
Effect of Aging and Cortical Stroke on Motor Adaptation to Overground Gait-Slips: Quantifying Differences in Adaptation Rate and Adaptation Plateau
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Setup
2.3. Repeated-Slip Protocol
2.4. Data Collection and Analysis
2.5. Outcome Measures
2.5.1. Primary Outcome Measures
2.5.2. Secondary Outcome Measures
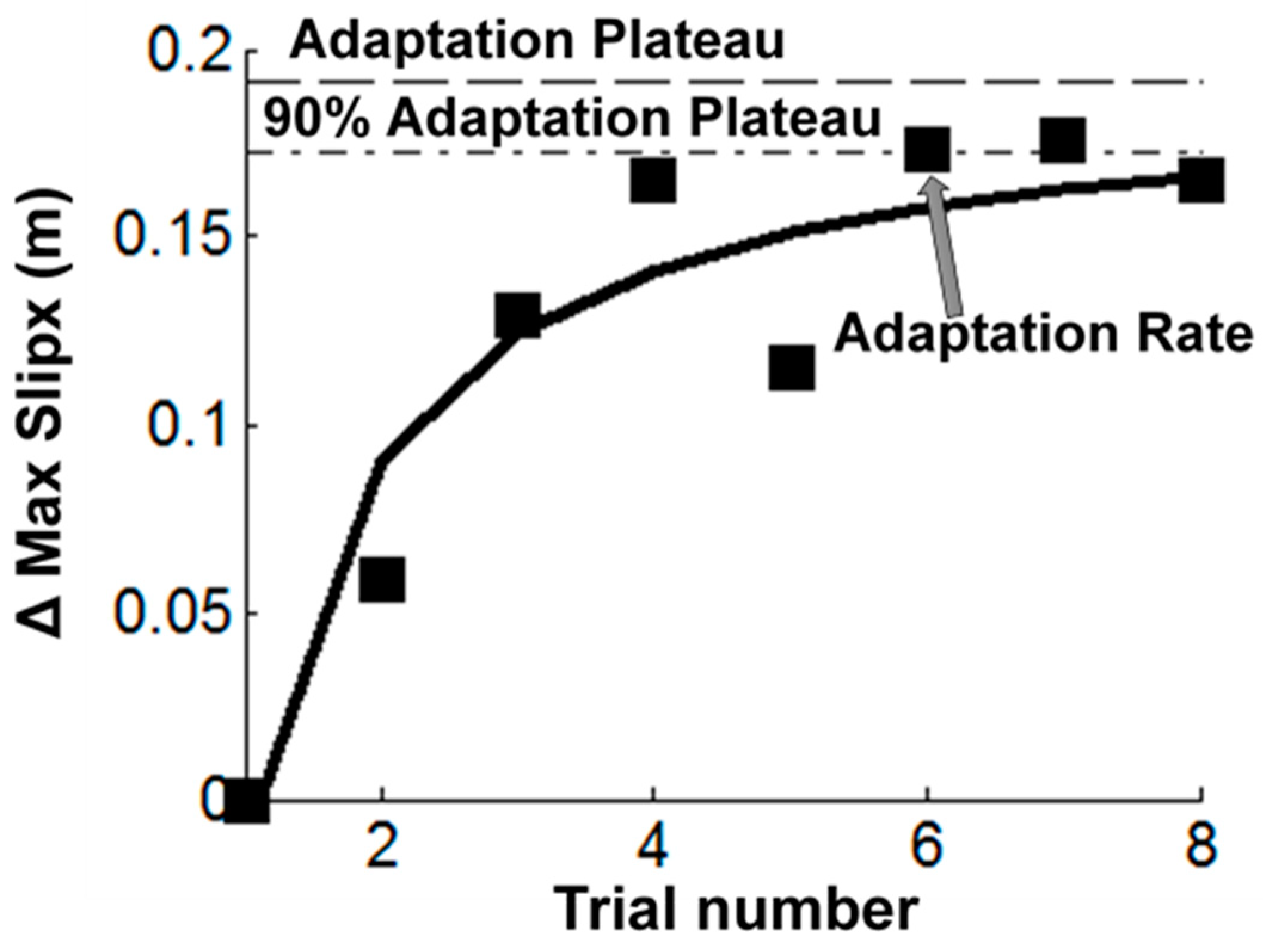
2.6. Adaptation Characteristics
2.7. Statistical Analysis
3. Results
3.1. Primary Outcome Measures
3.2. Secondary Outcome Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Tsao, C.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart disease and stroke statistics—2022 update: A report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics—2021 update: A report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; Djousse, L.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, S.F.; Goldie, P.; Hill, K. Falls incidence and factors associated with falling in older, community-dwelling, chronic stroke survivors (>1 year after stroke) and matched controls. Aging Clin. Exp. Res. 2005, 17, 74–81. [Google Scholar] [CrossRef]
- Simpson, L.A.; Miller, W.C.; Eng, J.J. Effect of stroke on fall rate, location and predictors: A prospective comparison of older adults with and without stroke. PLoS ONE 2011, 6, e19431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weerdesteijn, V.; Niet, M.D.; Van Duijnhoven, H.; Geurts, A.C. Falls in individuals with stroke. J. Rehabil. Res. Dev. 2008, 45, 1195–1213. [Google Scholar] [CrossRef]
- Schmid, A.A.; Yaggi, H.K.; Burrus, N.; McClain, V.; Austin, C.; Ferguson, J.; Fragoso, C.; Sico, J.J.; Miech, E.J.; Matthias, M.S.; et al. Circumstances and consequences of falls among people with chronic stroke. J. Rehabil. Res. Dev. 2013, 50, 1277–1286. [Google Scholar] [CrossRef]
- An, M.; Shaughnessy, M. The effects of exercise-based rehabilitation on balance and gait for stroke patients: A systematic review. J. Neurosci. Nurs. 2011, 43, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Kannan, L.; Vora, J.; Varas-Diaz, G.; Bhatt, T.; Hughes, S. Does Exercise-Based Conventional Training Improve Reactive Balance Control among People with Chronic Stroke? Brain Sci. 2020, 11, 2. [Google Scholar] [CrossRef]
- Lubetzky-Vilnai, A.; Kartin, D. The effect of balance training on balance performance in individuals poststroke: A systematic review. J. Neurol. Phys. Ther. JNPT 2010, 34, 127–137. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; van Wegen, E.; van Peppen, R.; van der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS ONE 2014, 9, e87987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baguma, M.; Yeganeh Doost, M.; Riga, A.; Laloux, P.; Bihin, B.; Vandermeeren, Y. Preserved motor skill learning in acute stroke patients. Acta Neurol. Belg. 2020, 120, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Platz, T.; Denzler, P.; Kaden, B.; Mauritz, K.H. Motor learning after recovery from hemiparesis. Neuropsychologia 1994, 32, 1209–1223. [Google Scholar] [CrossRef]
