

The Pharmacological Class Alpha 2 Agonists for Stress Control in Patients with Respiratory Failure: The Main Actor in the Different Acts
 , ,
, ,
Abstract
:1. Introduction
2. Alpha 2 Agonists Drugs: Principles
2.1. Pharmacokinetics
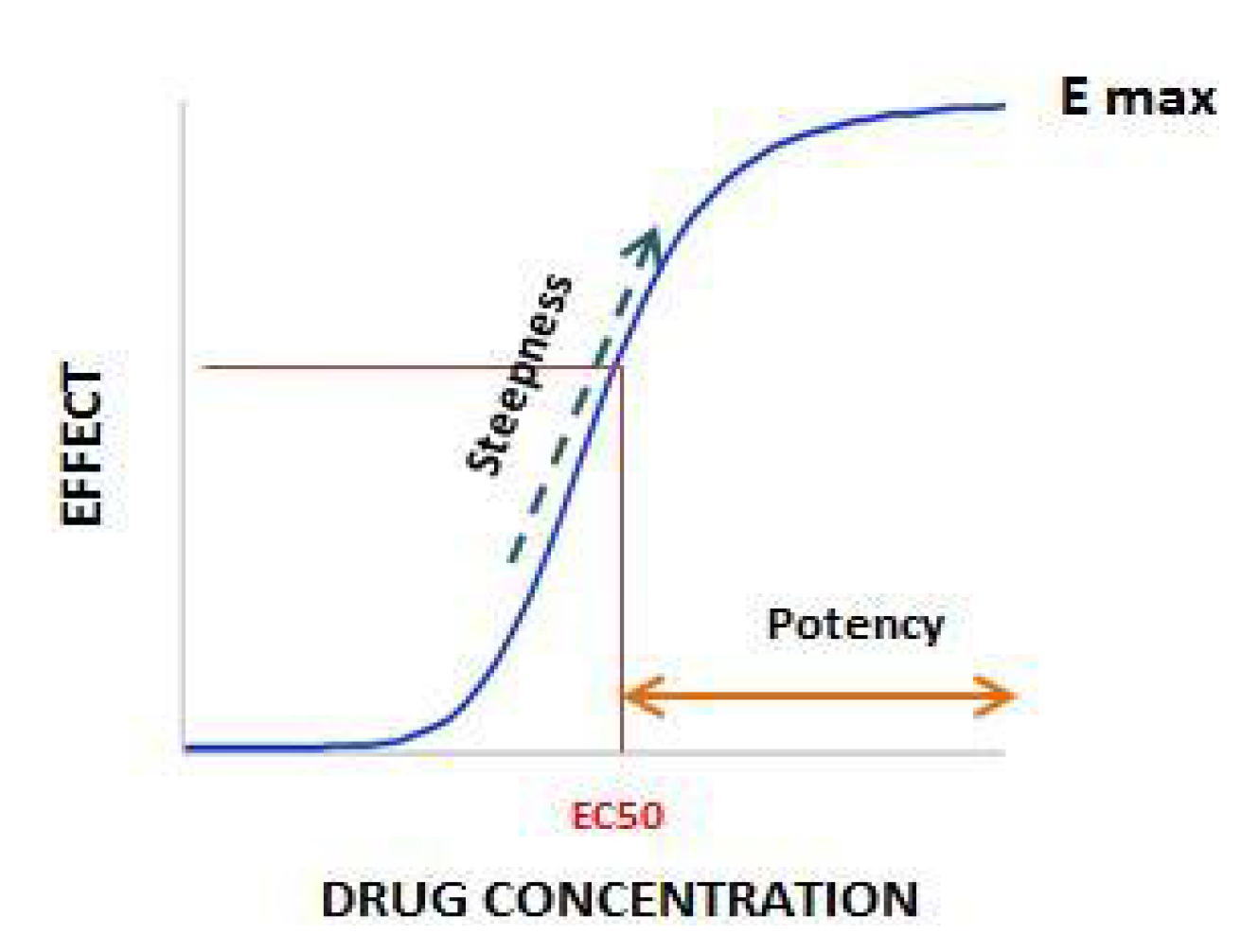
2.2. Pharmacodynamics Principles
2.2.1. The Receptors
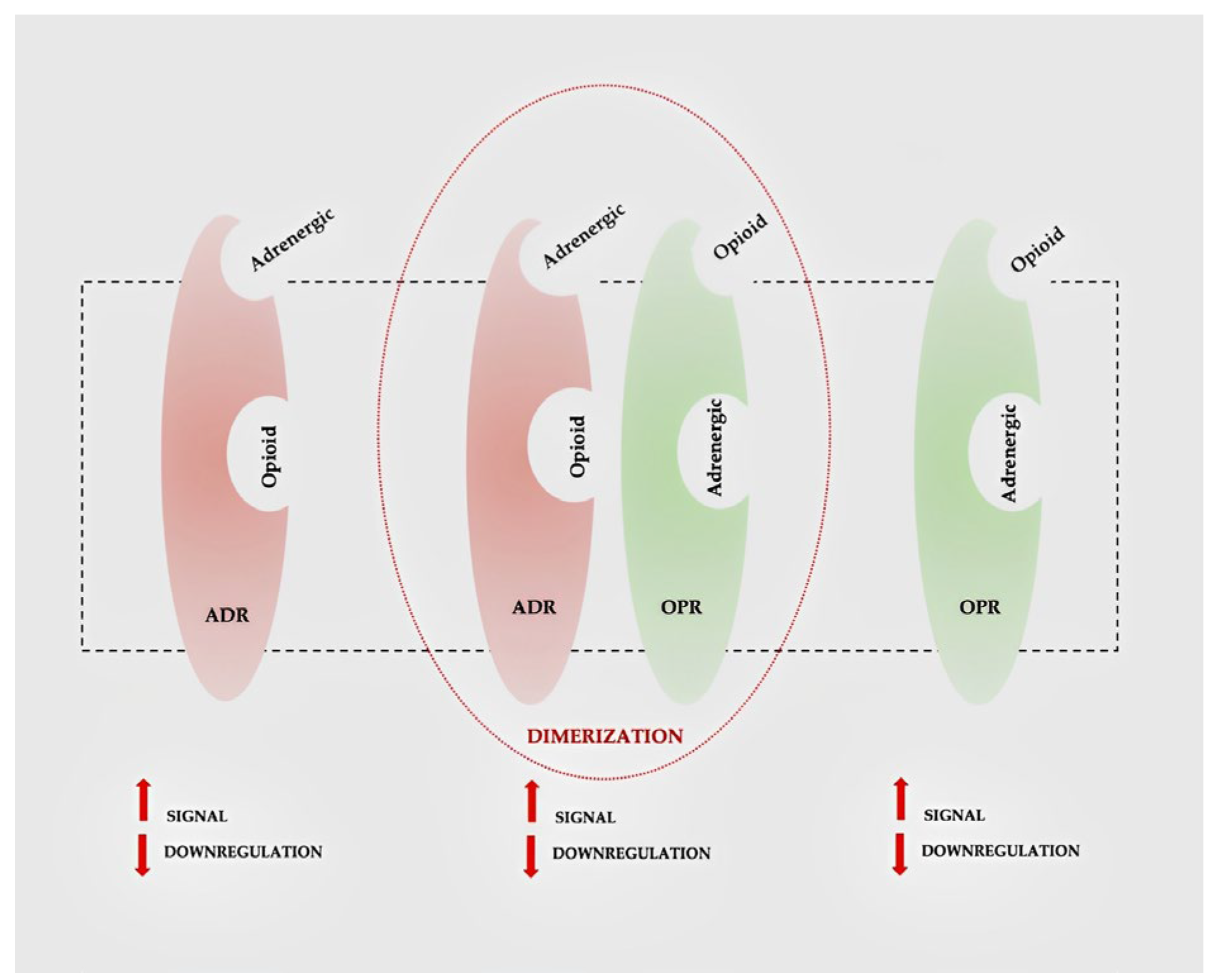
2.2.2. Drug Interactions
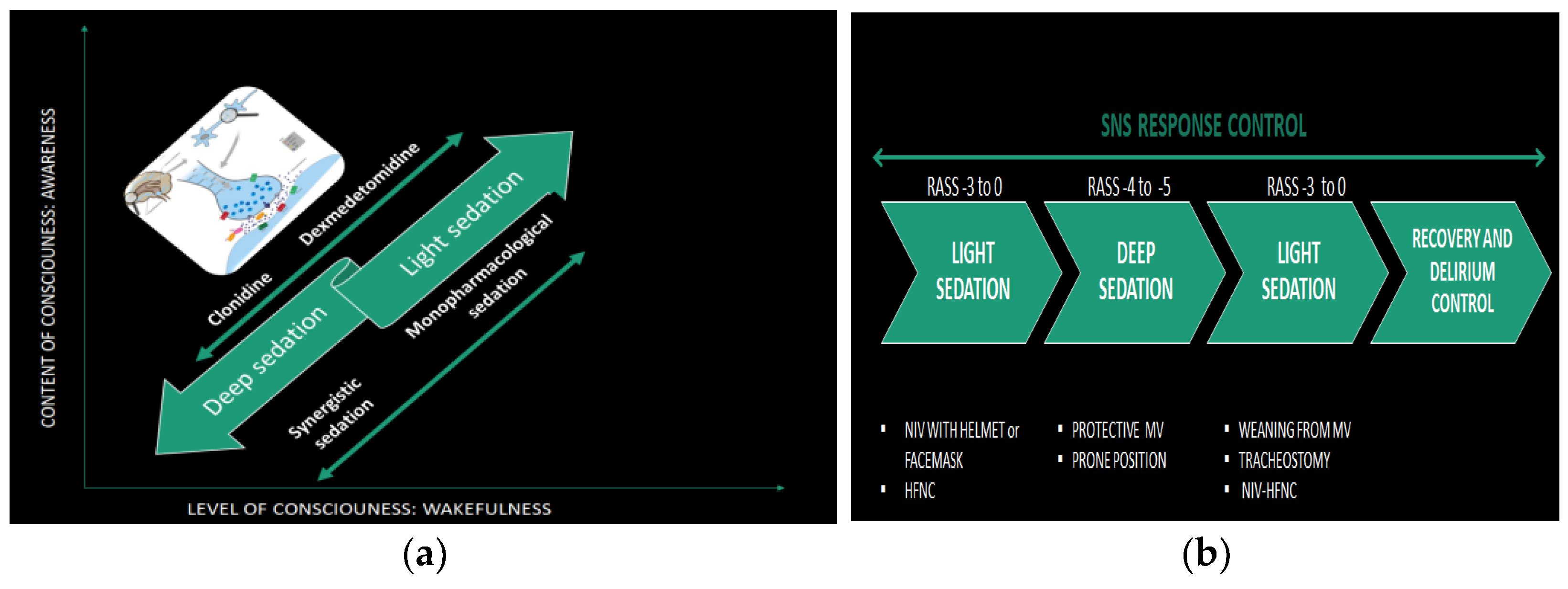
3. Pharmacological Scheme
4. Discussion
4.1. Alpha 2 Agonist Drugs: Fields of Application and Side Effects
4.2. Alpha 2 Agonist Drugs in Respiratory Failure
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carlson, D.E. Managing stress in critical illness. Crit. Care Med. 2012, 40, 3327–3328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dünser, M.W.; Hasibeder, W.R. Sympathetic Overstimulation During Critical Illness: Adverse Effects of Adrenergic Stress. J. Intensiv. Care Med. 2009, 24, 293–316. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovannitti, J.A.; Thoms, S.M.; Crawford, J.J. Alpha-2 Adrenergic Receptor Agonists: A Review of Current Clinical Applications. Anesth. Prog. 2015, 62, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Basler, S.; Singh, G.; Jacob, R. Clonidine in paediatrics—A review. Indian J. Anesth. 2009, 53, 270–280. [Google Scholar]
- Jamadarkhana, S.; Gopal, S. Clonidine in adults as a sedative agent in the intensive care unit. J. Anaesthesiol. Clin. Pharmacol. 2010, 26, 439. [Google Scholar] [CrossRef]
- Roberts, D.; Brown, J.; Medley, N.; Dalziel, S.R. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst. Rev. 2017, 3, CD004454. [Google Scholar] [CrossRef]
- Lee, S. Dexmedetomidine: Present and future directions. Korean J. Anesthesiol. 2019, 72, 323–330. [Google Scholar] [CrossRef]
- Weerink, M.; Struys, M.M.R.F.; Hannivoort, L.N.; Barends, C.R.M.; Absalom, A.R.; Colin, P. Clinical Pharmacokinetics and Pharmacodynamics of Dexmedetomidine. Clin. Pharmacokinet. 2017, 56, 893–913. [Google Scholar] [CrossRef] [Green Version]
