
Use of Overground Supported-Stepping Devices for Non-Ambulant Children, Adolescents, and Adults with Cerebral Palsy: A Scoping Review

1
Occupational Science and Occupational Therapy, Faculty of Medicine, University of British Columbia, Vancouver, BC V6T 2B5, Canada
2
Montgomery County Infants & Toddlers Program, Rockville, MD 20825, USA
*
Author to whom correspondence should be addressed.
Disabilities 2023, 3(2), 165-195; https://doi.org/10.3390/disabilities3020012
Submission received: 31 January 2023
/
Revised: 27 February 2023
/
Accepted: 20 March 2023
/
Published: 28 March 2023
Abstract
:Individuals with cerebral palsy functioning at Gross Motor Function Classification System (GMFCS) levels IV and V are unable to use hand-held walkers and require supported-stepping devices with trunk and pelvic support to allow overground stepping in natural environments. This scoping review explored what is known about the use of supported-stepping devices with individuals functioning at GMFCS IV or V. Comprehensive database and hand searches were completed in December 2022. Of 225 unique citations, 68 met the inclusion criteria: 10 syntheses and 58 primary studies including randomized, non-randomized, qualitative, observational and case study designs. Primary studies included 705 unique individuals functioning at GMFCS IV or V, aged 9 months to 47.7 years, while surveys and qualitative studies included 632 therapists. No new experimental studies have been published since previous reviews, however, lived experience and descriptive data suggest that upright positioning and mobility in supported-stepping devices have psycho-social significance with positive impacts on individual self-esteem and autonomy, as well as influencing the perception of others. Improved head and trunk control, use of hands, stepping and independent mobility may promote fitness, functioning, fun, friends, family and future, although environmental and physical challenges may limit use in adolescence and adulthood. Further research on all aspects of supported-stepping device use with individuals at GMFCS IV/V is warranted.

1. Introduction
Cerebral palsy (CP) is the most common cause of life-long disability and is diagnosed based on clinical symptoms. All individuals presenting with non-degenerative disorders of posture and movement due to disturbances in the fetal or infant brain fall under the umbrella definition of CP [1], with genetic and other diagnoses included [2]. The Gross Motor Function Classification System (GMFCS) classifies those with CP according to their mobility function and need for assistive devices in different age groups. School-aged children functioning at level I walk without aids as their primary method of community mobility, while those functioning at level V have very limited abilities to maintain or change position independently. They may achieve independent mobility in some environments using power mobility with complex adaptations [3,4].
Children, adolescents, and adults functioning at GMFCS IV and V are considered non-ambulant as they are primarily dependent on wheeled mobility (with or without physical or powered assistance) [4]. They are more likely to experience secondary musculoskeletal impairments, pain, and functional limitations [5], and young adults functioning at GMFCS IV and V spend most of their day in lying and sitting positions [6].
Asymmetrical lying and inability to change position is associated with windswept hips and scoliosis [7,8]. The need to reduce sedentary behavior in individuals with CP is increasingly recommended, but engaging in physical activity is challenging for those who are non-ambulant [9]. Individuals functioning at GMFCS V may receive the fewest evidence-based interventions [10]. In this paper, the phrase ‘individuals/those/children at GMFCS IV/V’ refers to individuals with CP functioning or classified at GMFCS IV/V.
The Prechtl General Movement Assessment Motor Optimality Score and the Hammersmith Infant Neurological Exam can be used to identify children at greatest risk of being classified at GMFCS IV or V within the first 12 months of life [11,12]. Early identification can help target management and intervention strategies appropriately. Early upright positioning and mobility experiences increase children’s activity and participation, and promote overall cognitive and social development [13]. Increasing opportunities for position change and movement throughout the day may facilitate adaptive behavior and help prevent secondary impairments such as contractures, thus enhancing motor function for children with non-ambulant CP [5].
Supported-stepping devices (referred to hereafter as SSDs or stepping devices) may be used by those with non-ambulant CP to promote active movement and mobility. They are most commonly used by children, but some non-ambulant adults have been reported to use gait aids [14]. Stepping devices provide trunk and pelvic support in an upright position and are individually prescribed for use in typical home and community settings for ‘walking’ or stepping. They are transportable (at least in a mini-van) and this distinguishes them from institutional-type devices that are designed for use in a therapy setting by multiple individuals. Stepping devices are also known as gait trainers or support walkers and are affordances for active, overground supported stepping. The term supported-stepping device is now preferred over gait trainer, since they are not used to ‘train gait’ for individuals at GMFCS IV/V. Those with non-ambulant CP are not expected to progress to independent walking without the device. The term ‘support walker’ also implies that individuals use the device for walking, while active upright positioning and stepping may be a more accurate description for many users.
The first systematic review of supported-stepping device outcomes [15] included children up to 18 years of age with any type of disability. Outcomes were divided by International Classification of Functioning, Disability and Health (ICF) categories of body structure and function (BSF), activity, and participation [16]. Several positive findings were reported, including statistically significant impact on mobility level and bowel function and an association between increased intervention time and bone mineral density. Descriptive evidence supported a positive impact on activity (primarily stepping) and participation with others [15]. Most participants were classified as GMFCS III or IV, while only two studies specifically identified some participants as GMFCS V [17,18]. Children at GMFCS III typically use stepping devices at younger ages and progress to using hand-held posterior walkers by school age [19].
The purpose of this scoping review is to describe the outcomes and use of supported-stepping devices for individuals with non-ambulant CP. A scoping methodology was chosen [20,21,22], and the search expanded to include all ages, grey literature, supporting evidence, reviews and expert opinion as well as any qualitative or quantitative studies.
The overall question is:
What is known about the use of supported-stepping devices with children, adolescents or adults with CP and classified at GMFCS IV or V?
Sub-questions articulate the scope of the enquiry as follows:
- What BSF, activity, and participation outcomes from supported-stepping device use have been reported?;
- Are there any data available regarding: rates of use; costs; abandonment; adverse effects; contraindications; or equipment type in relation to age, desired outcomes or GMFCS levels?;
- Do experiences of stakeholders differ in regard to supported-stepping device use?;
- What are the barriers and facilitators of supported-stepping device use?
2. Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-SCR) statement was used to structure this review [23]. The protocol was registered on the Open Science Framework on 9 December 2022 and may be retrieved at https://osf.io/s4286/ (accessed on 20 March 2023).
Electronic database searches included EBM Reviews, CINAHL, Medline, Embase, PEDro and Google Scholar and were completed during December 2022. Search terms such as “gait trainer”, “support walker”, “David Hart Walker”, NF-Walker”, “supported stepping”, “supported walking”, “overground gait training” and “locomotor training” were used with population descriptors such as cerebral palsy or spastic quadriplegia. Search terms were created by both authors and modified from the search strategy created with university librarian assistance for the previous systematic review. Google Scholar searches were limited to the first 50 results, otherwise, electronic databases were searched from database inception to December 2022. No limits were placed on age, language, study design or publication status. Electronic database searches were conducted by the first author and reviewed by the second author. See online for Supplementary File S1.
Reference lists of potentially relevant articles were hand-searched for additional studies. All articles included or referenced in a recent scoping review of supported-standing interventions for individuals at GMFCS IV/V [24] were hand-searched, as were reference lists from the previous systematic review of stepping device outcomes [15], and the related papers reviewing device features [19] and outcome measures [25].
Conference proceedings from the last three years were searched to identify unpublished studies, and other researchers. Proceedings included: International Seating Symposium; American Physical Therapy Association Academy of Pediatrics Conference; European Academy of Childhood Disability; American Academy of Cerebral Palsy and Developmental Medicine; and Australasian Academy of Cerebral Palsy and Developmental Medicine. Relevant periodicals were searched for the last three years to identify case reports, clinical descriptions or current expert opinion on use, benefits or challenges of stepping device use with non-ambulant CP. These included: Directions (https://nrrts.org/directions/ accessed on 11 December 2022); Mobility Management (https://mobilitymgmt.com/Home.aspx accessed on 11 December 2022); and Rehab Management (https://rehabpub.com/magazine/ accessed on 11 December 2022).
Known or potential researchers and clinical experts were contacted to identify unpublished studies or relevant grey literature. Further iterative Google and Google scholar searches were conducted to follow up on any potential devices, researchers or research studies identified in the hand and electronic searches, and for articles citing the previous systematic review [15]. Google translate was used to translate articles retrieved in other languages. Both authors reviewed titles and abstracts retrieved in the electronic and hand-searches and agreed those to be reviewed full-text. Both authors read all full-text articles and agreed upon those meeting the inclusion criteria, with any discrepancies resolved through discussion.
2.1. Inclusion Criteria
Studies were included if: at least 50% of participants were reported as being diagnosed with, or meeting clinical criteria for CP [2], and described as GMFCS IV and/or V; or if outcomes or data related to these individuals could be separated. Where this information was unclear in the published article, attempts were made to contact authors. In older studies where GMFCS was not used as a descriptor, spastic quadriplegia or tetraplegia was presumed to imply GMFCS IV/V. Spastic diplegia was presumed to imply GMFCS III, unless descriptions suggested that individuals were functioning at GMFCS IV according to descriptions from the GMFCS Expanded and Revised or Family and Self Report Questionnaire from the website: https://canchild.ca/en/resources/42-gross-motor-function-classification-system-expanded-revised-gmfcs-e-r (accessed on 11 December 2022).
A supported-stepping device is defined as a wheeled ‘walking’ frame or support walker that provides trunk and pelvic support and has a soft strap or solid seat. Stepping devices may provide upper limb support through a tray or arm troughs, or may be hands-free. They may support the individual from behind (posterior) or in front (anterior). Some posterior wheeled walkers that are typically considered hand-held walkers are convertible to a stepping device with the addition of trunk and pelvic supports, a sling seat, and they may also have arm troughs [19].
All study types providing data or recommendations for stepping device use with individuals at GMFCS IV/V were included: reviews, guidelines or opinion; intervention studies from randomized controlled trials to case studies; qualitative or survey studies including parents of individuals at GMFCS IV/V and/or educational staff, medical personnel or physical/occupational therapists having experience using stepping devices; and data describing use, tolerance, benefits or harms of stepping device use with individuals at GMFCS IV and/or V.
2.2. Exclusion Criteria
- Studies including mainly individuals classified as GMFCS I–III or those able to walk independently or use hand-held walkers;
- Studies using robotic devices, exoskeletons or mechanical stepping devices with external power sources, stationary systems (confined to parallel bars or treadmill), ceiling suspension systems or institutional-type gait trainers (e.g., LiteGait) too large to be used in a home or classroom environment;
- Where overground gait or ambulatory training was the comparison intervention, studies were included only if a supported-stepping device was the main comparison and not used in combination with partial body-weight supported treadmill training or other powered intervention(s).
2.3. Data Extraction and Appraisal
Included studies were appraised independently by both reviewers, and extracted data (participants, intervention, and results/findings), study design, themes and findings agreed upon through discussion. Where details were unclear, study authors were contacted for clarification. Study design was defined using Mixed Methods Appraisal Tool (MMAT) [26] criteria. Study quality was appraised for randomized and non-randomized group studies to allow comparison of study conduct. Since lived experience was a focus of this review, quality rating was also completed for qualitative and mixed-method studies. Remaining studies were descriptive and reported in a wide variety of formats, making comparative quality rating inappropriate.
Numbers of unique individual participants classified at GMFCS IV, GMFCS V, and GMFCS IV/V were totaled, without weighing for differences in study type, publication type or study quality. For longitudinal studies where the same population was measured more than once, only numbers from the original or largest n report were included in these calculations. Only those using a stepping device were counted in comparative group studies or in studies where only some individuals used a stepping device. Outcomes of stepping device use were grouped according to the ICF categories of BSF, activity, and participation. The number of therapists reporting agreement in surveys plus the number of expert opinion authors agreeing were totaled for each outcome. The number of unique non-ambulant participants reported for each outcome was totaled, with outcomes reported from a large clinical/commercial dataset counted separately so as not to skew findings.
The F-words [27] have expanded our understanding of the ICF and how these concepts apply to childhood development. Findings from lived experience and descriptive data were classified according to the F-words to allow for a deeper analysis of environmental factors from the family perspective and a consideration of Future which is not specifically included in the ICF. Fitness relates to the ICF component of BSF. Functioning is closely aligned to the ICF component of activity and Friends is related to the ICF component of participation. Fun is related to the ICF concept of personal factors and also participation, while Family represents the major environmental factor influencing the development of children [27].
In this analysis, inclusion in school or preschool activities, being eye-to-eye with peers, a sense of belonging, and social interaction, were considered to relate to Friends. Parent satisfaction with devices and services, the impact of interventions on family and other environmental factors such as the supports and attitudes of caregivers, schools, and therapists were included under Family. Future included interventions designed to impact future functioning, health, and well-being [28].
3. Results
Database searches yielded 698 citations and a further 48 citations were identified through hand searching. Once duplicates were removed, 225 citations remained. Following title and abstract review, 89 full-text articles were retrieved. Following a full-text review, 68 articles met the inclusion criteria and 21 records were removed for the following reasons: not retrieved [29,30,31]; not GMFCS IV/V [32,33,34,35,36,37,38]; not a stepping device or not a stepping device only [39,40,41,42,43,44,45,46,47]; no data [48]; and duplicate data to included study [49]. See Figure 1.
Included in this scoping review were: 10 syntheses [15,19,25,51,52,53,54,55,56,57]; 1 randomized controlled trial [58]; 2 non-randomized comparison group studies [17,59]; 4 pre-post single group studies [18,60,61,62]; 3 qualitative [63,64,65] and one mixed-methods study [66]; 2 single-subject research design multiple baseline designs [67,68]; 6 single-subject research design intervention-withdrawal (ABAB) designs [69,70,71,72,73,74]; 11 case-series or observational studies [75,76,77,78,79,80,81,82,83,84,85] and an unpublished longitudinal report [86] from a clinical/commercial dataset provided by the author (personal communication, Idoia Gandarias Mendieta, 16 January 2023); 4 surveys [14,87,88,89]; 12 single case studies [90,91,92,93,94,95,96,97,98,99,100,101]; and 6 multiple case studies [102,103,104,105,106,107]. One multiple case study [103] and 5 additional articles [108,109,110,111,112] provided expert opinion on the use and benefits of stepping devices with GMFCS IV and/or V.
3.1. Syntheses and Guidelines
Syntheses of evidence related to stepping device use included two clinical guidelines [55,56], an overview of intervention efficacy [53], a systematic review and meta-analysis of functional gait training interventions [52] and a scoping review of early interventions [57]. Other than a review completed as part of an undergraduate degree in Germany [51], remaining reviews were previously completed by both authors [15,19,25,54]. See Table 1 for details. Syntheses are listed chronologically, identified by first author and reference number.
Apart from the thesis, syntheses authors declared any conflict of interest, and studies were either unfunded or funded by independent grants with no input on study design, conduct or reporting. No synthesis reported funding for their included studies. Where conflict of interest or funding were reported for primary studies, these are noted in Table 2. In one study [60], the device distributor had input into study design and conduct. Three descriptive articles [77,86,110] were written and provided by the device distributor.
3.2. Primary Source Data
Of 17 studies included in the 2015 systematic review, 16 met the inclusion criteria for this review [17,18,58,59,61,64,67,69,70,71,72,73,74,75,93,101]. The strongest research design studies continue to be the previously included randomized [58] and non-randomized-group designs [17,59]. No new experimental studies were identified. Methodological quality for all comparative [17,58,59] or single group [18,60,61,62] intervention designs and qualitative or mixed method studies [63,64,65,66] was moderate (3/5) or high (4 or 5/5). See online Supplementary File S2 for quality rating details. Although seven [67,69,70,71,72,73,74] of the eight single-subject research design studies meeting the inclusion criteria for this review were included in the 2015 systematic review [15], information on three adults was added from previously included ABAB studies [71,74], and an additional multiple-baseline design [68] including an adult and a child were added in this review.
