen, H.C.; et al. Polyclonal and specific antibodies mediate protective immunity against enteric helminth infection. Cell. Host Microbe 2008, 4, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Nieves-Ramírez, M.E.; Partida-Rodríguez, O.; Laforest-Lapointe, I.; Reynolds, L.A.; Brown, E.M.; Valdez-Salazar, A.; Morán-Silva, P.; Rojas-Velázquez, L.; Morien, E.; Parfrey, L.W.; et al. Asymptomatic intestinal colonization with protist blastocystis is strongly associated with distinct microbiome ecological patterns. mSystems 2018, 3, e00007-18. [Google Scholar] [CrossRef]
- Cheng, H.S.; Guo, Y.L.; Shin, J.W. Hematological effects of Blastocystis hominis infection in male foreign workers in Taiwan. Parasitol. Res. 2003, 90, 48–51. [Google Scholar] [CrossRef]
- Puthia, M.K.; Vaithilingam, A.; Lu, J.; Tan, K.S.W. Degradation of human secretory immunoglobulin a by blastocystis. Parasitol. Res. 2005, 97, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Hussein, E.M.; Hussein, A.M.; Eida, M.M.; Atwa, M.M. Pathophysiological variability of different genotypes of human Blastocystis hominis Egyptian isolates in experimentally infected rats. Parasitol. Res. 2008, 102, 853–860. [Google Scholar] [CrossRef]
- Kristýna, F.; Matěj, R.; Eva, N.; Hana, G.; Juraj, B.; Michaela, C.; Matej, L.; David, S.; Tomáš, F. The Impact of DNA Extraction Methods on Stool Bacterial and Fungal Microbiota Community Recovery. Front. Microbiol. 2019, 10, 821. [Google Scholar]
- Chan, K.H.; Chandramathi, S.; Suresh, K.; Chua, K.H.; Kuppusamy, U.R. Effects of symptomatic and asymptomatic isolates of Blastocystis hominis on colorectal cancer cell line, HCT116. Parasitol. Res. 2012, 110, 2475–2480. [Google Scholar] [CrossRef]
- Wallace, K.L.; Zheng, L.B.; Kanazawa, Y.; Shih, D.Q. Immunopathology of inflammatory bowel disease. World J. Gastroenterol. 2014, 20, 16–21. [Google Scholar] [CrossRef]