- Zarfoss, E.L.; Garavaglia, J.; Hayanga, J.W.A.; Kabulski, G. Comparison of Standard-Dose Versus High-Dose Dexmedetomidine in Extracorporeal Membrane Oxygenation. Ann. Pharmacother. 2022. [published online ahead of print]. [Google Scholar] [CrossRef]
- Salahudeen, M.S.; Nishtala, P.S. An overview of pharmacodynamic modelling, ligand-binding approach and its application in clinical practice. Saudi Pharm. J. 2016, 25, 165–175. [Google Scholar] [CrossRef]
- Buchwald, P. A Receptor Model with Binding Affinity, Activation Efficacy, and Signal Amplification Parameters for Complex Fractional Response Versus Occupancy Data. Front. Pharmacol. 2019, 10, 605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pichot, C.; Ghignone, M.; Quintin, L. Dexmedetomidine and Clonidine. J. Intensiv. Care Med. 2011, 27, 219–237. [Google Scholar] [CrossRef] [PubMed]
- Chabot-Doré, A.-J.; Schuster, D.J.; Stone, L.S.; Wilcox, G.L. Analgesic synergy between opioid and α2-adrenoceptors. J. Cereb. Blood Flow Metab. 2014, 172, 388–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Root-Bernstein, R. Biased, Bitopic, Opioid–Adrenergic Tethered Compounds May Improve Specificity, Lower Dosage and Enhance Agonist or Antagonist Function with Reduced Risk of Tolerance and Addiction. Pharmaceuticals 2022, 15, 214. [Google Scholar] [CrossRef]
- Wang, J.G.; Belley-Coté, E.; Burry, L.; Duffett, M.; Karachi, T.; Perri, D.; Alhazzani, W.; D’Aragon, F.; Wunsch, H.; Rochwerg, B. Clonidine for sedation in the critically ill: A systematic review and meta-analysis. Crit. Care 2017, 21, 75. [Google Scholar] [CrossRef] [Green Version]
- Cruickshank, M.; Henderson, L.; MacLennan, G.; Fraser, C.; Campbell, M.; Blackwood, B.; Gordon, A.; Brazzelli, M. Alpha-2 agonists for sedation of mechanically ventilated adults in intensive care units: A systematic review. Health Technol. Assess. 2016, 20, 1–118. [Google Scholar] [CrossRef] [Green Version]
- Akeju, O.; Brown, E.N. Neural oscillations demonstrate that general anesthesia and sedative states are neurophysiologically distinct from sleep. Curr. Opin. Neurobiol. 2017, 44, 178–185. [Google Scholar] [CrossRef]
