
A Comprehensive Review on the Role of Human Epidermal Growth Factor Receptor 2 (HER2) as a Biomarker in Extra-Mammary and Extra-Gastric Cancers

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
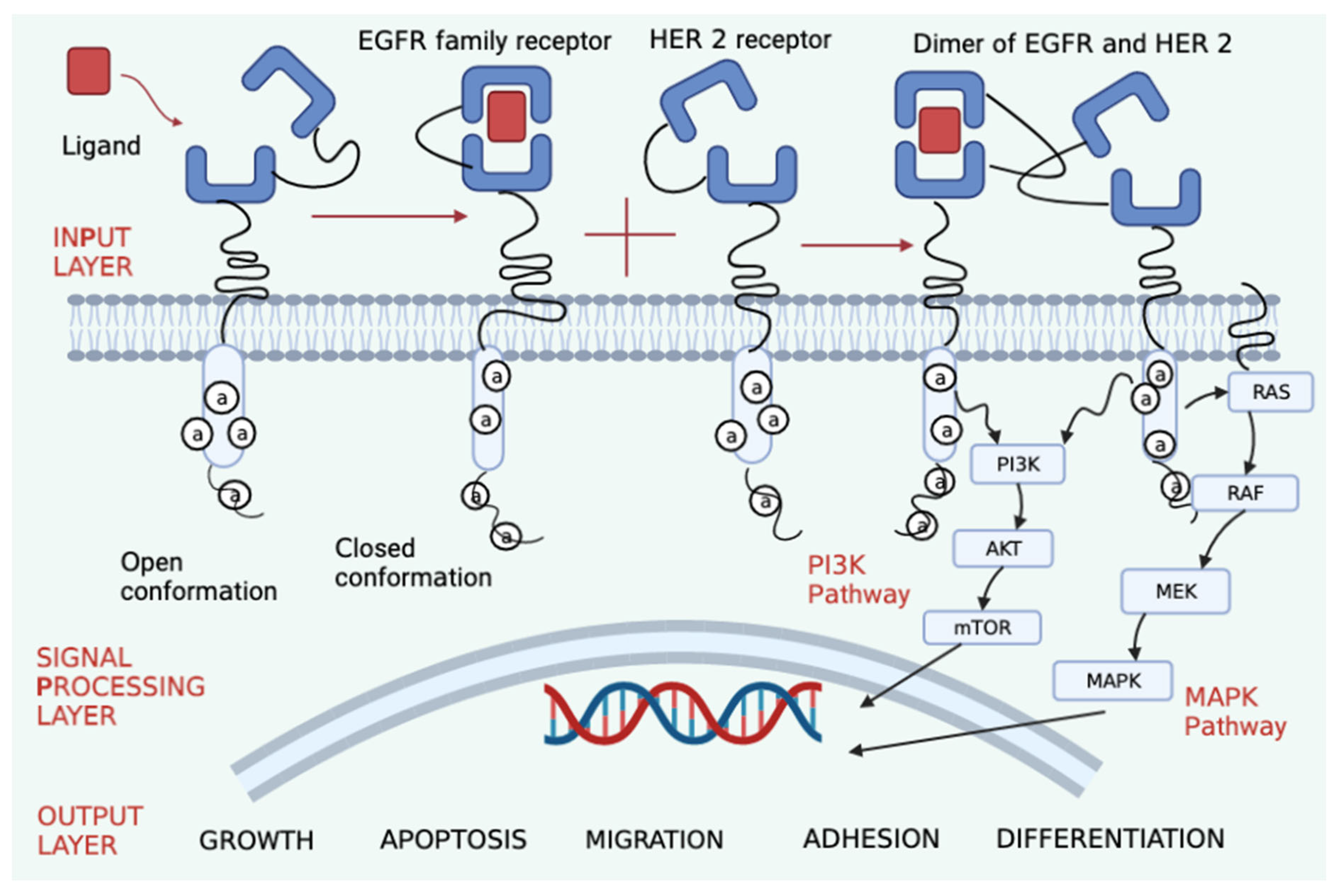
1.1. Nomenclature, Structure and Function
1.2. Testing for HER2 Neu
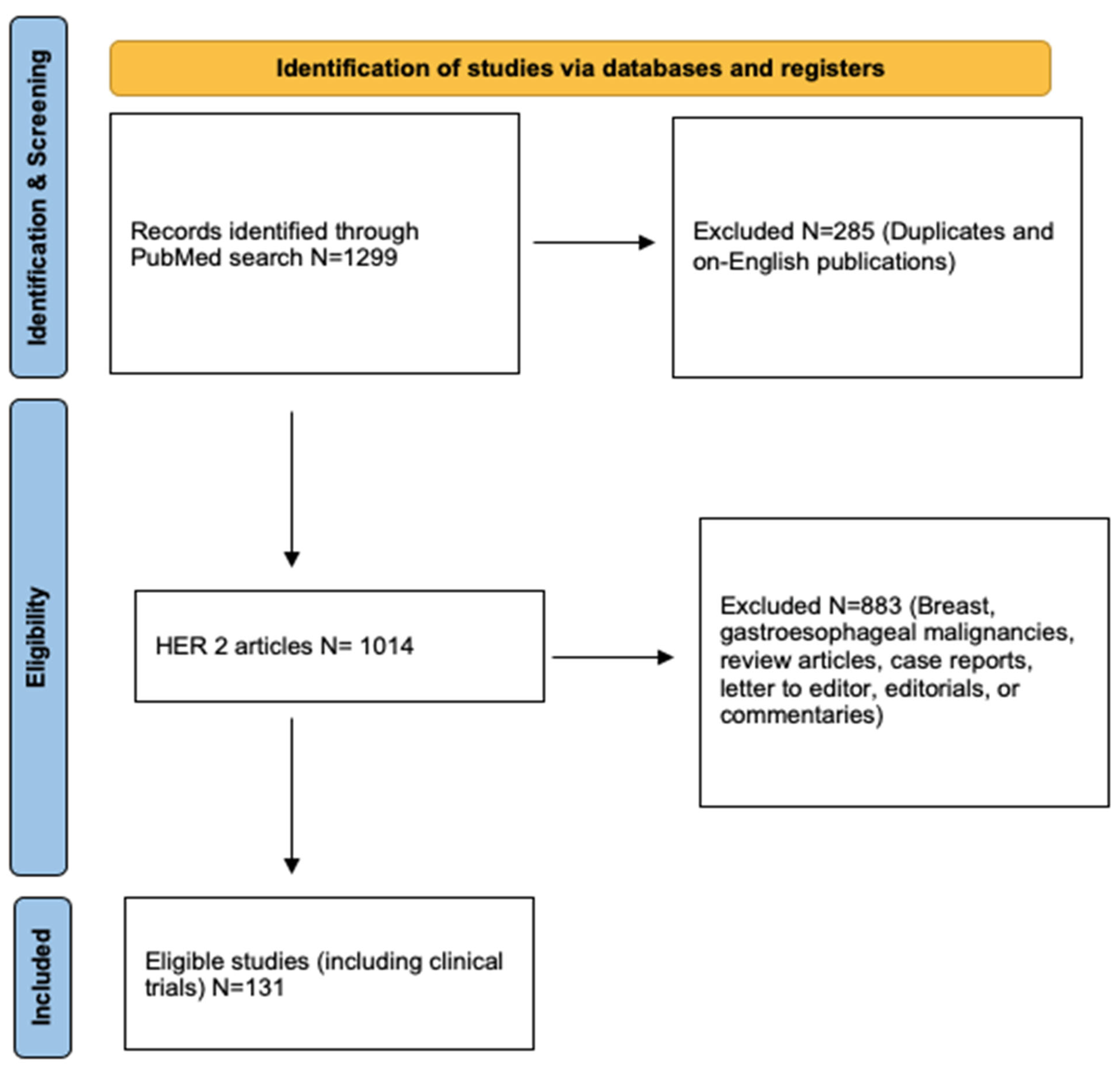
2. Strategies for Review
3. Results
3.1. Ovarian Cancer
3.2. Endometrial Cancer
3.3. Lung Cancer
3.4. Colorectal Cancer (CRC)
3.5. Salivary Gland Cancer
3.6. Pancreatic Cancer
3.7. Bladder Cancer
3.8. Prostate Cancer
3.9. Biliary Tract Cancer (BTC)
3.10. Other Malignancies
3.10.1. Osteosarcoma (OS)
3.10.2. Thyroid Cancer
3.10.3. Glioblastoma Multiforme (GBM)
3.10.4. Acute Lymphoblastic Leukemia (ALL)
3.10.5. Soft Tissue Sarcoma
3.10.6. Wilms Tumor
3.10.7. Melanoma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brandt-Rauf, P.W.; Pincus, M.R.; Carney, W.P. The c-erbB-2 protein in oncogenesis: Molecular structure to molecular epidemiology. Crit. Rev. Oncog. 1994, 5, 313–329. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.; Padhy, L.C.; Murray, M.; Weinberg, R.A. Transforming genes of carcinomas and neuroblastomas introduced into mouse fibroblasts. Nature 1981, 290, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Schechter, A.L.; Hung, M.C.; Vaidyanathan, L.; Weinberg, R.A.; Yang-Feng, T.L.; Francke, U.; Ullrich, A.; Coussens, L. The neu gene: An erbB-homologous gene distinct from and unlinked to the gene encoding the EGF receptor. Science 1985, 229, 976–978. [Google Scholar] [CrossRef] [PubMed]
- Schechter, A.L.; Stern, D.F.; Vaidyanathan, L.; Decker, S.J.; Drebin, J.A.; Greene, M.I.; Weinberg, R.A. The neu oncogene: An erb-B-related gene encoding a 185,000-Mr tumour antigen. Nature 1984, 312, 513–516. [Google Scholar] [CrossRef] [PubMed]
- King, C.R.; Kraus, M.H.; Aaronson, S.A. Amplification of a novel v-erbB-related gene in a human mammary carcinoma. Science 1985, 229, 974–976. [Google Scholar] [CrossRef]
- Cho, H.S.; Mason, K.; Ramyar, K.X.; Stanley, A.M.; Gabelli, S.B.; Denney, D.W.; Leahy, D.J. Structure of the extracellular region of HER2 alone and in complex with the Herceptin Fab. Nature 2003, 421, 756–760. [Google Scholar] [CrossRef]
- Cho, H.S.; Leahy, D.J. Structure of the extracellular region of HER3 reveals an interdomain tether. Science 2002, 297, 1330–1333. [Google Scholar] [CrossRef]
- Nahta, R.; Yuan, L.X.H.; Zhang, B.; Kobayashi, R.; Esteva, F.J. Insulin-like growth factor-I receptor/human epidermal growth factor receptor 2 heterodimerization contributes to trastuzumab resistance of breast cancer cells. Cancer Res. 2005, 65, 11118–11128. [Google Scholar] [CrossRef]
- Sierke, S.L.; Cheng, K.; Kim, H.H.; Koland, J.G. Biochemical characterization of the protein tyrosine kinase homology domain of the ErbB3 (HER3) receptor protein. Biochem. J. 1997, 322, 757–763. [Google Scholar] [CrossRef]
- Sliwkowski, M.X.; Schaefer, G.; Akita, R.W.; Lofgren, J.A.; Fitzpatrick, V.D.; Nuijens, A.; Fendly, B.M.; Cerione, R.A.; Vandlen, R.L.; Carraway, K.L., 3rd. Coexpression of erbB2 and erbB3 proteins reconstitutes a high affinity receptor for heregulin. J. Biol. Chem. 1994, 269, 14661–14665. [Google Scholar] [CrossRef]
- Wilson, G.R.; Cramer, A.; Welman, A.; Knox, F.; Swindell, R.; Kawakatsu, H.; Clarke, R.B.; Dive, C.; Bundred, N.J. Activated c-SRC in ductal carcinoma in situ correlates with high tumour grade, high proliferation and HER2 positivity. Br. J. Cancer 2006, 95, 1410–1414. [Google Scholar] [CrossRef]
- Timms, J.F.; White, S.L.; O’Hare, M.J.; Waterfield, M.D. Effects of ErbB-2 overexpression on mitogenic signalling and cell cycle progression in human breast luminal epithelial cells. Oncogene 2002, 21, 6573–6586. [Google Scholar] [CrossRef]
- Penault-Llorca, F.; Bilous, M.; Dowsett, M.; Hanna, W.; Osamura, R.Y.; Rüschoff, J.; van de Vijver, M. Emerging technologies for assessing HER2 amplification. Am. J. Clin. Pathol. 2009, 132, 539–548. [Google Scholar] [CrossRef]
- Press, M.F.; Slamon, D.J.; Flom, K.J.; Park, J.; Zhou, J.Y.; Bernstein, L. Evaluation of HER-2/neu gene amplification and overexpression: Comparison of frequently used assay methods in a molecularly characterized cohort of breast cancer specimens. J. Clin. Oncol. 2002, 20, 3095–3105. [Google Scholar] [CrossRef]
- Graves, H.; Czerniecki, B.J. Circulating tumor cells in breast cancer patients: An evolving role in patient prognosis and disease progression. Pathol. Res. Int. 2011, 2011, 621090. [Google Scholar] [CrossRef]
- Cao, S.; Li, Y.; Li, J.; Li, C.F.; Zhang, W.; Yang, Z.Q.; Meng, S.D. Quantitative determination of HER2 expression by confocal microscopy assay in CTCs of breast cancer. Oncol. Rep. 2010, 23, 423–428. [Google Scholar]
- De, P.; Smith, B.R.; Leyland-Jones, B. Human epidermal growth factor receptor 2 testing: Where are we? J. Clin. Oncol. 2010, 28, 4289–4292. [Google Scholar] [CrossRef]
- Lehmann-Che, J.; Amira-Bouhidel, F.; Turpin, E.; Antoine, M.; Soliman, H.; Legres, L.; Bocquet, C.; Bernoud, R.; Flandre, E.; Varna, M.; et al. Immunohistochemical anmolecular analyses of HER2 status in breast cancers are highly concordant and complementary approaches. Br. J. Cancer 2011, 104, 1739–1746. [Google Scholar] [CrossRef]
- Rubin, S.C.; Finstad, C.L.; Federici, M.G.; Scheiner, L.; Lloyd, K.O.; Hoskins, W.J. Prevalence and significance of HER-2/neu expression in early epithelial ovarian cancer. Cancer 1994, 73, 1456–1459. [Google Scholar] [CrossRef]
- Seki, A.; Yoshinouchi, M.; Seki, N.; Kodama, J.; Miyagi, Y.; Kudo, T. Detection of c-erbB-2 and FGF-3 (INT-2) gene amplification in epithelial ovarian cancer. Int. J. Oncol. 2000, 17, 103–106. [Google Scholar] [CrossRef]
- Gao, D.; Lu, Y.; Lu, Y.; Wang, Y.; Zhang, B.; Wu, B. Significance of HER-2/neu expression in ovarian epithelial tumours. Zhonghua Bing Li Xue Za Zhi 2002, 31, 268–270. [Google Scholar] [PubMed]
- Hogdall, E.V.; Christensen, L.; Kjaer, S.K.; Blaakaer, J.; Bock, J.E.; Glud, E.; Nørgaard-Pedersen, B.; Høgdall, C.K. Distribution of HER-2 overexpression in ovarian carcinoma tissue and its prognostic value in patients with ovarian carcinoma: From the Danish MALOVA Ovarian Cancer Study. Cancer 2003, 98, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Bookman, M.A.; Darcy, K.M.; Clarke-Pearson, D.; Boothby, R.A.; Horowitz, I.R. Evaluation of monoclonal humanized anti-HER2 antibody, trastuzumab in patients with recurrent or refractory ovarian or primary peritoneal carcinoma with overexpression of HER2: A phase II trial of the Gynaecologic Oncology Group. J. Clin. Oncol. 2003, 21, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Camilleri-Broet, S.; Hardy-Bessard, A.C.; Le Tourneau, A.; Paraiso, D.; Levrel, O.; Leduc, B.; Bain, S.; Orfeuvre, H.; Audouin, J.; Pujade-Lauraine, E. HER-2 overexpression is an independent marker of poor prognosis of advanced primary ovarian carcinoma: A multicentre study of the GINECO group. Ann. Oncol. 2004, 15, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Mano, M.; Awada, A.; Di Leo, A.; Durbecq, V.; Paesmans, M.; Cardoso, F.; Larsimont, D.; Piccart, M. Rates of topoisomerase II-alpha and HER-2 gene amplification and expression in epithelial ovarian carcinoma. Gynecol. Oncol. 2004, 92, 887–889. [Google Scholar] [CrossRef]
- Lee, C.H.; Huntsman, D.G.; Cheang, M.C.; Parker, R.L.; Brown, L.; Hoskins, P.; Miller, D.; Gilks, C.B. Assessment of Her-1, Her-2 and Her-3 expression and Her-2 amplification in advanced stage ovarian carcinoma. Int. J. Gynecol. Pathol. 2005, 24, 147–152. [Google Scholar] [CrossRef]
- Tuefferd, M.; Coutier, J.; Penault-Llorca, F.; Vincent-Salomon, A.; Broet, P.; Guastalla, J.P.; Allouache, D.; Combe, M.; Weber, B.; Pujade-Lauraine, E.; et al. HER2 status in ovarian carcinomas: A multicentre GINECO study of 320 patients. PLoS ONE 2007, 2, e1138. [Google Scholar] [CrossRef]
- Sasaki, N.; Kudoh, K.; Kita, T.; Tsuda, H.; Furuya, K.; Kikuchi, Y. Effect of HER-2/neu overexpression on chemoresistance and prognosis in ovarian carcinoma. J. Obstet. Gynaecol. Res. 2007, 33, 17–23. [Google Scholar] [CrossRef]
- Sueblinvong, T.; Manchana, T.; Khemapech, N.; Triratanachat, S.; Termrungruanglert, W.; Tresukosol, D. Lack of prognostic significance of HER-2/neu in early epithelial ovarian cancer. Asian Pac. J. Cancer Prev. 2007, 8, 502–506. [Google Scholar]
- Steffensen, K.D.; Waldstrom, M.; Jeppesen, U.; Jakobsen, E.; Brandslund, I.; Jakobsen, A. The prognostic importance of cyclooxygenase 2 and HER2 expression in epithelial ovarian cancer. Int. J. Gynecol. Cancer 2007, 17, 798–807. [Google Scholar] [CrossRef]
- Steffensen, K.D.; Waldstrom, M.; Andersen, R.F.; Olsen, D.A.; Jeppesen, U.; Knudsen, H.J.; Brandslund, I.; Jakobsen, A. Protein levels and gene expressions of the epidermal growth factor receptors, HER1, HER2, HER3 and HER4 in benign and malignant ovarian tumors. Int. J. Oncol. 2008, 33, 195–204. [Google Scholar] [CrossRef]