- Inceboz, T.; Usluca, S.; Over, L.; Yalcin, G.; Tuncay, S.; Ozkoc, S. The epidemiology research of Blastocystis hominis in the Dokuz Eylul University Medical Faculty Hospital between 2005 and 2009. Turk. Parazitolojii Derg. 2011, 35, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Stensvold, C.R.; Nielsen, H.V.; Mølbak, K.; Smith, H.V. Pursuing the Clinical Significance of Blastocystis—Diagnostic Limitations. Trends Parasitol. 2009, 25, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Nithyamathi, K.; Chandramathi, S.; Kumar, S. Predominance of Blastocystis sp. Infection among School Children in Peninsular Malaysia. PLoS ONE 2016, 11, e0136709. [Google Scholar] [CrossRef]
- Mumcuoglu, I.; Coskun, F.A.; Aksu, N.; Purnak, T.; Gungor, C. Role of Dientamoeba fragilis and Blastocystis spp. in irritable bowel syndrome. Turk. Parazitol. Derg. 2013, 37, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.L.; Chan, C.C.; Chen, H.P.; Fung, C.P.; Lin, C.P.; Chan, W.L.; Liu, C.Y. Clinical characteristics and endoscopic findings associated with Blastocystis hominis in healthy adults. Am. J. Trop. Med. Hyg. 2003, 69, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Tai, W.P.; Hu, P.J.; Wu, J.; Lin, X.C. Six ulcerative colitis patients with refractory symptoms co-infective with Blastocystis hominis in China. Parasitol. Res. 2011, 108, 1207–1210. [Google Scholar] [CrossRef] [PubMed]
- Yakoob, J.; Jafri, W.; Beg, M.A.; Abbas, Z.; Naz, S.; Islam, M.; Khan, R. Irritable bowel syndrome: Is it associated with genotypes of Blas-tocystis hominis. Parasitol. Res. 2010, 106, 1033–1038. [Google Scholar] [CrossRef]
- Nourrisson, C.; Scanzi, J.; Pereira, B.; NkoudMongo, C.; Wawrzyniak, I.; Cian, A.; Viscogliosi, E.; Livrelli, V.; Delbac, F.; Dapoigny, M.; et al. Blastocystis Is Associated with De-crease of Fecal Microbiota Protective Bacteria: Comparative Analysis be-tween Patients with Irritable Bowel Syn-drome and Control Subjects. PLoS ONE 2014, 9, e111868. [Google Scholar] [CrossRef]