- Jain, A.; Lamperti, M.; Doyle, D.J. Dexmedetomidine: Another arrow in the quiver to fight COVID-19 in intensive care units. Br. J. Anaesth. 2020, 126, e35–e38. [Google Scholar] [CrossRef]
- Zhao, H.; Davies, R.; Ma, D. Potential therapeutic value of dexmedetomidine in COVID-19 patients admitted to ICU. Br. J. Anaesth. 2020, 126, e33–e35. [Google Scholar] [CrossRef]
- Lewis, K.; Alshamsi, F.; Carayannopoulos, K.L.; Granholm, A.; Piticaru, J.; Al Duhailib, Z.; Chaudhuri, D.; Spatafora, L.; Yuan, Y.; Centofanti, J.; et al. Dexmedetomidine vs other sedatives in critically ill mechanically ventilated adults: A systematic review and meta-analysis of randomized trials. Intensiv. Care Med. 2022, 48, 811–840. [Google Scholar] [CrossRef] [PubMed]
- Møller, M.H.; Alhazzani, W.; Lewis, K.; Belley-Cote, E.; Granholm, A.; Centofanti, J.; McIntyre, W.B.; Spence, J.; Al Duhailib, Z.; Needham, D.M.; et al. Use of dexmedetomidine for sedation in mechanically ventilated adult ICU patients: A rapid practice guideline. Intensiv. Care Med. 2022, 48, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Page, V.; McKenzie, C. Sedation in the Intensive Care Unit. Curr. Anesthesiol. Rep. 2021, 11, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Maggiore, S.M.; Roca, O.; Spinelli, E.; Patel, B.K.; Thille, A.W.; Barbas, C.S.V.; de Acilu, M.G.; Cutuli, S.L.; Bongiovanni, F.; et al. Non-invasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ARDS. Intensiv. Care Med. 2021, 47, 851–866. [Google Scholar] [CrossRef]
- Ely, E.W.; Truman, B.; Shintani, A.; Thomason, J.W.W.; Wheeler, A.P.; Gordon, S.; Francis, J.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Monitoring Sedation Status Over Time in ICU Patients. JAMA 2003, 289, 2983–2991. [Google Scholar] [CrossRef] [Green Version]
- Paternoster, G.; Sartini, C.; Pennacchio, E.; Lisanti, F.; Landoni, G.; Cabrini, L. Awake pronation with helmet continuous positive airway pressure for COVID-19 acute respiratory distress syndrome patients outside the ICU: A case series. Med. Intensiv. 2020, 46, 65–71. [Google Scholar] [CrossRef]