3.2.1. Sources of Evidence According to Supported-Stepping Device (SSD) Type
Studies related to the David Hart or NF-walker® (hereafter referred to as a hands-free orthotic stepping device) were the most numerous of any specifically identified stepping device, and may speak to grant funding availability. The non-randomized two-group design [17], pre-post [18,61], and qualitative [64] studies were cited in the previous systematic review [15]. Additional studies included: a pre-post study [60] from Switzerland; a conference paper [77]; a dataset describing hands-free orthotic stepping device use in Spain between 2010 and 2022 [86]; a longitudinal study by independent researchers with a small sub-set of children from this dataset [81,82]; a mixed-methods study from Finland [66]; a protocol for selection of device candidates [76]; and three case reports [103,105,106].
Mobility Opportunities Via Education (MOVE®) traditionally involves the use of an anterior or front-leaning stepping device with arm support for non-ambulant children. In addition to the non-randomized two-group study [59], multiple baseline design [67], and the single case report [101] cited in the previous systematic review, two observational group studies [79,83] described in conference abstracts and three case reports [97,104,107] were added.
Remaining studies included use of various stepping device types. Two recent qualitative studies explored stakeholder experiences [63,65] while two surveys explored therapist impressions, one from the UK [87] and one from the US [88]. Stepping device use data was provided by two other surveys [14,89]. A new pre-post pilot study examined the effect of short-term intensive power training during physical education on walking speed, distance, and heart rate [62]. Previously reviewed case series [75] and single case reports [93,101] were supplemented by case reports identified from reference [92,94,98,99] and periodical searches [90,100]. Expert opinion on use of stepping devices was found in two other periodicals [109,111]. Five book chapters [91,95,102,108,112] contained either case studies or recommendations specific to stepping device use with GMFCS IV/V.
3.2.2. Use and Introduction of Supported-Stepping Devices (SSD) According to Age and GMFCS
Studies reported or examined the use of stepping devices with 235 individuals classified at GMFCS IV, 288 at GMFCS V, and 182 identified as either IV or V. A significant proportion (105 at GMFCS IV and 180 at GMFCS V) are from the Spanish dataset [86] that includes participants from other citations [77,81,82]. In addition, 632 therapists with experience using stepping devices with those classified at GMFCS IV and V participated in survey and qualitative studies. The most common stepping device use pattern reported was 30–60 min, 5–7 days a week, with a range from 10 min to 4 h daily. Survey and longitudinal studies suggest that the average duration of use may be 5–7 years, but it ranges from 6 months to >10 years.
Excluding the unpublished dataset [86], individuals classified as GMFCS IV ranged from 9 months to 22 years, while those at GMFCS V ranged from 9 months to 17 years with an average age around 7 years. Those classified only as IV/V ranged in age from 3 years to 47.7 years. When the adult ages were removed (four aged 19.2, 34, 42.2 and 47.2 years), the average age was around 9 years. The 122 current users in Spain are 2 years to 34 years old, with an average age of 13 years. Of 47 adults, 9 began using their hands-free orthotic stepping device over 18 years of age, while 36/285 continued use into adulthood [86].
Therapist recommendations for age of introduction range from 9 months to 2 years. Two recent studies from the UK [63,87] highlight a divide between therapists who support early stepping device use to promote stepping and participation, and those who wait until it is clear that the child will not be able to walk any other way, fearing that stepping device use will increase independence at the cost of typical movement patterns. No clear trends were identified regarding stepping device type or orientation in relation to age or GMFCS level. No differences in use or introduction were identified in relation to specific outcomes.
3.2.3. Contraindications and Benefits of Supported-Stepping Device (SSD) Use
Studies were primarily observational or descriptive, and few harms were reported. Contraindications included pain, lack of head control (that cannot be addressed with head or neck support), flexor withdrawal response to weight on the feet, behavioral issues, lack of caregiver support and significant lower limb contractures (orthotic stepping devices only). Benefits reported include increases in physical health, physical activity, stepping ability, motivation, participation, emotional well-being and self-esteem. See Table 2 for details. Studies are organized in alphabetical order by first author within study design groups. Publication source is noted, as well as conflict of interest and funding, if reported.
3.3. Expert Opinion
Expert opinion results support the introduction of stepping devices between 1 and 2 years of age to promote upright positioning, self-esteem, physical activity, physical development and social inclusion for children at GMFCS IV/V. Decreasing sedentary behavior and promoting play, participation, and independent mobility may be more important than typical gait patterns for this population. See Table 3.
3.4. BSF, Activity and Participation Outcomes
Outcomes were divided according to ICF categories of BSF, activity and participation. Increased stepping, walking speed, distance or mobility was reported for the greatest number of individuals (303). In addition, (a) hand-use, (b) maintaining head control or standing positions (c) motivation, happiness, confidence and self-esteem and (d) participation with peers were reported for 118, 89, 67 and 76 individuals, respectively. See Figure 2a. An additional 285 individuals were reported to have improved head and trunk control, and increased self-esteem, while 245/285 were able to take steps in the stepping device with or without assistance [86].
3.5. Lived Experience of Supported-Stepping Device (SSD) Use
For studies reporting qualitative data from parents and caregivers [64,65,66,104], findings were reported according to the F-words for childhood development [27]. See Figure 3. Under the F-words analysis, there are some differences in how findings were classified in comparison with the ICF analysis. Impacts on individual self-esteem and autonomy and impacts on societal or others’ attitudes were included under Future, as these factors may influence future opportunities and individual potential along with influences on physical health and overall development. Happiness, enjoyment and motivation were included under Fun which combines aspects of personal factors and participation.
4. Discussion
In the eight years since the original systematic review [15], little has been published specifically investigating stepping device interventions. In order to explore the topic in-depth, we sought out case studies, descriptive and grey literature for all ages and confirmed that successful use of stepping devices has been reported for over 700 individuals classified at GMFCS IV and V across a wide range of countries. This finding suggests that stepping device use is feasible for individuals with non-ambulant CP and may be considered standard-of-care in some settings.
4.1. Outcomes and Use of Supported-Stepping Devices (SSD)
Families, caregivers and therapists reported benefits on all components of the ICF and influencing all F-words for those classified as GMFCS V as well as GMFCS IV. Benefits were also reported for those with limited abilities to step without assistance. Introduction was demonstrated to be feasible from 9 months, in line with the call for provision of developmentally appropriate ‘ON-Time’ mobility [117]. Although challenges were reported in adolescence with increasing size, changed physical abilities and difficulties with transfers, this review identified at least 80 adults aged 18–47.7 years who used stepping devices. Since evidence continues to be primarily descriptive, conclusions as to efficacy of stepping device interventions are unchanged from the previous systematic review [15]. The remainder of the discussion is structured according to study aims; followed by clinical practice suggestions; and research recommendations based on the significant evidence gaps identified.
4.1.1. Use of Supported-Stepping Devices (SSD) for BSF, Activity, and Participation Outcomes
One included study measured a trend towards increased bone mineral density for children who spent more time weight-bearing in either a stander or a stepping device [17]. In a review of supported standing interventions for individuals at GMFCS IV/V, the strongest evidence was found for impact on bone mineral density and prevention of contractures [24]. In children with CP, differences in muscle are seen starting as early as 12–15 months when compared with children who are typically developing [118], and bone mineral density is lower in those who are non-ambulant [119]. Although no included studies examined impact on muscle length, prevention of contractures or hip stability, the benefits of stepping device use for these outcomes were reported by both therapists and parents. Early introduction of weight-bearing and promotion of upright positioning and supported stepping through adolescence into adulthood may help maintain muscle and prevent premature ageing and loss of mobility, as has been proposed for individuals with ambulant CP [120]. Parents and therapists reported benefits for bowel function following the use of stepping devices in qualitative, descriptive and survey studies, but only one study [17] measured decreased constipation for children using stepping devices in comparison to those using standers.
Physical fitness was the most highly reported benefit in the expert opinion analysis, but, until recently, no studies had examined this outcome. A small pilot study [62] measured statistically significant positive change in cardio-vascular exercise response, walking speed and distance following short-term intensive school-based physical training for children at GMFCS III and IV. Separate analysis of results for those classified as GMFCS IV only also revealed positive change, although this was greater across all measures for the younger children. The 10–11-year-old children showed minimal improvement or stable response to walking speed tests and heart rate measurement, although they were able to walk further at a self-selected walking speed on the 6-min walking endurance test. These preliminary results support use of stepping devices to increase physical fitness for children at GMFCS IV when incorporated into age-appropriate and meaningful sports activities with peers.
As in the systematic review, increased stepping, walking speed, distance or independent mobility outcomes, classified within the ICF domain of Activity, continue to be reported most frequently and were noted for 588/705 individuals in this review. However, improved head and trunk control, ability to maintain position, increased arm and hand use, improved transfers and participation in activities of daily living outcomes were also reported for large numbers of individuals across different study and report types. Although increased mobility was the primary reason for therapists prescribing a stepping device in one survey [88], physical fitness and participation outcomes may be as, or more, important.
A guideline [56], likewise, recommends that stepping devices should be used for inclusion and physical well-being rather than functional mobility for individuals at GMFCS IV/V. Case study results confirm that while children used stepping devices for participation and to reduce sedentary behavior, they relied on power wheelchairs for functional mobility and to keep up with peers over longer distances [90,91,95]. Mobility experience in stepping devices and power mobility may have reciprocal benefits. Stepping device use was not reduced, and even increased for some, following power mobility introduction in a group of young children [78]. In another study, a parent reported the benefits of increased spatial understanding from stepping device use, as it increased their child’s success with power mobility [61].
In the systematic review, increased social function and improved participation were reported in only one study reporting qualitative [64] and quantitative results [61]. In contrast, increased peer participation was reported for 97 individuals across the wider range of studies in this review. In addition, therapists indicated that the use of stepping devices increased family and peer participation and enhanced child autonomy, engagement, initiation, inclusion and sense of belonging. They reported an impact on these items at a similar rate to the impact on stepping, contrasting with the focus on mobility outcomes in intervention studies.
4.1.2. Use of Supported-Stepping Devices (SSD) According to GMFCS Level
Little has been published regarding options to increase physical activity and decrease sedentary behavior for individuals at GMFCS V [55,56,121,122]. However, although the majority of studies in this review demonstrated that individuals at GMFCS IV can achieve independent indoor and possibly outdoor mobility in stepping devices, some at GMFCS V were also able to walk more than short distances, at least on level surfaces [60,67,76,103]. Other studies suggested that there are physical health benefits from the upright positioning and active movement opportunities. These, along with psycho-social benefits and enhancement of inclusion and participation opportunities, were reported for individuals at GMFCS V who had more limited independent stepping abilities [77,85,100,102,105].
Although no clear trends were identified in regard to GMFCS, some recommendations were made in hands-free orthotic stepping device studies. Two studies reported that individuals at GMFCS V were the typical users [81,105]. These studies include participants from the clinical/commercial dataset [86], reporting a total of 180 individuals at GMFCS V and 105 at GMFCS IV. A protocol recommends both GMFCS IV and V and suggests that cognitive and social developmental level may influence stepping [76]. Another report on a subset of 137 users from the Spanish dataset suggests that this stepping device is not beneficial for individuals at GMFCS III who may be more functional in less supportive stepping devices at younger ages and transition to posterior hand-held walkers by school-age [77]. However, the longitudinal study from Canada [61] suggests that a number of children classified as GMFCS IV/V on study entry benefitted from the stepping device to develop trunk and upper limb control. These children (who used the stepping device daily for many hours at home, school and in community settings) progressed to using posterior hand-held walkers and were subsequently classified as GMFCS III (personal communication, Virginia Wright, 5 January 2023).
4.1.3. Use of Supported-Stepping Devices (SSD) in Relation to Equipment Type and Orientation
No clear trends were identified regarding stepping device type or orientation in relation to age, GMFCS or other factors. In the two surveys, anterior arm support style stepping devices were most reported. The 2011 US survey [88] suggests that the Kaye suspension system was also highly prescribed which seems unlikely. Therapists may have been reporting the prevalence of the posterior Kaye walker use rather than the add-on suspension system specifically. The more recent availability of solid seat stepping devices that can be used in either reverse hands-free orientation or anterior support-arms orientation is evident in the UK survey [87]. Posterior hands-free stepping devices were prescribed at a similar rate to the anterior-posterior option in this survey in comparison to the limited use reported in the US 2011 survey. Descriptive results and clinical experience suggest that different use patterns in North America may be identified if a contemporary survey was conducted.
Although no clear trends were identified overall, some different patterns of device use were reported from different locations worldwide. Although a comprehensive longitudinal study on the hands-free orthotic stepping device took place with 20 children in Canada [18,61,64], its ongoing use in North America was very limited, likely due to the funding environment. In contrast, a number of studies were completed in Europe, with the largest dataset reported from Spain [86]. Studies including anterior support-arms stepping devices are more commonly reported in the US, likely influenced by the MOVE® program, although MOVE® studies were also reported in the Netherlands [59] and India [123].
More recent studies from the US report use of hands-free stepping devices with younger children at GMFCS IV and V [80,85,90,95,102], as well as different anterior styles [100]. A descriptive study found that more young children at GMFCS V used hands-free posterior stepping devices in comparison to anterior support-arm styles, while the reverse was true for GMFCS IV [78]. A recent qualitative study from Spain described the physical and psycho-social benefits of a lower-cost charity-provided hands-free walker [65], while the use of hands-free stepping devices within a US special school program was associated with a variety of developmental gains for young children at GMFCS III-V with severe visual and communication disabilities [85].
In India, commercial hands-free stepping devices are generally not available, and one study reported modifying a posterior hand-held walker with the addition of a sling seat and trunk support. This low-cost modification was acceptable to parents and provided opportunities for the children to move hands-free, increasing participation in play and activities of daily living [84]. Stepping device costs, availability and the funding environment vary widely with location influencing opportunities to use different stepping devices. No studies comparing costs or cost-effectiveness were identified in this review.
4.1.4. Stakeholder Experiences of Supported-Stepping Device (SSD) Use
Two surveys of pediatric therapists were completed 10 years apart; the earlier one in the US [88] and the more recent in the UK [87]. US therapists reported that 50% of children using stepping devices progress to independent walking, with 6 months the average duration of use. This suggests that stepping devices were widely used for children with developmental delays and ambulant CP who required more support in early childhood, but went on to use hand-held walkers or to walk independently.
In contrast, UK therapists reported less than 20% of children using stepping devices progressing to hand-held walkers or independent walking. While some therapists believed that early use of stepping devices could facilitate walking progression, others feared that children would learn incorrect patterns. Similarly, UK physiotherapists participating in a qualitative study [63] were divided between prioritizing child function and participation versus quality of movement. Current recommendations suggest that child and family goals for inclusion, participation, engagement and physical well-being should be prioritized over typical gait patterns for those at GMFCS IV/V [56,111,124].
In the UK qualitative study [63], parents of children at GMFCS II–IV focused on the long-term physical and social benefits of walking while children (all GMFCS II/III) prioritized having fun, playing and keeping up with friends when choosing between using their walker or wheelchair. Ambulant children may focus on Fun, Family and Friends while therapists traditionally focus on Fitness, Function and Future [124]. These perspectives have been highlighted in other studies: children see walking as exercise rather than mobility [125], adolescents prioritize safety and efficiency depending on environmental and social demands [126], and children who use mobility aids to facilitate participation in school may prefer floor mobility or assisted mobility at home [127]. These perspectives may differ for children who are unable to move even short distances without assistive devices; however, few studies report views of those at GMFCS IV/V. Since cognitive, developmental and communication difficulties are more prevalent in this group [128], parent-proxy views are more commonly reported, but may differ from the child’s perspective.
Parent satisfaction was evaluated in two included studies [66,84] using the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) [129]. Scores ranged between 4 (satisfied) and 5 (very satisfied). A study-specific satisfaction scale used in a longitudinal pre-post study [18,61] reported similar satisfaction levels.
