
Spine Bracing: When to Utilize—A Narrative Review
 and
and
Abstract
:1. Introduction
2. Methods of Literature Search
3. Spinal Bracing Practices en Route to the ER
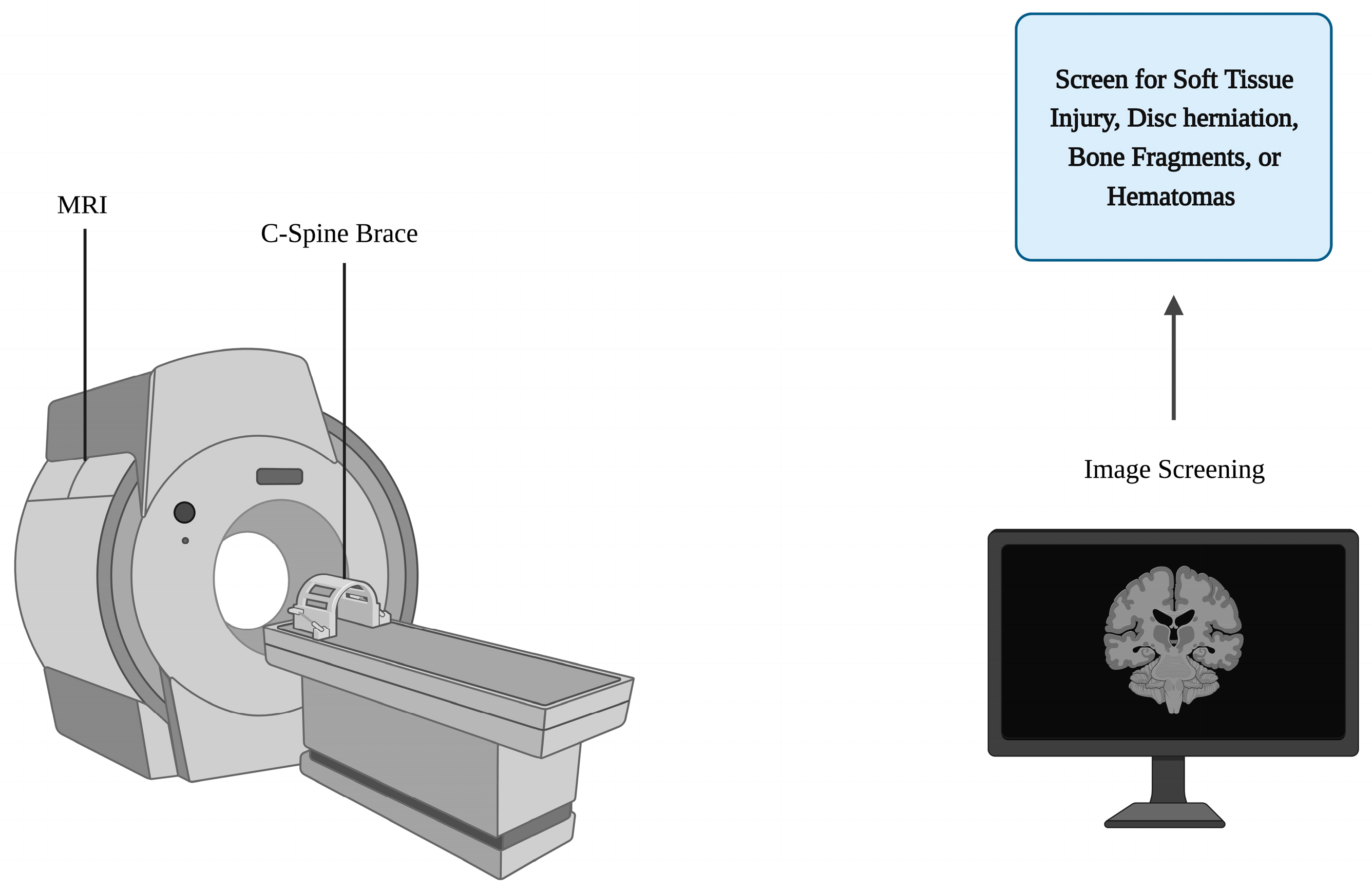
4. Spinal Bracing and Imaging Practices in the Emergency Room
5. Beyond the ER—Spinal Bracing for Spinal Deformities
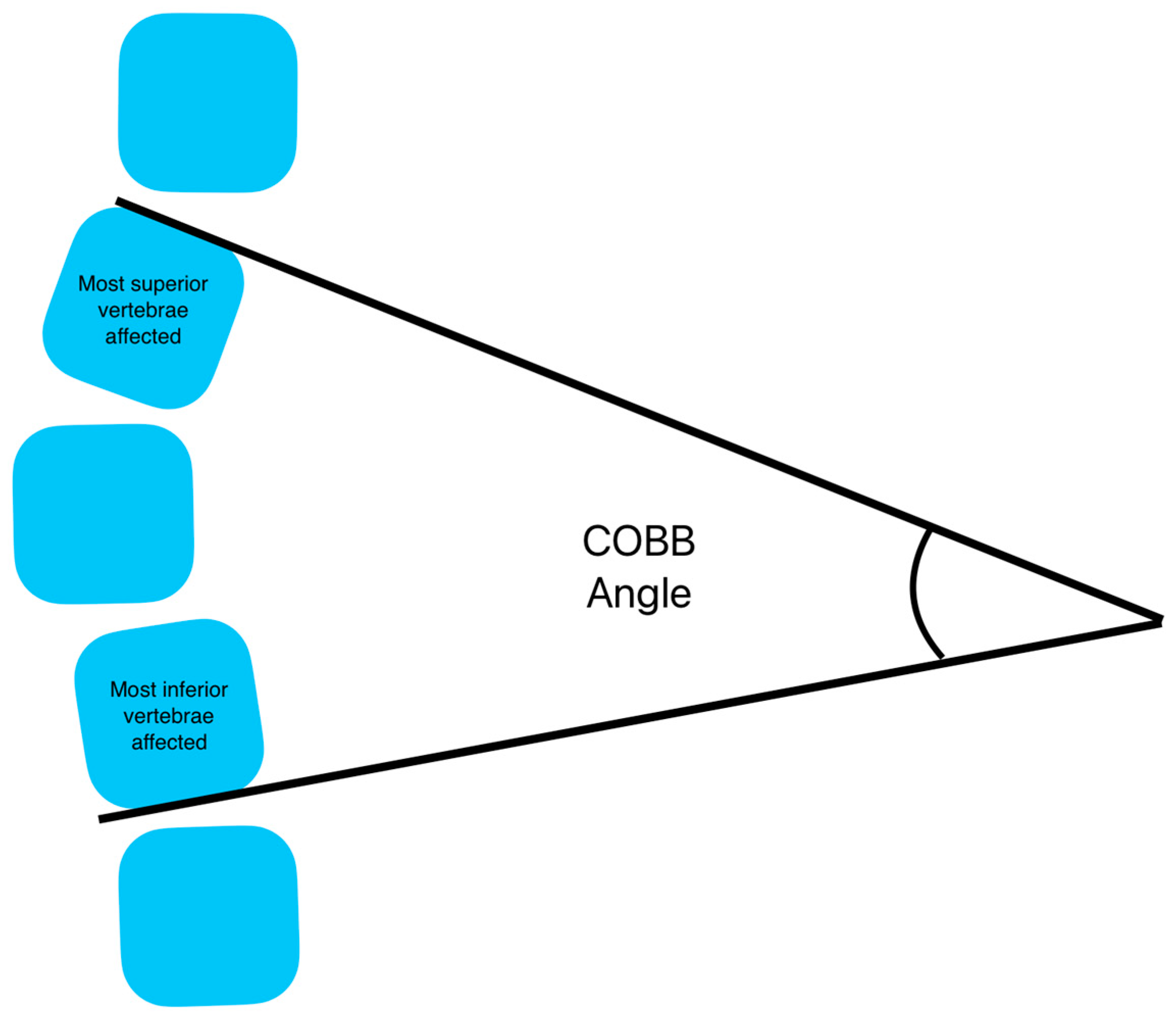
6. Spinal Deformity—Scoliosis
6.1. Diagnosis and Bracing Indications
6.2. Bracing Perscriptions for Scoliosis
6.3. Skeletal Maturity Evaluation in Scoliosis Patients
6.4. Adult Scoliosis
7. Spinal Deformity—Hyperkyphosis
8. Postoperative Spinal Bracing
9. Spinal Bracing for Chronic Lower Back Pain
10. Spinal Bracing for Pregnancy
11. Braces Currently Available
12. The Future of Bracing
13. Limitations
14. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, R.; Lim, J.; Mekary, R.A.; Rattani, A.; Dewan, M.C.; Sharif, S.Y.; Osorio-Fonseca, E.; Park, K.B. Traumatic Spinal Injury: Global Epidemiology and Worldwide Volume. World Neurosurg. 2018, 113, e345–e363. [Google Scholar] [CrossRef]
- Devivo, M.J. Epidemiology of traumatic spinal cord injury: Trends and future implications. Spinal Cord 2012, 50, 365–372. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, J.; Davis, A. Diagnosis and Management of Vertebral Compression Fractures. Am. Fam. Physician 2016, 94, 44–50. [Google Scholar] [PubMed]
- Agabegi, S.S.; Asghar, F.A.; Herkowitz, H.N. Spinal orthoses. J. Am. Acad. Orthop. Surg. 2010, 18, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Minozzi, S.; Bettany-Saltikov, J.; Chockalingam, N.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Romano, M.; Zaina, F. Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst. Rev. 2015, 6, CD006850. [Google Scholar] [CrossRef] [Green Version]
- Christensen, S.W.M.; Rasmussen, M.B.; Jespersen, C.L.; Sterling, M.; Skou, S.T. Soft-collar use in rehabilitation of whiplash-associated disorders—A systematic review and meta-analysis. Musculoskelet. Sci. Pract. 2021, 55, 102426. [Google Scholar] [CrossRef] [PubMed]
- Jhaveri, S.N.; Zeller, R.; Miller, S.; Lewis, S.J. The effect of intra-operative skeletal (skull femoral) traction on apical vertebral rotation. Eur. Spine J. 2009, 18, 352–356. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Adeoye, A.L.; Dahdaleh, N.S. Indications and complications of crown halo vest placement: A review. J. Clin. Neurosci. 2017, 40, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Sundstrom, T.; Asbjornsen, H.; Habiba, S.; Sunde, G.A.; Wester, K. Prehospital use of cervical collars in trauma patients: A critical review. J. Neurotrauma 2014, 31, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Hawary, R.E.; Zaaroor-Regev, D.; Floman, Y.; Lonner, B.S.; Alkhalife, Y.I.; Betz, R.R. Brace treatment in adolescent idiopathic scoliosis: Risk factors for failure-a literature review. Spine J. 2019, 19, 1917–1925. [Google Scholar] [CrossRef] [Green Version]