- Chen, K.; Lu, Z.; Xin, Y.; Cai, Y.; Chen, Y.; Pan, S. Alpha-2 agonists for long-term sedation during mechanical ventilation in critically ill patients. Cochrane Database Syst. Rev. 2015, 1, CD010269. [Google Scholar] [CrossRef]
- Shehabi, Y.; Howe, B.D.; Bellomo, R.; Arabi, Y.M.; Bailey, M.; Bass, F.E.; Bin Kadiman, S.; McArthur, C.J.; Murray, L.; Reade, M.C.; et al. Early Sedation with Dexmedetomidine in Critically Ill Patients. N. Engl. J. Med. 2019, 380, 2506–2517. [Google Scholar] [CrossRef]
- Shehabi, Y.; The SPICE III Study Investigators; Neto, A.S.; Howe, B.D.; Bellomo, R.; Arabi, Y.M.; Bailey, M.; Bass, F.E.; Bin Kadiman, S.; McArthur, C.J.; et al. Early sedation with dexmedetomidine in ventilated critically ill patients and heterogeneity of treatment effect in the SPICE III randomised controlled trial. Intensiv. Care Med. 2021, 47, 455–466. [Google Scholar] [CrossRef]
- Mehta, S.; Spies, C.; Shehabi, Y. Ten tips for ICU sedation. Intensiv. Care Med. 2017, 44, 1141–1143. [Google Scholar] [CrossRef]
- Cloesmeijer, M.E.; Oever, H.L.A.V.D.; Mathôt, R.A.; Zeeman, M.; Kruisdijk-Gerritsen, A.; Bles, C.M.; Nassikovker, P.; De Meijer, A.R.; Van Steveninck, F.L.; Arbouw, M.E. Optimising the dose of clonidine to achieve sedation in intensive care unit patients with population pharmacokinetics. Br. J. Clin. Pharmacol. 2020, 86, 1620–1631. [Google Scholar] [CrossRef] [PubMed]
- Shafer, S.L.; Hendrickx, J.F.A.; Flood, P.; Sonner, J.; Eger, I.E. Additivity Versus Synergy: A Theoretical Analysis of Implications for Anesthetic Mechanisms. Anesth. Analg. 2008, 107, 507–524. [Google Scholar] [CrossRef] [PubMed]
- Adams, C.D.; Altshuler, J.; Barlow, B.L.; Dixit, D.; Droege, C.A.; Effendi, M.K.; Heavner, M.S.; Johnston, J.P.; Kiskaddon, A.L.; Lemieux, D.G.; et al. Analgesia and Sedation Strategies in Mechanically Ventilated Adults with COVID-19. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- Buckley, M.S.; Smithburger, P.L.; Wong, A.; Fraser, G.L.; Reade, M.C.; Klein-Fedyshin, M.; Ardiles, T.; Kane-Gill, S.L. Dexmedetomidine for Facilitating Mechanical Ventilation Extubation in Difficult-to-Wean ICU Patients: Systematic Review and Meta-Analysis of Clinical Trials. J. Intensiv. Care Med. 2020, 36, 925–936. [Google Scholar] [CrossRef]