A longitudinal study from Spain [81,82] used the children’s version of QUEST 2.1 [130], which scores in the opposite direction with 1 representing the highest score and 7 the lowest. This difference in scoring, and the fact that QUEST 2.1 was designed to be more specific to satisfaction with computer technology, makes it challenging to compare parent satisfaction across studies. It is surprising that in the initial study [81], mean parent device satisfaction was 4.29 indicating mixed satisfaction, while in the 10-year follow-up study [82], a mean of 3.12 indicates parents were mostly satisfied, although only one adolescent/young adult out of 19 was still using the hands-free orthotic stepping device.
QUEST 2.0 developers suggest that ratings ≥ 4 represent acceptable satisfaction for mobility devices [131]. Studies exploring parent satisfaction with children’s use of power mobility devices have reported similar ratings [132,133]. However, a survey including parents of mobility device users in Iceland [134] reported that only 57% of wheeled walker users were satisfied or very satisfied with their device features. This difference may relate to ongoing use of a range of assistive devices, in comparison to the relatively recent introduction of a novel device that may have changed the child’s functioning and participation [66,84,132,133]. Continued satisfaction with a stepping device that the child could no longer use [82] may relate to the psycho-social significance of the upright position in society [64,125] and parents’ memories of a time of increased participation for their children.
Parents reported least satisfaction with ease-of-use for a hands-free orthotic stepping device [66]. Difficulty with transfers into this style of stepping device is confirmed by other included studies [17,18], particularly as the child got bigger [61,64,75]. However, one descriptive case study reports a modified transfer method that allowed continued use into adulthood with one caregiver [103].
4.1.5. Barriers and Facilitators of Supported-Stepping Device (SSD) Use
Few harms were discussed in included studies, other than the need to ensure safety and the potential for instability or falls as children’s height increases. Participants in one qualitative study commented on the stability of the stepping device used and that no falls had occurred [65]. Another study reported that two children had tipped over on uneven ground without sustaining injuries and no other harms were reported [18,61]. Transfer difficulties were the most common barriers reported overall. Other commonly reported environmental factors that could be barriers or facilitators were adequate space for use and caregiver support and supervision.
Hip, knee and ankle contractures are contraindications primarily for stepping devices with orthotic components. Increasing deformity and poor health, including contractures, hip subluxation and scoliosis, was the major reason reported for discontinuation of the hands-free orthotic stepping device [82]. In the total cohort of 285, this was also the case with the accompanying loss of ability to step, most commonly around 12–13 years of age [86]. It is not known if this would also hold true for other stepping device types. Setting up a stepping device for those with body structure or alignment differences, without increasing deformity or causing pain, may be influenced by the adjustability of the stepping device, the availability of accessories and therapist expertise. The value of the stepping device in promoting inclusion and engagement in meaningful and age-appropriate activities may also influence continued use into adolescence and adulthood.
Case series [80] and reports [96] suggest that transfers into, and stepping with anterior style stepping devices may be easier for older children. However, a variety of stepping device models have lift assistance built in and transfer aids are often used for older children. The anterior or front-leaning positioning may facilitate stepping for some children [114] and was recommended within the MOVE® program that started with the inclusion of older children who had not been given the opportunity to move at younger ages [107]. However, angled forward positioning to facilitate stepping can also be achieved with hands-free stepping devices [135].
Outgrowing the stepping device was reported as the primary reason for discontinuation or changing to another stepping device style by parents who were motivated to continue using it with their adolescent child [64]. As the child grows taller, the device needs to be significantly wider in order to remain stable, and safety concerns at older ages have been reported [64]. Larger models suitable for adolescents and adults have been developed for some stepping devices, but they are used much less than those for younger children. The increasing width may prevent them from fitting through standard doorways, and transportation difficulties may limit use in different settings.
The recent pilot study [62] combined games activities, e.g., basketball with high intensity interval training including short bursts of speed with and without increased weight. The incorporation of the training within a supportive school setting, along with other children who had similar abilities likely contributed to the high level of adherence achieved in this study. This emphasizes the importance of inclusion and participation in meaningful and age-appropriate activities with peers as a facilitator of stepping device use in children and young people with non-ambulant CP.
4.2. Recommendations for Clinical Practice
There is still limited research that clinicians can use for clinical decision making around stepping device prescription and training. No clear trends were identified in regard to stepping device prescription and use in regard to age, GMFCS level or outcomes, and device selection may be highly influenced by availability, funding and support for use of different devices in different locations. Individualized assessment and prescription are therefore essential, and detailed case studies and single-subject research designs would add to the literature. Prescription of individual stepping devices should take into account multiple factors, including: need for postural support; positioning and support needed to allow stepping; type of transfer and equipment or support required for transfers; space for use; context and environment where the device will be used e.g., indoors or outdoors; transportation; caregiver support; and opportunities for participation and inclusion with others.
The Gross Motor Function Measure (GMFM-88) [136] has been used in research to measure the significant difference in standing or walking function, with and without the stepping device [18,61], and it may be helpful for clinicians to demonstrate the impact of a stepping device to funders or providers. The Top-Down Motor Milestone Test [137] has no composite or summary score [123], and individuals may make progress on several sub-items without changing independence level. One study modified scoring to achieve a summary score [59], but this did not account for changes in sub-items. As a result, this measure may be helpful for clinicians to record individual progress in independence within functional tasks, both with and without the stepping device, but is less suited for analyzing change in group intervention studies. Individualized goal setting measures such as the Canadian Occupational Performance Measure [138] may also be useful in clinical practice for identifying meaningful goals and measuring change for individual children.
Goals varied according to GMFCS level in a recent study investigating outcomes of intensive robotic-assisted gait training. Parents of children at GMFCS III set functional mobility goals such as increasing walking speed, distance and stepping pattern, while parents of children at GMFCS IV and V set goals focused on increased independence, physical activity within the stepping device, participation in dressing and increased weight-bearing during transfers [45]. This suggests that, for individuals at GMFCS IV and V, therapists should focus on outcomes that extend beyond mobility and stepping, and even beyond activities occurring while in the stepping device.
4.3. Recommendations for Future Research
Studies on all aspects of stepping device use, benefits, and development are warranted, as evidence to date is primarily descriptive and there are significant evidence gaps in every area. Accurate classification of GMFCS level is essential for future experimental studies. While GMFCS has been shown to be stable [128], there are challenges at younger ages and reclassification after age 2 years is recommended [139]. Children at GMFCS II-IV are more likely to have their level overestimated under 6 years, leading to reclassification to a lower functional level at older ages [140]. GMFCS is a continuum and children should be classified based on usual function rather than on capacity [3]; however, GMFM-66 centiles [141] may assist in classifying, particularly younger children, more accurately for research purposes. The GMFM-88 can be scored with the child using assistive devices [136] but, as yet, centiles are not available for this measure.
Using a stepping device to break up long periods spent in sitting and lying positions reduces sedentary behavior. This may impact BSF or Fitness (including hip stability), as with other postural management interventions [54], and positively influence the sleep-wake cycle [122], outcomes that have yet to be measured in experimental studies. Improvements in bowel function have only been measured in one comparative group study, and further studies are warranted. Further studies investigating exercise response to use of stepping devices with individuals at both GMFCS IV and V are also needed. The recent pilot study suggests that inclusion in sports activities with a comparable peer group may be a significant facilitator of stepping device use to increase physical activity [62] and this merits further exploration both qualitatively and quantitatively. Interventions to help prevent musculoskeletal impairments and influence societal perspectives also fall under the F-word of Future [28]. A stepping device may help to increase activity or functioning in areas such as stepping and mobility, transfers and activities of daily living, or improving head, trunk, and upper limb control. Stepping devices may also impact participation and engagement or Friends. Each of these outcomes of a stepping device intervention require different types of outcome measures.
Outcome measures suited for individuals at GMFCS IV/V to measure stepping device outcomes continue to require development [25,142]. The Canadian Occupational Performance Measure [138] has been used successfully in a robotic-assisted gait training experimental study and results suggest that wider health outcomes and health-related quality of life should be measured in future research [45]. QUEST 2.0 has also been used successfully in stepping device studies [66,84], and may be useful in comparing parent satisfaction with different stepping device types or features in relation to child and environmental factor profile.
For individuals with non-ambulant CP, no significant benefits have been found for robotic-assisted gait training in comparison to partial body-weight supported treadmill training combined with overground training [45], and overground training may be essential if the goal is to improve overground walking [58]. Studies comparing intensive overground stepping device training directly with these other technologies is warranted. Incorporating use of stepping devices in real-life activities and environments following participation in intensive training also merits investigation.
A recent scoping review on the development of individuals with CP confirmed a lack of studies exploring the impact on participation and environmental factors over time [143] and longitudinal studies of the impact of stepping devices on development are needed. Numerous studies and expert opinion comments noted the impact on emotional and psycho-social development and studies evaluating these outcomes quantitatively and over time are warranted. For individuals at GMFCS IV/V the focus for research regarding stepping device use should be less on stepping and gait pattern, and more on physical fitness, overall health and participation, engagement and quality of life outcomes.
4.4. Limitations
Although extensive hand searching was undertaken, it is challenging to search within the grey literature. Unknown researchers and unpublished studies may have been missed. Three articles were not retrieved. Results of two were described in an included study [60] and suggest improved gait pattern [30], hand function, and participation [29] for children using hands-free orthotic stepping devices. These findings are supported by other studies in this review. The remaining thesis [31] compared partial body weight-supported treadmill training and overground gait training and reported positive benefits for both, but it is unclear from the abstract whether studies included non-ambulant or ambulant CP. The comparison between partial body-weight-supported treadmill training and overground gait training has been addressed by other included syntheses [52,55,56].
This review included primarily descriptive evidence, some of which was only reported in conference abstracts. Some case reports were described in book chapters and magazine articles, and the level of detail and quality of reporting varied. A quality rating tool was therefore inappropriate for the majority of included studies, and only used to allow comparison between the group intervention and qualitative studies. Conflict of interest and influence of funding sources was mainly reported in peer-reviewed studies. Although only one article reported that the funder and device distributor had input into the planning and conduct of the study [60], it is possible that this may have been the case in other included studies, but was not noted due to differing reporting and publication standards.
In synthesizing results for visual presentation, no allowance was made for the relative quality of different studies, and a simple count of participants for each outcome was calculated. The unpublished longitudinal data from Spain [86] came from a commercial source and was collected in clinical practice rather than in the context of a research study. It included 40% of the total participants at GMFCS IV/V and therefore outcomes were reported separately to avoid skewing overall findings with data from a non-peer reviewed source, a single location, and reporting a single stepping device type. However, interestingly, that dataset did confirm three of the five major outcomes (improved head and trunk control; emotional development; stepping and mobility) drawn from all included studies.
Although higher quality evidence was not identified since the previous systematic review, this review provides a more in-depth exploration of outcomes and the lived experience for individuals functioning at GMFCS IV and V. The significant number of participants included from a wide range of ages, settings, and countries may increase the credibility and transferability of the findings.
5. Conclusions
Use of supported-stepping devices is feasible for children, adolescents, and adults functioning at GMFCS IV and V, with introduction as young as 9 months of age. Benefits include impact on emotional and psycho-social development, improved head, trunk, and upper limb control, communication, inclusion and participation with others. Minimal harms have been reported other than the need to ensure safety and stability as children increase in size. Contraindications include pain and flexor withdrawal response to weight-bearing. Adequate family or caregiver support is essential to ensure safety, inclusion, engagement and participation in meaningful activities and routines.
Increased ability to step was reported for most users, although stepping devices are primarily prescribed to enhance physical fitness and participation for individuals functioning at GMFCS IV and V, rather than for functional mobility. Although there are challenges with the continued use of stepping devices into adulthood due to increasing physical limitations, a lack of appropriately sized devices, and transfer difficulties, feasibility for some has been demonstrated. Evidence for stepping device use continues to be primarily descriptive, but the significance of upright positioning and mobility cannot be overstated for reducing sedentary behavior and positively impacting self-esteem and participation, and positively influencing the perceptions of others for individuals with non-ambulant CP.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/disabilities3020012/s1, File S1: Search strategy; File S2: MMAT quality rating.
Author Contributions
Conceptualization, R.W.L. and G.S.P.; formal analysis, R.W.L. and G.S.P.; writing—original draft preparation, R.W.L.; writing—review and editing, G.S.P. and R.W.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data supporting the findings of this study are mainly available within the article and its supplementary materials. Any additional data is available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to acknowledge the Sunny Hill Health Centre and the University of British Columbia Library Staff for assisting with the search and retrieval of articles; Rikke Damkjær Moen for assistance in retrieving studies and contacting European researchers; Alvaro Hidalgo Robles and Lourdes Macias Merlo for their assistance with Spanish language articles and contacting researchers in Spain; Lori Potts and Zach Huleatt for their assistance in retrieving studies and clarifying outcome measure details; and Idoia Gandarias Mendieta, Isabel Rodriguez Costa, Frances George, Kate Willoughby, Virginia Wright, Minakshi Sharma and Sanyam Bajracharya for their willingness to share additional details regarding their research for this review.
Conflicts of Interest
R.W.L. declares no conflicts of interest. G.S.P. has worked as an educational consultant for Prime Engineering, a manufacturer of supported-standing and stepping devices. This relationship had no influence on this unfunded study.