- Šloufová, M.; Lhotská, Z.; Jirků, M.; Petrželková, K.J.; Stensvold, C.R.; Cinek, O.; Pomajbíková, K. Comparison of molecular diagnostic approaches for the detection and differentiation of the intestinal protist Blastocystis sp. in humans. Parasite 2022, 29, 30. [Google Scholar] [CrossRef]
- Roberts, T.; Barratt, J.; Harkness, J.; Ellis, J.; Stark, D. Comparison of microscopy, culture, and conventional polymerase chain reaction for detection of Blastocystis sp. in clinical stool samples. Am. J. Trop. Med. Hyg. 2011, 84, 308–312. [Google Scholar] [CrossRef]
- Eida, A.M.; Eida, M.M. Identification of Blastocystis hominis in patients with irritable bowel syndrome using microscopy and culture compared to PCR. Parasitol. United J. 2008, 1, 87–92. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Blastocystis sp. Infection (n, %) | OR | 95% CI for OR | p | ||
|---|---|---|---|---|---|---|
| Positive (n = 15) | Negative (n = 115) | |||||
| Age | <40 (n = 82) ≥40 (n = 48) | 11 (73.3%) 4 (26.7%) | 71 (61.7%) 44 (38.3%) | 1.70 | 0.55–5.10 | 0.38 |
| Gender | Male (n = 40) Female (n = 90) | 9 (60.0%) 6 (40.0%) | 51 (44.3%) 64 (55.7%) | 1.88 | 0.64–5.76 | 0.25 |
| Residence | Urban (n = 116) Rural (n = 14) | 9 (60.0%) 6 (40.0%) | 107 (93.0%) 8 (7.0%) | 0.11 | 0.03–0.40 | <0.01 * |
| SLE | No (n = 92) Yes (n = 38) | 10 (66.7%) 5 (33.3%) | 82 (71.3%) 33 (28.7%) | 0.80 | 0.27–2.25 | 0.71 |
| RA | No (n = 94) Yes (n = 36) | 14 (93.3%) 1 (6.7%) | 80 (69.6%) 35 (30.4%) | 6.13 | 1.07–66.72 | 0.06 |
| UC | No (n = 109) Yes (n = 21) | 10 (66.7%) 5 (33.3%) | 99 (86.1%) 16 (13.9%) | 0.32 | 0.09–0.97 | 0.06 |
| Crohn’s | No (n = 117) Yes (n = 13) | 13 (86.7%) 2 (13.3%) | 104 (90.4%) 11 (9.6%) | 0.69 | 0.15–3.39 | 0.65 |
| Psoriasis | No (n = 117) Yes (n = 13) | 14 (93.3%) 1 (6.7%) | 103 (89.6%) 12 (10.4%) | 1.63 | 0.24–18.64 | 0.65 |
| Eczema | No (n = 121) Yes (n = 9) | 14 (93.3%) 1 (6.7%) | 107 (93.0%) 8 (7.0%) | 1.05 | 0.17–12.38 | 0.97 |
