
Split-Belt Treadmill Training Improves Mechanical Energetics and Metabolic Cost in Women with Unilateral Hip Osteoarthritis: A Proof-of-Concept Study

Abstract
:1. Introduction
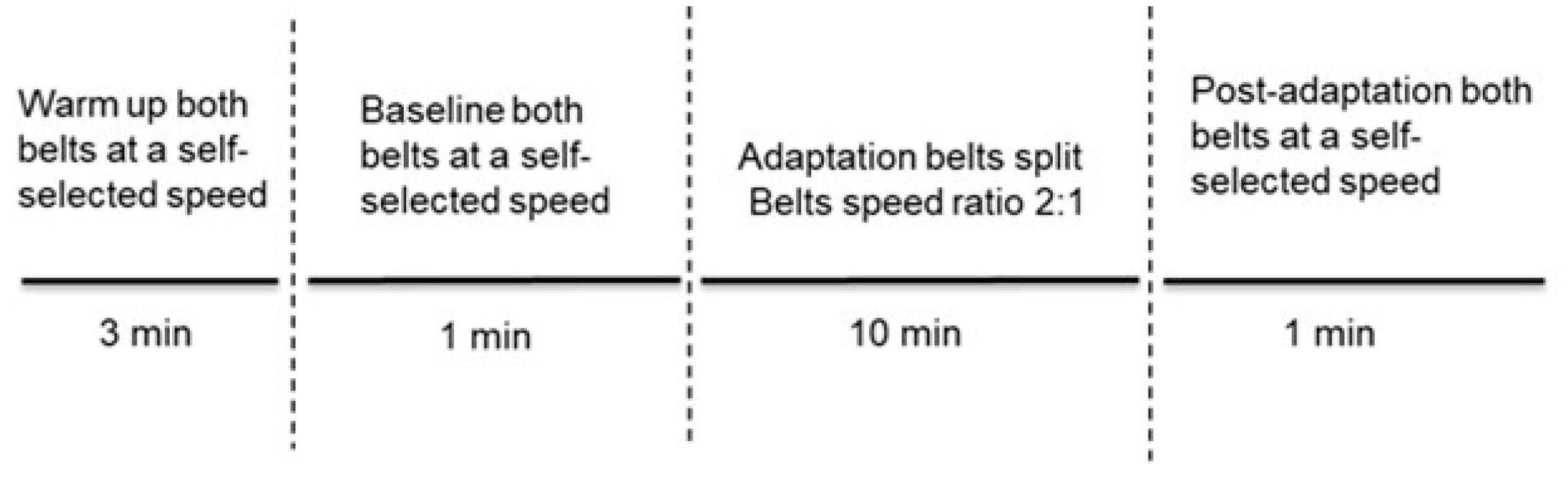
2. Materials and Methods
3. Results
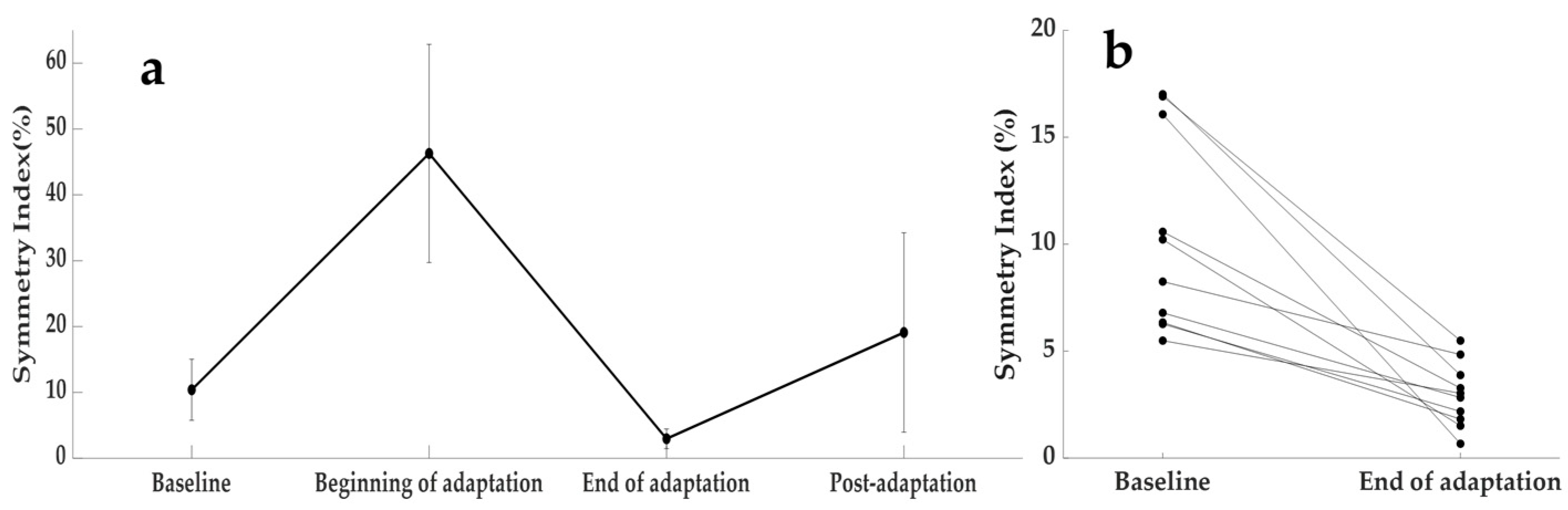
3.1. Changes in Step Length Asymmetry
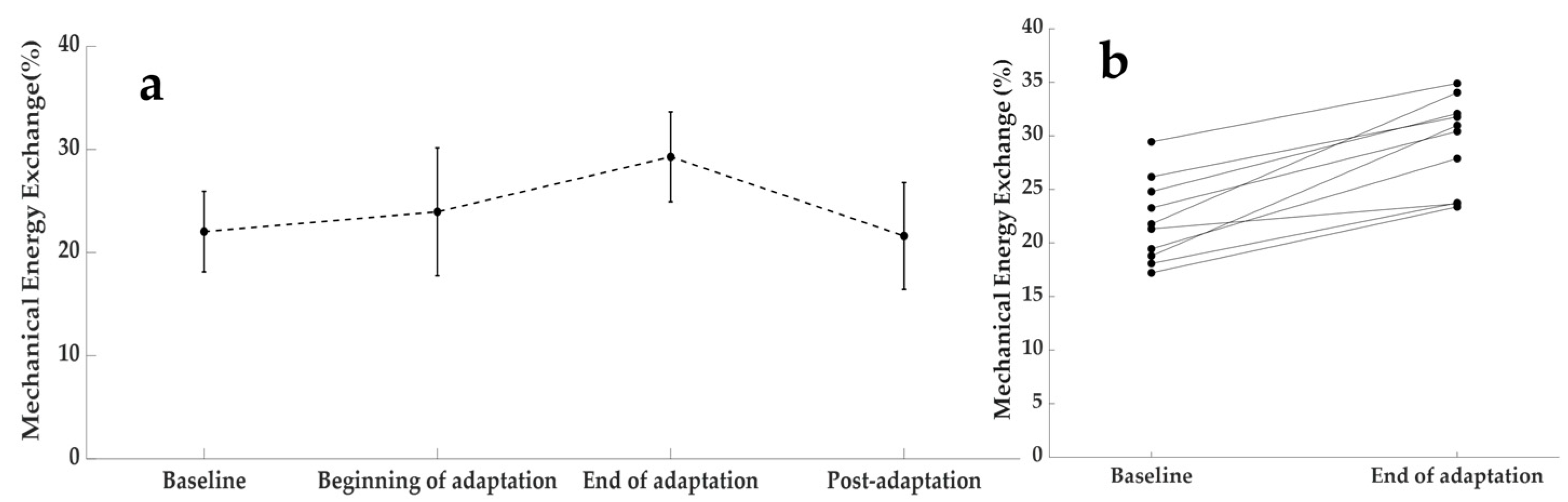
3.2. Changes in Mechanical Energy Exchange
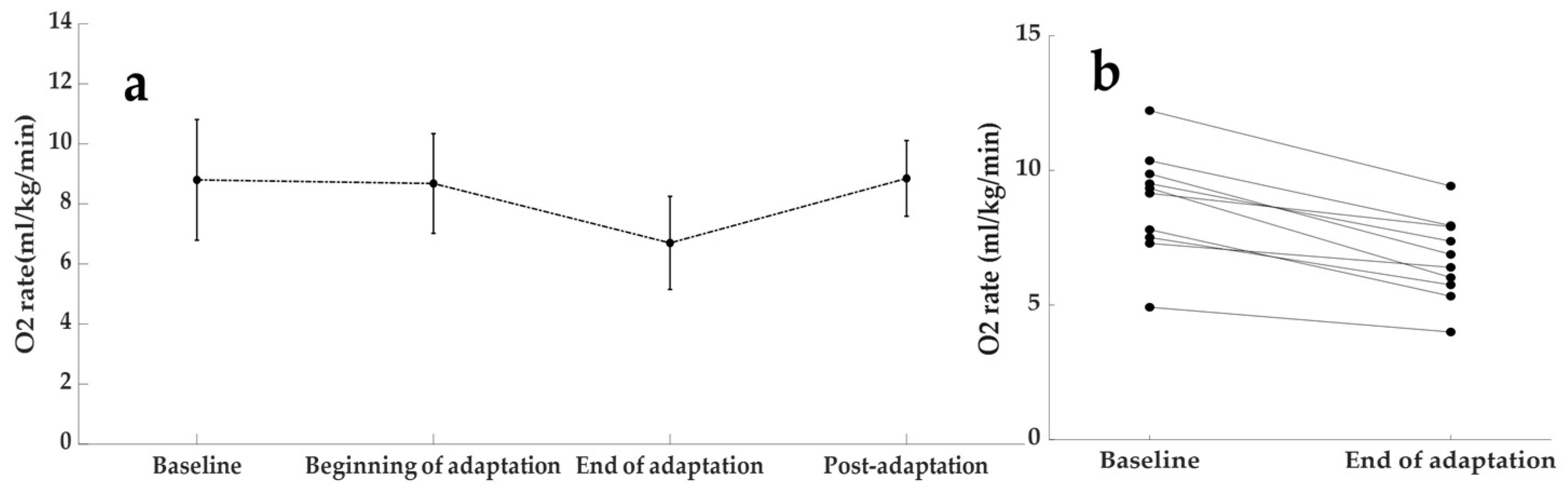
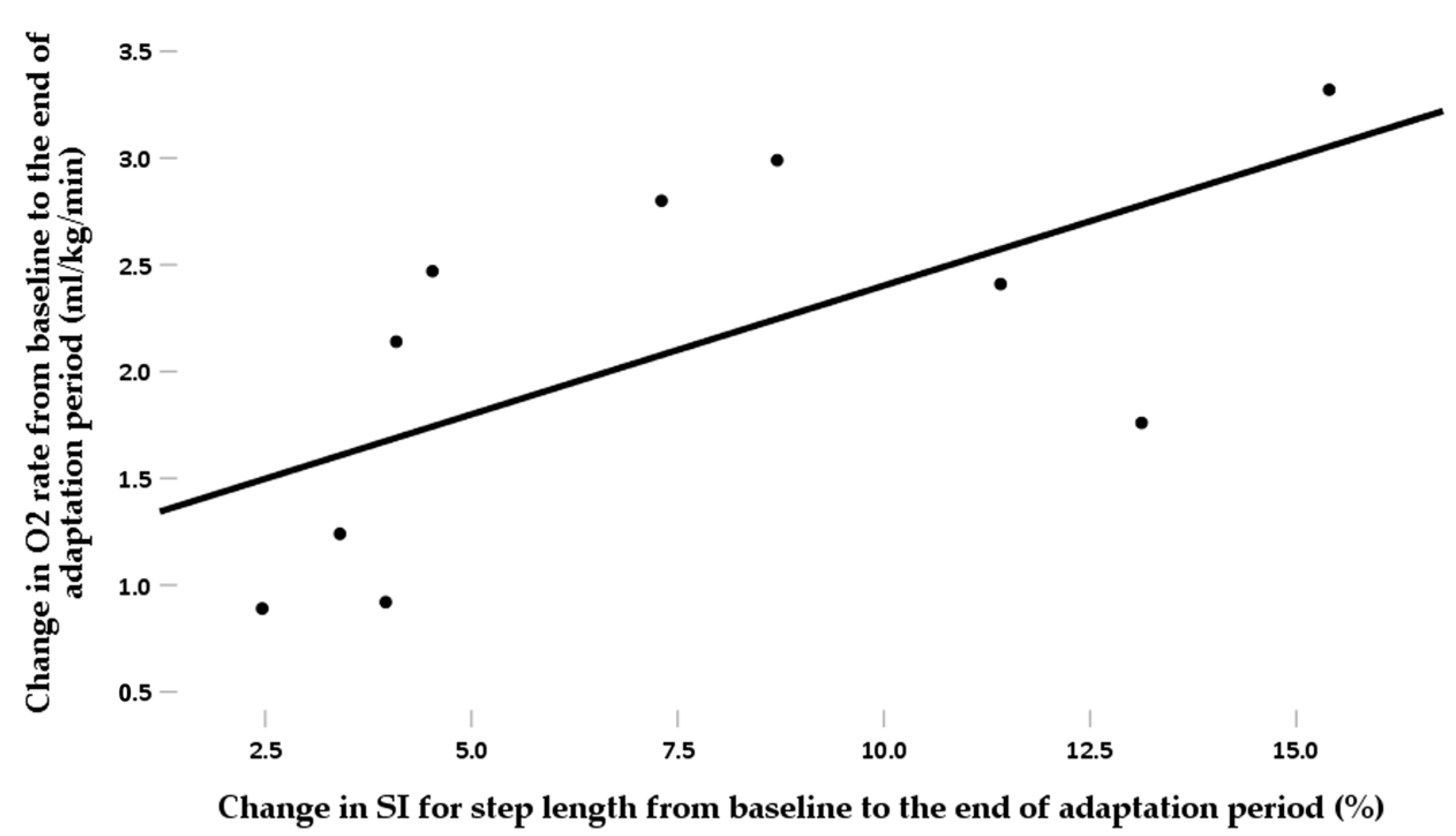
3.3. Changes in Oxygen Consumption
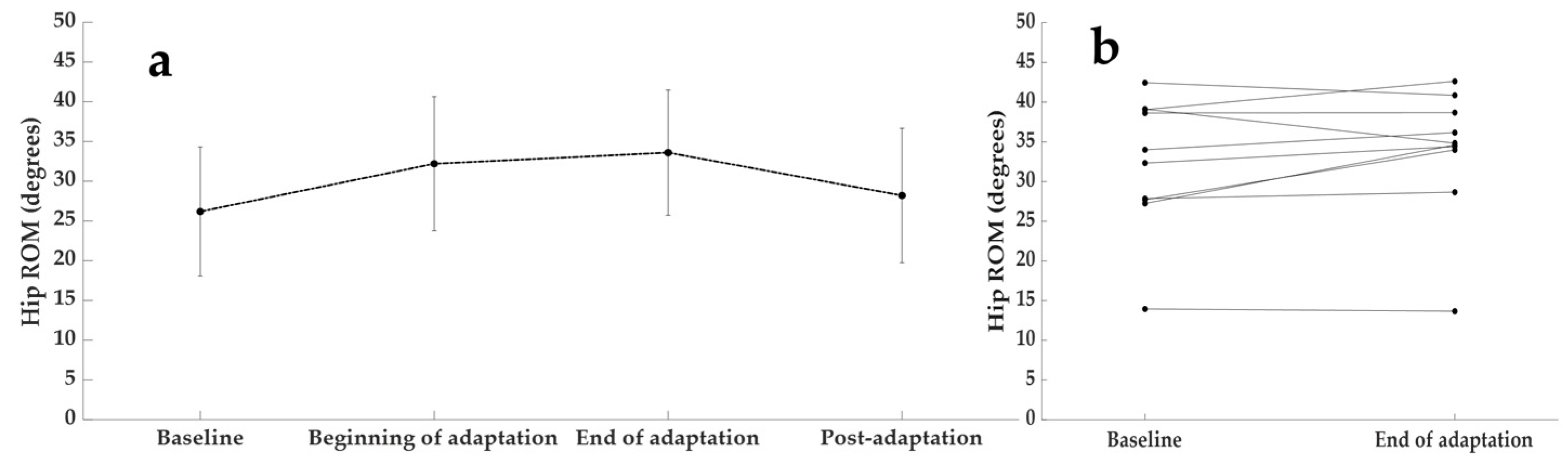
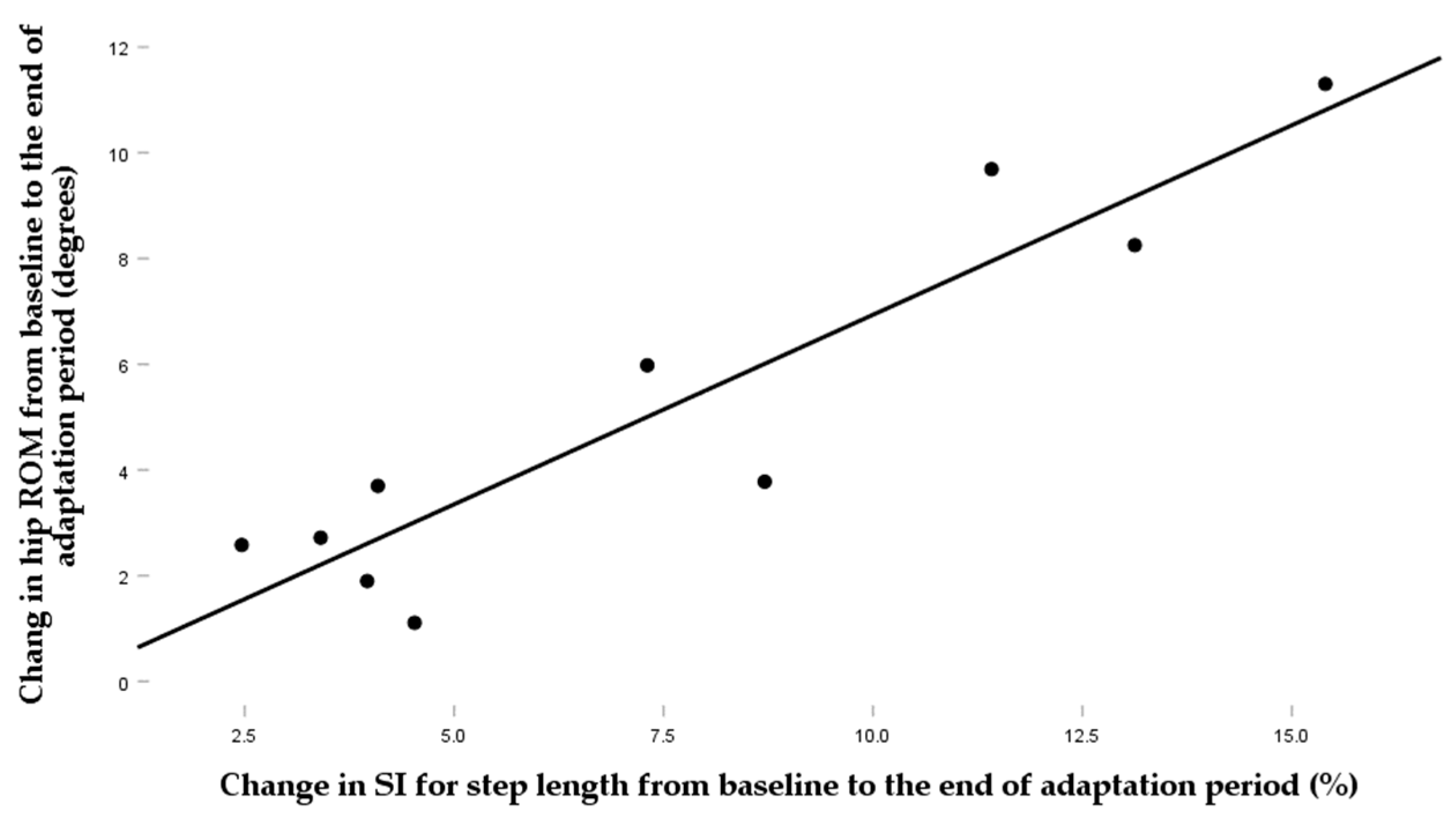
3.4. Changes in Hip Sagittal Plane ROM
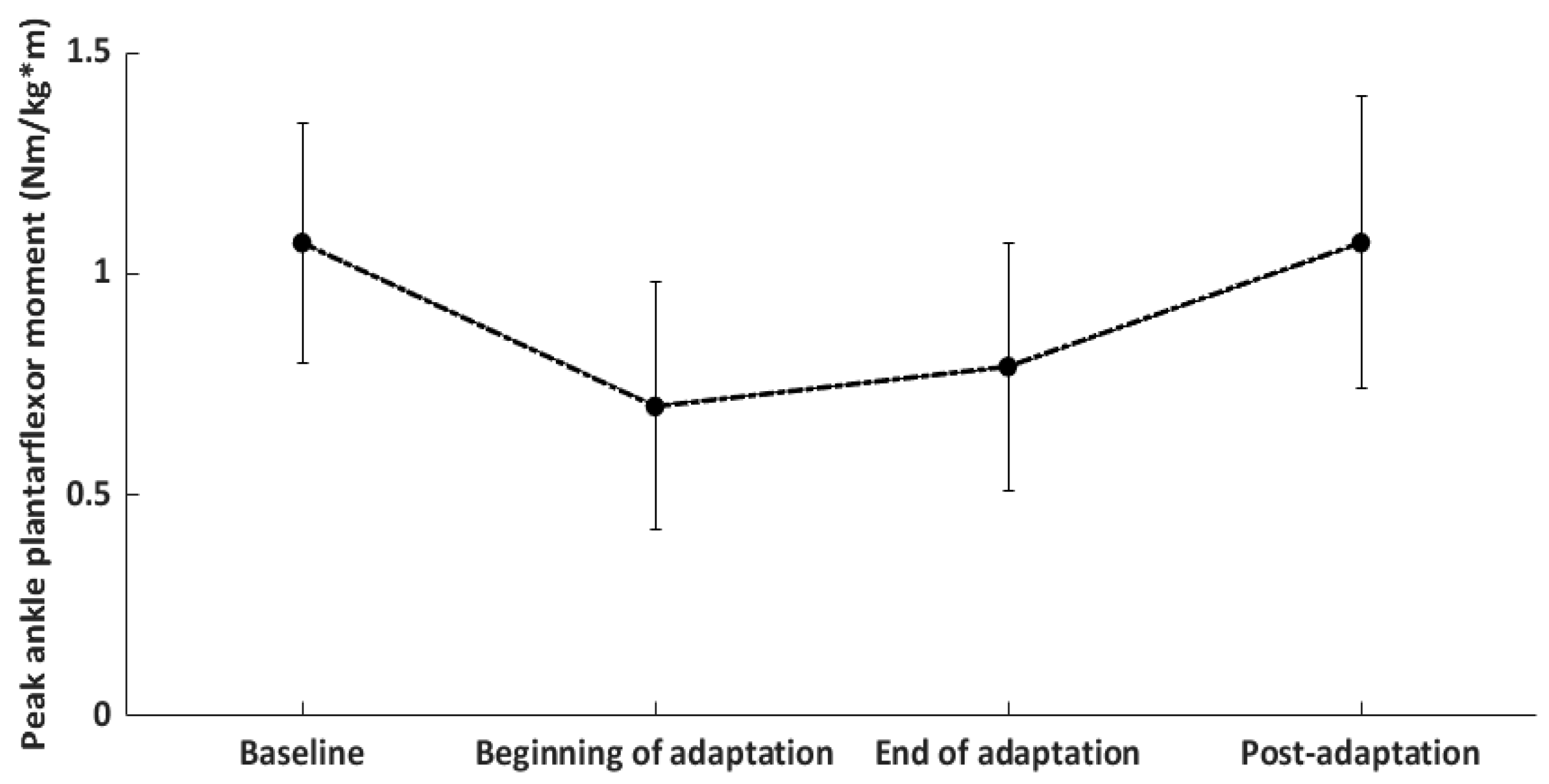
3.5. Changes in Peak Ankle Plantarflexor Moment during Push Off
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Bienias, J.L.; Bennett, D.A. Physical Activity Is Associated with Incident Disability in Community-Based Older Persons. J. Am. Geriatr. Soc. 2007, 55, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.; Boyle, P.; Yu, L.; Shah, R.; Wilson, R.; Bennett, D. Total daily physical activity and the risk of AD and cognitive decline in older adults. Neurology 2012, 78, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Kesaniemi, Y.K.; Danforth, E.; Jensen, M.D.; Kopelman, P.G.; Lefèbvre, P.; Reeder, B.A. Dose-response issues concerning physical activity and health: An evidence-based symposium. Med. Sci. Sports Exerc. 