References
- MacLennan, A.H.; Lewis, S.; Moreno-De-Luca, A.; Fahey, M.; Leventer, R.J.; McIntyre, S.; Ben-Pazi, H.; Corbett, M.; Wang, X.; Baynam, G.; et al. Genetic or Other Causation Should Not Change the Clinical Diagnosis of Cerebral Palsy. J. Child Neurol. 2019, 34, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Smithers-Sheedy, H.; Badawi, N.; Blair, E.; Cans, C.; Himmelmann, K.; Krägeloh-Mann, I.; McIntyre, S.; Slee, J.; Uldall, P.; Watson, L.; et al. What constitutes cerebral palsy in the twenty-first century? Dev. Med. Child Neurol. 2014, 56, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content validity of the expanded and revised Gross Motor Function Classification System. Dev. Med. Child Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef]
- Bartlett, D.J.; Chiarello, L.A.; Mccoy, S.W.; Palisano, R.J.; Jeffries, L.; Fiss, A.L.; Rosenbaum, P.; Wilk, P. Determinants of gross motor function of young children with cerebral palsy: A prospective cohort study. Dev. Med. Child Neurol. 2014, 56, 275–282. [Google Scholar] [CrossRef]
- Rodby-Bousquet, E.; Czuba, T.; Hägglund, G.; Westbom, L. Postural asymmetries in young adults with cerebral palsy. Dev. Med. Child Neurol. 2013, 55, 1009–1015. [Google Scholar] [CrossRef] [Green Version]
- Casey, J.; Agustsson, A.; Rosenblad, A.; Rodby-Bousquet, E. Relationship between scoliosis, windswept hips and contractures with pain and asymmetries in sitting and supine in 2450 children with cerebral palsy. Disabil. Rehabil. 2022, 44, 6738–6743. [Google Scholar] [CrossRef]
- Casey, J.; Rosenblad, A.; Rodby-Bousquet, E. Postural asymmetries, pain, and ability to change position of children with cerebral palsy in sitting and supine: A cross-sectional study. Disabil. Rehabil. 2022, 44, 2363–2371. [Google Scholar] [CrossRef]
- Ganz, F.; Hammam, N.; Pritchard, L. Sedentary behavior and children with physical disabilities: A scoping review. Disabil. Rehabil. 2021, 43, 2963–2975. [Google Scholar] [CrossRef]
- Bailes, A.F.P.; Greve, K.P.; Long, J.; Kurowski, B.G.M.; Vargus-Adams, J.M.; Aronow, B.; Mitelpunkt, A. Describing the Delivery of Evidence-Based Physical Therapy Intervention to Individuals with Cerebral Palsy. Pediatr. Phys. Ther. 2021, 33, 65–72. [Google Scholar] [CrossRef]
- Maitre, N.L.; Chorna, O.; Romeo, D.M.; Guzzetta, A. A High-Risk Infant Follow-Up Program. Pediatr. Neurol. 2016, 65, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einspieler, C.; Bos, A.F.; Krieber-Tomantschger, M.; Alvarado, E.; Barbosa, V.M.; Bertoncelli, N.; Burger, M.; Chorna, O.; Del Secco, S.; DeRegnier, R.-A.; et al. Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome. J. Clin. Med. 2019, 8, 1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobo, M.A.; Harbourne, R.T.; Dusing, S.C.; McCoy, S.W. Grounding Early Intervention: Physical Therapy Cannot Just Be About Motor Skills Anymore. Phys. Ther. 2013, 93, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Roquet, M.; Garlantezec, R.; Remy-Neris, O.; Sacaze, E.; Gallien, P.; Ropars, J.; Houx, L.; Pons, C.; Brochard, S. From childhood to adulthood: Health care use in individuals with cerebral palsy. Dev. Med. Child Neurol. 2018, 60, 1271–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paleg, G.; Livingstone, R. Outcomes of gait trainer use in home and school settings for children with motor impairments: A systematic review. Clin. Rehabil. 2015, 29, 1077–1091. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability & Health (ICF); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Eisenberg, S.; Zuk, L.; Carmeli, E.; Katz-Leurer, M. Contribution of Stepping While Standing to Function and Secondary Conditions Among Children with Cerebral Palsy. Pediatr. Phys. Ther. 2009, 21, 79–85. [Google Scholar] [CrossRef]
- Wright, F.V.; Belbin, G.; Slack, M.; Jutai, J. An evaluation of the David Hart Walker Orthosis: A new assistive device for children with Cerebral Palsy. Physiother. Can. 1999, 51, 280–291. [Google Scholar]
- Paleg, G.; Livingstone, R. Evidence-informed clinical perspectives on selecting gait trainer features for children with cerebral palsy. Int. J. Ther. Rehabil. 2016, 23, 444–454. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K.; Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, K.K.; Colquhoun, H.; Levac, D.; Baxter, L.; Tricco, A.C.; Straus, S.; Wickerson, L.; Nayar, A.; Moher, D.; O’Malley, L. Advancing scoping study methodology: A web-based survey and consultation of perceptions on terminology, definition and methodological steps. BMC Health Serv. Res. 2016, 16, 305. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean, L.J.; Paleg, G.S.; Livingstone, R.W. Supported-standing interventions for children and young adults with non-ambulant cerebral palsy: A scoping review. Dev. Med. Child Neurol. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, R.; Paleg, G. Measuring Outcomes for Children with Cerebral Palsy Who Use Gait Trainers. Technologies 2016, 4, 22. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. User guide. McGill. 2018, pp. 1–11. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 11 December 2022).
- Rosenbaum, P.; Gorter, J.W. The ‘F-words’ in childhood disability: I swear this is how we should think! Child Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Longo, E.; Monteiro, R.; Hidalgo-Robles, A.; Paleg, G.; Shrader, C.; De Campos, A.C. Intervention ingredients and F-words in early intervention for children with cerebral palsy functioning at GMFCS IV and V: A scoping review protocol. Front. Rehabil. Sci. 2023, 4, 1110552. [Google Scholar] [CrossRef]
- Becker, C.; Hoppstadter, W. Gehend Spielend Handeln. Bachelor’s Thesis, Ergotherapie Hogeschool Zuyd, Heerlen, The Netherlands, 2003. [Google Scholar]
- Gibbins, K.; Baltzopoulos, V. The Effects of the David Hart Orthosis on the Gait Development of Children with Cerebral Palsy. Master’s Thesis, University of Liverpool, Liverpool, UK, 1994. [Google Scholar]
- Hoyme, D. Body Weight Supported Treadmill Training Versus Gait Trainer in Young Children with Cerebral Palsy. Ph.D. Thesis, 2016. [Google Scholar]
- Hallemans, A.; Cuppers, R.; Truijen, S.; Truijen, S.; Ego, F.; Moens, M.; Wenmakers, D.; Caers, P.; Lebeer, J. Walking in the Hibbot, an Innovative Walking Aid Improves Gait Characteristics in Children with Cerebral Palsy: A Cross-Sectional Study. Preprint 2020. [Google Scholar] [CrossRef]
- Jung, T.; Kim, Y.; Kelly, L.E.; Abel, M.F. Biomechanical and perceived differences between overground and treadmill walking in children with cerebral palsy. Gait Posture 2016, 45, 1–6. [Google Scholar] [CrossRef]
- Paleg, G.; Wright, J. Schizencephaly: Children with a rare developmental disorder are treated with physical therapy. Adv. Phys. Ther. PT Assist. 1998, 35–36. [Google Scholar]
- Paleg, G. Different approach–Physical therapy for a child with CHARGE syndrome: A contrast in practice patterns. Adv. PT 2003, 45–46. [Google Scholar]
- Parent, A.; Letellier, G.; Lachapelle, J.; Marois, P.; Larochelle, J.; Mohebbi, A.; Ballaz, L. Arm-free overground walking with partial body weight support in children with cerebral palsy: A case study. Gait Posture 2022, 97, S139–S140. [Google Scholar] [CrossRef]
- van der Krogt, M.M.; Sloot, L.H.; Harlaar, J. Overground versus self-paced treadmill walking in a virtual environment in children with cerebral palsy. Gait Posture 2014, 40, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J. MOVE program enables children to develop functional ambulatory skills. PT Bull. 1996, 4–5. [Google Scholar]
- Akhter, N. Mother’s Perceptions towards Using Functional Mobility Aids for Their Children with Cerebral Palsy. Bachelor’s Thesis, University of Dakha, Bangladesh, South Asia, 2015. [Google Scholar]
- Kassim, N.; Pattnaik, M.; Mohanty, P.; Kavi, M. Comparison of Integrated Task Oriented Bodyweight Supported Overground Training with Body-Weight Supported Treadmill Training to Improve Functional Mobility in Children with Spastic Diplegic Cerebral Palsy—A Single Blinded Randomized Control Trial. Biomed. Pharmacol. J. 2022, 15, 651–662. [Google Scholar] [CrossRef]
- Laksana, P.; Setyanto, R.; Herdiman, L. Redesign paediatric walker for children with spastic cerebral palsy using TRIZ Method. J. Sist. Dan. Manaj. Ind. 2021, 5, 8–14. [Google Scholar] [CrossRef]
- Lestari, N.T.; Susmartini, S.; Herdiman, L. Redesign paediatric walker for children with spastic cerebral palsy using TRIZ Method. J. Phys. Conf. Ser. 2020, 1450. [Google Scholar] [CrossRef]
- O’Handley, R.D.; Dadakhodjaeva, K.; Radley, K.C.; Dart, E.H. Promoting independent ambulation: A case study of an elementary school student with developmental disabilities. Res. Dev. Disabil. 2016, 56, 153–159. [Google Scholar] [CrossRef]
- Pool, D.; Elliott, C.; Willis, C.; Thornton, A. The Experience of Locomotor Training From the Perspectives of Therapists and Parents of Children With Cerebral Palsy. Front. Rehabil. Sci. 2021, 2, 740426. [Google Scholar] [CrossRef]
- Pool, D.; Valentine, J.; Taylor, N.F.; Bear, N.; Elliott, C. Locomotor and robotic assistive gait training for children with cerebral palsy. Dev. Med. Child Neurol. 2021, 63, 328–335. [Google Scholar] [CrossRef]
- Snarski, K.E. Effects of stepping practice with postural support on gross motor abilities of a pre-ambulatory child with cerebral palsy: A case report. Physiother. Theory Pr. 2021, 37, 234–241. [Google Scholar] [CrossRef]
- Su, I.Y.; Chung, K.K.; Chow, D.H. Treadmill training with partial body weight support compared with conventional gait training for low-functioning children and adolescents with nonspastic cerebral palsy: A two-period crossover study. Prosthetics Orthot. Int. 2013, 37, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, L. Why We Love Gait Training. Mobility Management. 2016. Available online: https://mobilitymgmt.com/articles/2016/04/01/gait-training.aspx (accessed on 11 December 2022).
- Bradbury, J.-A. “Standing tall”: An Analysis of Parents’ Evaluations of a Walker for Children with Cerebral Palsy. Master’s Thesis, University of Toronto, Toronto, ON, Canada, 1997. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71, PMCID:PMC8005924. [Google Scholar] [CrossRef] [PubMed]
- Amacher, R.; Steiner, N. Der einsatz von stehgestellen bei kindern mit infantiler cerebralparese aus ergotherapeutischer sicht. Bachelor’s Thesis, Zurich University of Applied Sciences, Winterthur, Switzerland, 2010. Available online: https://digitalcollection.zhaw.ch/bitstream/11475/322/1/Amacher_Steiner.pdf (accessed on 11 December 2022).
- Booth, A.T.C.; Buizer, A.; Meyns, P.; Lansink, I.L.B.O.; Steenbrink, F.; van der Krogt, M. The efficacy of functional gait training in children and young adults with cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2018, 60, 866–883. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Mc Namara, M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paleg, G.; Livingstone, R. Evidence-informed clinical perspectives on postural management for hip health in children and adults with non-ambulant cerebral palsy. J. Pediatr. Rehabil. Med. 2022, 15, 39–48. [Google Scholar] [CrossRef]
- Gannotti, M.E.P.; Liquori, B.M.M.; Thorpe, D.E.P.; Fuchs, R.K.P. Designing Exercise to Improve Bone Health Among Individuals With Cerebral Palsy. Pediatr. Phys. Ther. 2021, 33, 50–56. [Google Scholar] [CrossRef]
- Jackman, M.; Sakzewski, L.; Morgan, C.; Boyd, R.N.; Brennan, S.E.; Langdon, K.; Toovey, R.A.M.; Greaves, S.; Thorley, M.; Novak, I. Interventions to improve physical function for children and young people with cerebral palsy: International clinical practice guideline. Dev. Med. Child Neurol. 2022, 64, 536–549. [Google Scholar] [CrossRef]
- de Campos, A.C.; Hidalgo Robles, A.; Longo, E.; Shrader, C.; Paleg, G. Scoping review of early interventions for young children classified as Gross Motor Function Classification System (GMFCS) IV and V. Dev. Med. Child Neurol. 2023; submitted. [Google Scholar]
- Willoughby, K.L.; Dodd, K.J.; Shields, N.; Foley, S. Efficacy of Partial Body Weight–Supported Treadmill Training Compared With Overground Walking Practice for Children With Cerebral Palsy: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2010, 91, 333–339. [Google Scholar] [CrossRef]
- van der Putten, A.; Vlaskamp, C.; Reynders, K.; Nakken, H. Children with profound intellectual and multiple disabilities: The effects of functional movement activities. Clin. Rehabil. 2005, 19, 613–620. [Google Scholar] [CrossRef]
- Kuenzle, C.; Brunner, R. The Effects of the Norsk Funktion-Walking Orthosis on the Walking Ability of Children With Cerebral Palsy and Severe Gait Impairment. JPO J. Prosthet. Orthot. 2009, 21, 138–144. [Google Scholar] [CrossRef]
- Wright, F.V.; Jutai, J.W. Evaluation of the longer-term use of the David Hart Walker Orthosis by children with cerebral palsy: A 3-year prospective evaluation. Disabil. Rehabil. Assist. Technol. 2006, 1, 155–166. [Google Scholar] [CrossRef]
- Smati, S.; Pouliot-Laforte, A.; Chevalier, M.; Lemay, M.; Ballaz, L. Effect of power training on locomotion capacities in children with cerebral palsy with GMFCS level III–IV. Disabil. Rehabil. 2022, 623. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, M.; Tierney, S. Perspectives of children with physical disabilities, parents and physiotherapists on use of walkers and their potential to increase physical activity. A qualitative exploration. J. Child Health Care 2022, 1–21. [Google Scholar] [CrossRef] [PubMed]
- McKeever, P.; Rossen, B.E.; Scott, H.; Robinson-Vincent, K.; Wright, V. The significance of uprightness: Parents’ reflections on children’s responses to a hands-free walker for children. Disabil. Soc. 2013, 28, 380–392. [Google Scholar] [CrossRef]
- Rodríguez-Costa, I.; De la Cruz-López, I.; Fernández-Zárate, I.; Maldonado-Bascón, S.; Lafuente-Arroyo, S.; Nunez-Nagy, S. Benefits of a Low-Cost Walking Device in Children with Cerebral Palsy: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 2808. [Google Scholar] [CrossRef]
- Paananen, L. Ihastuttaako vai vihastuttaako ? kävelyn apuvälineeseen. Master’s Thesis, Jamk University of Applied Sciences, Jyväskylä, Finland, 2009. Available online: https://www.theseus.fi/bitstream/handle/10024/6662/Paananen_Laila.pdf?sequence=1&isAllowed=y (accessed on 11 December 2022).
- Barnes, S.B.; Whinnery, K.W. Effects of Functional Mobility Skills Training for Young Students with Physical Disabilities. Except. Child. 2002, 68, 313–324. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Campodonico, F.; Piazzolla, G.; Scalini, L.; Oliva, D. Impact of favorite stimuli automatically delivered on step responses of persons with multiple disabilities during their use of walker devices. Res. Dev. Disabil. 2005, 26, 71–76. [Google Scholar] [CrossRef]
- Lancioni, G.; Nirbhay, N.; O’Reilly, F.; Campodonico, F.; Oliva, O.; Vigo, C. Promoting walker-assisted step responses by an adolescent with multiple disabilities through automatically delivered stimulation. J. Vis. Impair. Blind. 2005, 99, 109–113. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Oliva, D.; Scalini, L.; Castagnaro, F.; Di Bari, M. Promoting foot–leg movements in children with multiple disabilities through the use of support devices and technology for regulating contingent stimulation. Cogn. Process. 2007, 8, 279–283. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Oliva, D.; Piazzolla, G.; Pidala, S.; Smaldone, A.; Manfredi, F. Automatically Delivered Stimulation for Walker-Assisted Step Responses: Measuring its Effects in Persons with Multiple Disabilities. J. Dev. Phys. Disabil. 2007, 19, 1–13. [Google Scholar] [CrossRef]
- Lancioni, G.E.; De Pace, C.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Didden, R. Promoting Step Responses of Children with Multiple Disabilities through a Walker Device and Microswitches with Contingent Stimuli. Percept. Mot. Ski. 2008, 107, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Oliva, D.; Smaldone, A.; La Martire, M.L.; Stasolla, F.; Castagnaro, F.; Groeneweg, J. Promoting ambulation responses among children with multiple disabilities through walkers and microswitches with contingent stimuli. Res. Dev. Disabil. 2010, 31, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Oliva, D.; Campodonico, F.; Buono, S. Walker devices and microswitch technology to enhance assisted indoor ambulation by persons with multiple disabilities: Three single-case studies. Res. Dev. Disabil. 2013, 34, 2191–2199. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, J.; Woollam, P.J.; Major, R.; Stallard, J. Technical note: A rear support walking frame for severely disabled children with cerebral palsy: Initial development. Prosthet. Orthot. Int. 2000, 24, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Camallonga, M.O. Protocolo de valoración fisioterápica para el correcto uso del NF Walker en niños con PCI. Master’s Thesis, Universidad CEU Cardenal Herrera, Valencia, Spain, 2013. Available online: https://repositorioinstitucional.ceu.es/bitstream/10637/6026/4/Protocolo_Orti%20Camallonga_TFG_2013.pdf (accessed on 11 December 2022).