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.L.; Clement, C.M.; Lesiuk, H.; De Maio, V.J.; Laupacis, A.; Schull, M.; McKnight, R.D.; Verbeek, R.; et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA 2001, 286, 1841–1848. [Google Scholar] [CrossRef] [Green Version]
- Zileli, M.; Osorio-Fonseca, E.; Konovalov, N.; Cardenas-Jalabe, C.; Kaprovoy, S.; Mlyavykh, S.; Pogosyan, A. Early Management of Cervical Spine Trauma: WFNS Spine Committee Recommendations. Neurospine 2020, 17, 710–722. [Google Scholar] [CrossRef] [PubMed]
- American College of Surgeons. Committee on T: Advanced Trauma Life Support: Student Course Manual; American College of Surgeons: Chicago, IL, USA, 2018. [Google Scholar]
- Shank, C.D.; Walters, B.C.; Hadley, M.N. Current Topics in the Management of Acute Traumatic Spinal Cord Injury. Neurocrit. Care 2019, 30, 261–271. [Google Scholar] [CrossRef] [PubMed]
- National Association of Emergency Medical Technicians (NAEMT); American College of Surgeons. PHTLS: Prehospital Trauma Life Support; Jones & Bartlett Learning: Burlington, MA, USA, 2020. [Google Scholar]
- Hauswald, M.; Ong, G.; Tandberg, D.; Omar, Z. Out-of-hospital spinal immobilization: Its effect on neurologic injury. Acad. Emerg. Med. 1998, 5, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Kwan, I.; Bunn, F.; Roberts, I. Spinal immobilisation for trauma patients. Cochrane Database Syst. Rev. 2001, 2001, CD002803. [Google Scholar] [CrossRef] [PubMed]
- Bauer, D.; Kowalski, R. Effect of spinal immobilization devices on pulmonary function in the healthy, nonsmoking man. Ann. Emerg. Med. 1988, 17, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Totten, V.Y.; Sugarman, D.B. Respiratory effects of spinal immobilization. Prehospital Emerg. Care 1999, 3, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Schafermeyer, R.W.; Ribbeck, B.M.; Gaskins, J.; Thomason, S.; Harlan, M.; Attkisson, A. Respiratory effects of spinal immobilization in children. Ann. Emerg. Med. 1991, 20, 1017–1019. [Google Scholar] [CrossRef]
- Ham, W.H.; Schoonhoven, L.; Schuurmans, M.J.; Leenen, L.P. Pressure ulcers, indentation marks and pain from cervical spine immobilization with extrication collars and headblocks: An observational study. Injury 2016, 47, 1924–1931. [Google Scholar] [CrossRef]
- Barkana, Y.; Stein, M.; Scope, A.; Maor, R.; Abramovich, Y.; Friedman, Z.; Knoller, N. Prehospital stabilization of the cervical spine for penetrating injuries of the neck—Is it necessary? Injury 2000, 31, 305–309. [Google Scholar] [CrossRef]