2001, 33, S351–S358. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.E.; Rejeski, W.J.; Reboussin, B.; Have, T.R.T.; Ettinger, W.H. Physical activity, functional limitations, and disability in older adults. J. Am. Geriatr. Soc. 2000, 48, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef]
- Kraus, V.B.; Sprow, K.; Powell, K.E.; Buchner, D.; Bloodgood, B.; Piercy, K.; George, S.M.; Kraus, W.E.; Physical Activity Guidelines Advisory Committee. Effects of Physical Activity in Knee and Hip Osteoarthritis: A Systematic Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1324–1339. [Google Scholar] [CrossRef]
- Wallis, J.; Webster, K.; Levinger, P.; Taylor, N. What proportion of people with hip and knee osteoarthritis meet physical activity guidelines? A systematic review and meta-analysis. Osteoarthr. Cartil. 2013, 21, 1648–1659. [Google Scholar] [CrossRef]
- Coyle, P.C.; Schrack, J.A.; Hicks, G.E. Pain Energy Model of Mobility Limitation in the Older Adult. Pain Med. 2017, 19, 1559–1569. [Google Scholar] [CrossRef]
- Foucher, K.C.; Huang, C.-H.; Aydemir, B. Walking energetics and abductor strength are associated with physical activity in older women with hip osteoarthritis. Gait Posture 2021, 85, 151–156. [Google Scholar] [CrossRef]