- Vermeij, J.; Teugels, E.; Bourgain, C.; Xiangming, J.; Ghislain, V.; Neyns, B.; De Greve, J. Genomic activation of the EGFR and HER2-neu genes in a significant proportion of invasive epithelial ovarian cancers. BMC 2008, 8, 3. [Google Scholar] [CrossRef]
- Chekerov, R.; Koensgen, D.; Klaman, I.; Rosenthal, A.; Oskay-Oezcelik, G.; Mustea, A.; Lightenegger, W.; Dahl, E.; Sehouli, J. Tumor- and stromal cell-specific expression of topoisomerase IIα and HER-2/neu in primary and recurrent ovarian cancer: Results of a prospective study. Mol. Med. Rep. 2009, 2, 1011–1016. [Google Scholar] [CrossRef]
- Sylvia, M.T.; Kumar, S.; Dasari, P. The expression of immunohistochemical markers estrogen receptor, progesterone receptor, Her-2-neu, p53 and Ki-67 in epithelial ovarian tumors and its correlation with clinicopathologic variables. Indian J. Pathol. Microbiol. 2012, 55, 33–37. [Google Scholar] [CrossRef]
- Jafri, A.; Rizvi, S. Frequency of Her2/Neu Protein Expression in Ovarian Epithelial Cancers. J. Coll. Physic. Surg. Pak. 2017, 27, 544–546. [Google Scholar]
- Pankaj, S.; Kumari, J.; Choudhary, V.; Kumari, A.; Kumari, S.; Kumari, A.; Nazneen, S.; Madhawi, R.; Kumar, S. Prognostic Value of HER-2/neu Gene Amplification in Epithelial Ovarian Carcinoma. J. Obstet. Gynaecol. India. 2019, 69 (Suppl. S2), 177–181. [Google Scholar] [CrossRef]
- Makhija, S.; Amler, L.C.; Glenn, D.; Ueland, F.R.; Gold, M.A.; Dizon, D.S.; Paton, V.; Lin, C.Y.; Januario, T.; Ng, K.; et al. Clinical activity of gemcitabine plus pertuzumab in platinum-resistant ovarian cancer, fallopian tube cancer, or primary peritoneal cancer. J. Clin. Oncol. 2010, 28, 1215–1223. [Google Scholar] [CrossRef]
- Lin, W.-L.; Kuo, W.-H.; Chen, F.-L.; Lee, M.-Y.; Ruan, A.; Tyan, Y.-S.; Hsu, J.-D.; Chiang, H.; Han, C.-P. Identification of the coexisting HER2 gene amplification and novel mutations in the HER2 protein-overexpressed mucinous epithelial ovarian cancer. Ann. Surg. Oncol. 2011, 18, 2388–2394. [Google Scholar] [CrossRef]
- Lassus, H.; Sihto, H.; Leminen, A.; Joensuu, H.; Isola, J.; Nupponen, N.N.; Butzow, R. Gene amplification, mutation and protein expression of EGFR and mutations of ERBB2 in serousovarian carcinoma. J. Mol. Med. 2006, 84, 671–681. [Google Scholar] [CrossRef]
- Berchuck, A.; Kamel, A.; Whitaker, R.; Kerns, B.; Olt, G.; Kinney, R.; Soper, J.T.; Dodge, R.; Clarke-Pearson, D.L.; Marks, P.; et al. Overexpression of HER-2/neu is associated with poor survival in advanced epithelial ovarian cancer. Cancer Res. 1990, 50, 4087–4091. [Google Scholar]
- Rolitsky, C.D.; Theil, K.S.; McGaughy, V.R.; Copeland, L.J.; Niemann, T.H. HER-2/neu amplification and overexpression in endometrial carcinoma. Int. J. Gynecol. Pathol. 1999, 18, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Grushko, T.A.; Filiaci, V.L.; Mundt, A.J.; Ridderstråle, K.; Olopade, O.I.; Fleming, G.F.; Gynecologic Oncology Group. An exploratory analysis of HER-2 amplification and overexpression in advanced endometrial carcinoma: A Gynecologic Oncology Group study. Gynecol. Oncol. 2008, 108, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Bellone, S.; Van Stedum, S.; Bushen, W.; Palmieri, M.; Siegel, E.R.; De Las Casas, L.E.; Roman, J.J.; Burnett, A.; Pecorelli, S. Amplification of c-erbB2 oncogene: A major prognostic indicator in uterine serous papillary carcinoma. Cancer 2005, 104, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Bellone, S.; Gokden, M.; Palmieri, M.; Dunn, D.; Agha, J.; Roman, J.J.; Hutchins, L.; Pecorelli, S.; O’Brien, T.; et al. Overexpression of HER-2/neu in uterine serous papillary cancer. Clin. Cancer Res. 2002, 8, 1271–1279. [Google Scholar] [PubMed]
- Slomovitz, B.M.; Broaddus, R.R.; Burke, T.W.; Sneige, N.; Soliman, P.T.; Wu, W.; Sun, C.C.; Munsell, M.F.; Gershenson, D.M.; Lu, K.H. Her-2/neu overexpression and amplification in uterine papillary carcinoma. J. Clin. Oncol. 2004, 22, 3126–3132. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Bellone, S.; Siegel, E.R.; Palmieri, M.; Thomas, M.; Cannon, M.J.; Kay, H.H.; Roman, J.J.; Burnett, A.; Pecorelli, S. Racial differences in the overexpression of epidermal growth factor type II receptor (HER2/neu): A major prognostic indicator in uterine serous papillary cancer. Am. J. Obstet. Gynecol. 2005, 192, 813–818. [Google Scholar] [CrossRef]
- Diaz-Montes, T.P.; Ji, H.; Smith Sehdev, A.E.; Zahurak, M.L.; Kurman, J.; Armstrong, D.K.; Bristow, R.E. Clinical significance of Her-2/neu overexpression in uterine serous carcinoma. Gynecol. Oncol. 2006, 100, 139–144. [Google Scholar] [CrossRef]
- Villella, J.A.; Cohen, S.; Smith, D.H.; Hibshoosh, H.; Hershman, D. HER-2/neu overexpression in uterine papillary serous cancers and its possible therapeutic implications. Int. J. Gynecol. Cancer 2006, 16, 1897–1902. [Google Scholar] [CrossRef]
- Odicino, F.E.; Bignotti, E.; Rossi, E.; Pasinneti, E.; Tassi, R.A.; Donzelli, C.; Falchetti, M.; Fontana, P.; Grigolato, P.G.; Pecorelli, S. HER-2/neu overexpression and amplification in uterine serous papillary carcinoma: Comparative analysis of immunohistochemistry, real-time reverse transcription-polymerase chain reaction, and fluorescence in situ hybridization. Int. J. Gynecol. Cancer 2008, 18, 14–21. [Google Scholar] [CrossRef]
- Ren, Y.; Wang, H.; Zhou, X.; Yang, W.; Huang, X.; Lu, Y.; Shi, D. Clinicopathological characteristics and her-2/neu status in chinese patients with uterine papillary serous carcinoma. ISRN Obstet. Gynecol. 2011, 2011, 575327. [Google Scholar] [CrossRef]
- Togami, S.; Sasajima, Y.; Oi, T.; Ishikawa, M.; Onda, T.; Ikeda, S.-I.; Kato, T.; Tsuda, H.; Kasamatsu, T. Clinicopathological and prognostic impact of human epidermal growth factor receptor type 2 (HER2) and hormone receptor expression in uterine papillary serous carcinoma. Cancer Sci. 2012, 103, 926–932. [Google Scholar] [CrossRef]
- Banet, N.; Shahi, M.; Batista, D.; Yonescu, R.; Tanner, E.J.; Fader, A.N.; Cimino-Mathews, A. HER-2 Amplification in Uterine Serous Carcinoma and Serous Endometrial Intraepithelial Carcinoma. Am. J. Surg. Pathol. 2021, 45, 708–715. [Google Scholar] [CrossRef]
- Fleming, G.F.; Sill, M.W.; Darcy, K.M.; McMeekin, D.S.; Thigpen, J.T.; Adler, L.M.; Berek, J.S.; Chapman, J.A.; DiSilvestro, P.A.; Horowitz, I.R.; et al. Phase II trial of trastuzumab in women with advanced or recurrent, HER2-positive endometrial carcinoma: A Gynecologic Oncology Group study. Gynecol Oncol. 2010, 116, 15–20. [Google Scholar] [CrossRef]
- Tymon-Rosario, J.; Siegel, E.R.; Bellone, S.; Harold, J.; Adjei, N.; Zeybek, B.; Mauricio, D.; Altwerger, G.; Menderes, G.; Ratner, E.; et al. Trastuzumab tolerability in the treatment of advanced (stage III-IV) or recurrent uterine serous carcinomas that overexpress HER2/neu. Gynecol. Oncol. 2021, 163, 93–99. [Google Scholar] [CrossRef]
- Ai, X.; Song, Z.; Jian, H.; Zhou, Z.; Chen, Z.; Yu, Y.; Li, Z.; Lu, S. Pyrotinib combined with thalidomide in advanced non-small-cell lung cancer patients harboring HER2 exon 20 insertions (PRIDE): Protocol of an open-label, single-arm phase II trial. BMC Cancer 2021, 21, 1033. [Google Scholar] [CrossRef]
- Park, D.I.; Oh, S.J.; Park, S.H.; Yun, J.W.; Kim, H.J.; Cho, Y.K.; Sung, I.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; et al. Clinical significance of HER-2/neu expression in colon cancer. Korean J. Gastroenterol. 2004, 44, 147–152. [Google Scholar]
- Nakamura, H.; Kawasaki, N.; Taguchi, M.; Kabasawa, K. Association of HER2 overexpression with prognosis in non-small cell lung carcinoma: A metaanalysis. Cancer 2005, 103, 1865–1873. [Google Scholar] [CrossRef]
- Liu, L.; Shao, X.; Gao, W.; Bai, J.; Wang, R.; Huang, P.; Yin, Y.; Liu, P.; Shu, Y. The role of human epidermal growth factor receptor 2 as a prognostic factor in lung cancer: A meta-analysis of published data. J. Thorac. Oncol. 2010, 5, 1922–1932. [Google Scholar] [CrossRef]
- Shigematsu, H.; Takahashi, T.; Nomura, M.; Majmudar, K.; Suzuki, M.; Lee, H.; Wistuba, I.I.; Fong, K.M.; Toyooka, S.; Shimizu, N.; et al. Somatic mutations of the HER2 kinase domain in lung adenocarcinomas. Cancer Res. 2005, 65, 1642–1646. [Google Scholar] [CrossRef]
- Stephens, P.; Hunter, C.; Bignell, G.; Edkins, S.; Davies, H.; Teague, J.; Stevens, C.; O’Meara, S.; Smith, R.; Parker, A.; et al. Lung cancer: Intragenic ERBB2 kinase mutations in tumours. Nature 2004, 431, 525–526. [Google Scholar] [CrossRef]