- Nunez-Patino, R.A.; Rubiano, A.M.; Godoy, D.A. Impact of Cervical Collars on Intracranial Pressure Values in Traumatic Brain Injury: A Systematic Review and Meta-Analysis of Prospective Studies. Neurocrit. Care 2020, 32, 469–477. [Google Scholar] [CrossRef]
- Ozdogan, S.; Gokcek, O.; Katirci, Y.; Corbacioglu, S.K.; Emektar, E.; Cevik, Y. The effects of spinal immobilization at 20 degrees on intracranial pressure. Am. J. Emerg. Med. 2019, 37, 1327–1330. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, R.J.; Stoodley, M.A.; Fuller, J. Effect of cervical hard collar on intracranial pressure after head injury. ANZ J. Surg. 2002, 72, 389–391. [Google Scholar] [CrossRef]
- Backer, H.C.; Elias, P.; Braun, K.F.; Johnson, M.A.; Turner, P.; Cunningham, J. Cervical immobilization in trauma patients: Soft collars better than rigid collars? A systematic review and meta-analysis. Eur. Spine J. 2022, 31, 3378–3391. [Google Scholar] [CrossRef]
- Dixon, M.; O’Halloran, J.; Cummins, N.M. Biomechanical analysis of spinal immobilisation during prehospital extrication: A proof of concept study. Emerg. Med. J. 2014, 31, 745–749. [Google Scholar] [CrossRef] [Green Version]
- Maschmann, C.; Jeppesen, E.; Rubin, M.A.; Barfod, C. New clinical guidelines on the spinal stabilisation of adult trauma patients—Consensus and evidence based. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 77. [Google Scholar] [CrossRef] [PubMed]
- Vaillancourt, C.; Charette, M.; Kasaboski, A.; Maloney, J.; Wells, G.A.; Stiell, I.G. Evaluation of the safety of C-spine clearance by paramedics: Design and methodology. BMC Emerg. Med. 2011, 11, 1. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, J.R.; Mower, W.R.; Wolfson, A.B.; Todd, K.H.; Zucker, M.I. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N. Engl. J. Med. 2000, 343, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Paykin, G.; O’Reilly, G.; Ackland, H.M.; Mitra, B. The NEXUS criteria are insufficient to exclude cervical spine fractures in older blunt trauma patients. Injury 2017, 48, 1020–1024. [Google Scholar] [CrossRef]
- Healey, C.D.; Spilman, S.K.; King, B.D.; Sherrill, J.E., 2nd; Pelaez, C.A. Asymptomatic cervical spine fractures: Current guidelines can fail older patients. J. Trauma Acute Care Surg. 2017, 83, 119–125. [Google Scholar] [CrossRef]
- Spaniolas, K.; Cheng, J.D.; Gestring, M.L.; Sangosanya, A.; Stassen, N.A.; Bankey, P.E. Ground level falls are associated with significant mortality in elderly patients. J. Trauma 2010, 69, 821–825. [Google Scholar] [CrossRef] [PubMed]
- TQIP ACoSTQIPA: ACS TQIP Best Practices Guidelines in Imaging; American College of Surgeons: Chicago, IL, USA, 2018.