- Huang, C.-H.; Aydemir, B.; Jalasutram, A.; Kabir, I.; Foucher, K.C. Impact of step length asymmetry on walking energetics in women with hip Osteoarthritis: A pilot study. J. Biomech. 2021, 129, 110862. [Google Scholar] [CrossRef]
- Tateuchi, H.; Akiyama, H.; Goto, K.; So, K.; Kuroda, Y.; Ichihashi, N. Gait- and Posture-Related Factors Associated With Changes in Hip Pain and Physical Function in Patients With Secondary Hip Osteoarthritis: A Prospective Cohort Study. Arch. Phys. Med. Rehabil. 2019, 100, 2053–2062. [Google Scholar] [CrossRef]
- Constantinou, M.; Loureiro, A.; Carty, C.; Mills, P.; Barrett, R. Hip joint mechanics during walking in individuals with mild-to-moderate hip osteoarthritis. Gait Posture 2017, 53, 162–167. [Google Scholar] [CrossRef]
- Schmitt, D.; Vap, A.; Queen, R.M. Effect of end-stage hip, knee, and ankle osteoarthritis on walking mechanics. Gait Posture 2015, 42, 373–379. [Google Scholar] [CrossRef]
- Verlinden, V.J.; de Kruijf, M.; Bierma-Zeinstra, S.M.; Hofman, A.; Uitterlinden, A.G.; Ikram, M.A.; van Meurs, J.B.; van der Geest, J.N. Asymptomatic radiographic hip osteoarthritis is associated with gait differences, especially in women: A population-based study. Gait Posture 2017, 54, 248–254. [Google Scholar] [CrossRef]
- Vogt, L.; Banzer, W.; Bayer, I.; Schmidtbleicher, D.; Kerschbaumer, F. Overground and walkway ambulation with unilateral hip osteoarthritis: Comparison of step length asymmetries and reproducibility of treadmill mounted force plate readings. Physiother. Theory Pract. 2006, 22, 73–82. [Google Scholar] [CrossRef]