- Langer, C.J.; Stephenson, P.; Thor, A.; Vangel, M.; Johnson, D.H.; Eastern Cooperative Oncology Group Study 2598. Trastuzumab in the treatment of advanced non-small-cell lung cancer: Is there a role? Focus on Eastern Cooperative Oncology Group study 2598. J. Clin. Oncol. 2004, 22, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Zinner, R.G.; Glisson, B.S.; Fossella, F.V.; Pisters, K.M.; Kies, M.S.; Lee, P.M.; Massarelli, E.; Sabloff, B.; Fritsche, H.A., Jr.; Ro, J.Y.; et al. Trastuzumab in combination with cisplatin and gemcitabine in patients with Her2-overexpressing, untreated, advanced non-small cell lung cancer: Report of a phase II trial and findings regarding optimal identification of patients with Her2-overexpressing disease. Lung Cancer 2004, 44, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Lara, P.N., Jr.; Laptalo, L.; Longmate, J.; Lau, D.H.; Gandour-Edwards, R.; Gumerlock, P.H.; Doroshow, J.H.; Gandara, D.R.; California Cancer Consortium. Trastuzumab plus docetaxel in HER2/neu-positive non-small-cell lung cancer: A California Cancer Consortium screening and phase II trial. Clin. Lung Cancer 2004, 5, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T.; et al. Ado-Trastuzumab Emtansine for Patients with HER2-Mutant Lung Cancers: Results from a Phase II Basket Trial. J. Clin. Oncol. 2018, 36, 2532–2537. [Google Scholar] [CrossRef]
- Peters, S.; Stahel, R.; Bubendorf, L.; Bonomi, P.; Villegas, A.; Kowalski, D.M.; Baik, C.S.; Isla, D.; Carpeno, J.C.; Garrido, P.; et al. Trastuzumab Emtansine (T-DM1) in Patients with Previously Treated HER2-Overexpressing Metastatic Non-Small Cell Lung Cancer: Efficacy, Safety, and Biomarkers. Clin. Cancer Res. 2019, 25, 64–72. [Google Scholar] [CrossRef]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H.; Mazières, J.; Nagasaka, M.; Bazhenova, L.; Saltos, A.N.; Felip, E.; et al. Trastuzumab Deruxtecan in HER2-Mutant Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2022, 386, 241–251. [Google Scholar] [CrossRef]
- Kris, M.G.; Camidge, D.R.; Giaccone, G.; Hida, T.; Li, B.T.; O’Connell, J.; Taylor, I.; Zhang, H.; Arcila, M.E.; Goldberg, Z.; et al. Targeting HER2 aberrations as actionable drivers in lung cancers: Phase II trial of the pan-HER tyrosine kinase inhibitor dacomitinib in patients with HER2-mutant or amplified tumors. Ann. Oncol. 2015, 26, 1421–1427. [Google Scholar] [CrossRef]
- Dziadziuszko, R.; Smit, E.F.; Dafni, U.; Wolf, J.; Wasąg, B.; Biernat, W.; Finn, S.P.; Kammler, R.; Tsourti, Z.; Rabaglio, M.; et al. Afatinib in NSCLC with HER2 Mutations: Results of the Prospective, Open-Label Phase II NICHE Trial of European Thoracic Oncology Platform (ETOP). J. Thorac Oncol. 2019, 14, 1086–1094. [Google Scholar] [CrossRef]
- Fan, Y.; Chen, J.; Zhou, C.; Wang, H.; Shu, Y.; Zhang, J.; Hua, H.; Huang, D.C.-L.; Zhou, C. Afatinib in patients with advanced non-small cell lung cancer harboring HER2 mutations, previously treated with chemotherapy: A phase II trial. Lung Cancer 2020, 147, 209–213. [Google Scholar] [CrossRef]
- Buttitta, F.; Barassi, F.; Fresu, G.; Felicioni, L.; Chella, A.; Paolizzi, D.; Lattanzio, G.; Salvatore, S.; Camplese, P.P.; Rosini, S.; et al. Mutational analysis of the HER2 gene in lung tumors from Caucasian patients: Mutations are mainly present in adenocarcinomas with bronchoalveolar features. Int. J. Cancer 2006, 119, 2586–2591. [Google Scholar] [CrossRef]
- Sasaki, H.; Shimizu, S.; Endo, K.; Takada, M.; Kawahara, M.; Tanaka, H.; Matsumura, A.; Iuchi, K.; Haneda, H.; Suzuki, E.; et al. EGFR and erbB2 mutation status in Japanese lung cancer patients. Int. J. Cancer 2006, 118, 180–184. [Google Scholar] [CrossRef]
- Sun, Y.; Ren, Y.; Fang, Z.; Li, C.; Fang, R.; Gao, B.; Han, X.; Tian, W.; Pao, W.; Bin Chen, G.; et al. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J. Clin. Oncol. 2010, 28, 4616–4620. [Google Scholar] [CrossRef]
- Tomizawa, K.; Suda, K.; Onozato, R.; Kosaka, T.; Endoh, H.; Sekido, Y.; Shigematsu, H.; Kuwano, H.; Yatabe, Y.; Mitsudomi, T. Prognostic and predictive implications of HER2/ERBB2/neu gene mutations in lung cancers. Lung Cancer 2011, 74, 139–144. [Google Scholar] [CrossRef]
- Li, C.; Sun, Y.; Fang, R.; Han, X.; Luo, X.; Wang, R.; Pan, Y.; Hu, H.; Zhang, Y.; Pao, W.; et al. Lung adenocarcinomas with HER2-activating mutations are associated with distinct clinical features and EGFR/HER2 copy number gains. J. Thorac. Oncol. 2012, 7, 85–89. [Google Scholar] [CrossRef]
- Arcila, M.E.; Chaft, J.E.; Nafa, K.; Roy-Chowduri, S.; Lau, C.; Zaidinski, M.; Paik, P.K.; Zakowski, M.F.; Kris, M.G.; Ladanyi, M. Prevalence, clinicopathologic associations and molecular spectrum of ERBB2 (HER2) tyrosine kinase mutations in lung adenocarcinomas. Clin. Cancer Res. 2012, 18, 4910–4918. [Google Scholar] [CrossRef]
- Mazieres, J.; Peters, S.; Lepage, B.; Cortot, A.B.; Barlesi, F.; Beau-Faller, M.; Besse, B.; Blons, H.; Mansuet-Lupo, A.; Urban, T.; et al. Lung cancer that harbors an HER2 mutation: Epidemiologic characteristics and therapeutic perspectives. J. Clin. Oncol. 2013, 31, 1997–2003. [Google Scholar] [CrossRef]
- Cappuzzo, F.; Gregorc, V.; Rossi, E.; Cancellieri, A.; Magrini, E.; Paties, C.T.; Ceresoli, G.; Lombardo, L.; Bartolini, S.; Calandri, C.; et al. Gefitinib in pretreated non-small-cell lung cancer (NSCLC): Analysis of efficacy and correlation with HER2 and epidermal growth factor receptor expression in locally advanced or metastatic NSCLC. J. Clin. Oncol. 2003, 21, 2658–2663. [Google Scholar] [CrossRef]
- Gatzemeier, U.; Growth, G.; Hirsh, V.; Butts, C.; Van Zandwijk, N.; Shepherd, F.; Rosso, R.; Howell, J. A randomized phase II study of gemcitabine/cisplatin alone and with herceptin in patients with HER-2-positive non-small cell lung cancer. Proc. ECCO 2001, 37 (Suppl. S6), S50. [Google Scholar]
- Clamon, G.; Herndon, J.; Kern, J.; Govindan, R.; Garst, J.; Watson, D.; Green, M.; Cancer and Leukemia Group, B. Lack of trastuzumab activity in nonsmall cell lung carcinoma with overexpression of erb-B2: 39810: A phase II trial of Cancer and Leukemia Group B. Cancer 2005, 104, 1670–1675. [Google Scholar] [CrossRef]
- Krug, L.M.; Miller, V.A.; Patel, J.; Crapanzano, J.; Azzoli, C.G.; Gomez, J.; Kris, M.G.; Heelan, R.T.; Pizzo, B.; Tyson, L.; et al. Randomized phase II study of weekly docetaxel plus trastuzumab versus weekly paclitaxel plus trastuzumab in patients with previously untreated advanced nonsmall cell lung carcinoma. Cancer. 2005, 10, 2149–2155. [Google Scholar] [CrossRef]
- De Langen, A.J.; Jebbink, M.; Hashemi, S.M.S.; Kuiper, J.L.; de Bruin-Visser, J.; Monkhorst, K.; Thunnissen, E.; Smit, E.F. Trastuzumab and paclitaxel in patients with EGFR mutated NSCLC that express HER2 after progression on EGFR TKI treatment. Br. J. Cancer 2018, 119, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Soung, Y.H.; Seo, S.H.; Kim, S.Y.; Park, C.H.; Wang, Y.P.; Park, K.; Nam, S.W.; Park, W.S.; Kim, S.H.; et al. Somatic mutations of ERBB2 kinase domain in gastric, colorectal and breast carcinomas. Clin. Cancer Res. 2006, 12, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Shabbir, A.; Mirza, T.; Khalid, A.B.; Qureshi, M.A.; Asim, S.A. Frequency of Her2/neu expression in colorectal adenocarcinoma: A study from developing South Asian Country. BMC Cancer 2016, 16, 855. [Google Scholar] [CrossRef] [PubMed]
- Ingold Heppner, B.; Behrens, H.M.; Balschun, K.; Haag, J.; Krüger, S.; Becker, T.; Röcken, C. HER2/neu testing in primary colorectal carcinoma. Br. J. Cancer 2014, 111, 1977–1984. [Google Scholar] [CrossRef] [PubMed]
- Conradi, L.C.; Styczen, H.; Sprenger, T.; Wolff, H.A.; Rödel, C.; Nietert, M.; Homayounfar, K.; Gaedcke, J.; Kitz, J.; Talaulicar, R.; et al. Frequency of HER-2 positivity in rectal cancer and prognosis. Am. J. Surg. Pathol. 2013, 37, 522–531. [Google Scholar] [CrossRef]
- Rubinson, D.A.; Hochster, H.S.; Ryan, D.P.; Wolpin, B.M.; McCleary, N.J.; Abrams, T.A.; Chan, J.A.; Iqbal, S.; Lenz, H.J.; Lim, D.; et al. Multi-drug inhibition of the HER pathway in metastatic colorectal cancer: Results of a phase I study of pertuzumab plus cetuximab in cetuximab-refractory patients. Investig. New Drugs. 2014, 32, 113–122. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Trusolino, L.; Martino, C.; Bencardino, K.; Lonardi, S.; Bergamo, F.; Zagonel, V.; Leone, F.; Depetris, I.; Martinelli, E.; et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): A proof-of-concept, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 738–746, Erratum in Lancet Oncol. 2016, 17, e420. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Hurwitz, H.; Raghav, K.P.S.; McWilliams, R.R.; Fakih, M.; VanderWalde, A.; Swanton, C.; Kurzrock, R.; Burris, H.; Sweeney, C.; et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): An updated report from a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2019, 20, 518–530. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Lonardi, S.; Martino, C.; Fenocchio, E.; Tosi, F.; Ghezzi, S.; Leone, F.; Bergamo, F.; Zagonel, V.; Ciardiello, F.; et al. Pertuzumab and trastuzumab emtansine in patients with HER2-amplified metastatic colorectal cancer: The phase II HERACLES-B trial. ESMO Open 2020, 5, e000911. [Google Scholar] [CrossRef]