- Ehrlich, P.F.; Wee, C.; Drongowski, R.; Rana, A.R. Canadian C-spine Rule and the National Emergency X-Radiography Utilization Low-Risk Criteria for C-spine radiography in young trauma patients. J. Pediatr. Surg. 2009, 44, 987–991. [Google Scholar] [CrossRef]
- Viccellio, P.; Simon, H.; Pressman, B.D.; Shah, M.N.; Mower, W.R.; Hoffman, J.R.; for the NEXUS Group. A prospective multicenter study of cervical spine injury in children. Pediatrics 2001, 108, E20. [Google Scholar] [CrossRef] [Green Version]
- Garton, H.J.; Hammer, M.R. Detection of pediatric cervical spine injury. Neurosurgery 2008, 62, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.L.; Sena, M.; Greenholz, S.K.; Fledderman, M. A multidisciplinary approach to the development of a cervical spine clearance protocol: Process, rationale, and initial results. J. Pediatr. Surg. 2003, 38, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Pieretti-Vanmarcke, R.; Velmahos, G.C.; Nance, M.L.; Islam, S.; Falcone, R.A.; Wales, P.W.; Brown, R.L.; Gaines, B.A.; McKenna, C.; Moore, F.O.; et al. Clinical clearance of the cervical spine in blunt trauma patients younger than 3 years: A multi-center study of the american association for the surgery of trauma. J. Trauma 2009, 67, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.; Elliston, C.; Hall, E.; Berdon, W. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am. J. Roentgenol. 2001, 176, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Ghelichkhani, P.; Shahsavarinia, K.; Gharekhani, A.; Taghizadieh, A.; Baratloo, A.; Fattah, F.H.R.; Abbasi, N.; Gubari, M.I.M.; Faridaalee, G.; Dinpanah, H.; et al. Value of Canadian C-spine rule versus the NEXUS criteria in ruling out clinically important cervical spine injuries: Derivation of modified Canadian C-spine rule. Radiol. Med. 2021, 126, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Bailitz, J.; Starr, F.; Beecroft, M.; Bankoff, J.; Roberts, R.; Bokhari, F.; Joseph, K.; Wiley, D.; Dennis, A.; Gilkey, S.; et al. CT should replace three-view radiographs as the initial screening test in patients at high, moderate, and low risk for blunt cervical spine injury: A prospective comparison. J. Trauma 2009, 66, 1605–1609. [Google Scholar] [CrossRef] [PubMed]
- Duane, T.M.; Young, A.J.; Vanguri, P.; Wolfe, L.G.; Katzen, J.; Han, J.; Mayglothling, J.; Whelan, J.F.; Aboutanos, M.B.; Ivatury, R.R.; et al. Defining the cervical spine clearance algorithm: A single-institution prospective study of more than 9000 patients. J. Trauma Acute Care Surg. 2016, 81, 541–547. [Google Scholar] [CrossRef]
- Wood, K.B.; Li, W.; Lebl, D.R.; Ploumis, A. Management of thoracolumbar spine fractures. Spine J. 2014, 14, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Panjabi, M.M. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J. Spinal Disord. 1992, 5, 383–389. [Google Scholar] [CrossRef]
- Fernandez-de Thomas, R.J.; De Jesus, O. Thoracolumbar Spine Fracture; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- McMordie, J.H.; Viswanathan, V.K.; Gillis, C.C. Cervical Spine Fractures Overview; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Roberts, T.T.; Leonard, G.R.; Cepela, D.J. Classifications In Brief: American Spinal Injury Association (ASIA) Impairment Scale. Clin. Orthop. Relat. Res. 2017, 475, 1499–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, V.; Holly, L.T. Bracing for thoracolumbar fractures. Neurosurg. Focus 2014, 37, E3. [Google Scholar] [CrossRef] [Green Version]
- Vaccaro, A.R.; Hulbert, R.J.; Patel, A.A.; Fisher, C.; Dvorak, M.; Lehman, R.A.; Anderson, P.; Harrop, J.; Oner, F.C.; Arnold, P.; et al. The subaxial cervical spine injury classification system: A novel approach to recognize the importance of morphology, neurology, and integrity of the disco-ligamentous complex. Spine 2007, 32, 2365–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.Y.; Vaccaro, A.R.; Lim, M.R.; Öner, F.; Hulbert, R.J.; Hedlund, R.; Fehlings, M.G.; Arnold, P.; Harrop, J.; Bono, C.M.; et al. Thoracolumbar injury classification and severity score: A new paradigm for the treatment of thoracolumbar spine trauma. J. Orthop. Sci. 2005, 10, 671–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denis, F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983, 8, 817–831. [Google Scholar] [CrossRef]