- Reisman, D.S.; Bastian, A.J.; Morton, S.M. Neurophysiologic and Rehabilitation Insights From the Split-Belt and Other Locomotor Adaptation Paradigms. Phys. Ther. 2010, 90, 187–195. [Google Scholar] [CrossRef]
- Reisman, D.S.; Wityk, R.; Silver, K.; Bastian, A.J. Locomotor adaptation on a split-belt treadmill can improve walking symmetry post-stroke. Brain 2007, 130, 1861–1872. [Google Scholar] [CrossRef]
- Reisman, D.S.; Wityk, R.; Silver, K.; Bastian, A.J. Split-Belt Treadmill Adaptation Transfers to Overground Walking in Persons Poststroke. Neurorehabilit. Neural Repair 2009, 23, 735–744. [Google Scholar] [CrossRef]
- Kline, P.W.; Davis-Wilson, H.C.; So, N.F.; Fields, T.T.; Christiansen, C.L. Feasibility of repeated session error-augmentation gait training for people with nontraumatic transtibial amputation. Prosthet. Orthot. Int. 2022, 46, 553–559. [Google Scholar] [CrossRef]
- Finley, J.M.; Bastian, A.J.; Gottschall, J.S. Learning to be economical: The energy cost of walking tracks motor adaptation. J. Physiol. 2013, 591, 1081–1095. [Google Scholar] [CrossRef]