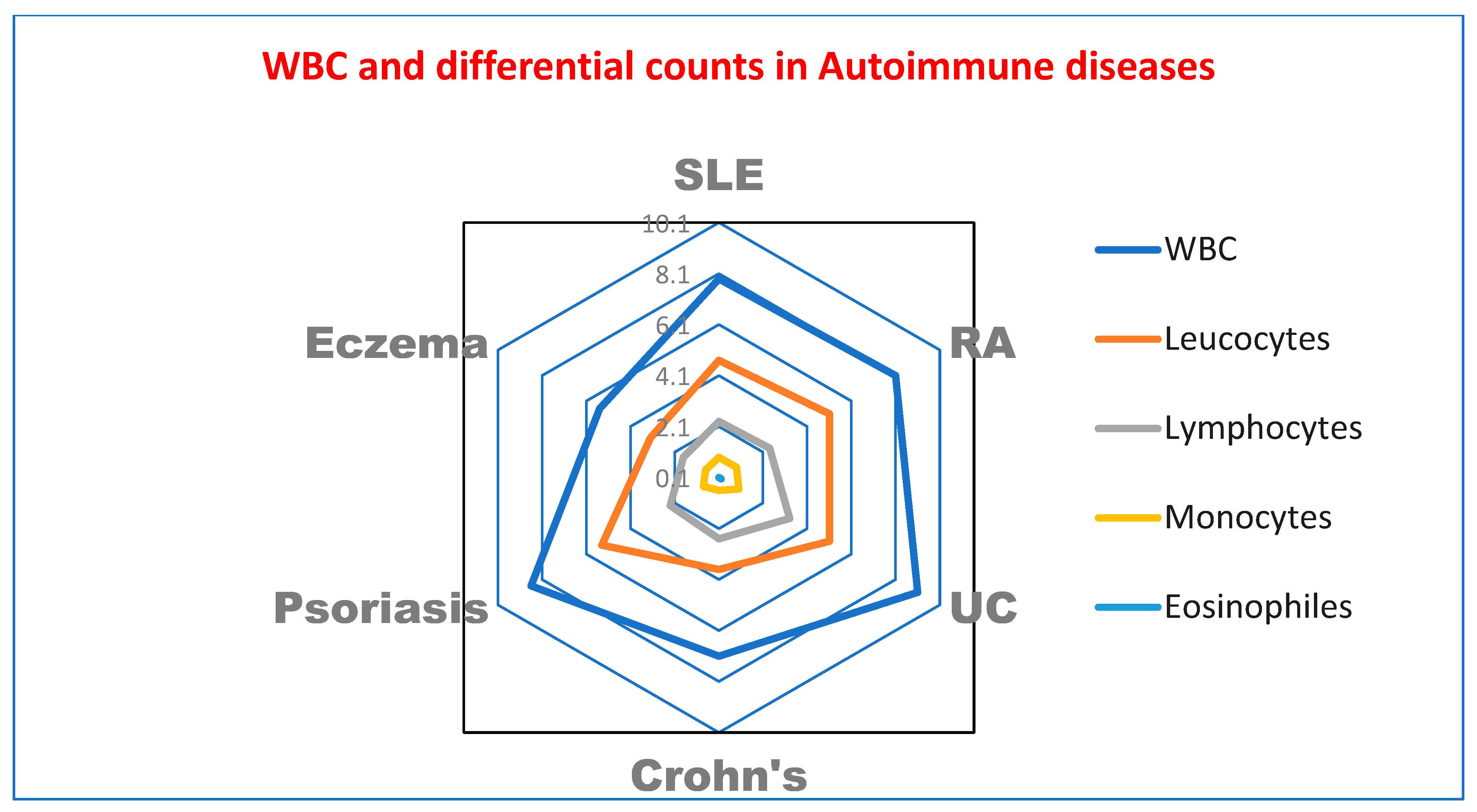
| Diseases | Case (Mean, ±SD) | Control (Mean, ±SD) | p | |
|---|---|---|---|---|
| SLE | WBCs | 7.39, (2.65) | 9.12, (2.41) | 0.04 * |
| Neutrophiles | 4.76, (2.19) | 5.79, (1.99) | 0.14 | |
| Lymphocytes | 2.35, (1.19) | 2.22, (0.97) | 0.7 | |
| Monocytes | 0.94, (0.53) | 0.99, (0.49) | 0.75 | |
| Eosinophiles | 0.13, (0.15) | 0.11, (0.14) | 0.8 | |
| RA | WBCs | 8.05, (2.51) | 7.52, (2.84) | 0.56 |
| Neutrophiles | 5.09, (1.86) | 4.49, (2.23) | 0.39 | |
| Lymphocytes | 2.46, (0.88) | 2.67, (0.95) | 0.52 | |
| Monocytes | 0.91, (0.49) | 0.78, (0.52) | 0.44 | |
| Eosinophiles | 0.10, (0.15) | 0.11, (0.11) | 0.79 | |
| UC | WBCs | 9.06, (3.58) | 9.51, (4.62) | 0.8 |
| Neutrophiles | 5.07, (2.55) | 18.85, (19.93) | 0.03 * | |
| Lymphocytes | 3.31, (1.32) | 16.59, (18.89) | 0.02 * | |
| Monocytes | 1.01, (0.54) | 4.23, (5.42) | 0.053 | |
| Eosinophiles | 0.22, (0.19) | 0.71, (0.98) | 0.11 | |
| Crohn’s | WBCs | 7.04, (2.17) | 6.83, (2.64) | 0.88 |
| Neutrophiles | 3.76, (1.47) | 10.61, (15.09) | 0.22 | |
| Lymphocytes | 2.52, (1,13) | 11.58, (21.14) | 0.24 | |
| Monocytes | 0.62, (0.16) | 2.26, (4.15) | 0.28 | |
| Eosinophiles | 0.14, (0.09) | 0.68, (1.24) | 0.23 | |
| Psoriasis | WBCs | 8.66, (1.92) | 9.39, (5.12) | 0.73 |
| Neutrophiles | 5.47, (1.59) | 5.54, (4.08) | 0.97 | |
| Lymphocytes | 2.31, (1.19) | 3.51, (1.70) | 0.16 | |
| Monocytes | 0.84, (0.48) | 0.69, (0.43) | 0.55 | |
| Eosinophiles | 0.12, (0.15) | 0.18, (0.19) | 0.54 | |
| Eczema | WBCs | 5.51, (1.31) | 8.40, (3.94) | 0.21 |
| Neutrophiles | 3.26, (1.26) | 4.06, (2.42) | 0.57 | |
| Lymphocytes | 1.79, (0.48) | 3.61, (1.75) | 0.09 | |
| Monocytes | 0.71, (0.36) | 0.69, (0.29) | 0.98 | |
| Eosinophiles | 0.07, (0.09) | 0.34, (0.22) | 0.06 |
| Diseases | Blastocyst | Case (n) | Control (n) | p |
|---|---|---|---|---|
| SLE | Positive (n = 5) Negative (n = 33) | 5 15 | 0 18 | 0.02 * |