- Siena, S.; Di Bartolomeo, M.; Raghav, K.; Masuishi, T.; Loupakis, F.; Kawakami, H.; Yamaguchi, K.; Nishina, T.; Fakih, M.; Elez, E.; et al. Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2021, 22, 779–789. [Google Scholar] [CrossRef]
- Rossi, H.A.; Liu, Q.; Banner, B.; Hsieh, C.C.; Savas, L.; Savarese, D. The prognostic value of invariant chain (Ii) and Her-2/neu expression in curatively resected colorectal cancer. Cancer J. 2002, 8, 268–275. [Google Scholar] [CrossRef]
- Knösel, T.; Yu, Y.; Stein, U.; Schwabe, H.; Schlüns, K.; Schlag, P.M.; Dietel, M.; Petersen, I. Overexpression of c-erbB-2 protein correlates with chromosomal gain at the c-erbB-2 locus and patient survival in advanced colorectal carcinomas. Clin. Exp. Metastasis 2002, 19, 401–407. [Google Scholar] [CrossRef]
- Nathanson, D.R.; Culliford, A.T., IV; Shia, J.; Chen, B.; D’Alessio, M.; Zeng, Z.S.; Nash, G.M.; Gerald, W.; Barany, F.; Paty, P.B. HER 2/neu expression and gene amplification in colon cancer. Int. J. Cancer 2003, 105, 796–802. [Google Scholar] [CrossRef]
- Schuell, B.; Gruenberger, T.; Scheithauer, W.; Zielinski, C.; Wrba, F. HER 2/neu protein expression in colorectal cancer. BMC Cancer 2006, 6, 123. [Google Scholar] [CrossRef]
- Kountourakis, P.; Pavlakis, K.; Psyrri, A.; Rontogianni, D.; Xiros, N.; Patsouris, E.; Pectasides, D.; Economopoulos, T. Clinicopathologic significance of EGFR and Her-2/neu in colorectal adenocarcinomas. Cancer J. 2006, 12, 229–236. [Google Scholar] [CrossRef]
- Park, D.I.; Kang, M.S.; Oh, S.J.; Kim, H.J.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Han, W.K.; Kim, H.; et al. HER-2/neu overexpression is an independent prognostic factor in colorectal cancer. Int. J. Colorectal. Dis. 2007, 22, 491–497. [Google Scholar] [CrossRef]
- Ismail, H.M.; El-Baradie, M.; Moneer, M.; Khorshid, O.; Touny, A. Clinico-Pathological and Prognostic Significance of p53, Bcl-2 and Her-2/neu Protein Markers in Colorectal Cancer Using Tissue Microarray. J. Egypt. Natl. Cancer Inst. 2007, 19, 3–14. [Google Scholar]
- Kavanagh, D.O.; Chambers, G.; O’Grady, L.; Barry, K.M.; Waldron, R.P.; Bennani, F.; Eustace, P.W.; Tobbia, I. Is overexpression of HER-2 a predictor of prognosis in colorectal cancer? BMC Cancer 2009, 9, 1. [Google Scholar] [CrossRef]
- Marx, A.H.; Burandt, E.C.; Choschzick, M.; Simon, R.; Yekebas, E.; Kaifi, J.T.; Mirlacher, M.; Atanackovic, D.; Bokemeyer, C.; Fiedler, W.; et al. Heterogenous high-level HER-2 amplification in a small subset of colorectal cancers. Hum. Pathol. 2010, 41, 1577–1585. [Google Scholar] [CrossRef]
- Li, Q.; Wang, D.; Li, J.; Chen, P. Clinicopathological and prognostic significance of HER-2/neu and VEGF expression in colon carcinomas. BMC Cancer 2011, 11, 277. [Google Scholar] [CrossRef]
- Herreros-Villanueva, M.; Rodrigo, M.; Claver, M.; Muñiz, P.; Lastra, E.; García-Girón, C.; Coma del Corral, M.J. KRAS, BRAF, EGFR and HER2 gene status in a Spanish population of colorectal cancer. Mol. Biol. Rep. 2011, 38, 1315–1320. [Google Scholar] [CrossRef] [PubMed]
- Pappas, A.; Lagoudianakis, E.; Seretis, C.; Tsiambas, E.; Koronakis, N.; Toutouzas, K.; Katergiannakis, V.; Manouras, A. Clinical role of HER-2/neu expression in colorectal cancer. J. BUON 2013, 18, 98–104. [Google Scholar] [PubMed]
- Kwak, Y.; Yun, S.; Nam, S.K.; Seo, A.N.; Lee, K.S.; Shin, E.; Oh, H.K.; Kim, D.W.; Kang, S.B.; Kim, W.H.; et al. Comparative analysis of the EGFR, HER2, c-MYC, and MET variations in colorectal cancer determined by three different measures: Gene copy number gain, amplification status and the 2013 ASCO/CAP guideline criterion for HER2 testing of breast cancer. J. Transl. Med. 2017, 15, 167. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.S.; Fakih, M.; Ali, S.M.; Elvin, J.A.; Schrock, A.B.; Suh, J.; Vergilio, J.A.; Ramkissoon, S.; Severson, E.; Daniel, S.; et al. Targeting HER2 in colorectal cancer: The landscape of amplification and short variant mutations in ERBB2 and ERBB3. Cancer 2018, 124, 1358–1373. [Google Scholar] [CrossRef] [PubMed]
- Hasan, R.; Bhatt, D.; Khan, S.; Khan, V.; Verma, A.K.; Anees, A.; Dev, K. Association of Her-2 Expression and Clinicopathological Parameters in Colorectal Carcinoma in Indian Population. Open Access Maced. J. Med. Sci. 2018, 7, 6–11. [Google Scholar] [CrossRef]
- Richman, S.D.; Southward, K.; Chambers, P.; Cross, D.; Barrett, J.; Hemmings, G.; Taylor, M.; Wood, H.; Hutchins, G.; Foster, J.M.; et al. HER2 overexpression and amplification as a potential therapeutic target in colorectal cancer: Analysis of 3256 patients enrolled in the QUASAR, FOCUS and PICCOLO colorectal cancer trials. J. Pathol. 2016, 238, 562–570. [Google Scholar] [CrossRef]
- Ramanathan, R.K.; Hwang, J.J.; Zamboni, W.C.; Sinicrope, F.A.; Safran, H.; Wong, M.K.; Earle, M.; Brufsky, A.; Evans, T.; Troetschel, M.; et al. Low overexpression of HER-2/neu in advanced colorectal cancer limits the usefulness of trastuzumab (Herceptin) and irinotecan as therapy. A phase II trial. Cancer Investig. 2004, 22, 858–865. [Google Scholar] [CrossRef]
- Hashimoto, K.; Yamamoto, H.; Shiratsuchi, H.; Nakashima, T.; Tamiya, S.; Nishiyama, K.I.; Higaki, Y.; Komune, S.; Tsuneyoshi, M.; Oda, Y. HER-2/neu gene amplification in carcinoma ex pleomorphic adenoma in relation to progression and prognosis: A chromogenic in-situ hybridization study. Histopathology 2012, 60, E131–E142. [Google Scholar] [CrossRef]
- Haddad, R.; Colevas, A.; Krane, J.F.; Cooper, D.; Glisson, B.; Amrein, P.C.; Weeks, L.; Costello, R.; Posner, M. Herceptin in patients with advanced or metastatic salivary gland carcinomas. A phase II study. Oral Oncol. 2003, 39, 724–727. [Google Scholar] [CrossRef]
- Agulnik, M.; Cohen, E.W.; Cohen, R.B.; Chen, E.X.; Vokes, E.E.; Hotte, S.J.; Winquist, E.; Laurie, S.; Hayes, D.N.; Dancey, J.E.; et al. Phase II study of lapatinib in recurrent or metastatic epidermal growth factor receptor and/or erbB2 expressing adenoid cystic carcinoma and non adenoid cystic carcinoma malignant tumors of the salivary glands. J. Clin. Oncol. 2007, 25, 3978–3984. [Google Scholar] [CrossRef]
- Perissinotti, A.J.; Lee Pierce, M.; Pace, M.B.; El-Naggar, A.; Kies, M.S.; Kupferman, M. The role of trastuzumab in the management of salivary ductal carcinomas. Anticancer Res. 2013, 33, 2587–2591. [Google Scholar]
- Lee, J.S.; Kwon, O.J.; Park, J.J.; Seo, J.H. Salivary duct carcinoma of the parotid gland: Is adjuvant HER-2-targeted therapy required? J. Oral Maxillofac. Surg. 2014, 72, 1023–1031. [Google Scholar] [CrossRef]
- Takahashi, H.; Tada, Y.; Saotome, T.; Akazawa, K.; Ojiri, H.; Fushimi, C.; Masubuchi, T.; Matsuki, T.; Tani, K.; Osamura, R.Y.; et al. Phase II Trial of Trastuzumab and Docetaxel in Patients with Human Epidermal Growth Factor Receptor 2-Positive Salivary Duct Carcinoma. J. Clin. Oncol. 2019, 37, 125–134. [Google Scholar] [CrossRef]
- Press, M.F.; Pike, M.C.; Hung, G.; Zhou, J.Y.; Ma, Y.; George, J.; Dietz-Band, J.; James, W.; Slamon, D.J.; Batsakis, J.G.; et al. Amplification and overexpression of HER-2/neu in carcinomas of the salivary gland: Correlation with poor prognosis. Cancer Res. 1994, 54, 5675–5682. [Google Scholar]
- Skalova, A.; Starek, K.V.; Szepe, P.; Plank, L. Salivary duct carcinoma-a highly aggressive salivary gland tumour with HER-2/neuoncoprotein overexpression. Pathol. Res. Pract. 2001, 197, 621–626. [Google Scholar] [CrossRef]
- Skalova, A.; Starek, I.; Vanecek, T.; Kucerova, V.; Plank, L.; Szepe, P.; Di Palma, S.; Leivo, I. Expression of HER-2/neu gene and protein in salivary duct carcinomas of parotid gland as revealed by fluorescence in-situ hybridization and immunohistochemistry. Histopathology 2003, 42, 348–356. [Google Scholar] [CrossRef]
- Etges, A.; Pinto, D.S., Jr.; Kowalski, L.P.; Soares, F.A.; Araujo, V.C. Salivary duct carcinoma: Immunohistochemical profile of an aggressive salivary gland tumour. J. Clin. Pathol. 2003, 56, 914–918. [Google Scholar] [CrossRef]
- Jaehne, M.; Roeser, K.; Jaekel, T.; Schepers, J.D.; Albert, N.; Loning, T. Clinical and immunohistologic typing of salivary duct carcinoma: A report of 50 cases. Cancer 2005, 103, 2526–2533. [Google Scholar] [CrossRef]
- Cornolti, G.; Ungari, M.; Morassi, M.L.; Facchetti, F.; Rossi, E.; Lombardi, D.; Nicolai, P. Amplification and overexpression of HER2/neu gene and HER2/neu protein in salivary duct carcinoma of the parotid gland. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 1031–1036. [Google Scholar] [CrossRef]
- Johnson, C.J.; Barry, M.B.; Vasef, M.A.; Deyoung, B.R. Her-2/neu expression in salivary duct carcinoma: An immunohistochemical and chromogenic in situ hybridization study. Appl. Immunohistochem. Mol. Morphol. 2008, 16, 54–58. [Google Scholar] [CrossRef]