- Mansfield, A.; Aqui, A.; Danells, C.J.; Knorr, S.; Centen, A.; DePaul, V.G.; Schinkel-Ivy, A.; Brooks, D.; Inness, E.L.; Mochizuki, G. Does perturbation-based balance training prevent falls among individuals with chronic stroke? A randomised controlled trial. BMJ Open 2018, 8, e021510. [Google Scholar] [CrossRef]
- Nevisipour, M.; Grabiner, M.D.; Honeycutt, C.F. A single session of trip-specific training modifies trunk control following treadmill induced balance perturbations in stroke survivors. Gait Posture 2019, 70, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Pai, Y.-C.; Bhatt, T.; Yang, F.; Wang, E.; Kritchevsky, S. Perturbation training can reduce community-dwelling older adults’ annual fall risk: A randomized controlled trial. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 1586–1594. [Google Scholar] [CrossRef]
- Schinkel-Ivy, A.; Huntley, A.H.; Aqui, A.; Mansfield, A. Does perturbation-based balance training improve control of reactive stepping in individuals with chronic stroke? J. Stroke Cerebrovasc. Dis. 2019, 28, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Maki, B.E.; McIlroy, W.E. Change-in-support balance reactions in older persons: An emerging research area of clinical importance. Neurol. Clin. 2005, 23, 751–783. [Google Scholar] [CrossRef] [PubMed]
- Maki, B.E.; McIlroy, W.E. Control of rapid limb movements for balance recovery: Age-related changes and implications for fall prevention. Age Ageing 2006, 35, ii12–ii18. [Google Scholar] [CrossRef] [Green Version]
- Maki, B.E.; Mcilroy, W.E.; Fernie, G.R. Change-in-support reactions for balance recovery. IEEE Eng. Med. Biol. Mag. 2003, 22, 20–26. [Google Scholar] [CrossRef]
- Maki, B.E.; Cheng, K.C.; Mansfield, A.; Scovil, C.Y.; Perry, S.D.; Peters, A.L.; McKay, S.; Lee, T.; Marquis, A.; Corbeil, P.; et al. Preventing falls in older adults: New interventions to promote more effective change-in-support balance reactions. J. Electromyogr. Kinesiol. 2008, 18, 243–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maki, B.E.; McIlroy, W.E. The role of limb movements in maintaining upright stance: The “change-in-support” strategy. Phys. Ther. 1997, 77, 488–507. [Google Scholar] [CrossRef] [PubMed]
- Runge, C.; Shupert, C.; Horak, F.; Zajac, F. Ankle and hip postural strategies defined by joint torques. Gait Posture 1999, 10, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Gerards, M.H.G.; McCrum, C.; Mansfield, A.; Meijer, K. Perturbation-based balance training for falls reduction among older adults: Current evidence and implications for clinical practice. Geriatr. Gerontol. Int. 2017, 17, 2294–2303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansfield, A.; Wong, J.S.; Bryce, J.; Knorr, S.; Patterson, K.K. Does perturbation-based balance training prevent falls? Systematic review and meta-analysis of preliminary randomized controlled trials. Phys. Ther. 2015, 95, 700–709. [Google Scholar] [CrossRef] [PubMed]
- McCrum, C.; Gerards, M.H.G.; Karamanidis, K.; Zijlstra, W.; Meijer, K. A systematic review of gait perturbation paradigms for improving reactive stepping responses and falls risk among healthy older adults. Eur. Rev. Aging Phys. Act. 2017, 14, 3. [Google Scholar] [CrossRef] [Green Version]