- Reisman, D.S.; McLean, H.; Keller, J.; Danks, K.A.; Bastian, A.J. Repeated Split-Belt Treadmill Training Improves Poststroke Step Length Asymmetry. Neurorehabilit. Neural Repair 2013, 27, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.F.; Lamont, E.V.; Pang, M.Y.C. Split-Belt Treadmill Stepping in Infants Suggests Autonomous Pattern Generators for the Left and Right Leg in Humans. J. Neurosci. 2005, 25, 6869–6876. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Aydemir, B.; Foucher, K.C. Sagittal plane ankle kinetics are associated with dynamic hip range of motion and gait efficiency in women with hip osteoarthritis. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2022, 41, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Moisio, K.C.; Sumner, D.; Shott, S.; Hurwitz, D.E. Normalization of joint moments during gait: A comparison of two techniques. J. Biomech. 2003, 36, 599–603. [Google Scholar] [CrossRef]
- Lugade, V.; Wu, A.; Jewett, B.; Collis, D.; Chou, L.-S. Gait asymmetry following an anterior and anterolateral approach to total hip arthroplasty. Clin. Biomech. 2010, 25, 675–680. [Google Scholar] [CrossRef]
- Stagni, R.; Fantozzi, S.; Cappello, A.; Leardini, A. Quantification of soft tissue artefact in motion analysis by combining 3D fluoroscopy and stereophotogrammetry: A study on two subjects. Clin. Biomech. 2005, 20, 320–329. [Google Scholar] [CrossRef]
- Hallemans, A.; Aerts, P.; Otten, B.; De Deyn, P.P.; De Clercq, D. Mechanical energy in toddler gait A trade-off between economy and stability? J. Exp. Biol. 2004, 207, 2417–2431. [Google Scholar] [CrossRef]