- Gandarias Mendieta, I. Control Postural En Fisioterapia Pediátrica: Bipedestación Activa Y Compresión Dinámica. Jorn. Científicas La Soc. Española Rehabil. Infant. 2012, 2, 28–32. [Google Scholar]
- Livingstone, R.W.; Paleg, G.S.; Field, D.A. Supported Standing and Stepping Device Use in Young Children with Cerebral Palsy, Gross Motor Function Classification System III, IV and V: A Descriptive Study. Assist. Technol. 2023; in press. [Google Scholar]
- Low, S. Effects of the MOVE (Mobility Opportunities Via Education) curriculum on range of motion, motor skills, and functional mobility of children with severe multiple disabilities: A pilot program. Pediatr. Phys. Ther. 2005, 17, 94–95. [Google Scholar]
- Low, S.; Westcott-McCoy, S.; Adams, J.; Beling, J. A comparison of two support walkers on the gait parameters of children with cerebral palsy. Physiotherapy 2011, 97, eS709. [Google Scholar] [CrossRef] [Green Version]
- Martín Gómez, M.; Laguna Mena, C.; Martín Maroto, M.; Arroyo Riaño, M. Evaluation of the NF-Walker. English translation of article originally published in: Jornadas Cientificas de la Sociedad Espanola de Rehabilitacion Infantil. 2012. Available online: https://cdn2.hubspot.net/hubfs/2252381/Documentation%20_%20How%20to/NF-Walker/NF-Walker%20an%20evaluation.pdf (accessed on 11 December 2022).
- Martín Gómez, M.; Laguna Mena, C.; Martín Maroto, M.; Echevarria Ulloa, M.; Dumitrescu, A.; Arroyo Riaño, M. Evaluation and follow-up of NF-Walker technical aid during the transition to adult life. Dev. Med. Child Neurol. 2021, 63 (Suppl. S2), 42. [Google Scholar] [CrossRef]
- Paleg, V.S. Teaching older children with cerebral palsy to sit, stand and walk. Dev. Med. Child Neurol. 1997, 39 (Suppl. 75), 10–11. [Google Scholar]
- Sharma, M.; Bajracharya, S. Low cost modified reverse walker to assist children with cerebral palsy. RGUHS J. Allied Health Sci. 2021, 1, 18–24. Available online: https://journalgrid.com/view/article/rjahs/37 (accessed on 11 December 2022).
- Wright-Ott, C. Mobility Matters—Imbedding Hands-Free Locomotion Experiences into the Preschool and Elementary Curricula for Students with Severe Speech and Motor Impairment: The Bridge School Experience. Available online: https://curriculum.bridgeschool.org/wp-content/uploads/sites/5/2018/06/mobility_matters.pdf (accessed on 27 January 2023).
- Gandarias Mendieta, I.; (Clinica Pixuflitos, Bilboa, Spain). Personal communication, 2023.
- George, C.; Levin, W.; Ryan, J.M. The use and perception of support walkers for children with disabilities: A United Kingdom survey. BMC Pediatr. 2020, 20, 528. [Google Scholar] [CrossRef] [PubMed]
- Low, S.A.; McCoy, S.W.; Beling, J.; Adams, J. Pediatric Physical Therapists’ Use of Support Walkers for Children With Disabilities: A nationwide survey. Pediatr. Phys. Ther. 2011, 23, 381–389. [Google Scholar] [CrossRef]
- Peredo, D.E.; Davis, B.E.; Norvell, D.C.; Kelly, P.C. Medical equipment use in children with disabilities: A descriptive survey. J. Pediatr. Rehabil. Med. 2010, 3, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Altizer, W.; Paleg, G. Everyday with Emmitt. Directions 2020, 3, 42–47. Available online: https://issuu.com/nrrts/docs/directions_202020v3-full_20mag (accessed on 11 December 2022).
- Benson, K.; Capone, K.; Duch, K.; Palmer-Casey, C. Mobility supports in educational curriculum for children and youth with cerebral palsy. In Cerebral Palsy; Miller, F., Bachrach, S.J., Lennon, N., O’Neil, M.E., Eds.; Springer Nature: Berlin, Germany, 2020; pp. 2903–2916. [Google Scholar] [CrossRef]
- Carnevale, D. PS7 2: The Functional Architecture of a Gait Trainer. In Proceedings of the International Seating Symposium, Nashville, TN, USA, 26–28 February 2015; pp. 221–222. [Google Scholar]
- Farrell, E.; Naber, E.; Geigle, P. Description of a multifaceted rehabilitation program including overground gait training for a child with cerebral palsy: A case report. Physiother. Theory Pr. 2010, 26, 56–61. [Google Scholar] [CrossRef]
- George, F.K. The importance of static and dynamic posture: How making static equipment dynamic may improve movement and function of children with neurological impairment—A retrospective service evaluation. Assoc. Paediatr. Chart Physiother. J. 2018, 9, 56–62. [Google Scholar]
- Jones, M.A. Wheeled mobility options and indications for children and youth with cerebral palsy. In Cerebral Palsy; Miller, F., Bachrach, S.J., Lennon, N., O’Neil, M.E., Eds.; Springer Nature: Berlin, Germany, 2020; pp. 2949–2961. [Google Scholar] [CrossRef]
- Low, S. Comparison of two support walkers on the gait and mobility of a child with cerebral palsy: A case report. Pediatr. Phys. Ther. 2004, 16, 60–61. [Google Scholar]
- Paleg, G. Mobility Opportunities Via Education: (The MOVE story). Tomorrow’s PT 1997, 10–11. [Google Scholar]
- Paleg, G. Holoprosencephaly: Rare developmental disorder presents clinically as cerebral palsy. Adv. PT 1998, 34–35. [Google Scholar]
- Paleg, G. When Needs are Special: Determining Mobility Requirements for a Child with Joubert Syndrome. Available online: https://rehabpub.com/mobility/when-needs-are-special/ (accessed on 11 December 2022).
- Pope, E.; Tally, M. The importance of supporting the equipment needs of pediatric clients with complex neuromotor disorders. Directions 2022, 2, 32–41. Available online: https://issuu.com/nrrts/docs/directions_2022v2_full_issuu/s/15304057 (accessed on 11 December 2022).
- Whinnery, K.; Barnes, S. Mobility Training Using the MOVE® Curriculum A Parent’s View. Teach. Except. Child. 2002, 34, 44–50. Available online: http://cec.metapress.com/index/MM83015262427641.pdf (accessed on 11 December 2022). [CrossRef]
- Gordon, A.; Magill, R.; Paleg, G. Motor learning: Application of principles to pediatric rehabilitation. In Physical Therapy for Children, 6th ed.; Campbell, S., Linden, R., Palisano, R., Eds.; Elsevier: St. Louis, MI, USA, 2023; pp. 91–111. [Google Scholar]
- Kannegießer-leitner, C. The NF-Walker in the Rehabilitation of Children with a Pronounced Movement Disorder. Made for Movement Product Studies. Available online: https://cdn2.hubspot.net/hubfs/2252381/Documentation%20_%20Know-How/NF-Walker/NF-Walker%20in%20the%20rehabilitation%20of%20children%20with%20a%20pronounced%20movement%20disorder.pdf (accessed on 11 December 2022).
- Paleg, G. The MOVE approach to disabilities: Lifting bodies and spirits. PT OT Today 1997, 5, 12–27. [Google Scholar]
- Schneiders, S. Does Early Application of Medical Aid Devices Make Sense? Based on the Example of the NF Walker. Made for Movement Product Studies. Available online: https://cdn2.hubspot.net/hubfs/2252381/Documentation%20_%20How%20to/NF-Walker/NF-Walker%20Does%20early%20application%20of%20medical%20aid%20devices%20make%20sense.pdf (accessed on 11 December 2022).
- Schwerin, A.; Francke, A.; Weiß, P. NF-walker and botulinum toxin therapy for children with spastic tetraparesis. Neuropediatrics 2005, 36, 111. [Google Scholar] [CrossRef]
- Thompson, G. Children with Severe Disabilities and the MOVE Curriculum: Foundations of a Task-Oriented Therapy Approach; East River Press: New York, NY, USA, 2005. [Google Scholar]
- Bolton, M.; Donohoe, M. Ambulatory assistive devices for children and youth with cerebral palsy. In Cerebral Palsy; Miller, F., Bachrach, S.J., Lennon, N., O’Neil, M.E., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; pp. 2963–2975. [Google Scholar] [CrossRef]
- Covert, S.Y. Promoting Pediatric Participation. Rehab. Manag. 2019, 32, 20–23. Available online: http://digitaledition.rehabpub.com/rehabpub/diged/20191112/index.html (accessed on 11 December 2022).
- Gandarias Mendieta, I. NF-Walker: Dynamic and Mobile Standing Orthosis. Made for Movement Product Studies. 2008. Available online: https://cdn2.hubspot.net/hubfs/2252381/Documentation%20_%20Know-How/NF-Walker/NF-Walker%20Dynamic%20and%20mobile%20standing%20orthosis.pdf (accessed on 11 December 2022).
- Marquez, G.M. Promoting Function and Independence in the Cerebral Palsy Population. Rehab. Manag. 2019, 32, 24–26. Available online: http://digitaledition.rehabpub.com/rehabpub/diged/20190708/index.html (accessed on 11 December 2022).
- Thunberg, G.; Livingstone, R.; Buchholz, M.; Field, D. Environmental Adaptations. In Early Detection and Early Intervention in Developmental Motor Disorders; Hadders-Algra, M., Ed.; Mac Keith Press: London, UK, 2021; pp. 228–241. [Google Scholar] [CrossRef]
- Botega, R.; Medola, F.O.; Santos, C.B.A.; Silva, A.T.; Iunes, D.H.; Purquerio, B.D.M. A new walking aid with axillary support for children with cerebral palsy: Electromyographic evaluation. Disabil. Rehabil. Assist. Technol. 2013, 8, 507–510. [Google Scholar] [CrossRef]
- Meadows, C.; Meyerink, J.; Farley, R.; Gilmour, A. The Arrow Walker. Physiotherapy 1992, 78, 679–680. [Google Scholar] [CrossRef]
- Stallard, J.; Major, R.E.; Farmer, S.E. The potential for ambulation by severely handicapped cerebral palsy patients. Prosthet. Orthot. Int. 1996, 20, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Paleg, G.; Huang, M.; Gabela, S.C.V.; Sprigle, S.; Livingstone, R. Comparison of the inertial properties and forces required to initiate movement for three gait trainers. Assist. Technol. 2016, 28, 137–143. [Google Scholar] [CrossRef]
- Sabet, A.; Feldner, H.; Tucker, J.; Logan, S.W.; Galloway, J.C. ON Time Mobility: Advocating for Mobility Equity. Pediatr. Phys. Ther. 2022, 34, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Willerslev-Olsen, M.; Lund, M.C.; Lorentzen, J.; Barber, L.; Kofoed-Hansen, M.; Nielsen, J.B. Impaired muscle growth precedes development of increased stiffness of the triceps surae musculotendinous unit in children with cerebral palsy. Dev. Med. Child Neurol. 2018, 60, 672–679. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.-K.; Yoon, Y.K.; Chung, K.B.; Rhee, Y.; Cho, S.-R. Patients with non-ambulatory cerebral palsy have higher sclerostin levels and lower bone mineral density than patients with ambulatory cerebral palsy. Bone 2017, 103, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Shortland, A. Muscle deficits in cerebral palsy and early loss of mobility: Can we learn something from our elders? Dev. Med. Child Neurol. 2009, 51, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Verschuren, O.; Peterson, M.D.; Balemans, A.C.; Hurvitz, E.A. Exercise and physical activity recommendations for people with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 798–808. [Google Scholar] [CrossRef]
- Verschuren, O.; Hulst, R.Y.; Voorman, J.; Pillen, S.; Luitwieler, N.; Dudink, J.; Gorter, J.W. 24-hour activity for children with cerebral palsy: A clinical practice guide. Dev. Med. Child Neurol. 2020, 63, 54–59. [Google Scholar] [CrossRef]
- Tedla, J.S.; Ganesan, S.; Katragadda, S. Inter-rater reliability of the Top Down Motor Milestone Test: A cross-sectional study. Clin. Rehabil. 2009, 23, 725–729. [Google Scholar] [CrossRef]
- Bradbury, M.; Bennison, E.; Mason, H.; Gregory, J. Tools for participation: Living aids and the F-words for childhood development. Paediatr. Child Health 2021, 31, 352–358. [Google Scholar] [CrossRef]
- Gibson, B.E.; Teachman, G.; Wright, V.; Fehlings, D.; Young, N.L.; McKeever, P. Children’s and parents’ beliefs regarding the value of walking: Rehabilitation implications for children with cerebral palsy. Child Care Health Dev. 2012, 38, 61–69. [Google Scholar] [CrossRef]
- Palisano, R.J.; Shimmell, L.J.; Stewart, D.; Lawless, J.J.; Rosenbaum, P.L.; Russell, D.J. Mobility Experiences of Adolescents with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2009, 29, 133–153. [Google Scholar] [CrossRef]
- Huang, I.-C.; Sugden, D.; Beveridge, S. Children’s perceptions of their use of assistive devices in home and school settings. Disabil. Rehabil. Assist. Technol. 2009, 4, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Huroy, M.; Behlim, T.; Andersen, J.; Buckley, D.; Fehlings, D.; Kirton, A.; Pigeon, N.; Mishaal, R.A.; Wood, E.; Shevell, M.; et al. Stability of the Gross Motor Function Classification System over time in children with cerebral palsy. Dev. Med. Child Neurol. 2022, 64, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Weiss-lambrou, R.; Ska, B. The Quebec User Evaluation of Satisfaction with assistive Technology (QUEST 2.0): An overview and recent progress. Technol. Disabil. 2002, 14, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Murchland, S.; Kernot, J.; Parkyn, H. Children’s Satisfaction With Assistive Technology Solutions for Schoolwork Using the QUEST 2.1: Children’s Version. Assist. Technol. 2011, 23, 162–176. [Google Scholar] [CrossRef]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. Item Analysis of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST). Assist. Technol. 2000, 12, 96–105. [Google Scholar] [CrossRef]
- Field, D.A.; Livingstone, R.W. Parents’ and Therapists’ Satisfaction with Four Early Childhood Power Mobility Devices. Can. J. Occup. Ther. 2022, 89, 364–375. [Google Scholar] [CrossRef]
- Tefft, D.; Guerette, P.; Furumasu, J. The Impact of Early Powered Mobility on Parental Stress, Negative Emotions, and Family Social Interactions. Phys. Occup. Ther. Pediatr. 2011, 31, 4–15. [Google Scholar] [CrossRef]
- Gudjonsdottir, B.; Gudmundsdottir, S.B. Mobility devices for children with physical disabilities: Use, satisfaction and impact on participation. Disabil. Rehabil. Assist. Technol. 2021, 1–8. [Google Scholar] [CrossRef]
- Fox-Hustwaite, M. What moves you? Teaching mobility versus developing motor skills based on the developmental continuum. Rehab. Manag. 2013, 26, 36–41. [Google Scholar]
- Russell, D.J.; Gorter, J.W. Assessing functional differences in gross motor skills in children with cerebral palsy who use an ambulatory aid or orthoses: Can the GMFM-88 help? Dev. Med. Child Neurol. 2005, 47, 462–467. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15991866 (accessed on 11 December 2022). [CrossRef]
- van der Putten, A.; Vlaskamp, C.; Reynders, K.; Nakken, H. Movement skill assessment in children with profound multiple disabilities: A psychometric analysis of the Top Down Motor Milestone Test. Clin. Rehabil. 2005, 19, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Baptiste, S.; McColl, M.; Opzoomer, A.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: An Outcome Measure for Occupational Therapy. Can. J. Occup. Ther. 1990, 57, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Gorter, J.W.; Ketelaar, M.; Rosenbaum, P.; Helders, P.J.M.; Palisano, R. Use of the GMFCS in infants with CP: The need for reclassification at age 2 years or older. Dev. Med. Child Neurol. 2009, 51, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.J.; Cameron, D.; Rosenbaum, P.L.; Walter, S.D.; Russell, D. Stability of the Gross Motor Function Classification System. Dev. Med. Child Neurol. 2006, 48, 424–428. [Google Scholar] [CrossRef]
- Hanna, S.E.; Bartlett, D.J.; Rivard, L.M.; Russell, D.J. Reference Curves for the Gross Motor Function Measure: Percentiles for Clinical Description and Tracking Over Time Among Children With Cerebral Palsy. Phys. Ther. 2008, 88, 596–607. [Google Scholar] [CrossRef]
- Dumas, H.M.; Fragala-Pinkham, M.A.; Moed, R. Scoping Review of Judgment-Based Measures of Ambulation with Assistive Devices for Children and Youth. Phys. Occup. Ther. Pediatr. 2021, 41, 120–137. [Google Scholar] [CrossRef]
- Chagas, P.S.C.; Magalhães, E.D.D.; Junior, R.R.S.; Romeros, A.C.S.F.; Palisano, R.J.; Leite, H.R.; Rosenbaum, P. Development of children, adolescents, and young adults with cerebral palsy according to the ICF: A scoping review. Dev. Med. Child Neurol. 2022, 1–9. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 flow diagram [50].