- Pai, Y.C.; Bhatt, T.; Wang, E.; Espy, D.; Pavol, M.J. Inoculation against falls: Rapid adaptation by young and older adults to slips during daily activities. Arch. Phys. Med. Rehabil. 2010, 91, 452–459. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, T.; Yang, F.; Pai, Y.-C. Learning to resist gait-slip falls: Long-term retention in community-dwelling older adults. Arch. Phys. Med. Rehabil. 2012, 93, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Bhatt, T.; Wang, S.; Yang, F.; Pai, Y.-C.C. Retention of the “first-trial effect” in gait-slip among community-living older adults. Geroscience 2017, 39, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, T.; Dusane, S.; Patel, P. Does severity of motor impairment affect reactive adaptation and fall-risk in chronic stroke survivors? J. Neuroeng. Rehabil. 2019, 16, 43. [Google Scholar] [CrossRef]
- Dusane, S.; Bhatt, T. Mixed slip-trip perturbation training for improving reactive responses in people with chronic stroke. J. Neurophysiol. 2020, 124, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Dusane, S.; Bhatt, T. Effect of Multisession Progressive Gait-Slip Training on Fall-Resisting Skills of People with Chronic Stroke: Examining Motor Adaptation in Reactive Stability. Brain Sci. 2021, 11, 894. [Google Scholar] [CrossRef] [PubMed]
- Dusane, S.; Bhatt, T. Can prior exposure to repeated non-paretic slips improve reactive responses on novel paretic slips among people with chronic stroke? Exp. Brain Res. 2022, 240, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Dusane, S.; Wang, E.; Bhatt, T. Transfer of reactive balance adaptation from stance-slip perturbation to stance-trip perturbation in chronic stroke survivors. Restor. Neurol. Neurosci. 2019, 37, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, T.; Wening, J.D.; Pai, Y.C. Adaptive control of gait stability in reducing slip-related backward loss of balance. Exp. Brain Res. 2006, 170, 61–73. [Google Scholar] [CrossRef]
- Tan, K.M.; Tan, M.P. Stroke and Falls-Clash of the Two Titans in Geriatrics. Geriatric 2016, 1, 31. [Google Scholar] [CrossRef] [Green Version]
- Yousufuddin, M.; Young, N. Aging and ischemic stroke. Aging 2019, 11, 2542–2544. [Google Scholar] [CrossRef]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Executive summary: Heart disease and stroke statistics—2012 update: A report from the American Heart Association. Circulation 2012, 125, 188–197. [Google Scholar] [CrossRef]
- Purohit, R.; Wang, S.; Dusane, S.; Bhatt, T. Age-related differences in reactive balance control and fall-risk in people with chronic stroke. Gait Posture, 2021; under review. [Google Scholar]
- Lawson, I. Monofilaments. Occup. Med. 2018, 68, 559–561. [Google Scholar]
- Shaffer, S.; Harrison, A.; Brown, K.; Brennan, K. Reliability and validity of Semmes-Weinstein Monofilament testing in older community-dwelling adults. J. Geriatr. Phys. Ther. 2005, 28, 112–113. [Google Scholar] [CrossRef]
- Feng, Y.; Schlösser, F.J.; Sumpio, B.E. The Semmes Weinstein monofilament examination as a screening tool for diabetic peripheral neuropathy. J. Vasc. Surg. 2009, 50, 675–682.e671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajrolkar, T.; Bhatt, T. Falls-risk post-stroke: Examining contributions from paretic versus non paretic limbs to unexpected forward gait slips. J. Biomech. 2016, 49, 2702–2708. [Google Scholar] [CrossRef] [PubMed]
