
Designing, Development, and Evaluation of an Informatics Platform for Enhancing Treatment Adherence in Latent Tuberculosis Infection Patients: A Study Protocol

 , , ,
, , , {kind=link}
Abstract
:1. Introduction
2. Current Status of Research Studies
3. Rationale of the Study
4. Aims and Objectives of the Study
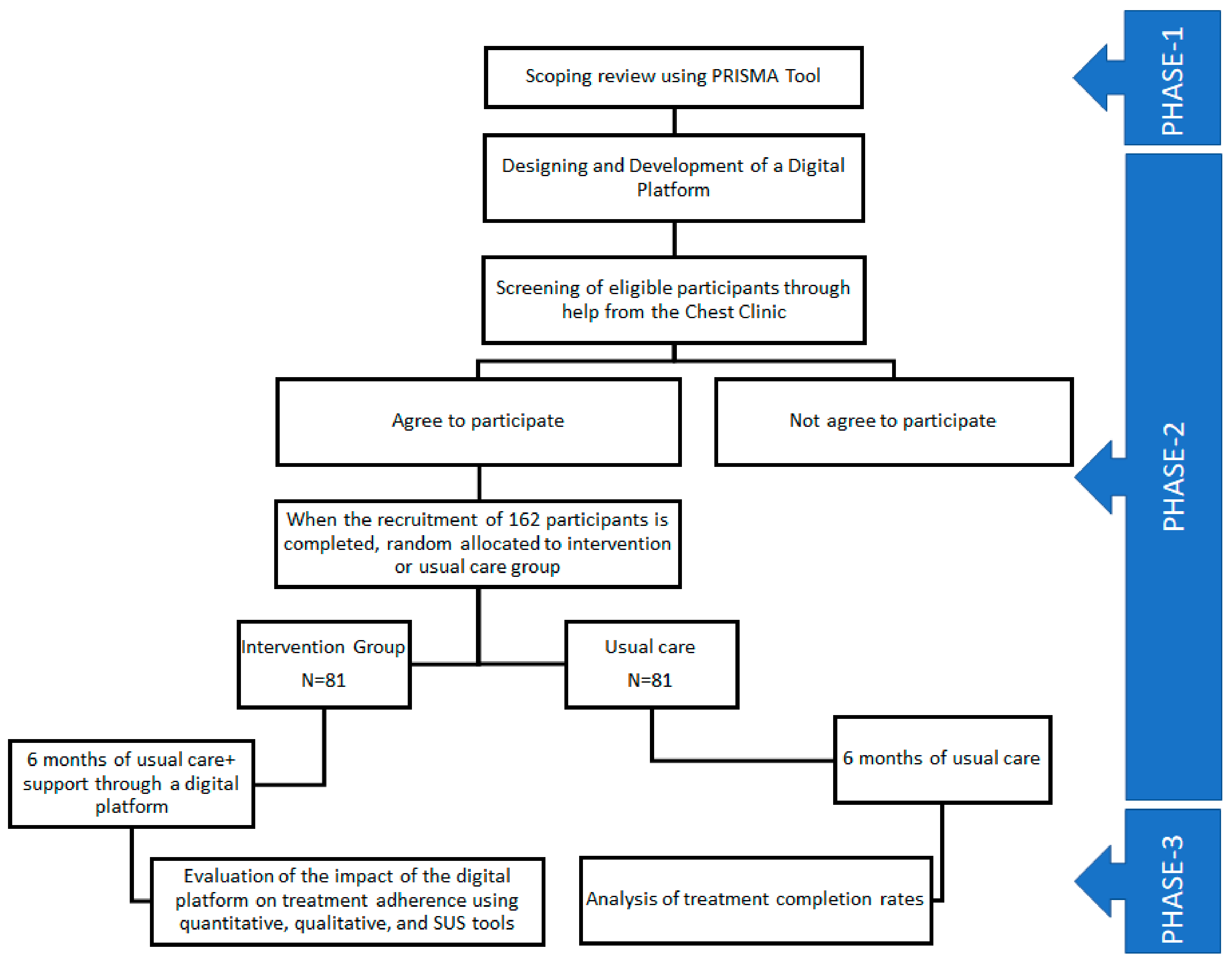
5. Geography, Methodology, and Study Design
5.1. Methodology and Study Design
- Patients who will start LTBI treatment;
- Patients have mobile phones;
- Patients who give written consent and are willing to participate;
- Patients understand Hindi;
- In the case of patients less than 18 years of age, parents are willing to participate.