Figure 1.
PRISMA 2020 flow diagram [50].

Figure 2.
(a) Individual ICF outcomes reported. (b) Expert opinion on ICF outcomes. BSF Emotional function: regulation, happiness, motivation, confidence and self-esteem. Physical function: fitness, muscle strength and exercise. BMD: bone mineral density. Activity: Attention: watching, focusing attention and learning; maintaining position: head control, standing, trunk control; ADL: activities of daily living; stepping/mobility: includes walking speed and distance. Participation: Autonomy/engagement: engagement in school or play, autonomy, independence, initiation and sense of belonging.
Figure 2.
(a) Individual ICF outcomes reported. (b) Expert opinion on ICF outcomes. BSF Emotional function: regulation, happiness, motivation, confidence and self-esteem. Physical function: fitness, muscle strength and exercise. BMD: bone mineral density. Activity: Attention: watching, focusing attention and learning; maintaining position: head control, standing, trunk control; ADL: activities of daily living; stepping/mobility: includes walking speed and distance. Participation: Autonomy/engagement: engagement in school or play, autonomy, independence, initiation and sense of belonging.

Figure 3.
Lived experience data classified according to the F-words for childhood development [27].
Figure 3.
Lived experience data classified according to the F-words for childhood development [27].


{kind=link}
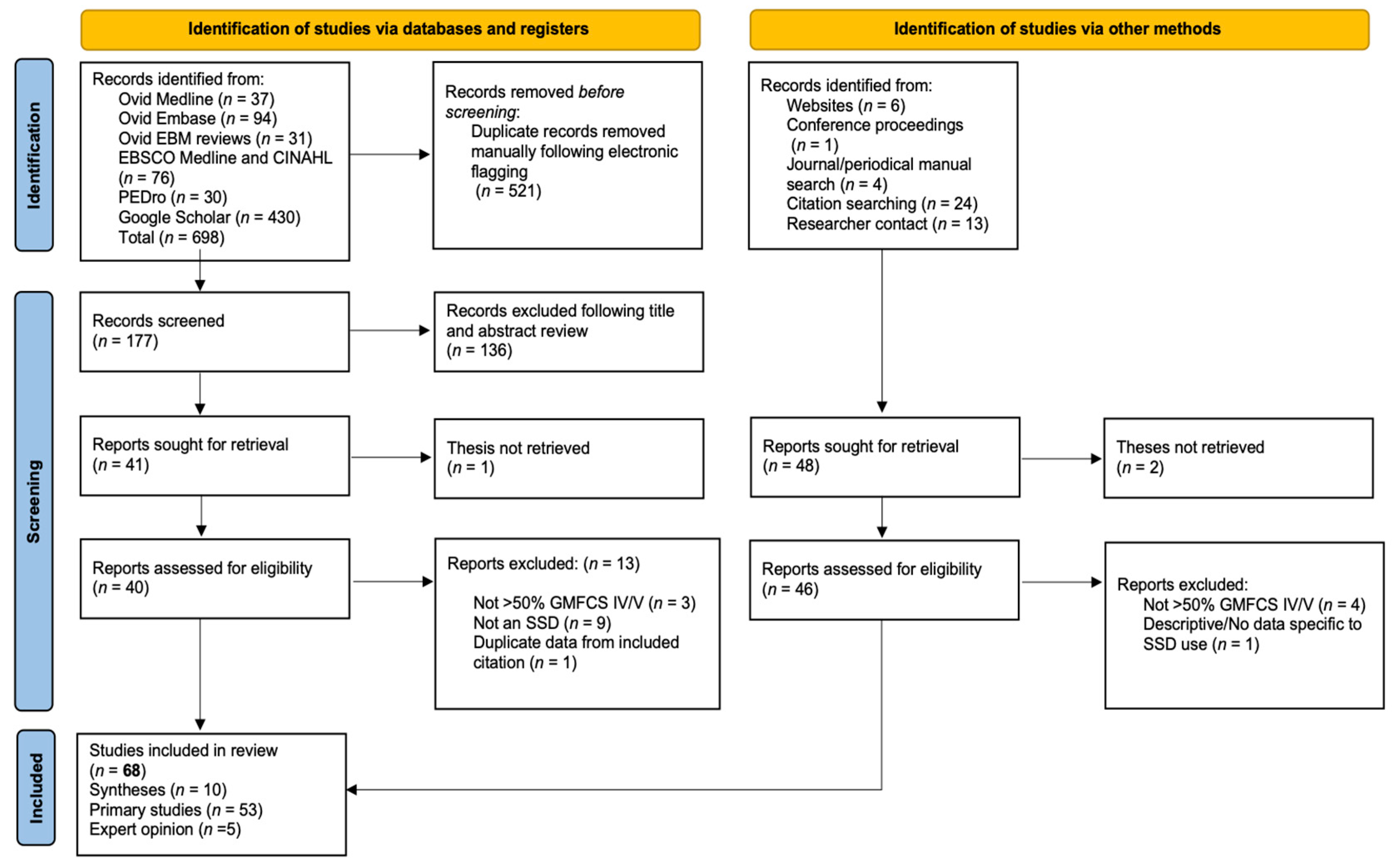{kind=link}
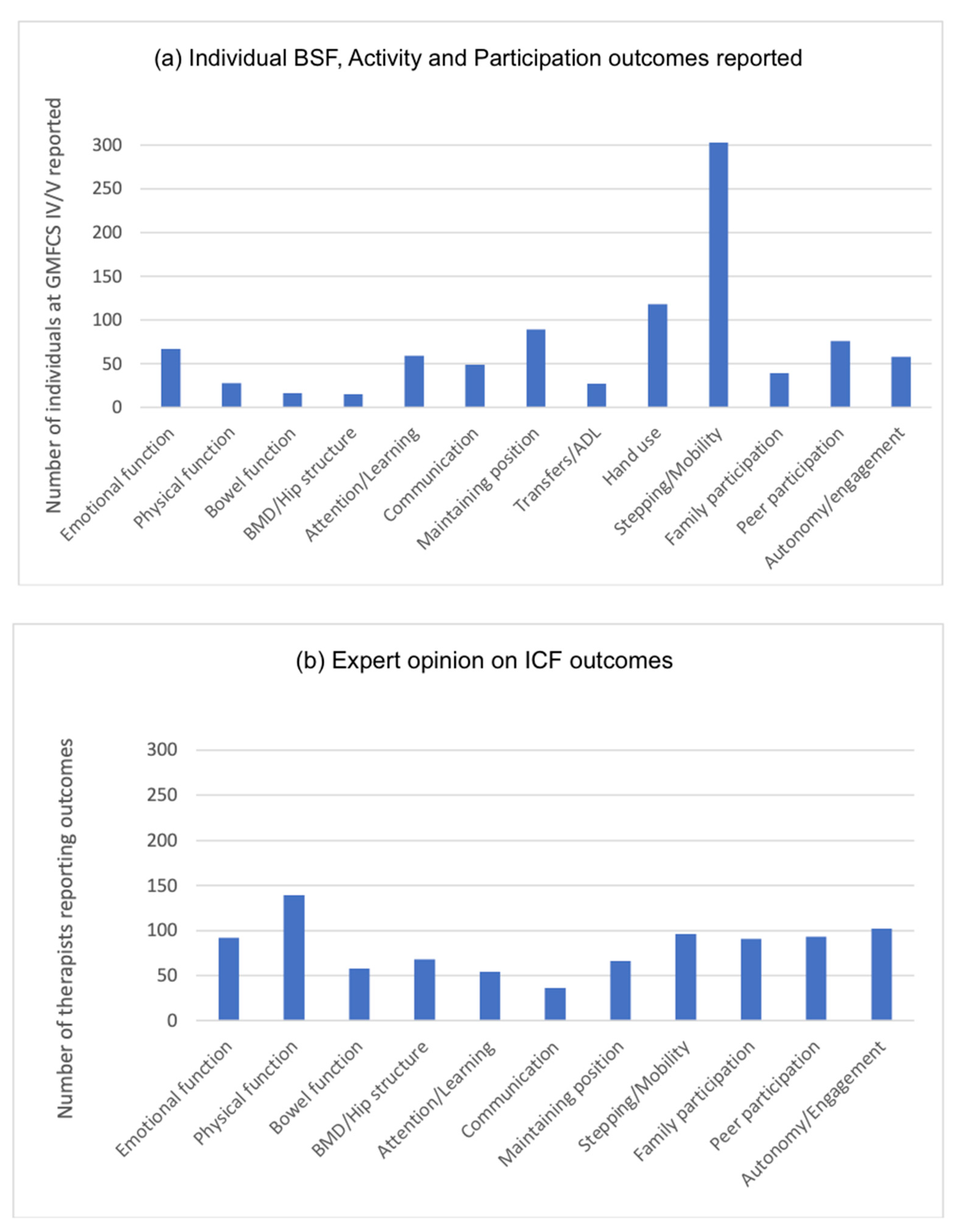{kind=link}
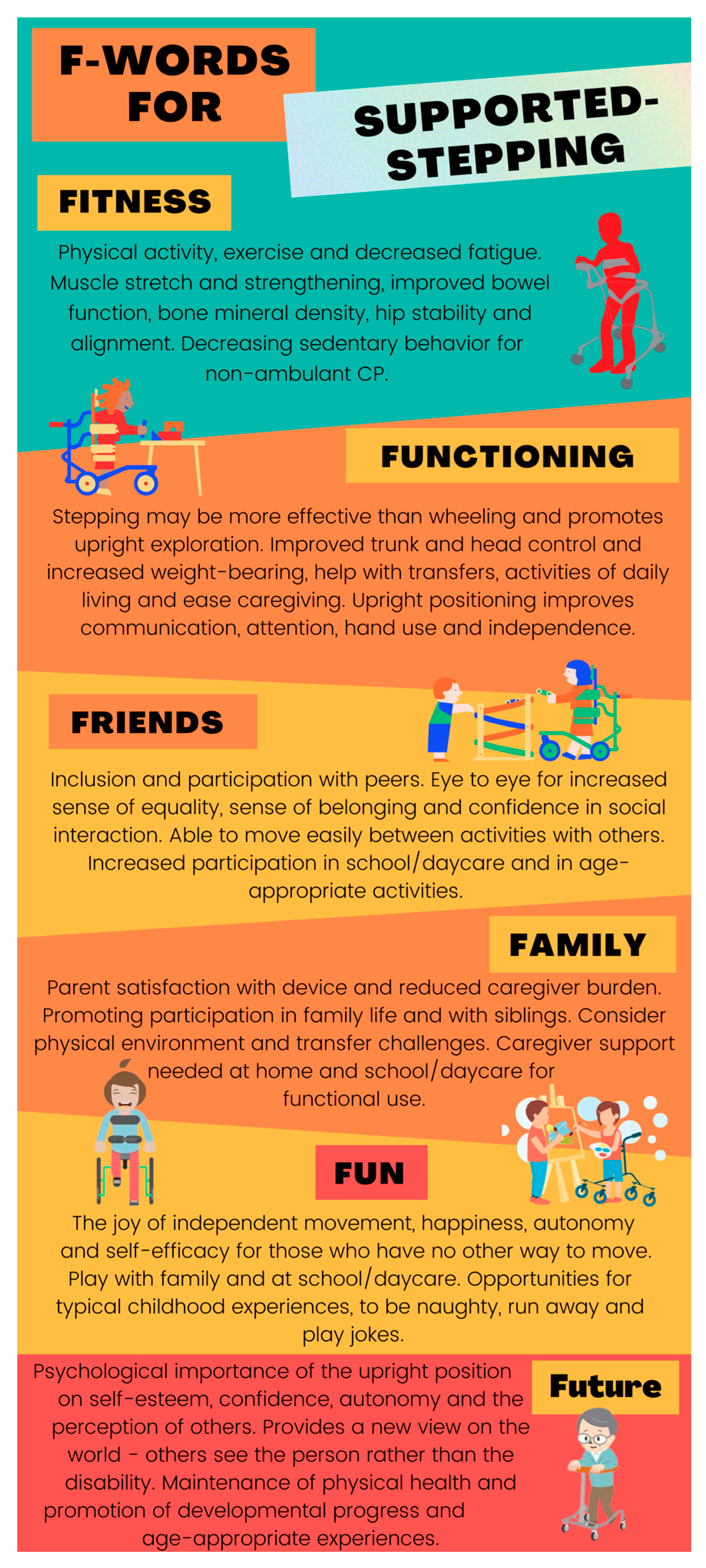{kind=link}
Table 1.
Reviews or guidelines relevant to use of stepping devices (SSDs) with GMFCS IV/V.
| Citation | Purpose | Relevant Studies | Conclusions |
|---|---|---|---|
| Amacher- Steiner, 2010 [51] | Review evidence for supported standing in relation to occupational therapy theory | Kuenzle [60], Eisenberg [17], Wright [61] | Dynamic standers (SSDs) positively impact mobility and hand function. Prescription is supported by occupational therapy theory. |
| Paleg, 2015 [15] COI reported Unfunded | Examine effect of SSDs on BSF, Activity or Participation outcomes for children up to 18 years | Barnes [67], Broadbent [75], Eisenberg [17], Farrell [93], Lancioni [69,70,71,72,73,74], McKeever [64], Van der Putten [59], Whinnery [101], Willoughby [58], Wright [18,61] | Youngest reported: 2–3 years; mean: 10 years. Recommended starting at 9–12 months. Mainly positive evidence, but primarily descriptive and insufficient to draw strong conclusions. Trend to increased walking distance and number of steps. Significant increase in mobility level and improved bowel function. Association between increased weight-bearing and bone mineral density. Positive impact on affect, motivation, and participation. |
| Paleg, 2016 [19] COI reported Unfunded | To review evidence and clinical considerations for selection of SSD features | 6 interventions [17,18,61,64,75,93], 3 devices [113,114,115], 1 device properties [116], 3 expert opinions [80,92,96], 1 survey [88] | Evidence supporting selection of SSDs and/or SSD features is descriptive. Research on all aspects of SSD development and prescription is needed. |
| Livingstone, 2016 [25] COI reported Unfunded | To review evidence supporting outcome measures that have been used, or may be useful for SSD outcomes | Barnes [67], Eisenberg [17], Farrell [93], Lancioni [69,70,71], Van der Putten [59], Willoughby [58], Wright [18,61] | Functional and individualized measures are more useful than spatio-temporal measures for GMFCS IV/V. Outcome measures for this population and intervention require development. |
| Booth, 2018 [52] Independent grant | Effectiveness of functional gait training in improving gait in children with CP | Willoughby [58], Farrell [93] | Functional gait training is safe and more effective for improving walking speed than standard physical therapy. Only interventions with partial body weight support are suitable for GMFCS IV/V. |
| Novak, 2020 [53] No COI | Summarize best available evidence for managing CP in 2019 | Paleg, 2015 [15] | Low quality evidence supports use of SSDs to increase gross-motor function and ability to step for GMFCS IV/V. Weak + recommendation. |
| Paleg, 2021 [54] COI reported Unfunded | Review use of postural management interventions to promote hip health in children and adults with non-ambulatory CP | Paleg, 2015 [15] | No studies have examined impact of SSDs on hip health. Clinical recommendation: active weightbearing and movement in SSD to promote position change and reduce sedentary behavior. |
| Gannotti, 2021 [55] Declared no COI Independent grant | Exercise interventions for bone health: guidelines for individuals with CP | N/A | Overground fast walking in SSD may provide moderate osteogenic exercise for GMFCS IV. Active assisted movement opportunities may benefit GMFCS V. |
| Jackman, 2022 [56] Declared no COI Independent grant | Clinical guideline: interventions to improve physical function in children with CP | Novak, 2020 [53], Booth, 2018 [52] | Overground more effective than partial body-weight supported treadmill training to increase walking distance for GMFCS IV/V. SSDs used for inclusion and well-being rather than functional mobility. |
| de Campos, 2023 [57] COI reported Unfunded | Scoping review: early interventions for young children GMFCS IV/V | Jackman [56], Eisenberg [17] | SSDs positively impact functioning, fitness, fun, friends, family and future for children under 5 years who are non-ambulant. |
COI: conflict of interest.