- Santana, T.; Pavel, A.; Martinek, P.; Steiner, P.; Grossmann, P.; Baněčková, M.; Skálová, A. Biomarker immunoprofile and molecular characteristics in salivary duct carcinoma: Clinicopathological and prognostic implications. Hum. Pathol. 2019, 93, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.D.; Roberts, D.B.; Kies, M.S.; Mao, L.; Weber, R.S.; El-Naggar, A.K. Genetic and expression analysis of HER-2 and EGFR genes in salivary duct carcinoma: Empirical and therapeutic significance. Clin. Cancer Res. 2010, 16, 2266–2274. [Google Scholar] [CrossRef] [PubMed]
- Clauditz, T.S.; Reiff, M.; Gravert, L.; Gnoss, A.; Tsourlakis, M.C.; Münscher, A.; Sauter, G.; Bokemeyer, C.; Knecht, R.; Wilczak, W. Human epidermal growth factor receptor 2 (HER2) in salivary gland carcinomas. Pathology 2011, 43, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Nardi, V.; Sadow, P.M.; Juric, D.; Zhao, D.; Cosper, A.K.; Bergethon, K.; Scialabba, V.L.; Batten, J.M.; Borger, D.R.; Iafrate, A.J.; et al. Detection of novel actionable genetic changes in salivary duct carcinoma helps direct patient treatment. Clin. Cancer Res. 2013, 19, 480–490. [Google Scholar] [CrossRef]
- Xia, L.; Hu, Y.; Li, J.; Gu, T.; Zhang, C.; Wang, L.; Tian, Z. A low percentage of HER-2 amplification whereas indicates poor prognosis in salivary carcinoma ex pleomorphic adenoma: A study of 140 cases. J. Oral Pathol. Med. 2017, 46, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Tsiambas, E.; Karameris, A.; Dervenis, C.; Lazaris, A.C.; Giannakou, N.; Gerontopoulos, K.; Patsouris, E. HER2/neu expression and gene alterations in pancreatic ductal adenocarcinoma: A comparative immunohistochemistry and chromogenic in situ hybridization study based on tissue microarrays and computerized image analysis. JOP 2006, 7, 283–294. [Google Scholar]
- Chou, A.; Waddell, N.; Cowley, M.J.; Gill, A.J.; Chang, D.K.; Patch, A.-M.; Nones, K.; Wu, J.; Pinese, M.; Johns, A.L.; et al. Clinical and molecular characterization of HER2 amplified-pancreatic cancer. Genome Med. 2013, 5, 78. [Google Scholar] [CrossRef]
- Safran, H.; Iannitti, D.; Ramanathan, R.; Schwartz, J.D.; Steinhoff, M.; Nauman, C.; Hesketh, P.; Rathore, R.; Wolff, R.; Tantravahi, U.; et al. Herceptin and gemcitabine for metastatic pancreatic cancers that overexpress HER-2/neu. Cancer Investig. 2004, 22, 706–712. [Google Scholar] [CrossRef]
- Assenat, E.; Azria, D.; Mollevi, C.; Guimbaud, R.; Tubiana-Mathieu, N.; Smith, D.; Delord, J.P.; Samalin, E.; Portales, F.; Larbouret, C.; et al. Dual targeting of HER1/EGFR and HER2 with cetuximab and trastuzumab in patients with metastatic pancreatic cancer after gemcitabine failure: Results of the “THERAPY”phase 1-2 trial. Oncotarget 2015, 6, 12796–12808. [Google Scholar] [CrossRef]
- Lei, S.; Appert, H.E.; Nakata, B.; Domenico, D.R.; Kim, K.; Howard, J.M. Overexpression of HER2/neu oncogene in pancreatic cancer correlates with shortened survival. Int. J. Pancreatol. 1995, 17, 15–21. [Google Scholar] [CrossRef]
- Day, J.D.; Digiuseppe, J.A.; Yeo, C.; Lai-Goldman, M.; Anderson, S.M.; Goodman, S.N.; Kern, S.E.; Hruban, R.H. Immunohistochemical evaluation of HER-2/neu expression in pancreatic adenocarcinoma and pancreatic intraepithelial neoplasms. Hum. Pathol. 1996, 27, 119–124. [Google Scholar] [CrossRef]
- Dugan, M.C.; Dergham, S.T.; Kucway, R.; Singh, K.; Biernat, L.; Du, W.; Vaitkevicius, V.K.; Crissman, J.D.; Sarkar, F.H. HER-2/neu expression in pancreatic adenocarcinoma: Relation to tumor differentiation and survival. Pancreas 1997, 14, 229–236. [Google Scholar] [CrossRef]
- Safran, H.; Steinhoff, M.; Mangray, S.; Rathore, R.; King, T.C.; Chai, L.; Berzein, K.; Moore, T.; Iannitti, D.; Reiss, P.; et al. Overexpression of the HER-2/neu oncogene in pancreatic adenocarcinoma. Am. J. Clin. Oncol. 2001, 24, 496–499, Erratum in Am. J. Clin. Oncol. 2002, 25, 181. [Google Scholar] [CrossRef]
- Novotný, J.; Petruzelka, L.; Vedralová, J.; Kleibl, Z.; Matous, B.; Juda, L. Prognostic significance of c-erbB-2 gene expression in pancreatic cancer patients. Neoplasma 2001, 48, 188–191. [Google Scholar]
- Potti, A.; Ganti, A.K.; Tendulkar, K.; Chitajallu, S.; Sholes, K.; Koch, M.; Kargas, S. HER-2/neu and CD117 (C-kit) overexpression in hepatocellular and pancreatic carcinoma. Anticancer Res. 2003, 23, 2671–2674. [Google Scholar]
- Hermanová, M.; Lukás, Z.; Nenutil, R.; Brázdil, J.; Kroupová, I.; Kren, L.; Pazourková, M.; Růzicka, M.; Díte, P. Amplification and overexpression of HER-2/neu in invasive ductal carcinomas of the pancreas and pancreatic intraepithelial neoplasms and the relationship to the expression of p21(WAF1/CIP1). Neoplasma 2004, 51, 77–83. [Google Scholar]
- Tamiolakis, D.; Venizelos, I.; Simopoulos, C.; Kotini, A.; Jivannakis, T.; Papadopoulos, N. Correlation of immunohistochemically detected HER-2/neu (c-erbB-2) with histological stage and perineural invasion in pancreatic cancer. Hepatogastroenterology 2004, 51, 334–337. [Google Scholar]
- Stoecklein, N.H.; Luebke, A.M.; Erbersdobler, A.; Knoefel, W.T.; Schraut, W.; Verde, P.E.; Stern, F.; Scheunemann, P.; Peiper, M.; Eisenberger, C.F.; et al. Copy number of chromosome 17 but not HER2 amplification predicts clinical outcome of patients with pancreatic ductal adenocarcinoma. J. Clin. Oncol. 2004, 22, 4737–4745. [Google Scholar] [CrossRef]
- Sharif, S.; Ramanathan, R.K.; Potter, D.; Cieply, K.; Krasinskas, A.M. HER2 gene amplification and chromosome 17 copy number do not predict survival of patients with resected pancreatic adenocarcinoma. Dig. Dis. Sci. 2008, 53, 3026–3032. [Google Scholar] [CrossRef]
- Komoto, M.; Nakata, B.; Amano, R.; Yamada, N.; Yashiro, M.; Ohira, M.; Wakasa, K.; Hirakawa, K. HER2 overexpression correlates with survival after curative resection of pancreatic cancer. Cancer Sci. 2009, 100, 1243–1247. [Google Scholar] [CrossRef]
- Harder, J.; Ihorst, G.; Heinemann, V.; Hofheinz, R.; Moehler, M.; Buechler, P.; Kloeppel, G.; Röcken, C.; Bitzer, M.; Boeck, S.; et al. Multicentre phase II trial of trastuzumab and capecitabine in patients with HER2 overexpressing metastatic pancreatic cancer. Br. J. Cancer 2012, 106, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Assenat, E.; Mineur, L.; Mollevi, C.; Lopez-Crapez, E.; Lombard-Bohas, C.; Samalin, E.; Portales, F.; Walter, T.; Forges, H.; Dupuy, M.; et al. Phase II study evaluating the association of gemcitabine, trastuzumab and erlotinib as first-line treatment in patients with metastatic pancreatic adenocarcinoma (GATE 1). Int. J. Cancer 2021, 148, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Gan, K.; Gao, Y.; Liu, K.; Xu, B.; Qin, W. The Clinical Significance and Prognostic Value of HER2 Expression in Bladder Cancer: A Meta-Analysis and a Bioinformatic Analysis. Front. Oncol. 2021, 11, 653491. [Google Scholar] [CrossRef]
- Hussain, M.H.; MacVicar, G.R.; Petrylak, D.P.; Dunn, R.L.; Vaishampayan, U.; Lara, P.N., Jr.; Chatta, G.S.; Nanus, D.M.; Glode, L.M.; Trump, D.L.; et al. Trastuzumab, paclitaxel, carboplatin, and gemcitabine in advanced human epidermal growth factor receptor-2/neu-positive urothelial carcinoma: Results of a multicenter phase II National Cancer Institute trial. J. Clin. Oncol. 2007, 25, 2218–2224, Erratum in J. Clin. Oncol. 2008, 26, 3295. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Huddart, R.A.; Elliott, T.; Sarker, S.J.; Ackerman, C.; Jones, R.; Hussain, S.; Crabb, S.; Jagdev, S.; Chester, J.; et al. Phase III, Double-Blind, Randomized Trial that Compared Maintenance Lapatinib Versus Placebo after First-Line Chemotherapy in Patients with Human Epidermal Growth Factor Receptor 1/2-Positive Metastatic Bladder Cancer. J. Clin. Oncol. 2017, 35, 48–55. [Google Scholar] [CrossRef]
- Sheng, X.; Yan, X.; Wang, L.; Shi, Y.; Yao, X.; Luo, H.; Shi, B.; Liu, J.; He, Z.; Yu, G.; et al. Open-label, Multicenter, Phase II Study of RC48-ADC, a HER2-Targeting Antibody-Drug Conjugate, in Patients with Locally Advanced or Metastatic Urothelial Carcinoma. Clin. Cancer Res. 2021, 27, 43–51. [Google Scholar] [CrossRef]
- Nishio, Y.; Yamada, Y.; Kokubo, H.; Nakamura, K.; Aoki, S.; Taki, T.; Honda, N.; Nakagawa, A.; Saga, S.; Hara, K. Prognostic significance of immunohistochemical expression of the Her-2/neu oncoprotein in bone metastatic prostate cancer. Urology 2006, 68, 110–115. [Google Scholar] [CrossRef]
- Morote, J.; de Torres, I.; Caceres, C.; Vallejo, C.; Schwartz, S., Jr.; Reventos, J. Prognostic value of immunohistochemical expression of the c-erbB-2 oncoprotein in metastatic prostate cancer. Int. J. Cancer 1999, 84, 421–425. [Google Scholar] [CrossRef]
- Neto, A.S.; Tobias-Machado, M.; Wroclawski, M.L.; Fonseca, F.L.; Teixeira, G.K.; Amarante, R.D.; Wroclawski, E.R.; Del Giglio, A. Her-2/neu expression in prostate adenocarcinoma: A systematic review and meta-analysis. J. Urol. 2010, 184, 842–850. [Google Scholar] [CrossRef]
- Ziada, A.; Barqawi, A.; Glode, L.M.; Varella-Garcia, M.; Crighton, F.; Majeski, S.; Rosenblum, M.; Kane, M.; Chen, L.; Crawford, E.D. The use of trastuzumab in the treatment of hormone refractory prostate cancer; phase II trial. Prostate 2004, 60, 332–337. [Google Scholar] [CrossRef]