- Cavagna, G.A.; Thys, H.; Zamboni, A. The sources of external work in level walking and running. J. Physiol. 1976, 262, 639–657. [Google Scholar] [CrossRef]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591. [Google Scholar] [CrossRef]
- Leys, C.; Ley, C.; Klein, O.; Bernard, P.; Licata, L. Detecting outliers: Do not use standard deviation around the mean, use absolute deviation around the median. J. Exp. Soc. Psychol. 2013, 49, 764–766. [Google Scholar] [CrossRef]
- Roemmich, R.T.; Leech, K.A.; Gonzalez, A.J.; Bastian, A.J. Trading Symmetry for Energy Cost During Walking in Healthy Adults and Persons Poststroke. Neurorehabilit. Neural Repair 2019, 33, 602–613. [Google Scholar] [CrossRef]
- Sánchez, N.; Park, S.; Finley, J.M. Evidence of Energetic Optimization during Adaptation Differs for Metabolic, Mechanical, and Perceptual Estimates of Energetic Cost. Sci. Rep. 2017, 7, 7682. [Google Scholar] [CrossRef]
- Sánchez, N.; Simha, S.; Donelan, J.M.; Finley, J.M. Taking advantage of external mechanical work to reduce metabolic cost: The mechanics and energetics of split-belt treadmill walking. J. Physiol. 2019, 597, 4053–4068. [Google Scholar] [CrossRef]
- Sánchez, N.; Simha, S.N.; Donelan, J.M.; Finley, J.M. Using asymmetry to your advantage: Learning to acquire and accept external assistance during prolonged split-belt walking. J. Neurophysiol. 2021, 125, 344–357. [Google Scholar] [CrossRef]