- Kajrolkar, T.; Yang, F.; Pai, Y.C.; Bhatt, T. Dynamic stability and compensatory stepping responses during anterior gait-slip perturbations in people with chronic hemiparetic stroke. J. Biomech. 2014, 47, 2751–2758. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, T.; Wening, J.D.; Pai, Y.C. Influence of gait speed on stability: Recovery from anterior slips and compensatory stepping. Gait Posture 2005, 21, 146–156. [Google Scholar] [CrossRef]
- Pai, Y.C.; Iqbal, K. Simulated movement termination for balance recovery: Can movement strategies be sought to maintain stability in the presence of slipping or forced sliding? J. Biomech. 1999, 32, 779–786. [Google Scholar] [CrossRef]
- de Leva, P. Adjustments to Zatsiorsky-Seluyanov's segment inertia parameters. J. Biomech. 1996, 29, 1223–1230. [Google Scholar] [CrossRef]
- Bhatt, T.; Pai, Y.C. Long-term retention of gait stability improvements. J. Neurophysiol. 2005, 94, 1971–1979. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.S.; Hui-Chan, C.W. The timed up & go test: Its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1641–1647. [Google Scholar]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [PubMed] [Green Version]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in stroke rehabilitation: A systematic review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, T.J. Detecting change in patients with stroke using the Berg Balance Scale. Aust. J. Physiother. 2001, 47, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Graham, J.E.; Ostir, G.V.; Fisher, S.R.; Ottenbacher, K.J. Assessing walking speed in clinical research: A systematic review. J. Eval. Clin. Pract. 2008, 14, 552–562. [Google Scholar] [CrossRef]
- Feldman, L.S.; Cao, J.; Andalib, A.; Fraser, S.; Fried, G.M. A method to characterize the learning curve for performance of a fundamental laparoscopic simulator task: Defining “learning plateau” and “learning rate”. Surgery 2009, 146, 381–386. [Google Scholar] [CrossRef]
- Bloomer, C.; Wang, S.; Kontson, K. Creating a standardized, quantitative training protocol for upper limb bypass prostheses. Phys. Med. Rehabil. Res. 2018, 3, 1. [Google Scholar] [CrossRef]
- Kasahara, S.; Saito, H. Effect of loading parameters on motor performance during a dynamic weight-shift task. Gait Posture 2015, 41, 100–105. [Google Scholar] [CrossRef]
- Wadden, K.P.; Asis, K.D.; Mang, C.S.; Neva, J.L.; Peters, S.; Lakhani, B.; Boyd, L.A. Predicting motor sequence learning in individuals with chronic stroke. Neurorehabilit. Neural Repair 2017, 31, 95–104. [Google Scholar] [CrossRef]
- Kitago, T.; Krakauer, J.W. Motor learning principles for neurorehabilitation. Handb. Clin. Neurol. 2013, 110, 93–103. [Google Scholar]
- Walker, M.P.; Brakefield, T.; Allan Hobson, J.; Stickgold, R. Dissociable stages of human memory consolidation and reconsolidation. Nature 2003, 425, 616–620. [Google Scholar] [CrossRef]