- Saul, D.; Khosla, S. Fracture Healing in the Setting of Endocrine Diseases, Aging, and Cellular Senescence. Endocr. Rev. 2022, 43, 984–1002. [Google Scholar] [CrossRef]
- Al-Hadithy, N.; Sewell, M.D.; Bhavikatti, M.; Gikas, P.D. The effect of smoking on fracture healing and on various orthopaedic procedures. Acta Orthop. Belg. 2012, 78, 285–290. [Google Scholar]
- Jiao, H.; Xiao, E.; Graves, D.T. Diabetes and Its Effect on Bone and Fracture Healing. Curr. Osteoporos. Rep. 2015, 13, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.; Fontanari, V.; Fontana, M.; Schmolz, W. Spinal Deformities and Advancement in Corrective Orthoses. Bioengineering 2020, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Trobisch, P.; Suess, O.; Schwab, F. Idiopathic scoliosis. Dtsch. Ärzteblatt Int. 2010, 107, 875–883. [Google Scholar] [CrossRef]
- Aebi, M. The adult scoliosis. Eur. Spine J. 2005, 14, 925–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaelin, A.J. Adolescent idiopathic scoliosis: Indications for bracing and conservative treatments. Ann. Transl. Med. 2020, 8, 28. [Google Scholar] [CrossRef]
- Kuznia, A.L.; Hernandez, A.K.; Lee, L.U. Adolescent Idiopathic Scoliosis: Common Questions and Answers. Am. Fam. Physician 2020, 101, 19–23. [Google Scholar] [PubMed]
- Rowe, D.E.; Bernstein, S.M.; Riddick, M.F.; Adler, F.; Emans, J.B.; Gardner-Bonneau, D. A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J. Bone Jt. Surg. Am. 1997, 79, 664–674. [Google Scholar] [CrossRef]
- Richards, B.S.; Bernstein, R.M.; D’Amato, C.R.; Thompson, G.H. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine 2005, 30, 2068–2075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Will, R.E.; Stokes, I.A.; Qiu, X.; Walker, M.R.; Sanders, J.O. Cobb angle progression in adolescent scoliosis begins at the intervertebral disc. Spine 2009, 34, 2782–2786. [Google Scholar] [CrossRef]
- Bunnell, W.P. An objective criterion for scoliosis screening. J. Bone Jt. Surg. Am. 1984, 66, 1381–1387. [Google Scholar] [CrossRef]
- Murrell, G.A.; Coonrad, R.W.; Moorman, C.T., 3rd; Fitch, R.D. An assessment of the reliability of the Scoliometer. Spine 1993, 18, 709–712. [Google Scholar] [CrossRef]
- El-Hawary, R.; Chukwunyerenwa, C. Update on evaluation and treatment of scoliosis. Pediatr. Clin. N. Am. 2014, 61, 1223–1241. [Google Scholar] [CrossRef] [PubMed]
- Dolan, L.A.; Donzelli, S.; Zaina, F.; Weinstein, S.L.; Negrini, S. Adolescent Idiopathic Scoliosis Bracing Success Is Influenced by Time in Brace: Comparative Effectiveness Analysis of BrAIST and ISICO Cohorts. Spine 2020, 45, 1193–1199. [Google Scholar] [CrossRef]
- Karol, L.A.; Virostek, D.; Felton, K.; Jo, C.; Butler, L. The Effect of the Risser Stage on Bracing Outcome in Adolescent Idiopathic Scoliosis. J. Bone Jt. Surg. Am. 2016, 98, 1253–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, D.E.; Richards, B.S.; Browne, R.H.; Herring, J.A. A comparison between the Boston brace and the Charleston bending brace in adolescent idiopathic scoliosis. Spine 1997, 22, 1302–1312. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of bracing in adolescents with idiopathic scoliosis. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, C.-L.; Piao, J.; Wong, M.S.; Chen, Z. Study of Textile Fabric Materials used in Spinal Braces for Scoliosis. J. Med. Biol. Eng. 2020, 40, 356–371. [Google Scholar] [CrossRef]
- Konieczny, M.R.; Hieronymus, P.; Krauspe, R. Time in brace: Where are the limits and how can we improve compliance and reduce negative psychosocial impact in patients with scoliosis? A retrospective analysis. Spine J. 2017, 17, 1658–1664. [Google Scholar] [CrossRef]
- Whitaker, A.T.; Hresko, M.T.; Miller, P.E.; Verhofste, B.P.; Beling, A.; Emans, J.B.; Karlin, L.I.; Hedequist, D.J.; Glotzbecker, M.P. Bracing for juvenile idiopathic scoliosis: Retrospective review from bracing to skeletal maturity. Spine Deform. 2022, 10, 1349–1358. [Google Scholar] [CrossRef]
- Costa, L.; Schlosser, T.P.C.; Jimale, H.; Homans, J.F.; Kruyt, M.C.; Castelein, R.M. The Effectiveness of Different Concepts of Bracing in Adolescent Idiopathic Scoliosis (AIS): A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2145. [Google Scholar] [CrossRef]