- Eitzen, I.; Fernandes, L.; Nordsletten, L.; Risberg, M.A. Sagittal plane gait characteristics in hip osteoarthritis patients with mild to moderate symptoms compared to healthy controls: A cross-sectional study (vol 13, 258, 2012). BMC Musculoskelet. Disord. 2015, 16, 52. [Google Scholar] [CrossRef]
- Steultjens, M.P.M.; Dekker, J.; Van Baar, M.E.; Oostendorp, R.A.; Bijlsma, J.W.J. Range of joint motion and disability in patients with osteoarthritis of the knee or hip. Rheumatology 2000, 39, 955–961. [Google Scholar] [CrossRef]
- Foucher, K.C. Sex-specific hip osteoarthritis-associated gait abnormalities: Alterations in dynamic hip abductor function differ in men and women. Clin. Biomech. 2017, 48, 24–29. [Google Scholar] [CrossRef]
- Allison, K.; Hall, M.; Wrigley, T.V.; Pua, Y.-H.; Metcalf, B.; Bennell, K.L. Sex-specific walking kinematics and kinetics in individuals with unilateral, symptomatic hip osteoarthritis: A cross sectional study. Gait Posture 2018, 65, 234–239. [Google Scholar] [CrossRef]
- Smith, L.K.; Lelas, J.L.; Kerrigan, D.C. Gender Differences in Pelvic Motions and Center of Mass Displacement during Walking: Stereotypes Quantified. J. Women’s Health Gender-Based Med. 2002, 11, 453–458. [Google Scholar] [CrossRef]