- Lara, P.N., Jr.; Chee, K.G.; Longmate, J.; Ruel, C.; Meyers, F.J.; Gray, C.R.; Edwards, R.G.; Gumerlock, P.H.; Twardowski, P.; Doroshow, J.H.; et al. Trastuzumab plus docetaxel in HER-2/neu-positive prostate carcinoma: Final results from the California Cancer Consortium Screening and Phase II Trial. Cancer 2004, 100, 2125–2131. [Google Scholar] [CrossRef]
- Curigliano, G.; De Braud, F.; Teresa Sandri, M.; Renne, G.; Zorzino, L.; Scardino, E.; Rocco, B.; Spitaleri, G.; De Pas, T.; Noberasco, C.; et al. Gefitinib combined with endocrine manipulation in patients with hormone-refractory prostate cancer: Quality of life and surrogate markers of activity. Anticancer Drugs 2007, 18, 949–954. [Google Scholar] [CrossRef]
- de Bono, J.S.; Bellmunt, J.; Attard, G.; Droz, J.P.; Miller, K.; Flechon, A.; Sternberg, C.; Parker, C.; Zugmaier, G.; Hersberger-Gimenez, V.; et al. Open-label phase II study evaluating the efficacy and safety of two doses of pertuzumab in castrate chemotherapy-naive patients with hormone-refractory prostate cancer. J. Clin. Oncol. 2007, 25, 257–262. [Google Scholar] [CrossRef]
- Agus, D.B.; Sweeney, C.J.; Morris, M.J.; Mendelson, D.S.; McNeel, D.G.; Ahmann, F.R.; Wang, J.; Derynck, M.K.; Ng, K.; Lyons, B.; et al. Efficacy and safety of single-agent pertuzumab (rhuMAb 2C4), a human epidermal growth factor receptor dimerization inhibitor, in castration-resistant prostate cancer after progression from taxane-based therapy. J. Clin. Oncol. 2007, 25, 675–681. [Google Scholar] [CrossRef]
- Vuky, J.; Porter, C.; Isacson, C.; Vaughan, M.; Kozlowski, P.; Picozzi, V.; Corman, J. Phase II trial of neoadjuvant docetaxel and gefitinib followed by radical prostatectomy in patients with high-risk, locally advanced prostate cancer. Cancer 2009, 115, 784–791. [Google Scholar] [CrossRef]
- Whang, Y.E.; Armstrong, A.J.; Rathmell, W.K.; Godley, P.A.; Kim, W.Y.; Pruthi, R.S.; Wallen, E.M.; Crane, J.M.; Moore, D.T.; Grigson, G.; et al. A phase II study of lapatinib, a dual EGFR and HER-2 tyrosine kinase inhibitor, in patients with castration-resistant prostate cancer. Urol. Oncol. 2013, 31, 82–86. [Google Scholar] [CrossRef]
- Roa, I.; de Toro, G.; Schalper, K.; de Aretxabala, X.; Churi, C.; Javle, M. Overexpression of the HER2/neu gene: A new therapeutic possibility for patients with advanced gallbladder cancer. Gastrointest. Cancer Res. 2014, 7, 42–48. [Google Scholar]
- Kawamoto, T.; Krishnamurthy, S.; Tarco, E.; Trivedi, S.; Wistuba, I.I.; Li, D.; Roa, I.; Roa, J.C.; Thomas, M.B. HER receptor family: Novel candidate for targeted therapy for gallbladder and extrahepatic bile duct cancer. Gastrointest. Cancer Res. 2007, 1, 221–227. [Google Scholar]
- Toledo, C.; Matus, C.E.; Barraza, X.; Arroyo, P.; Ehrenfeld, P.; Figueroa, C.D.; Bhoola, K.D.; Del Pozo, M.; Poblete, M.T. Expression of HER2 and bradykinin B(1) receptors in precursor lesions of gallbladder carcinoma. World J. Gastroenterol. 2012, 18, 1208–1215. [Google Scholar] [CrossRef]
- Harder, J.; Waiz, O.; Otto, F.; Geissler, M.; Olschewski, M.; Weinhold, B.; Blum, H.E.; Schmitt-Graeff, A.; Opitz, O.G. EGFR and HER2 expression in advanced biliary tract cancer. World J. Gastroenterol. 2009, 15, 4511–4517. [Google Scholar] [CrossRef]
- Albrecht, T.; Rausch, M.; Roessler, S.; Geissler, V.; Albrecht, M.; Halske, C.; Seifert, C.; Renner, M.; Singer, S.; Mehrabi, A.; et al. HER2 gene (ERBB2) amplification is a low-frequency driver with potential predictive value in gallbladder carcinoma. Virchows Arch. 2020, 476, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.; Churi, C.; Kang, H.C.; Shroff, R.; Janku, F.; Surapaneni, R.; Zuo, M.; Barrera, C.; Alshamsi, H.; Krishnan, S.; et al. HER2/neu-directed therapy for biliary tract cancer. J. Hematol. Oncol. 2015, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Pignochino, Y.; Sarotto, I.; Peraldo-Neia, C.; Penachioni, J.Y.; Cavalloni, G.; Migliardi, G.; Casorzo, L.; Chiorino, G.; Risio, M.; Bardelli, A.; et al. Targeting EGFR/HER2 pathways enhances the antiproliferative effect of gemcitabine in biliary tract and gallbladder carcinomas. BMC Cancer 2010, 10, 631. [Google Scholar] [CrossRef] [PubMed]
- Gorlick, R.; Huvos, A.G.; Heller, G.; Aledo, A.; Beardsley, G.P.; Healey, J.H.; Meyers, P.A. Expression of HER2/erbB-2 correlates with survival in osteosarcoma. J. Clin. Oncol. 1999, 17, 2781–2788. [Google Scholar] [CrossRef] [PubMed]
- Onda, M.; Matsuda, S.; Higaki, S.; Iijima, T.; Fukushima, J.; Yokokura, A.; Kojima, T.; Horiuchi, H.; Kurokawa, T.; Yamamoto, T. ErbB-2 expression is correlated with poor prognosis for patients with osteosarcoma. Cancer 1996, 77, 71–78. [Google Scholar] [CrossRef]
- Akatsuka, T.; Wada, T.; Kokai, Y.; Sawada, N.; Yamawaki, S.; Ishii, S. Loss of ErbB2 expression in pulmonary metastatic lesions in osteosarcoma. Oncology 2001, 60, 361–366. [Google Scholar] [CrossRef]
- Thomas, D.G.; Giordano, T.J.; Sanders, D.; Biermann, J.S.; Baker, L. Absence of HER2/neu gene expression in osteosarcoma and skeletal Ewing’s sarcoma. Clin. Cancer Res. 2002, 8, 788–793. [Google Scholar]
- Anninga, J.K.; van de Vijver, M.J.; Cleton-Jansen, A.M.; Kristel, P.M.; Taminiau, A.H.; Nooij, M.; Egeler, R.M.; Hogendoorn, P.C. Overexpression of the HER-2 oncogene does not play a role in high-grade osteosarcomas. Eur. J. Cancer 2004, 40, 963–970. [Google Scholar] [CrossRef]
- Kremser, R.; Obrist, P.; Spizzo, G.; Erler, H.; Kendler, D.; Kemmler, G.; Mikuz, G.; Ensinger, C. Her2/neu overexpression in differentiated thyroid carcinomas predicts metastatic disease. Virchows Arch. 2003, 442, 322–328. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Campennì, A.; Giuffrè, G.; Giovanella, L.; Siracusa, M.; Simone, A.; Branca, G.; Scarfì, R.; Trimarchi, F.; Ieni, A.; et al. HER2 Analysis in Sporadic Thyroid Cancer of Follicular Cell Origin. Int. J. Mol. Sci. 2016, 17, 2040. [Google Scholar] [CrossRef]
- Haugen, D.R.; Akslen, L.A.; Varhaug, J.E.; Lillehaug, J.R. Expression of c-erbB-2 protein in papillary thyroid carcinomas. Br. J. Cancer 1992, 65, 832–837. [Google Scholar] [CrossRef]
- Ensinger, C.; Prommegger, R.; Kendler, D.; Gabriel, M.; Spizzo, G.; Mikuz, G.; Kremser, R. Her2/neu expression in poorly-differentiated and anaplastic thyroid carcinomas. Anticancer Res. 2003, 23, 2349–2353. [Google Scholar]
- Ensinger, C.; Prommegger, R.; Kendler, D.; Gabriel, M.; Spizzo, G.; Mikuz, G.; Kremser, R. Her2/neu expression in C-cell hyperplasia and medullary thyroid carcinomas. Anticancer Res. 2003, 23, 2241–2243. [Google Scholar]
- Koka, V.; Potti, A.; Forseen, S.E.; Pervez, H.; Fraiman, G.N.; Koch, M.; Levitt, R. Role of Her-2/neu overexpression and clinical determinants of early mortality in glioblastoma multiforme. Am. J. Clin. Oncol. 2003, 26, 332–335. [Google Scholar] [CrossRef]
- Forseen, S.E.; Potti, A.; Koka, V.; Koch, M.; Fraiman, G.; Levitt, R. Identification and relationship of HER-2/neu overexpression to short-term mortality in primary malignant brain tumors. Anticancer Res. 2002, 22, 1599–1602. [Google Scholar]
- Mineo, J.F.; Bordron, A.; Quintin-Roué, I.; Loisel, S.; Ster, K.L.; Buhé, V.; Lagarde, N.; Berthou, C. Recombinant humanised anti-HER2/neu antibody (Herceptin) induces cellular death of glioblastomas. Br. J. Cancer 2004, 91, 1195–1199. [Google Scholar] [CrossRef]
- Buhring, H.J.; Sures, I.; Jallal, B.; Weiss, F.U.; Busch, F.W.; Ludwig, W.D.; Handgretinger, R.; Waller, H.D.; Ullrich, A. The receptor tyrosine kinase p185HER2 is expressed on a subset of B-lymphoid blasts from patients with acute lymphoblastic leukemia and chronic myelogenous leukemia. Blood 1995, 86, 1916–1923. [Google Scholar] [CrossRef]
- Chevallier, P.; Robillard, N.; Wuilleme-Toumi, S.; Mechinaud, F.; Harousseau, J.L.; Avet-Loiseau, H. Overexpression of Her2/neu is observed in one third of adult acute lymphoblastic leukemia patients and is associated with chemoresistance in these patients. Haematologica 2004, 89, 1399–1401. [Google Scholar]
- Muller, M.R.; Grunebach, F.; Kayser, K.; Vogel, W.; Nencioni, A.; Brugger, W.; Kanz, L.; Brossart, P. Expression of her-2/neu on acute lymphoblastic leukemias: Implications for the development of immunotherapeutic approaches. Clin. Cancer Res. 2003, 9, 3448–3453. [Google Scholar]
- Haen, S.P.; Schmiedel, B.J.; Rothfelder, K.; Schmied, B.J.; Dang, T.M.; Mirza, N.; Möhle, R.; Kanz, L.; Vogel, W.; Salih, H.R. Prognostic relevance of HER2/neu in acute lymphoblastic leukemia and induction of NK cell reactivity against primary ALL blasts by trastuzumab. Oncotarget 2016, 7, 13013–13030. [Google Scholar] [CrossRef]
- Chevallier, P.; Robillard, N.; Charbonnier, A.; Raffoux, E.; Maury, S.; Carras, S.; Chabrot, C.; Fohrer, C.; Bernard, M.; Blade, J.S.; et al. Trastuzumab for treatment of refractory/relapsed HER2-positive adult B-ALL: Results of a phase 2 GRAALL study. Blood 2012, 119, 2474–2477. [Google Scholar] [CrossRef] [PubMed]