- Constantin, J.-M.; Godet, T.; James, A.; Monsel, A. A small step for sedation that may become a giant leap for critical care medicine. Anaesth. Crit. Care Pain Med. 2019, 38, 425–427. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Type | n | Drug | Results |
|---|---|---|---|---|
| Chen, 2015 [27] | Systematic review | 7 trials, 1624 pts | Dexmedetomidine/clonidine | Dexmedetomidine reduces duration MV and ICU length of stay. No evidence in reducing delirium and overall death rate. Slow heartbeat incidence is doubled. More studies are needed for clonidine |
| Cruickshank, 2016 [17] | Systematic review | 18 trials, 2489 pts | Clonidine/dexmedetomidine/propofol/ benzodiazepines | Evidence on the use of clonidine is very limited. Dexmedetomidine may be effective in reducing ICU length of stay and time to extubation. Risk of bradycardia, but not overall mortality, is higher among patients treated with dexmedetomidine. |
| Wang, 2017 [16] | Systematic review and metanalysis | 8 trials, 642 pts | Clonidine/other sedatives | Clonidine is a narcotic sparing agent but increases incidence of hypotension. Data on clonidine are insufficient. |
| Shehabi, 2019 [28] | Randomized controlled trial | 4000 pts | Dexmedetomidine/usual standard sedatives | Rate of death in dexmedetomidine is similar to standard care group, but more sedatives are required and more adverse effects occur. |
| Shehabi, 2021 [29] | Bayesan analysis of clinical trial | 3904 pts | Dexmedetomidine/ usual standard sedatives | Dexmedetomidine can reduce mortality in older patients and increase it in younger patients (≤65 years) with non post-operative status. |
| Page, 2021 [23] | Narrative review | Sedation literature over the 5 previous years | Dexmedetomidine/clonidine/other drugs | Except for dexmedetomidine, more attention in literature is required for other drugs. |