- Censor, N.; Sagi, D.; Cohen, L.G. Common mechanisms of human perceptual and motor learning. Nat. Rev. Neurosci. 2012, 13, 658–664. [Google Scholar] [CrossRef] [Green Version]
- Krakauer, J.W. Motor learning: Its relevance to stroke recovery and neurorehabilitation. Curr. Opin. Neurol. 2006, 19, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, T.; Wang, E.; Pai, Y.-C. Retention of adaptive control over varying intervals: Prevention of slip-induced backward balance loss during gait. J. Neurophysiol. 2006, 95, 2913–2922. [Google Scholar] [CrossRef]
- Horak, F.B.; Diener, H.; Nashner, L. Influence of central set on human postural responses. J. Neurophysiol. 1989, 62, 841–853. [Google Scholar] [CrossRef] [PubMed]
- Scheidt, R.A.; Dingwell, J.B.; Mussa-Ivaldi, F.A. Learning to move amid uncertainty. J. Neurophysiol. 2001, 86, 971–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vetter, P.; Wolpert, D.M. Context estimation for sensorimotor control. J. Neurophysiol. 2000, 84, 1026–1034. [Google Scholar] [CrossRef]
- Lee, A.; Bhatt, T.; Liu, X.; Wang, Y.; Wang, S.; Pai, Y.-C.C. Can treadmill slip-perturbation training reduce longer-term fall risk upon overground slip exposure? J. Appl. Biomech. 2020, 36, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Frost, S.B.; Barbay, S.; Friel, K.M.; Plautz, E.J.; Nudo, R.J. Reorganization of remote cortical regions after ischemic brain injury: A potential substrate for stroke recovery. J. Neurophysiol. 2003, 89, 32053214. [Google Scholar] [CrossRef]
- Morton, S.M.; Bastian, A.J. Cerebellar contributions to locomotor adaptations during splitbelt treadmill walking. J. Neurosci. 2006, 26, 9107–9116. [Google Scholar] [CrossRef] [Green Version]
- Morton, S.M.; Bastian, A.J. Cerebellar control of balance and locomotion. Neuroscience 2004, 10, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Surgent, O.J.; Dadalko, O.I.; Pickett, K.A.; Travers, B.G. Balance and the brain: A review of structural brain correlates of postural balance and balance training in humans. Gait Posture 2019, 71, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Thach, W.T.; Bastian, A.J. Role of the cerebellum in the control and adaptation of gait in health and disease. Prog. Brain Res. 2004, 143, 353–366. [Google Scholar]
- Wittenberg, E.; Thompson, J.; Nam, C.S.; Franz, J.R. Neuroimaging of human balance control: A systematic review. Front. Hum. Neurosci. 2017, 11, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reisman, D.S.; Wityk, R.; Silver, K.; Bastian, A.J. Locomotor adaptation on a split-belt treadmill can improve walking symmetry post-stroke. Brain 2007, 130, 1861–1872. [Google Scholar] [CrossRef]
- Savin, D.N.; Tseng, S.-C.; Whitall, J.; Morton, S.M. Poststroke hemiparesis impairs the rate but not magnitude of adaptation of spatial and temporal locomotor features. Neurorehabilit. Neural Repair 2013, 27, 24–34. [Google Scholar] [CrossRef] [Green Version]
- Paul, T.; Wiemer, V.M.; Grafton, S.T.; Fink, G.R.; Volz, L.J. P 11 Motor adaptation learning and the effects of reinforcement in the acute phase post-stroke. Clin. Neurophysiol. 2022, 137, e20–e21. [Google Scholar] [CrossRef]