Table 2.
Included primary studies.
| Citation | Participants | Intervention | Results/Findings |
|---|---|---|---|
| Source | Randomized controlled group design (RCT) | ||
| Willoughby et al., 2009 [58] Peer-reviewed MMAT 4/5 Declared no COI Independent funding | Controls: 11 GMFCS IV 3 GMFCS III 11.24 ± 4.17 years Participants: 7 GMFCS IV 5 GMFCS III 10.35 ± 3.14 years | 30 min 2 times per week for 9 weeks Controls: Overground walking with anterior support-arms SSD # (GMFCS IV) or posterior walker # (GMFCS III) Participants: Partial body-weight supported treadmill training (PBWSTT) | No statistically significant between-group differences in: endurance (10 Minute Walk Test); or speed (10 Meter Walk Test). Trend to increased walking distance and endurance favoring overground training. Trend to decreased walking distance in PBWSTT group. Conclusion: to improve overground walking, practice overground. |
| Non-randomized group designs | |||
| Eisenberg et al., 2009 [17] Peer-reviewed MMAT 4/5 COI and funding not reported | Participants: 11 GMFCS IV/V 6.1 ± 2.1 years Controls: 11 GMFCS IV/V 6.8 ± 1.7 years | Use over 6 months: Participants: Hands-free orthotic SSD 2.1 ± 1.8 increased to 4.5 ± 2.3 h per week Controls: Stander 2.1 ± 1.8 h per week | Participants: Increased PEDI mobility (p = 0.03). Decreased constipation (p = 0.02). Increased walking distance. Participants and Controls: Moderate association between increased BMD and increased weightbearing in stander or SSD. |
| van der Putten et al., 2005 [59] Peer-reviewed MMAT 3/5 COI and funding not reported | Participants: 32 GMFCS IV/V Mean 8.8 years Controls: 12 GMFCS IV/V Mean 10.6 years | Participants: 12 months MOVE® program including use of anterior support-arms SSD with sling seat Controls: 12 months regular education and therapy program | Both groups increased movement skill independence on TDMMT. MOVE®: 19.2 ± 13.5 to 22.8 ± 14.5. Controls: 20.2 ± 16.3 to 22.3 ± 19.2. Significant increase (p < 0.001) with moderate ES (0.69): MOVE® group. 4/12 controls improved. 20/32 MOVE® group improved. |
| Pre-post single group designs | |||
| Kuenzle and Brunner, 2009 [60] Peer-reviewed MMAT 4/5 Declared no COI Distributor involved in study conduct and planning | 45 GMFCS IV 48 GMFCS V Mean 7.6 years (1.8–18 years) | Hands-free orthotic SSD 88/93 completed 3-month evaluation: 1 deceased, 4 returned SSD Mean use: 0.8 h (0.2 to 2.5) day, 5 times per week (range 2–7) | 78 walked with little/no assistance; 10 used for dynamic standing only. Distance: 98.5 m ± 11.06 (2–463 m). Significant increase in walking abilities (WeeFIM) p < 0.001. Parents rated significantly increased mobility independence compared with no SSD (p < 0.001), but only hand function improved compared with previous device (p < 0.001). Goals for SSD met or exceeded: 81% parents and 86% therapists. Contraindications: hip/knee flexion contractures > 20 degrees; ankle dorsiflexion < 0 degrees. |
| Smati et al., 2022 [62] Peer-reviewed MMAT 4/5 Declared no COI Independent funding | 4 GMFCS III 5 GMFCS IV 6–11 years | 12-week, 50 min, 3 times per week intensive power training during school PE GMFCS IV used SSDs GMFCS III used walkers | Results for GMFCS IV only: HR/min 1.57 ± 0.72 to 0.95 ± 0.53. 10 MWT 15.62 ± 10.1 to 11.86 ± 5.65 s. 10 MFWT 10.32 ± 3.14 to 8.64 ± 3.42 s. 50 MST 67.4 ± 34.63 to 50.4 ± 17.78 s. 6-min walk endurance 162.75 ± 44.46–269.77 ± 88.05 m. Greatest change: children 6, 7, 8 yrs. 10, 11 yr. old results relatively stable. |
| Wright and Jutai, 1999 [18] Peer-reviewed MMAT 4/5 Independent funding | 5 GMFCS IV 15 GMFCS V 7.9 ± 2.9 years | Hands-free orthotic SSD for 12 months Initial use: 30 min daily Mean use from 2–12 months: 322 min ± 190.5 per week (range 92.5–860) | Significant increase (p = 0.006) in GMFM walk run jump (WRJ) score in SSD from 2–12 months: 6.1 ± 6.1. DMA significant increase (p = 0.01) from 2–12 months: 6.6 ± 10.7. Significantly increased walking speed and distance (p < 0.05). PEDI mobility score increased mean 10% points (p = 0.04) with SSD introduction, then remained stable. PEDI social function increased 6% points ± 8.5 by 12 months. 6 children walked indoors and out; 6 within home and classroom; 7 used for standing and exercise. |
| Wright and Jutai, 2006 [61] Peer-reviewed MMAT 3/5 Independent funding | 9 GMFCS III 10 GMFCS IV Mean age at 36-month follow-up 10.7 ± 3.1 years 12 children > 12 years | Hands-free orthotic SSD | 13/20 still used as main SSD. 6/7 who discontinued were >12 years and had outgrown the device. For 12/13 still using this SSD: non-significant increases (<3% points) in GMFM stand or WRJ. DMA: significant increase in steering ability between 12 and 36 months: 12 to 28.6 (p = 0.02). Walking speed unchanged. PEDI caregiver assistance scale: mean gains in self-care (4; p = 0.52) and social function (6; p = 0.04) scales from 24–36 months. |
| Qualitative | |||
| Bradbury and Tierney, 2022 [63] Peer-reviewed MMAT 4/5 Declared no COI Independent funding | Parent of 1 GMFCS IV 10 PTs (Excluded 7 children and 5 parents at GMFCS II/III) | 1 GMFCS IV: ring style SSD PTs discussed varied SSDs | Child safety, comfort, and happiness influence parent use of SSDs. PTs split between valuing child function and participation and promoting gait pattern. Recommendation: prioritize participation and child/family goals. |
| McKeever et al., 2013 [64] Peer-reviewed MMAT 5/5 Independent funding | Parents of children 10 GMFCS IV 9 GMFCS III Mean 10.7 years ± 3.1 years | Hands-free orthotic SSD Parents interviewed 36 months after provision. 13 children still using this specific SSD | Theme 1. Bodily function, position, and comportment. Theme 2. Communication. Theme 3. Participation and inclusion. Theme 4. Freedom and independence. Parents report child appeared more able. They valued SSD for enabling social inclusion in daily life as much as enhanced independent mobility. |
| Rodriguez Costa et al., 2021 [65] Peer-reviewed MMAT 5/5 Declared no COI Independent funding | 2 parents, 2 educational professionals and 4 PTs interviewed regarding experiences using the low-cost hands-free SSD with four children at GMFCS IV # Mean age 8.75 ± 5.5 years at time of study Children started using SSD at age 3–6 years | Low-cost charity developed Hands-free SSD used for 2.5 ± 1 years | Theme 1. Emotional welfare: happiness, emotional regulation, and self-esteem. Theme 2. Physical well-being: improved fitness, bowel function, balance and walking. Theme 3. Social Enjoyment: integration with others, increased hand-use, and independent exploration. Conclusion: Using the SSD made the children happier, increased self-confidence and autonomy, and enhanced participation. |
| Mixed methods | |||
| Paananen, 2009 [66] Thesis MMAT 4/5 | GMFCS IV/V * 7 aged 3–6 years 5 aged 7–15 years | Hands-free orthotic SSD 7 used 4–6 months 1 used 7–9 months 4 used > 12 months Used 30 min to 2 h daily | Parents satisfied (score 4) or very satisfied (score 5) (QUEST 2.0). Device satisfaction 4.6 ± 0.93. Services satisfaction 4.02 ± 1.01. Most important factors: Effective: Satisfied (2/12) or very satisfied (10/12). Ease of use: only 5/12 satisfied. Comfort: Satisfied (3/12) or very satisfied (9/12). Children were motivated to use. 7/12 used for both standing and walking. Used indoors and out. Increased participation in family life and with other children at school. Physical and attention benefits. Negatives: difficulty with transfers. |
| Single-subject research: Multiple baseline design | |||
| Barnes et al., 2002 [67] Peer-reviewed | Case 3: 3.5 years; GMFCS V * Case 4: 9 years GMFCS IV * Excluded participants: Cases 1 and 2: Independent walking Case 5: did not use SSD | Anterior support-arms SSD with sling seat, as part of MOVE® intervention over 8–9 months: stepping data collected twice weekly Case 3: 15-week baseline; 37-week intervention Case 4: 20-week baseline; 32-week intervention Two years maintenance data | Case 3: Initially unable to weight-bear unless fully supported in stander. Unable to step in SSD or with adult support during baseline or intervention. Able to walk 100 ft in SSD in maintenance phase. Case 4: Progressed to walking 70 ft in SSD; 9 min 20 s after 30 trials; 4 min 54 s by trial 53. Child unavailable in maintenance phase. |
| Lancioni, 2005a [68] Peer-reviewed | GMFCS IV/V * Profound intellectual disability Case 1: 10.8 years Case 2: 47.7 years | Straddle style SSD with chest support, saddle, and foot divider. Modified with automatic step counter and microswitch technology to activate preferred stimuli on stepping. 5-min sessions, 3–4 times daily, 4–6 times per week | Steps counted in baseline (Case 1: 6; Case 2: 24 sessions) but preferred stimuli (e.g., music, lights, vibration) activated only during intervention. Significant increase (p < 0.01) in steps (Case 1: 24 to 103; Case 2: 70 to 194) and indices of happiness: (Case 1: 1 to 5; Case 2: 1 to 7) during intervention phases for both. |
| Single-subject research designs: ABAB | |||
| Lancioni et al., [69,70,71,72,73,74] Peer-reviewed 2005b [69] 2007a [70] 2007b [71] 2008 [72] 2010 [73] 2013 [74] | GMFCS IV/V *; 3 to 43 years; Mean 13.26 ± 10.26 years; Profound intellectual disability; 9/17 severe visual impairment Case 1: 13 years; 1 month [69] Cases 2, 3: 10 years; 8 years [70] Cases 4–7: 6.7 years; 8.9 years; 19.2 years; 41.2 years [71] Case 8: 3 years (AB only) [72] Case 9: 12 years [72] Cases 10–14: 5.6 years; 6.5 years; 7.2 years; 11.4 years; 10.1 (AB only) years [73] Cases 15–17: 10.5 years; 12 years; 34 years [74] | Ring walker SSD with saddle or sling seat Modified with automatic step counter and microswitch technology to activate preferred stimuli Intervention: 4.7 ± 0.82 (2–5) minutes 7.6 ± 7.74 (4–28) times per day Total sessions in each intervention phase: 133.6 ± 171.82 (33 to 873) | Significant increases (p < 0.01) in stepping, pushing or leg-foot movements in SSD and indices of happiness during intervention phases, with change of slope towards baseline during withdrawal phase. Cases 4 and 5: stepping significant at p < 0.05. |
| Case series and observational studies | |||
| Broadbent et al., 2000 [75] Peer-reviewed | GMFCS IV * Case 1: 9 years Case 2: 14.5 years Case 3: 8 years Case 4: 8 years | Study-specific hands-free orthotic SSD 1. 30 min 3 times per week 2. 2 h 4 times per week 3. 4 h 5 times per week 4. 40 min 2–4 times per week | Independent walking increased (body weight support %). 1. >400 m indoor/outdoor (37%). 2. 10–25 m indoors (81%). 3. >400 m indoor/outdoor (69%). 4. 100–400 m outdoors (63%). |
| Camallonga, 2010 [76] Thesis | 10 children, aged 1–4 years. 6 GMFCS IV 4 GMFCS V Age 18–52 months; children determined not to be candidates: 3 GMFCS IV, 3 GMFCS V; Level of Sitting Scale (LSS): LSS 2:1; LSS 3:3; LSS 8:1 Developmental age: 3 weeks to 3 months, 3 weeks | Hands-free orthotic SSD used in early intervention setting | Case 1: 29 months, GMFCS IV, LSS 4, dev. age 11 months. Case 2: 21 months, GMFCS IV, LSS 4 dev. age 7 months, 2 weeks. Case 3: 38 months, GMFCS V, LSS 3, dev. age 6 months. Case 4: 44 months, GMFCS IV, LSS 4, dev. age 18 months. Protocol for successful candidates: LSS 2–4; GMFCS IV/V; developmental age 6 months. 3/4 stepping to explore classroom. 1/4 mainly standing. All increased motivation, self-expression. |
| Gandarias Mendieta, 2012 [77] Conference paper Device distributor | 126 children < 18 years GMFCS IV/V 11 adults GMFCS IV/V 18–37 years | Longitudinal follow-up: hands-free orthotic SSD | GMFCS III: this SSD type limits their autonomy and function. GMFCS IV: achieve most functional stepping, indoor and outdoor use. GMFCS V: improved posture, head, and saliva control. Important for self-esteem. May use for dynamic standing and some can step. |
| Gandarias Mendieta, 2023 [86] Unpublished longitudinal clinical database, all new device users in Spain provided by author 16 January 2023 Device distributor | 40 GMFCS III/other conditions 105 GMFCS IV 180 GMFCS V Total GMFCS IV/V: 285 Includes population from previously reported 137 users [77] and 26 users from two independent studies [81,82] Contact lost: 27 users Deceased: 6 GMFCS V, 3 others | Longitudinal follow-up of hands-free orthotic SSD use from 2010 to 2022 Age: 12 months to 37 years Average age of introduction: 3–6 years Average use: 7 years GMFCS IV: 96 <18 years; 9 adults/105 GMFCS V: 142 <18 years; 38 adults/180 | Current users as of December 2022: 37 GMFCS IV and 74 GMFCS V. Aged 2–34 years: mean 13 years. Able to step: 32 GMFCS IV and 63 GMFCS V. Using other SSD: 37 GMFCS IV and 4 GMFCS V. No longer using due to poor health: 5 GMFCS IV and 42 GMFCS V. Outgrown size: 33 GMFCS IV and 48 GMFCS V. |
| Livingstone et al., 2023 [78] Manuscript under review COI reported Unfunded | 8 GMFCS III 15 GMFCS IV 19 GMFCS V 47.74 months ± 14.71 months | SSD use over 6 months Baseline: III:6/8 IV:13/15 V:13/19 6 months: III: 8/8 IV:14/15 V:14/19 | SSD type according to GMFCS: III: 6 Convertible; 2 Support-arms. IV: 9 Support-arms; 5 Hands-free. V: 12 Hands-free; 2 Support-arms. No significant change in SSD use over 6 months. Power mobility introduction did not reduce SSD use at any GMFCS level. |
| Low, 2005 [79] Conference abstract | 39 severe multiple disabilities >50% GMFCS IV/V * Mean 9.2 years (3.5–13 years) | Anterior support-arms SSD with sling seat as part of MOVE® program over 1 year | 31/39 increased mobility level 1/39 independent walking. Increased independence in sitting, standing, and walking for all ages. Increased alertness and ease-of-care. |
| Low et al., 2011 [80] Conference abstract | 9 GMFCS IV 1 GMFCS V 7.5 ± 3.3 years | Comparison of *anterior support-arms SSD and *posterior hands-free SSD after 1 week trial in each | No significant group differences in gait speed/quality. Both SSDs improved upright mobility. For 6/10 new to SSDs, walking speed/gait quality better in hands-free SSD. 6 families preferred anterior. SSD: ease of transfers and use. |
| Martin Gomez et al., 2012 [81] English translation Manufacturer web publication | 7 GMFCS IV 19 GMFCS Mean 10.2 years | Hands-free orthotic SSD Mean use: 8.5 h per week for 25.5 months | Typical user is GMFCS V. 20/26 parents were very satisfied. QUEST 2.1 mean score 4.29 (2.4–6.3). |
| Martin Gomez et al., 2021 [82] Conference abstract | 19/26 GMFCS IV/V followed longitudinally since 2012 analysis | Hands-free orthotic SSD Mean use 5.2 years Range 2–9 years | 1/19 still using device. Reasons for discontinuation: increased deformity (13); size (3); improved abilities (2); time (1). QUEST 2.1 mean 3.12 (1.2–5.3). |