| RA | Positive (n = 1) Negative (n = 35) | 0 21 | 1 14 | 0.43 |
| UC | Positive (n = 5) Negative (n = 16) | 5 7 | 0 9 | 0.04 * |
| Crohn’s | Positive (n = 2) Negative (n = 11) | 2 6 | 0 5 | 0.49 |
| Psoriasis | Positive (n = 1) Negative (n = 12) | 0 7 | 1 5 | 0.99 |
| Eczema | Positive (n = 1) Negative (n = 8) | 0 4 | 1 4 | 0.99 |
| Test | Total 130 | Cases | Control | Test of Sign | ||||
|---|---|---|---|---|---|---|---|---|
| Positive n | Negative n | Positive n | Negative n | Positive n | Negative n | χ2 | p Value | |
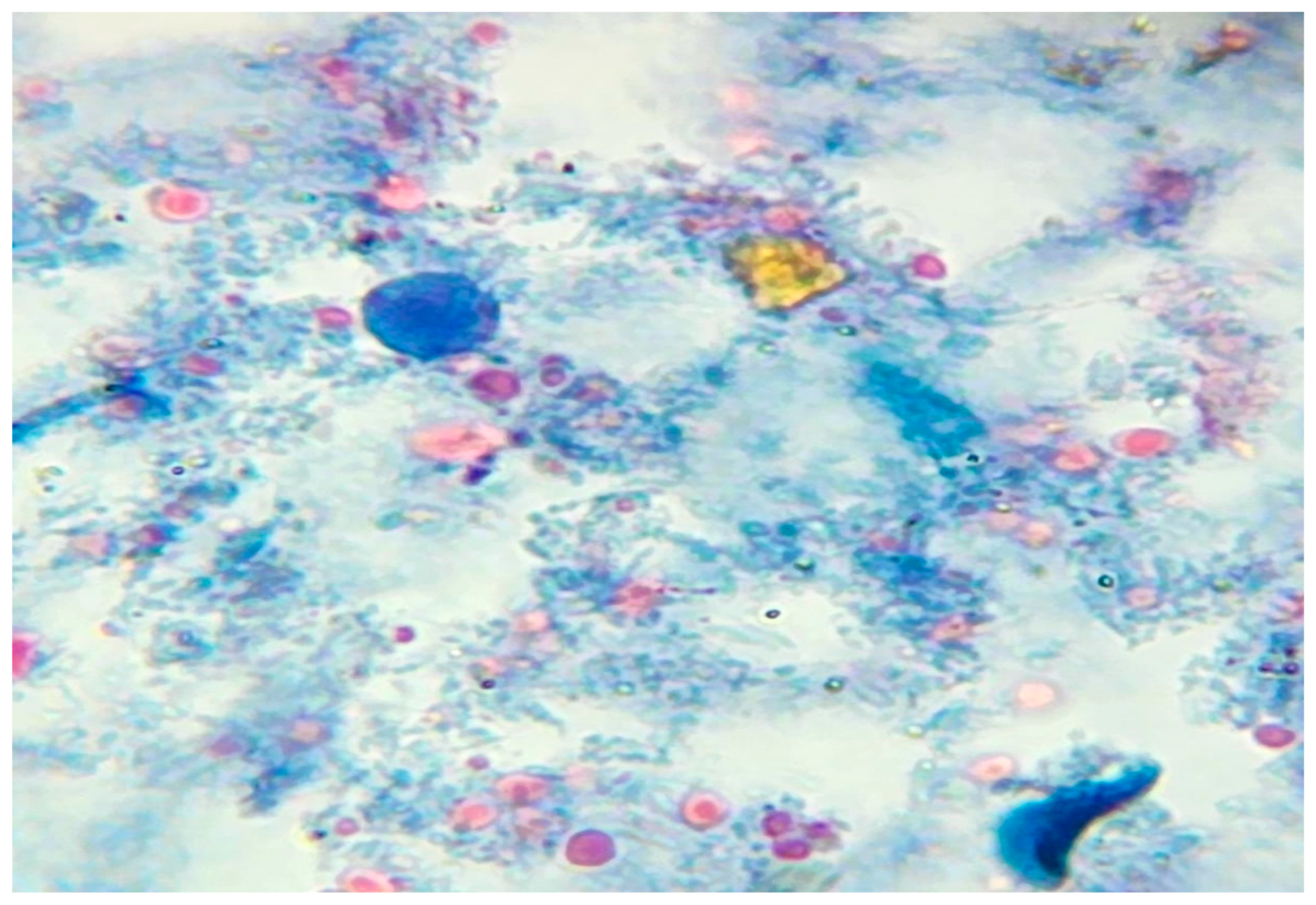
| Microscopy | 10 | 120 | 9 | 63 | 1 | 57 | 5.245 | 0.02 * |
| PCR | 15 | 115 | 12 | 60 | 3 | 54 | 4.03 | 0.04 * |
| Test | Positive | Negative | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | Agreements % (Kappa Test) | ||
|---|---|---|---|---|---|---|---|---|---|
| True | False | True | False | ||||||
| Wet mount microscopy | 10 | 0 | 120 | 5 | 66.67% (38.38–88.18) | 100 (96.97–100.0) | 100 | 96.77% (92.9–98.56) | 80.1 (0.353) |
| PCR assay | 15 | 0 | 115 | 0 | NA | NA | NA | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmoud, A.M.; Ismail, K.A.; Khalifa, O.M.; Abdel-wahab, M.M.; Hagag, H.M.; Mahmoud, M.K. Molecular Identification of Blastocystis hominis Isolates in Patients with Autoimmune Diseases. Appl. Microbiol. 2023, 3, 417-428. https://doi.org/10.3390/applmicrobiol3020029
Mahmoud AM, Ismail KA, Khalifa OM, Abdel-wahab MM, Hagag HM, Mahmoud MK. Molecular Identification of Blastocystis hominis Isolates in Patients with Autoimmune Diseases. Applied Microbiology. 2023; 3(2):417-428. https://doi.org/10.3390/applmicrobiol3020029
Chicago/Turabian StyleMahmoud, Ahmed M., Khadiga A. Ismail, Osama M. Khalifa, Maha M. Abdel-wahab, Howaida M. Hagag, and Mahmoud K. Mahmoud. 2023. "Molecular Identification of Blastocystis hominis Isolates in Patients with Autoimmune Diseases" Applied Microbiology 3, no. 2: 417-428. https://doi.org/10.3390/applmicrobiol3020029