- Adkin, A.L.; Campbell, A.D.; Chua, R.; Carpenter, M.G. The influence of postural threat on the cortical response to unpredictable and predictable postural perturbations. Neurosci Lett 2008, 435, 120–125. [Google Scholar] [CrossRef]
- Payne, A.M.; Hajcak, G.; Ting, L.H. Dissociation of muscle and cortical response scaling to balance perturbation acceleration. J. Neurophysiol. 2019, 121, 867–880. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.M.; Ting, L.H. Worse balance is associated with larger perturbation-evoked cortical responses in healthy young adults. Gait Posture 2020, 80, 324–330. [Google Scholar] [CrossRef]
- Sibley, K.M.; Mochizuki, G.; Frank, J.S.; McIlroy, W.E. The relationship between physiological arousal and cortical and autonomic responses to postural instability. Exp. Brain Res. 2010, 203, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Adkin, A.L.; Frank, J.S.; Carpenter, M.G.; Peysar, G.W. Postural control is scaled to level of postural threat. Gait Posture 2000, 12, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, D.C.; Hynd, A.L.; Minke, K.A.; Minemoto, T.; Blanchard, R.J. Human defensive behaviors to threat scenarios show parallels to fear-and anxiety-related defense patterns of non-human mammals. Neurosci. Biobehav. Rev. 2001, 25, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, M.G.; Frank, J.S.; Silcher, C.P.; Peysar, G.W. The influence of postural threat on the control of upright stance. Exp. Brain Res. 2001, 138, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, O., Jr.; Portugal, L.C.; Alves, R.C.; Campagnoli, R.R.; Mocaiber, I.; David, I.P.; Erthal, F.C.; Volchan, E.; de Oliveira, L.; Pereira, M.G. How you perceive threat determines your behavior. Front. Hum. Neurosci. 2013, 7, 632. [Google Scholar] [CrossRef]
- Kostka, J.; Niwald, M.; Guligowska, A.; Kostka, T.; Miller, E. Muscle power, contraction velocity and functional performance after stroke. Brain Behav. 2019, 9, e01243. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, O.H.; Stenager, E.; Dalgas, U. Muscle Strength and Poststroke Hemiplegia: A Systematic Review of Muscle Strength Assessment and Muscle Strength Impairment. Arch. Phys. Med. Rehabil. 2017, 98, 368–380. [Google Scholar] [CrossRef]
- Neckel, N.D.; Blonien, N.; Nichols, D.; Hidler, J. Abnormal joint torque patterns exhibited by chronic stroke subjects while walking with a prescribed physiological gait pattern. J. Neuroeng. Rehabil. 2008, 5, 19. [Google Scholar] [CrossRef] [Green Version]
- Pandian, S.; Arya, K.N. Motor impairment of the ipsilesional body side in poststroke subjects. J. Bodyw. Mov. Ther. 2013, 17, 495–503. [Google Scholar] [CrossRef]
- Pandian, S.; Arya, K.N.; Kumar, D. Does motor training of the nonparetic side influences balance and function in chronic stroke? A pilot RCT. Sci. World J. 2014, 2014, 769726. [Google Scholar] [CrossRef] [Green Version]
- Son, S.M.; Kang, K.W. Relationship between ipsilateral motor deficits on the less-affected side and motor function stage on the affected side. J. Korean Phys. Ther. 2018, 30, 234–239. [Google Scholar] [CrossRef]
- Wang, S.; Pai, Y.-C.; Bhatt, T. Is there an optimal recovery step landing zone against slip-induced backward falls during walking? Ann. Biomed. Eng. 2020, 48, 1768–1778. [Google Scholar] [CrossRef]