- Nuciforo, P.G.; Pellegrini, C.; Fasani, R.; Maggioni, M.; Coggi, G.; Parafioriti, A.; Bosari, S. Molecular and immunohistochemical analysis of HER2/neu oncogene in synovial sarcoma. Hum. Pathol. 2003, 34, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Peiper, M.; Heinecke, A.; Zurakowski, D.; Eisenberger, C.F.; Hosch, S.; Knoefel, W.T.; Izbicki, J.R. Expression of HER2/neu does not correlate with survival in soft tissue sarcoma. Onkologie 2003, 26, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Babashahi, M.; Mehrazma, M.; Nasiri, S.J.; Azizi Jalilian, F.; Rezaei-Tavirani, M. Her2/neu Expression in Wilms’ Tumor and Correlation with Histopathologic Findings. Iran J. Cancer Prev. 2013, 6, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Ragab, S.M.; Samaka, R.M.; Shams, T.M. HER2/neu expression: A predictor for differentiation and survival in children with Wilms tumor. Pathol. Oncol. Res. 2010, 16, 61–67. [Google Scholar] [CrossRef]
- Kluger, H.M.; DiVito, K.; Berger, A.J.; Halaban, R.; Ariyan, S.; Camp, R.L.; Rimm, D.L. Her2/neu is not a commonly expressed therapeutic target in melanoma—A large cohort tissue microarray study. Melanoma Res. 2004, 14, 207–210. [Google Scholar] [CrossRef]
- Tarantino, P.; Morganti, S.; Curigliano, G. Targeting HER2 in breast cancer: New drugs and paradigms on the horizon. Explor. Target. Antitumor Ther. 2021, 2, 139–155. [Google Scholar] [CrossRef]
- Fong, C.; Chau, I. HER2 Inhibition in Gastric Cancer-Novel Therapeutic Approaches for an Established Target. Cancers 2022, 14, 3824. [Google Scholar] [CrossRef]
- Grieb, B.C.; Agarwal, R. HER2-Directed Therapy in Advanced Gastric and Gastroesophageal Adenocarcinoma: Triumphs and Troubles. Curr. Treat. Options Oncol. 2021, 22, 88. [Google Scholar] [CrossRef]
- Fader, A.N.; Roque, D.M.; Siegel, E.; Buza, N.; Hui, P.; Abdelghany, O.; Chambers, S.K.; Secord, A.A.; Havrilesky, L.; O’Malley, D.M.; et al. Randomized Phase II Trial of Carboplatin-Paclitaxel Versus Carboplatin-Paclitaxel-Trastuzumab in Uterine Serous Carcinomas That Overexpress Human Epidermal Growth Factor Receptor 2/neu. J. Clin. Oncol. 2018, 36, 2044–2051. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| IHC Score | Result | Staining Pattern | Percentage Of Stained Cells |
|---|---|---|---|
| 0 | Negative | Absent staining | 0 |
| 1+ | Negative | Faint or weak incomplete staining | <10% |
| 2+ | Equivocal | Thin circumferential membrane staining or heterogeneity in staining distribution | >10% but < 30% |
| 3+ | Positive | Diffuse intense circumferential membrane “chicken-wire” | >30% |
| Name of the Study | Number of Patients | Protein Overexpression (%) | Amplification (%) |
|---|---|---|---|
| Rubin SC et al., 1994 [19] | 40 | 20 | - |
| Seki A et al., 2000 [20] | 48 | - | 25 |
| Gao D et al., 2002 [21] | 54 | 25.9 | - |
| Hogdall et al., 2003 [22] | 181 | 13.3 | - |
| Bookman MA et al., 2003 [23] | 837 | 11.4 | - |
| Camilleri-Broet et al., 2004 [24] | 95 | 15.8 | - |
| Mano MS et al., 2004 [25] | 64 | - | 12.5 |
| Lee CH et al., 2005 [26] | 102 | 4.9 | 2 |
| Tuefferd M et al., 2007 [27] | 320 | 12.8 | 6.6 |
| Sasaki N et al., 2007 [28] | 141 | 12.8 | - |
| Sueblinvong et al., 2007 [29] | 74 | 10.2 | - |
| Stefensen KD et al., 2008 [30] | 99 | 14.1 | - |
| Vermeij et al., 2008 [31] | 52 | 35 | 10 |
| Farley J et al., 2009 [32] | 133 | - | 6.8 |
| Chekerov R et al., 2009 [33] | 50 | 52 | - |
| Slyvia MT et al., 2012 [34] | 60 | 21 | - |
| Jafri A et al., 2017 [35] | 56 | 37.5 | - |
| Pankaj S et al., 2019 [36] | 98 | 22.45 | - |
| Clinical Trial | Study Description | Indication | PEP and Treatment Arms | Outcomes |
|---|---|---|---|---|
| 1. Bookman MA et al., 2003 [23] | Single arm, Phase II, N = 95 | HER2 2+ or 3+ overexpressing refractory epithelial ovarian or primary peritoneal cancer | ORR and Trastuzumab |
|
| 2. Makhija S et al., 2010 [37] | Phase II, Randomized, N = 130 | Advanced, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer who had received a maximum of one prior treatment for recurrent cancer | Safety/PFS and Pertuzumab + Gemcitabine vs. Gemcitabine |
|
| Name of the Study | Number of Patients | Protein Overexpression (%) | Amplification (%) |
|---|---|---|---|
| Santin AD et al., 2002 [44] | 10 | 80 | - |
| Solomovitz BM et al., 2004 [45] | 68 | 18 | 2.9 |
| Santin AD et al., 2005 [46] | 30 | - | 47 |
| Santin AS et al., 2005 [43] | 26 | 62 | 42 |
| Diaz-Montes TP et al., 2006 [47] | 25 | 48 | - |
| Villella JA et al., 2006 [48] | 19 | 26 | - |
| Odicino FE et al., 2008 [49] | 12 | 16.6 | 16.6 |
| Ren Y et al., 2011 [50] | 36 | 36.1 | 11.1 |
| Togami S et al., 2012 [51] | 71 | 14 | - |
| Banet et al., 2021 [52] | 68 | 9 | - |
| Clinical Trial | Study Description | Indication | PEP and Treatment Arms | Outcomes |
|---|---|---|---|---|
| 1. Fleming GF et al., 2009, [53] | Single arm, Phase II, N = 34 | Stage III, IV or recurrent endometrial carcinoma with either 2+/3+ HER2 overexpression or gene amplification | ORR and Trastuzumab |
|
| 2.Tymon-Rosario J et al., 2021 [54] | Multi-center, Phase II, N = 60 | Recurrent/Advanced (Stage III–IV) HER2/neu overexpressing uterine serous carcinoma | PFS and Carboplatin/Paclitaxel +Trastuzumab vs. Carboplatin/Paclitaxel alone |
|
| Name of the Study | Number of Patients | Mutations (%) |
|---|---|---|
| Shingematsu, H.I. et al., 2005 [59] | 671 | 2.6 |
| Buttitta, F.L. et al., 2006 [70] | 403 | 2.2 |
| Sasaki, Y. et al., 2006 [71] | 122 | 0.8 |
| Sun, Y. et al., 2010 [72] | 52 | 3.8 |
| Tomizawa, K. et al., 2011 [73] | 504 | 2.6 |
| Li, C. et al., 2012 [74] | 224 | 3.6 |
| Arcila, M. et al., 2012 [75] | 1478 | 1.7 |
| Mazieres, J.I. et al., 2013 [76] | 3800 | 1.7 |
| Clinical Trial, Study Description | Study Description | Indication | PEP and Treatment Arms | Outcomes |
|---|---|---|---|---|
| 1. Cappuzzo, F. et al., 2003 [77] | Phase II, N = 63 | Advanced NSCLC | TP and Gefitinib |
|
| 2. Langer, C.J. et al., 2004 [78] | Phase II, N = 56 | HER2 overexpressing advanced NSCLC | OS and Trastuzumab + Paclitaxel + Carboplatin |
|
| 3. Gatzemeier, U. et al., 2004 [61] | Phase II Randomized, N= 103 | Untreated stage IIIB/IV HER2-positive NSCLC | ORR and Trastuzumab + Cisplatin + gemcitabine vs. Cisplatin + gemcitabine alone |
|
| 4. Zinner, R.G. et al., 2004 [62] | Phase II, N = 21 | HER2-overexpressing (IHC >1+ or HER2 neu antigen in serum) stages IIIB or IV NSCLC | ORR and Trastuzumab + cisplatin +Gemcitabine | 8 (38%) patients had a partial response
|
| 5. Lara, P.N., Jr. et al., 2004 [63] | Phase II, N = 13 | Advanced NSCLC in which primary platinum-based therapy had failed | Screening for HER2, ORR and Single agent Trastuzumab or docetaxel followed by combination Trastuzumab + Docetaxel |
|
| 6. Clamon, G. et al., 2005 [79] | Phase II, N = 29 | Stage IIIB or Stage IV NSCLC with 2+/3+ HER2 expression with at least 1 prior chemotherapy regimen. | Screening for HER2, ORR Single agent Trastuzumab |
|
| 7. Krug, L.M. et al., 2005 [80] | Phase II, Randomized, N = 169 | Previously untreated advanced NSCLC | ORR and Trastuzumab + Docetaxel or Trastuzumab + Paclitaxel |
|
| 8. Kris, M.G. et al., 2015 [67] | Phase II, N = 30 | Stage IIIB/IV lung cancers with HER2 mutations in exon 20 or amplification. | PRS, OS, toxicity and Dacomitinib |
|
| 9. Li, B.T. et al., 2018 [64] | Phase II, N = 18 | HER2 mutant lung adenocarcinomas | ORR and Ado-Trastuzumab emastine |
|
| 10. De Langen, A.J. et al., 2018 [81] | Phase II, N = 24 | NSCLC with a sensitizing EGFR mutation who show HER2 expression after progression on EGFR TKI treatment | ORR and Trastuzumab + Paclitaxel |
|
| 11. Peters, S. et al., 2019 [65] | Phase II, N = 49 | HER2-overexpressing advanced NSCLC who have received previous platinum-based chemotherapy and targeted therapy in the case of EGFR mutation or ALK gene rearrangement | ORR and Ado-Trastuzumab emastine |
|
| 12. ETOP TRIAL, Dziadziuszko et al., 2019 [68] | Phase II, N = 13 | Pretreated advanced NSCLC harboring HER2 exon 20 mutations | ORR and Afatinib |
|
| 13. Fan, Y. et al., 2020 [69] | Phase II, N = 18 | HER2 mutation positive Stage IIIB/IV non-small cell lung cancer had failed one or two prior lines of chemotherapy and were EGFR/HER2-inhibitor naïve. | ORR and Afatinib followed by Afatinib + Paclitaxel |
|
| 14. DESTINYLUNG01 TRIAL (NCT03505710) 2022 [66] | Phase II, N = 91 | HER2 mutant metastatic NSCLC refractory to standard treatment | ORR and Trastuzumab Deruxtecan |
|
| Name of the Study | Number of Patients | Protein Overexpression (%) | Amplification (%) |
|---|---|---|---|
| Rossi, H. et al., 2002 [91] | 156 | 24 | - |
| Knosel, T. et al., 2002 [92] | 74 | 51 | - |
| Nathanson, D.R. et al., 2003 [93] | 139–169 | 3.6 (5/139) | 2.4 (4/169) |
| Park, D.I. et al., 2004 [56] | 88 | 12.5 | - |