- Buurke, T.J.; Sharma, N.; Swart, S.B.; van der Woude, L.H.; Otter, R.D.; Lamoth, C.J. Split-belt walking: An experience that is hard to forget. Gait Posture 2022, 97, 184–187. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | SD | Range | Number |
|---|---|---|---|---|
| Age (years) | 64.7 | 6.2 | 56–76 | - |
| Height (m) | 1.59 | 0.09 | 1.50–1.73 | - |
| Weight (kg) | 81.33 | 19.59 | 56.7–119.29 | - |
| BMI (kg/m2) | 31.95 | 5.97 | 24.22–42.27 | - |
| Race White | - | - | - | 3 |
| Black or African American | - | - | - | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-H.; Aydemir, B.; Foucher, K.C. Split-Belt Treadmill Training Improves Mechanical Energetics and Metabolic Cost in Women with Unilateral Hip Osteoarthritis: A Proof-of-Concept Study. Biomechanics 2023, 3, 220-230. https://doi.org/10.3390/biomechanics3020019
Huang C-H, Aydemir B, Foucher KC. Split-Belt Treadmill Training Improves Mechanical Energetics and Metabolic Cost in Women with Unilateral Hip Osteoarthritis: A Proof-of-Concept Study. Biomechanics. 2023; 3(2):220-230. https://doi.org/10.3390/biomechanics3020019
Chicago/Turabian StyleHuang, Chun-Hao, Burcu Aydemir, and Kharma C. Foucher. 2023. "Split-Belt Treadmill Training Improves Mechanical Energetics and Metabolic Cost in Women with Unilateral Hip Osteoarthritis: A Proof-of-Concept Study" Biomechanics 3, no. 2: 220-230. https://doi.org/10.3390/biomechanics3020019