- Patients who do not have mobile phones;
- Patients who do not understand Hindi;
- Patients are not willing to sign a consent form;
- Patients suffering from active tuberculosis.
5.2. Materials
5.3. Target Population and Sample Size
5.4. Data Analysis and Results
5.5. Outcome Measures
5.6. Data Confidentiality and Privacy
5.7. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Lillebaek, T.; Dirksen, A.; Baess, I.; Strunge, B.; Thomsen, V.Ø.; Andersen, Å.B. Molecular Evidence of Endogenous Reactivation of Mycobacterium Tuberculosis after 33 Years of Latent Infection. J. Infect. Dis. 2002, 185, 401–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization; the Ministry of Health of the Russian Federation. First WHO Global Ministerial Conference on Ending TB in the Sustainable Development Era: A Multisectoral Response in Moscow Declaration to End TB; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Houben, R.M.G.J.; Dodd, P.J. The Global Burden of Latent Tuberculosis Infection: A Re-Estimation Using Mathematical Modelling. PLoS Med. 2016, 13, e1002152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Zhu, T.; Wang, Z.; Peng, H.; Kong, W.; Zhou, Y.; Shao, Y.; Zhu, L.; Lu, W. High Latent TB Infection Rate and Associated Risk Factors in the Eastern China of Low TB Incidence. PLoS ONE 2015, 10, e0141511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, P.; Lebina, L.; Motsomi, K.; Bosch, Z.; Milovanovic, M.; Ratsela, A.; Lala, S.; Variava, E.; Golub, J.E.; Webb, E.L.; et al. Prevalence and Risk Factors for Latent Tuberculosis Infection among Household Contacts of Index Cases in Two South African Provinces: Analysis of Baseline Data from a Cluster-Randomised Trial. PLoS ONE 2020, 15, e0230376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.J.; Lee, S.H.; Kim, Y.E.; Cho, Y.J.; Jeong, Y.Y.; Kim, H.C.; Lee, J.D.; Kim, J.R.; Hwang, Y.S.; Kim, H.J.; et al. Risk Factors for Latent Tuberculosis Infection in Close Contacts of Active Tuberculosis Patients in South Korea: A Prospective Cohort Study. BMC Infect. Dis. 2014, 14, 566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lester, R.; Park, J.J.; Bolten, L.M.; Enjetti, A.; Johnston, J.C.; Schwartzman, K.; Tilahun, B.; Delft, A. von. Mobile Phone Short Message Service for Adherence Support and Care of Patients with Tuberculosis Infection: Evidence and Opportunity. J. Clin. Tuberc. Other Mycobact. Dis. 2019, 16, 100108. [Google Scholar] [CrossRef] [PubMed]
- HIMSS. HIMSS Defines Digital Health for the Global Healthcare Industry|HIMSS. Available online: https://www.himss.org/news/himss-defines-digital-health-global-healthcare-industry (accessed on 11 December 2022).
- World Health Organization. Monitoring and Evaluating Digital Health Interventions: A Practical Guide to Conducting Research and Assessment; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- International Telecommunication Union. ICT Facts and Figure: The World in 2015; International Telecommunication Union: Geneva, Switzerland, 2015. [Google Scholar]
- GSMA Intelligence. Global Mobile Trends; GSMA Intelligence: London, UK, 2016. [Google Scholar]
- Falzon, D.; Raviglione, M. The Internet of Things to Come: Digital Technologies and the End TB Strategy. BMJ Glob. Health 2016, 1, e000038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Handbook for the Use of Digital Technologies to Support Tuberculosis Medication Adherence; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Lam, C.K.; McGinnis Pilote, K.; Haque, A.; Burzynski, J.; Chuck, C.; Macaraig, M. Using Video Technology to Increase Treatment Completion for Patients with Latent Tuberculosis Infection on 3-Month Isoniazid and Rifapentine: An Implementation Study. J. Med. Internet Res. 2018, 20, e287. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Raviglione, M.C.; Flahault, A. Use of Digital Technology to Enhance Tuberculosis Control: Scoping Review. J. Med. Internet Res. 2020, 22, e15727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, J.C.; van der Kop, M.L.; Smillie, K.; Ogilvie, G.; Marra, F.; Sadatsafavi, M.; Romanowski, K.; Budd, M.A.; Hajek, J.; Cook, V.; et al. The Effect of Text Messaging on Latent Tuberculosis Treatment Adherence: A Randomised Controlled Trial. Eur. Respir. J. 2018, 51, 1701488. [Google Scholar] [CrossRef] [PubMed]
- Naraghi, S.; Mutsvangwa, T.; Goliath, R.; Rangaka, M.X.; Douglas, T.S. Mobile Phone-Based Evaluation of Latent Tuberculosis Infection: Proof of Concept for an Integrated Image Capture and Analysis System. Comput. Biol. Med. 2018, 98, 76–84. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. Mobile Cellular Subscriptions (per 100 People)|Data. Available online: https://data.worldbank.org/indicator/IT.CEL.SETS.P2?end=2019&start=1960 (accessed on 9 January 2023).