| Schuell, B. et al., 2006 [94] | 77 | 3.8 | - |
| Kountourakis, P. et al., 2006 [95] | 106 | 5.6 | - |
| Park, D.I. et al., 2007 [96] | 137 | 47.4 | 1.4 |
| Ismail, H.M. et al., 2007 [97] | 104 | 9.6 | - |
| Kavanagh, D.O., 2009 [98] | 132 | 11 | 3 |
| Marx, A.H. et al., 2010 [99] | 1439 | 2.5 | 2.7 |
| Li, Q. et al., 2011 [100] | 317 | 15.5 | - |
| Herreros Villanaueva, M. et al., 2011 [101] | 186 | - | 26.3 |
| Pappas, A. et al., 2013 [102] | 51 | 3.9 | - |
| Shabbir, A. et al., 2016 [83] | 95 | 78.9 | - |
| Kwak, Y. et al., 2017 [103] | 334 | - | 6 |
| Ross, J.S. et al., 2018 [104] | 8887 | - | 58.5 |
| Hasan, R. et al., 2018 [105] | 83 | 40.96 | - |
| Richman et al., 2019 [106] | 3256 | 1.6 | 1.4 |
| Clinical Trial | Study Description | Indication | PEP and Treatment Arms | Outcomes |
|---|---|---|---|---|
| 1. Ramanathan, R.K. et al., 2014 [107] | Phase II, N = 9 | HER2 overexpressing advanced CRC | HER2 expression rate, MTD and Trastuzumab + Irinotecan |
|
| 2. Rubinson, D.A. et al., 2014 [86] | Open label, Multi-center Phase I/II, N = 13 | Metastatic colorectal cancer with cetuximab resistance | Dose-limiting toxicity and Pertuzumab + cetuximab |
|
| 3. HERCALESA TRIAL, 2016 [87] | Multi-center, Open label, Phase II, N = 27 | KRAS exon 2 (codons 12 and 13) wild-type and HER2-positive metastatic colorectal cancer refractory to standard of care (including cetuximab or panitumumab) | ORR and Trastuzumab + lapatinib |
|
| 4. MY PATHWAY TRIAL (NCT02091141) 2019 [88] | Phase IIA, Multiple Basket, N = 57 | Refractory, histologically confirmed HER2-amplified metastatic colorectal cancer | ORR and Trastuzumab +Pertuzumab |
|
| 5. HERACLESB TRIAL (NCT03225937) 2020 [89] | Single arm, Phase II, N = 31 | Histologically confirmed RAS/BRAF wild-type and HER2+ metastatic CRC refractory to standard treatments | ORR and Trastuzumab emtansine +Pertuzumab |
|
| 6. DESTINYCRC01 TRIAL (NCT03384940) 2021 [90] | Open label, Multi-center, Phase II, N = 78 | HER-positive metastatic colorectal cancer that had progressed on two or more previous regimens (HER2-targeted therapies other than trastuzumab deruxtecan permitted) | ORR and Trastuzumab deruxtecan vs. standard treatment |
|
| Name of the Study | Histology | Number of Patients | Protein Overexpression (%) | Amplification (%) |
|---|---|---|---|---|
| Press, M.F. et al., 1994 [114] | Mucoepidermoid carcinoma | 58 | 38 | 21 |
| Skalova et al., 2001 [115] | SDC | 15 | 93.3 | - |
| Skalova, A. et al., 2003 [116] | SDC | 11 | 100 | 36.4 |
| Erges, A. et al., 2003 [117] | SDC | 5 | 80 | - |
| Jaehne et al., 2005 [118] | SDC | 50 | 20.6 | - |
| Cornolti, G. et al., 2007 [119] | SDC | 13 | 10/13 | 8/10 |
| Johnson, C.J. et al., 2008 [120] | SDC | 12 | 33.3 | 33.3 |
| Santana, T. et al., 2019 [121] | SDC | 25 | 42 | |
| William, M.D. et al., 2010 [122] | SDC | 66 | 10/66 | 6/10 |
| Clauditz, T.S. et al., 2011 [123] | SDC | 14 | 3/14 | 3/3 |
| Nardi, V. et al., 2013 [124] | SDC | 27 | - | 29.6 |
| Xia, L. et al., 2017 [125] | Invasive carcinoma ex pleomorphic adenoma | 140 | 25 |
| Clinical Trial | Study Description | Indication | PEP | Treatment Arms | Outcomes |
|---|---|---|---|---|---|
| 1. Haddad, R. et al., 2003, [109] | Single arm, Phase II, N = 14 | HER2 overexpressing (2+/3+) advanced incurable salivary gland tumors | TP | Trastuzumab |
|
| 2. Agulnik, M. et al., 2007 [110] | Single arm, Phase II, N = 40 | Progressive, recurrent, or metastatic adenoid cystic carcinoma (ACC) immunohistochemically expressing at least 1+ EGFR and/or 2+ erbB2 | ORR | Lapatinib |
|
| 3. Takahashi, H. et al., 2019 [113] | Single center, Single arm, Open label, Phase II, N = 57 | Locally advanced and/or recurrent or metastatic HER-positive SDC | ORR | Trastuzumab + Docetaxel |
|
| Name of the Study | Number of Patients | Protein Overexpression (%) | Amplification (%) |
|---|---|---|---|
| Lei, S. et al., 1995 [130] | 27 | 44.4 | - |
| Day, J.D. et al., 1996 [131] | 19 | 69 | - |
| Dugan, M.C. et al., 1997 [132] | 79 | 58 | - |
| Safran, H. et al., 2001 [133] | 154 | 21 | 7.1 |
| Novotny, J. et al., 2001 [134] | 57 | 19.2 | - |
| Potti et al., 2003 [135] | 39 | None | - |
| Hermanova, M. et al., 2004 [136] | 49 | 18.75 | 4 |
| Tamiolakis, D. et al., 2004 [137] | 100 | 21 | - |
| Sroecklein, N.H. et al., 2004 [138] | 50 | 10 | 24 |
| Tsiambas E et al., 2006 [126] | 50 | 59, 22, 12, 8 (0, 1+, 2+ and 3+ expression) | 16 |
| Sharif, S. et al., 2008 [139] | 63 | - | 25 |
| Komoro, M. et al., 2009 [140] | 129 | 61.2 | - |
| Harder, J. et al., 2012 [141] | 207 | 26 | 3.9 |
| Chou, A. et al., 2013 [127] | 469 | 7.2 | 2.1 |
| Clinical Trial | Study Description | Indication | PEP and Treatment Arms | Outcomes |
|---|---|---|---|---|
| 1. Safran, H. et al., 2004 [128] | Phase II, N = 34 | HER2 overexpressing metastatic pancreatic cancer | OS and Trastuzumab + Gemcitabine vs. Gemcitabine alone |
|
| 2.Harder, J. et al., 2012 [141] | Multi-center, Phase II, N = 17 | HER2 overexpressing metastatic Pancreatic adenocarcinoma | PFS and Trastuzumab + capecitabine |
|
| 3. THERAPY TRIAL (NCT00923299) 2015 [129] | Multi-center, Phase I/II, Single arm, Non-randomized | Advanced pancreatic cancer patients after first-line gemcitabine-based chemotherapy failure | ORR, OS, PFS and Trastuzumab + Cetuximab |
|
| 4. GATE I TRIAL (NCT01204372) 2021 [142] | Multi-center, Phase II, N = 63 | Metastatic pancreatic adenocarcinoma | DCR and Gemcitabine, Trastuzumab, Erlotinib vs. standard therapy |
|
| Clinical Trial | Study Description | Indication | PEP | Treatment Arms | Outcomes |
|---|---|---|---|---|---|
| 1. Hussain, M.H.A. et al., 2007 [144] | Multi-center, Phase II, Non-randomized prospective trial, N = 57 | HER2 overexpressing advanced urothelial carcinoma with no prior chemotherapy for metastasis | Cardiac toxicity | Trastuzumab+ Paclitaxel +Carboplatin +Gemcitabine (TPCG) |
|
| 2. Powles, T. et al., 2016 [145] | Phase III, Double blinded, Randomized, N = 232 | HER1/HER2 expressing metastatic urothelial bladder cancer after first-line chemotherapy for maintenance | PFS | Lapatinib |
|
| 3. Sheng, X. et al., 2021 [146] | Multi-center, Phase II, Single arm, N = 43 | HER2 expressing (2+/3+) locally advanced or metastatic urothelial carcinoma who previously failed at least one line of systemic chemotherapy. | ORR | RC48-ADC |
|
| Clinical Trial | Study Description | Indication | PEP | Treatment Arms | Outcomes |
|---|---|---|---|---|---|
| 1. Ziada, A. et al., 2004 [150] | Single arm, Phase II, N = 18 | HER2 overexpressing advanced hormone refractory prostate cancer | ORR | Trastuzumab |
|
| 2. Lara, P.N., Jr. et al., 2004 [151] | Open label, Phase II, N = 4 | HER2 overexpressing advanced hormone refractory prostate cancer | OS | Trastuzumab or Docetaxel alone followed by Trastuzumab + Docetaxel |
|
| 3. Curigliano, G. et al., 2007 [152] | Phase II, N = 23 | Hormone-refractory prostate cancer. | PSA measurement | Gefitinib + antiandrogen + Luteinizing releasing hormone analogue |
|
| 4. De Bono, J.S. et al., 2007 [153] | Open label, Phase II, N = 23 | Castrate patient with hormone refractory prostate cancer | Prostate-specific antigen (PSA) 50% decline rate within 24 weeks | Pertuzumab at 420 mg vs. 1050 mg |
|
| 5. Agus, D.B. et al., 2007 [154] | Phase II, N = 42 | Castration-resistant prostate cancer (CRPC) patients who had experienced progression after at least one taxane-based regimen. | Safety, ORR | Single agent Pertuzumab |
|
| 6. Vuky, J. et al., 2009 [155] | Phase II, N = 31 | Neoadjuvant therapy in high-risk localized prostate cancer before radical prostatectomy | PCR | Gefitinib + Docetaxel |
|
| 7. Whang, Y.E. et al., 2013 [156] | Multi-center, Phase II, Open label, N = 29 | Rising PSA levels on androgen deprivation therapy and chemotherapy naïve prostate cancer | >50% confirmed PSA decline from baseline | Lapatinib |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amisha, F.; Malik, P.; Saluja, P.; Gautam, N.; Patel, T.H.; Roy, A.M.; Singh, S.R.K.; Malapati, S.J. A Comprehensive Review on the Role of Human Epidermal Growth Factor Receptor 2 (HER2) as a Biomarker in Extra-Mammary and Extra-Gastric Cancers. Onco 2023, 3, 96-124. https://doi.org/10.3390/onco3020008
Amisha F, Malik P, Saluja P, Gautam N, Patel TH, Roy AM, Singh SRK, Malapati SJ. A Comprehensive Review on the Role of Human Epidermal Growth Factor Receptor 2 (HER2) as a Biomarker in Extra-Mammary and Extra-Gastric Cancers. Onco. 2023; 3(2):96-124. https://doi.org/10.3390/onco3020008
Chicago/Turabian StyleAmisha, Fnu, Paras Malik, Prachi Saluja, Nitesh Gautam, Tanvi Harishbhai Patel, Arya Mariam Roy, Sunny R. K. Singh, and Sindhu Janarthanam Malapati. 2023. "A Comprehensive Review on the Role of Human Epidermal Growth Factor Receptor 2 (HER2) as a Biomarker in Extra-Mammary and Extra-Gastric Cancers" Onco 3, no. 2: 96-124. https://doi.org/10.3390/onco3020008