- Wittschieber, D.; Schmeling, A.; Schmidt, S.; Heindel, W.; Pfeiffer, H.; Vieth, V. The Risser sign for forensic age estimation in living individuals: A study of 643 pelvic radiographs. Forensic Sci. Med. Pathol. 2013, 9, 36–43. [Google Scholar] [CrossRef]
- Subramanian, S.; Viswanathan, V.K. Bone Age; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kawasaki, S.; Shigematsu, H.; Tanaka, M.; Suga, Y.; Yamamoto, Y.; Tanaka, Y. Is brace treatment unnecessary for cases of adolescent idiopathic scoliosis above Risser sign 3? J. Orthop. Sci. 2020, 25, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Glassman, S.; Horton, W.; Shaffrey, C.; Schwab, F.; Zebala, L.P.; Lenke, L.G.; Hilton, J.F.; Shainline, M.; Baldus, C.; et al. Does treatment (nonoperative and operative) improve the two-year quality of life in patients with adult symptomatic lumbar scoliosis: A prospective multicenter evidence-based medicine study. Spine 2009, 34, 2171–2178. [Google Scholar] [CrossRef] [PubMed]
- McAviney, J.; Mee, J.; Fazalbhoy, A.; Du Plessis, J.; Brown, B.T. A systematic literature review of spinal brace/orthosis treatment for adults with scoliosis between 1967 and 2018: Clinical outcomes and harms data. BMC Musculoskelet. Disord. 2020, 21, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Mauroy, J.C.; Lecante, C.; Barral, F.; Pourret, S. Prospective study of 158 adult scoliosis treated by a bivalve polyethylene overlapping brace and reviewed at least 5 years after brace fitting. Scoliosis Spinal Disord. 2016, 11, 28. [Google Scholar] [CrossRef] [Green Version]
- Koele, M.C.; Lems, W.F.; Willems, H.C. The Clinical Relevance of Hyperkyphosis: A Narrative Review. Front. Endocrinol. 2020, 11, 5. [Google Scholar] [CrossRef] [Green Version]
- Hofler, R.C.; Jones, G.A. Bracing for Acute and Subacute Osteoporotic Compression Fractures: A Systematic Review of the Literature. World Neurosurg. 2020, 141, e453–e460. [Google Scholar] [CrossRef]
- Bezalel, T.; Carmeli, E.; Been, E.; Kalichman, L. Scheuermann’s disease: Current diagnosis and treatment approach. J. Back Musculoskelet. Rehabil. 2014, 27, 383–390. [Google Scholar] [CrossRef]
- Palazzo, C.; Sailhan, F.; Revel, M. Scheuermann’s disease: An update. Jt. Bone Spine 2014, 81, 209–214. [Google Scholar] [CrossRef]
- Sachs, B.; Bradford, D.; Winter, R.; Lonstein, J.; Moe, J.; Willson, S. Scheuermann kyphosis. Follow-up of Milwaukee-brace treatment. J. Bone Jt. Surg. Am. 1987, 69, 50–57. [Google Scholar] [CrossRef]
- Weiss, H.R.; Dieckmann, J.; Gerner, H.J. Effect of intensive rehabilitation on pain in patients with Scheuermann’s disease. Stud. Health Technol. Inform. 2002, 88, 254–257. [Google Scholar]
- Montgomery, S.P.; Erwin, W.E. Scheuermann’s kyphosis-long-term results of Milwaukee braces treatment. Spine 1981, 6, 5–8. [Google Scholar] [CrossRef]
- Katzman, W.B.; Wanek, L.; Shepherd, J.A.; Sellmeyer, D.E. Age-related hyperkyphosis: Its causes, consequences, and management. J. Orthop. Sports Phys. Ther. 2010, 40, 352–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caitriona, C.; Mark, M.G.; Elaine, H.; Claire, G.; Michelle, F.; Persson, U.M.; Sherrington, C.; Blake, C. Management of hospitalised osteoporotic vertebral fractures. Arch. Osteoporos. 2020, 15, 14. [Google Scholar] [CrossRef]
- Kweh, B.T.S.; Lee, H.Q.; Tan, T.; Rutges, J.; Marion, T.; Tew, K.S.; Bhalla, V.; Menon, S.; Oner, F.C.; Fisher, C.; et al. The Role of Spinal Orthoses in Osteoporotic Vertebral Fractures of the Elderly Population (Age 60 Years or Older): Systematic Review. Glob. Spine J. 2021, 11, 975–987. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Pinto-Pinto, B.; Romero-Morales, C.; Lopez-Lopez, D.; de-Labra, C.; Garcia-Perez-de-Sevilla, G. Efficacy of Bracing on Thoracic Kyphotic Angle and Functionality in Women with Osteoporosis: A Systematic Review. Medicina 2022, 58, 693. [Google Scholar] [CrossRef] [PubMed]
- Di, G.; Di, G.T. Türk Geriatri Dergisi; Geriatri Derneği: Ankara, Turkey, 2006. [Google Scholar]
- Mak, S.K.D.; Accoto, D. Review of Current Spinal Robotic Orthoses. Healthcare 2021, 9, 70. [Google Scholar] [CrossRef] [PubMed]