- Xingda, Q.; Xinyao, H.; Fui Ling, L. Differences in lower extremity muscular responses between successful and failed balance recovery after slips. Int. J. Ind. Ergon. 2012, 42, 499–504. [Google Scholar] [CrossRef]
- Liu, J. Aging effect on joint moment generation strategy in successful reactive-recovery from unexpected slips. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Orlando, FL, USA, 26–30 September 2005; SAGE Publications: Los Angeles, CA, USA, 2005; pp. 1302–1305. [Google Scholar]
- Morton, S.M.; Bastian, A.J. Prism adaptation during walking generalizes to reaching and requires the cerebellum. J. Neurophysiol. 2004, 92, 2497–2509. [Google Scholar] [CrossRef]
- Redfern, M.S.; Cham, R.; Gielo-Perczak, K.; Grönqvist, R.; Hirvonen, M.; Lanshammar, H.; Marpet, M.; Pai, C.Y.; Powers, C. Biomechanics of slips. Ergonomics 2001, 44, 1138–1166. [Google Scholar] [CrossRef]
- Tokur, D.; Grimmer, M.; Seyfarth, A. Review of balance recovery in response to external perturbations during daily activities. Hum. Mov. Sci. 2020, 69, 102546. [Google Scholar] [CrossRef] [PubMed]
- Miall, R.C.; Christensen, L.O.D.; Cain, O.; Stanley, J. Disruption of state estimation in the human lateral cerebellum. PLoS Biol. 2007, 5, e316. [Google Scholar] [CrossRef] [Green Version]
- Joiner, W.M.; Smith, M.A. Long-term retention explained by a model of short-term learning in the adaptive control of reaching. J. Neurophysiol. 2008, 100, 2948–2955. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.A.; Ghazizadeh, A.; Shadmehr, R. Interacting adaptive processes with different timescales underlie short-term motor learning. PLoS Biol 2006, 4, e179. [Google Scholar] [CrossRef] [Green Version]
- Hung, C.S.; Hsieh, Y.W.; Wu, C.Y.; Lin, Y.T.; Lin, K.C.; Chen, C.L. The Effects of Combination of Robot-Assisted Therapy With Task-Specific or Impairment-Oriented Training on Motor Function and Quality of Life in Chronic Stroke. PM R 2016, 8, 721–729. [Google Scholar] [CrossRef]
- Lee, Y.C.; Li, Y.C.; Lin, K.C.; Yao, G.; Chang, Y.J.; Lee, Y.Y.; Liu, C.T.; Hsu, W.L.; Wu, Y.H.; Chu, H.T.; et al. Effects of robotic priming of bilateral arm training, mirror therapy, and impairment-oriented training on sensorimotor and daily functions in patients with chronic stroke: Study protocol of a single-blind, randomized controlled trial. Trials 2022, 23, 566. [Google Scholar] [CrossRef] [PubMed]
- Platz, T.; van Kaick, S.; Möller, L.; Freund, S.; Winter, T.; Kim, I.H. Impairment-oriented training and adaptive motor cortex reorganisation after stroke: A fTMS study. J. Neurol. 2005, 252, 1363–1371. [Google Scholar] [CrossRef] [PubMed]
- Platz, T. Impairment-oriented training (IOT)—Scientific concept and evidence-based treatment strategies. Restor. Neurol. Neurosci. 2004, 22, 301–315. [Google Scholar] [PubMed]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. J. Appl. Stat. Pharm. Ind. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Faria, C.d.A.; Alves, H.V.D.; Charchat-Fichman, H. The most frequently used tests for assessing executive functions in aging. Dement. Neuropsychol. 2015, 9, 149–155. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Mean (SD) | p Value | ||