| Paleg, 1997 [83] Conference abstract | 19 GMFCS IV/V # Unable to sit, stand or walk Mean 6 years (2–14) | Anterior support-arms SSD as part of one-week intensive in-patient 20-h program based on MOVE® | 18/19 children able to reciprocally step more than 19 feet in SSD. 11/19 maintain head control 30 s in upright supported sitting. 8/19 maintain hip and knee extension 30 s. |
| Sharma and Bajracharya., 2022 [84] Peer reviewed Declared no COI Funding declared | 5 GMFCS II-IV Results here reported for: 3 GMFCS IV # Case 1: 8 years Case 2: 7 years Case 3: 6 years | Examined feasibility and parent satisfaction with a low-cost hands-free SSD: modified standard 4-wheel reverse walker by adding circumferential trunk support and sling seat | # Parents quite/very satisfied: QUEST 2.0 total 4.85 ± 0.25. Most important items: dimensions: 4.85 ± 0.25; ease of use: 5/5; effectiveness: 4 ± 1. All able to take a few steps hands-free. Case 1 able to play ball games and drink independently in SSD. Modification: feasible option for lower-resourced settings. |
| Wright-Ott, 2018 [85] Web Publication | 29 children 3–10 years 1 GMFCS III 5 GMFCS IV 20 GMFCS V 3 unknown genetic | Hands-free SSDs Preschool aged children; used 30–60 min daily Elementary aged children; used 15 min daily in recess and 30 min 3 times per week in gym and math/science | Teacher, family, and therapist observations: increased interaction with peers, visual attention, self-initiated behavior, problem solving, engagement, upper extremity use, physical motor control and communication. |
| Cross-sectional: Descriptive | |||
| George et al., 2020 [87] Peer-reviewed Declared no COI No funding | UK SSD prescribers (105 PTs, 1 OT, 1 PT aide) and 18 non-prescribers (worked with children using SSDs: PT, OT, education staff) | Prescribers/non-prescribers familiar with a wide range of SSD types. Most commonly prescribed SSDs were: anterior support-arm with sling seat (95/107); anterior-posterior with saddle seat (42/107) and posterior hands-free (38/107). Prescribed use: as much as able (53/107); <30 min (6/107); 30–60 min (34/107); >1 h (14/107) Actual use: <10 min (1/17); 10–30 min (6/17); 30–60 min (6/17); >1 h (4/17) Mean use: 2–5 years (1–10+) | Mean age of introduction 3.6 ± 1.6 years. Youngest age 2.4 ± 1.4 years, dependent on condition, cognition, motivation and motor ability. Conflict between early SSD use as bridge to independent walking or when other options unsuccessful. Contraindications: lack of head control, pain, behavioral problems. Most common reason for discontinuing use: functional deterioration. Challenges: lack of staff, space, or child prefers other mobility method. Top benefits: prescribers: physical activity, enjoyment, participation. Non-prescribers: independence, physical activity, enjoyment. <20% children progress to using hand-held walkers. |
| Low et al., 2011 [88] Peer-reviewed Declared no COI | 513 US pediatric PTs who used SSDs | Commonly prescribed SSDs: anterior support-arms with sling seat (402/513); suspension posterior walker (360/513); anterior support-arms with solid seat (329/513); posterior hands-free (46/513) Time used: <5 h/week (42%); 5–10 h/week (63%); >10 h/week (74%) Duration of use: <6 months (36%); 6 months–1 year (20%); 1–2 years (12%); >2 years (15%) | Factors influencing success: GMFCS level, motivation to walk, and cognition. Commonly recommended to increase exercise. Used in both posterior (65%) and anterior (53%) configurations. PTs consider hip stability, respiratory, and cardiovascular function and BMD when prescribing SSDs. Use of SSDs encouraged through participation with peers and school activities and within ADL activities. 30–50% children progress to walking with hand-held walkers. |
| Peredo et al., 2010 [89] Peer-reviewed Declared no COI | 52 children with CP (GMFCS not reported) as part of survey of medical device use in 108 children with disabilities | Unspecified SSD | 10/52 CP used SSDs, 11/52 used walkers. One other child/108 with a genetic condition used an SSD. 4/11 with SSD never used them, 2 used weekly, and 5 used daily. |
| Roquet et al., 2018 [14] Peer-reviewed Declared no COI Independent funding | 234 GMFCS IV/V 65 aged 2 to 17 years 170 aged 18 to >40 years | Examine change in health-care use for individuals with CP in one region in northern France by age and GMFCS | Use of gait aids (unspecified) is stable but limited. 14–19% across all age groups for GMFCS IV/V. In comparison 68% ≤17 years use standing frames with decline to 16% at 18–24 years and 7% ≥25 years. |
| Case reports | |||
| Altizer and Paleg, 2020 [90] Periodical | GMFCS IV 6 years | Hands-free SSD used daily from 12 months | SSD used to walk with support for exercise. Helps maintain fitness and participation with friends at the playground, store, and at school. Power mobility for longer distances. |
| Benson, 2020 [91] Book chapter | GMFCS IV 4 years | Unspecified SSD used daily in school | Used for free movement within the classroom and for short distances in school. Required power mobility for independence over longer distances. |
| Carnevale, 2015 [92] Conference paper | GMFCS IV 8 years | A. Anterior support-arms SSD B. Posterior hands-free SSD for 12 months C. Anterior SSD with hand holds | Anterior support-arms SSD: bore all weight on arms and dragged feet. Posterior hands-free SSD with full trunk support introduced: Over 12 months, learned to walk in upright position. Anterior orientation re-introduced: able to use hands for steering rather than for support. |
| Farrell et al., 2010 [93] Peer-reviewed Declared no COI | GMFCS IV * 10 years | Anterior support-arms SSD with sling seat 30 min, 3–5 times per week: 4 weeks in-patient program | Able to walk 150 feet with steering assistance. Increased weightbearing, weight shift and decreased hip flexion during stance. Increased GMFM (from 29.62 to 38.45) and PAM scores. Improved standing transfers and bed mobility. |
| George, 2018 [94] Peer-reviewed COI reported | GMFCS IV # 6 years Excluded: cases 2 and 3: not using SSD | # Anterior support-arms SSD with solid seat Stander with side-to-side rocking base 10 min 3–5 times per week for 6 weeks | TDMMT overall, standing, and walking scores improved from level 3 (dependent) to level 2 (walks 10 m with assistance). GAS-Light: consistently initiates and steps continuously over 10 m. Increased reciprocal stepping. |
| Gordon, 2023 [102] Book chapter online video cases | Case 1: GMFCS IV 3 years Case 2: GMFCS V 3 years | Hands-free SSD Daily use from 9 months | Case 1: Participation in family routines, improved hand use and play with siblings. Case 2: Limited active stepping and propulsion with assistance. Increased motivation and participation in gym games with other children in preschool. |
| Jones, 2020 [95] Book chapter | GMFCS IV 3 years | Hands-free SSD | Able to take steps and walk short distances (up to 25 feet) inside the home. Power wheelchair prescribed to keep up with peers outdoors. |
| Kannegießer-Leitner (undated) [103] Manufacturer web publication | Case 1: GMFCS IV/V * 4 years Case 2: GMFCS IV * 22 years Case 3: GMFCS V * 16 years | Hands-free orthotic SSD | Case 1: Improved posture, able to step independently. Increased participation with family. Case 2: Motivated to walk 2–4 km daily. Increased sense of autonomy. Case 3: Enjoys going for a walk outside after school 1.5–2 km daily. |
| Low, 2004 [96] Conference abstract | GMFCS IV * 12 years | Anterior support-arms SSD compared with previously used posterior hands-free SSD | Improved gait quality in anterior SSD. Easier transfers and increased mobility at home and school. |
| Paleg, 1997 [97] Periodical | Spastic diplegia GMFCS IV # 5–9 years | Anterior support-arms SSD with sling seat 4 years MOVE® program | Able to run in SSD, pull to stand, get up from floor with minimal assistance and sit independently. |
| Paleg, 1997 [104] Periodical | Case 1: dystonic quadriplegia GMFCS IV # 5 years Case 2: spastic quadriplegia GMFCS IV # 17 years | Anterior support-arms SSD with sling seat MOVE® program for 1 year Anterior support-arms SSD with sling seat MOVE® program | Able to walk all over school in SSD. He is happy, has friends, is communicating and able to feed himself. Able to take a few independent steps at age 17. Improved speech, bowel function, and self-esteem. |
| Paleg, 1998 [98] Periodical | Holoprosencephaly GMFCS IV # 3 years | SSD, stander, and classroom seat used 20 min each daily for one year | Able to sit to stand with hands held, maintains for 15 s, takes reciprocal steps for 10 feet in SSD. |
| Paleg, 2007 [99] Periodical | Joubert syndrome GMFCS IV # 3 years | Anterior support-arms SSD with solid seat used daily and PBWSTT 8 min 3 times per week from 12 months | 27 months: able to step forward and backwards in SSD with solid seat. 36 months: able to sit to stand and step taking partial body-weight in dynamic anterior sling seat SSD. |
| Pope et al., 2022 [100] Periodical | GMFCS V 5 years | # Anterior support-arms SSD with solid seat | Early upright positioning with stander. SSD for mobility and participation with siblings outdoors. |
| Schneiders (undated) [105] Manufacturer web publication | Several GMFCS V Starting at 18 months | Hands-free orthotic SSD | Alternate between active and static standing. Increased field of view and upright posture changes self-perception and perception of others. Increased self-determination: able to actively approach people or toys or communicate ‘no’ by moving away. Opportunity for motor and socio-emotional development. |
| Schwerin, 2005 [106] Conference abstract | 3 GMFCS IV 4–10 years | Hands-free orthotic SSD for 6 months following botulinum toxin injections to decrease scissoring | Increased trunk control and weightbearing. Improved communication, attention, exploration and independent activity. Caregiver support and space needed for implementation. |
| Thompson, 2005 [107] Book | Case 1: GMFCS IV * 12 years Case 2: GMFCS IV * 6 ½ years | Case 1. Anterior support-arms SSD with sling seat as part of MOVE® program for 2.5 years Case 2. Anterior support-arms SSD with sling seat as part of MOVE® program for 4 years | Case 1: Walks 500 ft in SSD. Increased independence on TDMMT. Increased peer participation. Case 2: Increased independence on TDMMT. Walks length of gym in SSD and practices sit to stand. Stands with two-hand support. Uses power wheelchair with supervision. |
| Whinnery et al., 2002 [101] Periodical | GMFCS IV * 4 years | Anterior support-arms SSD with sling seat daily 6 months MOVE® program | Average daily steps increased from 0 to 125. |
* Indicates GMFCS classified by review authors based on clinical descriptors. # Although not in the original publication, GMFCS classification or additional details were provided by study author(s). DMA: directional mobility assessment; ES: effect size; GAS: goal attainment scaling; GMFM: Gross Motor Function Measure; MOVE: Mobility Opportunities Via Education; m: meters; MMAT: Mixed Methods Appraisal Tool; PAM: Physical Abilities Measure; PEDI: Pediatric Evaluation of Disability Inventory; QUEST: Quebec User Evaluation of Satisfaction with assistive Technology; s: seconds; TDMMT: Top-Down Motor Milestone Test; w/o: without; yrs: years; 10 MWT: 10-m walk test; 10 MFWT: 10-m fast walk test; 50 MST: 50-m sprint test.
Table 3.
Expert opinion recommendations for use and benefits of stepping devices (SSDs) for GMFCS IV or V.
Table 3.
Expert opinion recommendations for use and benefits of stepping devices (SSDs) for GMFCS IV or V.
| Citation | Source | Topic | Comments or Recommendations for GMFCS IV or V |
|---|---|---|---|
| Bolton and Donohoe, 2020 [108] | Book chapter | Use of ambulatory assistive devices for children with CP | Can begin trial at 2 years with GMFCS IV/V Not useful for those with persistent flexor withdrawal response. |
| Covert, 2019 [109] | Periodical | Promote pediatric participation with standers, SSDs and wheeled mobility | SSDs can promote physical activity for GMFCS IV and possibly GMFCS V. When prescribing an SSD to promote participation and self-initiated mobility in the community, consider folding and ease of transportation. |
| Gandarias Mendieta, 2008 [110] | Manufacturer website translation of original Spanish language article | Use and benefits of hands-free orthotic SSD | For standing: promotes even weightbearing and slight movement in standing. Peer-level positioning increases participation with other children. For stepping: Promotes reciprocal gait, well-aligned posture, is stable and safe, increases child inclusion, participation and self-esteem. Contraindications: Difficult to turn: not suitable for children able to walk with posterior walker or with hands held. Contractures at hips or knees > 20 degrees. |
| Kannegießer- Leitner (undated) [103] | Manufacturer web publication | Benefits of hands-free orthotic SSD | Increases autonomy and independence for children requiring manual assistance to step. Reciprocating orthosis increases walking distance and reduces caregiver burden. Transfers may be modified for larger children by attaching trunk first, then knees and feet last. Beneficial for hip development. Others perceive child as more able. |
| Marquez, 2019 [111] | Periodical | Promoting function and independence in CP population | SSDs provide more support than walkers and can be used in anterior or posterior orientation. Maximize participation and independence rather than perfecting posture and gait mechanics. |
| Thunberg et al., 2021 [112] | Book chapter | Environmental modifications: for children with developmental motor disorders | Introduce SSDs around 12 months. SSDs promote upright positioning, active stepping and fitness, play, exploration and interaction. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Livingstone, R.W.; Paleg, G.S. Use of Overground Supported-Stepping Devices for Non-Ambulant Children, Adolescents, and Adults with Cerebral Palsy: A Scoping Review. Disabilities 2023, 3, 165-195. https://doi.org/10.3390/disabilities3020012
AMA Style
Livingstone RW, Paleg GS. Use of Overground Supported-Stepping Devices for Non-Ambulant Children, Adolescents, and Adults with Cerebral Palsy: A Scoping Review. Disabilities. 2023; 3(2):165-195. https://doi.org/10.3390/disabilities3020012
Chicago/Turabian StyleLivingstone, Roslyn W., and Ginny S. Paleg. 2023. "Use of Overground Supported-Stepping Devices for Non-Ambulant Children, Adolescents, and Adults with Cerebral Palsy: A Scoping Review" Disabilities 3, no. 2: 165-195. https://doi.org/10.3390/disabilities3020012