- Bible, J.E.; Biswas, D.; Whang, P.G.; Simpson, A.K.; Rechtine, G.R.; Grauer, J.N. Postoperative bracing after spine surgery for degenerative conditions: A questionnaire study. Spine J. 2009, 9, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.P.; Tetreault, L.A.; Sorefan-Mangou, F.; Garwood, P.; Wilson, J.R. Efficacy, safety, and economics of bracing after spine surgery: A systematic review of the literature. Spine J. 2018, 18, 1513–1525. [Google Scholar] [CrossRef]
- Sinha, S.; Caplan, I.; Schuster, J.; Piazza, M.; Glauser, G.; Sharma, N.; Welch, W.C.; Osiemo, B.; Mcclintock, S.; Ozturk, A.K.; et al. Evaluation of Lumbar Spine Bracing as a Postoperative Adjunct to Single-level Posterior Lumbar Spine Surgery. Asian J. Neurosurg. 2020, 15, 333–337. [Google Scholar] [CrossRef]
- Bogaert, L.; Van Wambeke, P.; Thys, T.; Swinnen, T.W.; Dankaerts, W.; Brumagne, S.; Moke, L.; Peers, K.; Depreitere, B.; Janssens, L. Postoperative bracing after lumbar surgery: A survey amongst spinal surgeons in Belgium. Eur. Spine J. 2019, 28, 442–449. [Google Scholar] [CrossRef]
- Nasi, D.; Dobran, M.; Pavesi, G. The efficacy of postoperative bracing after spine surgery for lumbar degenerative diseases: A systematic review. Eur. Spine J. 2020, 29, 321–331. [Google Scholar] [CrossRef]
- Hasan, S.; Babrowicz, J.; Waheed, M.A.; Piche, J.D.; Patel, R.; Aleem, I. The Utility of Postoperative Bracing on Radiographic and Clinical Outcomes Following Cervical Spine Surgery: A Systematic Review. Glob. Spine J. 2022, 21925682221098361. [Google Scholar] [CrossRef]
- Caplan, I.; Sinha, S.; Schuster, J.; Piazza, M.; Glauser, G.; Osiemo, B.; McClintock, S.; Welch, W.; Sharma, N.; Ozturk, A.; et al. The Utility of Cervical Spine Bracing as a Postoperative Adjunct to Single-level Anterior Cervical Spine Surgery. Asian J. Neurosurg. 2019, 14, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Dailey, A.T.; Ghogawala, Z.; Choudhri, T.F.; Watters, W.C.; Resnick, D.K.; Sharan, A.; Eck, J.C.; Mummaneni, P.V.; Wang, J.C.; Groff, M.W.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 14: Brace therapy as an adjunct to or substitute for lumbar fusion. J. Neurosurg. Spine 2014, 21, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Yan, C.; Avadhani, N.G.; Iqbal, J. The effects of smoke carcinogens on bone. Curr. Osteoporos. Rep. 2011, 9, 202–209. [Google Scholar] [CrossRef]
- Duetzmann, S.; Cole, T.; Senft, C.; Seifert, V.; Ratliff, J.K.; Park, J. Clavicle pain and reduction of incisional and fascial pain after posterior cervical surgery. J. Neurosurg. Spine 2015, 23, 684–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Duijvenbode, I.C.; Jellema, P.; van Poppel, M.N.; van Tulder, M.W. Lumbar supports for prevention and treatment of low back pain. Cochrane Database Syst. Rev. 2008, 2008, CD001823. [Google Scholar] [CrossRef]
- Schott, C.; Zirke, S.; Schmelzle, J.M.; Kaiser, C.; Fernandez, L.A.I. Effectiveness of lumbar orthoses in low back pain: Review of the literature and our results. Orthop. Rev. 2018, 10, 7791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annaswamy, T.M.M.; Cunniff, K.J.; Kroll, M.M.; Yap, L.; Hasley, M.D.; Lin, C.-K.; Petrasic, J. Lumbar Bracing for Chronic Low Back Pain: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2021, 100, 742–749. [Google Scholar] [CrossRef]
- Mu, X.; Peng, W.; Ou, Y.; Li, P.; Li, Z.; Wei, J. Non-surgical therapy for the treatment of chronic low back pain in patients with Modic changes: A systematic review of the literature. Heliyon 2022, 8, e09658. [Google Scholar] [CrossRef]
- Azadinia, F.; Ebrahimi-Takamjani, I.; Kamyab, M.; Parnianpour, M.; Asgari, M. A RCT comparing lumbosacral orthosis to routine physical therapy on postural stability in patients with chronic low back pain. Med. J. Islam. Repub. Iran. 2017, 31, 26. [Google Scholar] [CrossRef] [Green Version]
- Im, S.C.; Seo, S.W.; Kang, N.Y.; Jo, H.; Kim, K. The Effect of Lumbar Belts with Different Extensibilities on Kinematic, Kinetic, and Muscle Activity of Sit-to-Stand Motions in Patients with Nonspecific Low Back Pain. J. Pers. Med. 2022, 12, 1678. [Google Scholar] [CrossRef]