|---|---|---|---|---|
| YAwCS | OAwCS | HOA | ||
| Age, y | 51.67 (7.05) | 65.36 (4.16) | 69.23 (5.17) | 0.001 a,b |
| Sex, M/F | 10/5 | 12/2 | 7/6 | 0.61 |
| Height, m | 1.73 (0.08) | 1.70 (0.11) | 1.68 (0.15) | 0.39 |
| Weight, kg | 80.40 (11.65) | 82.52 (16.06) | 76.10 (15.92) | 0.51 |
| Chronicity, y | 7.2 (3.85) | 13.4 (7.46) | N/A | 0.01 a |
| Type of stroke, H/I | 5/10 | 8/6 | N/A | 0.36 |
| AFO/No AFO | 10/5 | 7/7 | N/A | 0.20 |
| CMSA (Leg), (out of 7) | 4.87 (1.06) | 5.13 (0.74) | N/A | 0.50 |
| BBS (/56) | 49.4 (3.60) | 48.86 (6.19) | 53.86 (1.96) | 0.01 b,c |
| Adaptation Rate | Variables | Mean (SD) | Kruskal–Wallis | |||
|---|---|---|---|---|---|---|
| YAwCS | OAwCS | HOA | p Value | χ2 Value | ||
| Proactive | Pre-slip STA | 3.07 (2.09) | 3.64 (1.78) | 3.54 (1.94) | 0.56 | 1.16 |
| Pre-slip COMx | 4.07 (2.02) | 4.5 (2.03) | 5.3 (1.65) | 0.28 | 2.58 | |
| Pre-slip COMv | 2.2 (1.57) | 2.29 (1.33) | 2.46 (2.29) | 0.74 | 0.59 | |
| Reactive | Post-slip STA | 5.2 (1.82) | 5.07 (1.69) | 4.54 (1.51) | 0.52 | 1.3 |
| Post-slip COMx | 5.47 (1.46) | 4.43 (1.83) | 4.77 (1.83) | 0.15 | 3.75 | |
| Post-slip COMv | 4.2 (1.42) | 4.5 (1.7) | 4 (1.63) | 0.54 | 1.23 | |
| Max slipx | 3.93 (2.01) | 4 (1.62) | 5.46 (1.94) | 0.1 | 4.69 | |
| Max slipv | 4.67 (1.87) | 4.79 (1.93) | 4.62 (1.98) | 0.95 | 0.1 | |
| Comp SL | 4.93 (1.94) | 4.07 (2.43) | 5.31 (2.36) | 0.34 | 2.15 | |
| Adaptation Plateau | Variables | Mean (SD) | ANOVA | |||
|---|---|---|---|---|---|---|
| YAwCS | OAwCS | HOA | p Value | F Value | ||
| Proactive | Pre-slip STA | 0.04 (0.09) | 0.08 (0.09) | 0.06 (0.05) | 0.57 | 0.57 |
| Pre-slip COMx | 0.15 (0.11) | 0.25 (0.23) | 0.24 (0.17) | 0.23 | 1.55 | |
| Pre-slip COMv | 0.01 (0.08) | 0.05 (0.18) | 0.01 (0.09) | 0.62 | 0.49 | |
| Reactive | Post-slip STA | 1.05 (0.33) | 1.14 (0.26) | 1.36 (0.16) | 0.01 b,c | 4.95 |
| Post-slip COMx | 1.89 (0.51) | 1.7 (0.38) | 1.89 (0.32) | 0.39 | 0.95 | |
| Post-slip COMv | 0.24 (0.18) | 0.25 (0.18) | 0.43 (0.16) | 0.01 b,c | 5.17 | |
| Max slipx | 0.23 (0.25) | 0.31 (0.1) | 0.43 (0.18) | 0.03 b,c | 3.69 | |
| Max slipv | 0.83 (0.5) | 0.94 (0.35) | 1.28 (0.47) | 0.03 b,c | 3.81 | |
| Comp SL | 0.36(0.2) | 0.34(0.27) | 0.49(0.14) | 0.13 | 2.11 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Purohit, R.; Wang, S.; Bhatt, T. Effect of Aging and Cortical Stroke on Motor Adaptation to Overground Gait-Slips: Quantifying Differences in Adaptation Rate and Adaptation Plateau. Biomechanics 2023, 3, 29-44. https://doi.org/10.3390/biomechanics3010003
Purohit R, Wang S, Bhatt T. Effect of Aging and Cortical Stroke on Motor Adaptation to Overground Gait-Slips: Quantifying Differences in Adaptation Rate and Adaptation Plateau. Biomechanics. 2023; 3(1):29-44. https://doi.org/10.3390/biomechanics3010003
Chicago/Turabian StylePurohit, Rudri, Shuaijie Wang, and Tanvi Bhatt. 2023. "Effect of Aging and Cortical Stroke on Motor Adaptation to Overground Gait-Slips: Quantifying Differences in Adaptation Rate and Adaptation Plateau" Biomechanics 3, no. 1: 29-44. https://doi.org/10.3390/biomechanics3010003