| Lewis, 2022 [21] | Systematic Review | 77 trials, pts | Dexmedetomidine/ GABAergic drugs | Dexmedetomidine use results in a lower risk of delirium and a modest reduction in duration of MV and ICU stay, but the risks of bradycardia and hypotension are increased |
| Score | Term | Description |
|---|---|---|
| +4 | Combative | Overtly combative, violent, immediate danger to staff |
| +3 | Very agitated | Pulls or removes tube(s) or catheter(s); aggressive |
| +2 | Agitated | Frequent non-purposeful movement, fights ventilator |
| +1 | Restless | Anxious but movements not aggressive or vigorous |
| 0 | Alert and Calm | |
| −1 | Drowsy | Not fully alert, but has sustained awakening (eye-opening/eye contact) to voice (>10 s) |
| −2 | Light sedation | Briefly awakens with eye contact to voice (<10 s) |
| −3 | Moderate sedation | Movement or eye opening to voice (but no eye contact) |
| −4 | Deep sedation | No response to voice, but movement or eye opening to physical stimulation |
| −5 | Unarousable | No response to voice or physical stimulation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Recchia, A.; Tonti, M.P.; Mirabella, L.; Izzi, A.; Del Gaudio, A. The Pharmacological Class Alpha 2 Agonists for Stress Control in Patients with Respiratory Failure: The Main Actor in the Different Acts. Stresses 2023, 3, 1-10. https://doi.org/10.3390/stresses3010001
Recchia A, Tonti MP, Mirabella L, Izzi A, Del Gaudio A. The Pharmacological Class Alpha 2 Agonists for Stress Control in Patients with Respiratory Failure: The Main Actor in the Different Acts. Stresses. 2023; 3(1):1-10. https://doi.org/10.3390/stresses3010001
Chicago/Turabian StyleRecchia, Andreaserena, Maria Pia Tonti, Lucia Mirabella, Antonio Izzi, and Alfredo Del Gaudio. 2023. "The Pharmacological Class Alpha 2 Agonists for Stress Control in Patients with Respiratory Failure: The Main Actor in the Different Acts" Stresses 3, no. 1: 1-10. https://doi.org/10.3390/stresses3010001