- The World Bank. Individuals Using the Internet (% of Population)|Data. Available online: https://data.worldbank.org/indicator/IT.NET.USER.ZS (accessed on 11 December 2023).
- Holzschuh, E.L.; Province, S.; Johnson, K.; Walls, C.; Shemwell, C.; Martin, G.; Showalter, A.; Dunlay, J.; Conyers, A.; Griffin, P.; et al. Use of Video Directly Observed Therapy for Treatment of Latent Tuberculosis Infection—Johnson County, Kansas, 2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 387–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Kop, M.L.; Memetovic, J.; Patel, A.; Marra, F.; Sadatsafavi, M.; Hajek, J.; Smillie, K.; Thabane, L.; Taylor, D.; Johnston, J.; et al. The Effect of Weekly Text-Message Communication on Treatment Completion among Patients with Latent Tuberculosis Infection: Study Protocol for a Randomised Controlled Trial (WelTel LTBI). BMJ Open 2014, 4, e004362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, N.; Basu, S.; Chopra, K.K. Achieving TB Elimination in India: The Role of Latent TB Management. Indian J. Tuberc. 2019, 66, 30–33. [Google Scholar] [CrossRef] [PubMed]
- STATISTA. India: Mobile Internet Users. Available online: https://www.statista.com/statistics/558610/number-of-mobile-internet-user-in-india/ (accessed on 11 December 2022).
- Subbaraman, R.; de Mondesert, L.; Musiimenta, A.; Pai, M.; Mayer, K.H.; Thomas, B.E.; Haberer, J. Digital Adherence Technologies for the Management of Tuberculosis Therapy: Mapping the Landscape and Research Priorities. BMJ Glob. Health 2018, 3, e001018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government of India, C.T.D. National Strategic Plan 2017–2025 for TB Elimination in India: Central TB Division. Available online: https://tbcindia.gov.in/index1.php?lang=1&level=2&sublinkid=5450&lid=3266 (accessed on 10 December 2022).
- Government of India, C.T.D. Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India: Central TB Division. Available online: https://tbcindia.gov.in/showfile.php?lid=3625 (accessed on 10 December 2022).
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.; Godfrey, C.; McInerney, P.; Soares, C.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews; The Joanna Briggs Institute: Adelaide, SA, Australia, 2015. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, R.; Singhal, M.; Kumar, D.; Joshi, A.; Islam, K.M. Designing, Development, and Evaluation of an Informatics Platform for Enhancing Treatment Adherence in Latent Tuberculosis Infection Patients: A Study Protocol. BioMedInformatics 2023, 3, 252-259. https://doi.org/10.3390/biomedinformatics3010016
Kumar R, Singhal M, Kumar D, Joshi A, Islam KM. Designing, Development, and Evaluation of an Informatics Platform for Enhancing Treatment Adherence in Latent Tuberculosis Infection Patients: A Study Protocol. BioMedInformatics. 2023; 3(1):252-259. https://doi.org/10.3390/biomedinformatics3010016
Chicago/Turabian StyleKumar, Rohitashwa, Manmohan Singhal, Devendra Kumar, Ashish Joshi, and KM Monirul Islam. 2023. "Designing, Development, and Evaluation of an Informatics Platform for Enhancing Treatment Adherence in Latent Tuberculosis Infection Patients: A Study Protocol" BioMedInformatics 3, no. 1: 252-259. https://doi.org/10.3390/biomedinformatics3010016