- Phaner, V.; Fayolle-Minon, I.; Lequang, B.; Valayer-Chaleat, E.; Calmels, P. Are there indications (other than scoliosis) for rigid orthopaedic brace treatment in chronic, mechanical low back pain? Ann. Phys. Rehabil. Med. 2009, 52, 382–393. [Google Scholar] [CrossRef] [Green Version]
- Harman, E.A.; Rosenstein, R.M.; Frykman, P.N.; Nigro, G.A. Effects of a belt on intra-abdominal pressure during weight lifting. Med. Sci. Sports Exerc. 1989, 21, 186–190. [Google Scholar] [CrossRef] [Green Version]
- Fares, M.Y.; Fares, J.; Salhab, H.A.; Khachfe, H.H.; Bdeir, A.; Fares, Y. Low Back Pain Among Weightlifting Adolescents and Young Adults. Cureus 2020, 12, e9127. [Google Scholar] [CrossRef]
- Samani, M.; Shirazi, Z.R.; Hadadi, M.; Sobhani, S. A randomized controlled trial comparing the long-term use of soft lumbosacral orthoses at two different pressures in patients with chronic nonspecific low back pain. Clin. Biomech. 2019, 69, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Bin, Y.U. A Review: Biomechanical Substitutions during Pregnancy and Application of Orthoses". J. Univ. Med. Dent. Coll. 2022, 13, 446–452. [Google Scholar] [CrossRef]
- Heydari, Z.; Aminian, G.; Biglarian, A.; Shokrpour, M.; Mardani, M.A. Comparison of the Modified Lumbar Pelvic Belt with the Current Belt on Low Back and Pelvic Pain in Pregnant Women. J. Biomed. Phys. Eng. 2022, 12, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Borg-Stein, J.; Dugan, S.A.; Gruber, J. Musculoskeletal aspects of pregnancy. Am. J. Phys. Med. Rehabil. 2005, 84, 180–192. [Google Scholar] [CrossRef]
- Carr, C.A. Use of a maternity support binder for relief of pregnancy-related back pain. J. Obstet. Gynecol. Neonatal Nurs. 2003, 32, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Barati, K.; Arazpour, M.; Vameghi, R.; Abdoli, A.; Farmani, F. The Effect of Soft and Rigid Cervical Collars on Head and Neck Immobilization in Healthy Subjects. Asian Spine J. 2017, 11, 390–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron, M.H.; Monroe, L.G. Physical Rehabilitation: Evidence-Based Examination, Evaluation, and Intervention; Saunders/Elsevier: St. Louis, MO, USA, 2007. [Google Scholar]
- Muzin, S.; Isaac, Z.; Walker, J.; Abd, O.E.; Baima, J. When should a cervical collar be used to treat neck pain? Curr. Rev. Musculoskelet. Med. 2008, 1, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Karimi, M.T.; Kamali, M.; Fatoye, F. Evaluation of the efficiency of cervical orthoses on cervical fracture: A review of literature. J. Craniovertebr. Junction Spine. 2016, 7, 13–19. [Google Scholar] [CrossRef]
- Koutsogiannis, P.; Dowling, T.J. Halo Brace; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Lauweryns, P. Role of conservative treatment of cervical spine injuries. Eur. Spine J. 2010, 19 (Suppl. 1), S23–S26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebraheim, N.A.; Liu, J.; Patil, V.; Sanford, C.G.; Crotty, M.J.; Haman, S.P.; Yeasting, R.A. Evaluation of skull thickness and insertion torque at the halo pin insertion areas in the elderly: A cadaveric study. Spine J. 2007, 7, 689–693. [Google Scholar] [CrossRef]
- Glaser, J.A.; Whitehill, R.; Stamp, W.G.; Jane, J.A. Complications associated with the halo-vest. A review of 245 cases. J. Neurosurg. 1986, 65, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, H. Brace Treatment for Adolescent Idiopathic Scoliosis. J. Clin. Med. 2018, 7, 136. [Google Scholar] [CrossRef] [Green Version]
- Misterska, E.; Glowacki, J.; Glowacki, M.; Okret, A. Long-term effects of conservative treatment of Milwaukee brace on body image and mental health of patients with idiopathic scoliosis. PLoS ONE 2018, 13, e0193447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallstrom, K.; Cochran, T.; Nachemson, A. Long-term effects on personality development in patients with adolescent idiopathic scoliosis. Influence of type of treatment. Spine 1986, 11, 756–758. [Google Scholar] [CrossRef]
- Ali, A.; Fontanari, V.; Schmoelz, W.; Fontana, M. Actuator and Contact Force Modeling of an Active Soft Brace for Scoliosis. Bioengineering 2022, 9, 303. [Google Scholar] [CrossRef] [PubMed]
- Ye, B.K.; Kim, H.S.; Kim, Y.W. Correction of camptocormia using a cruciform anterior spinal hyperextension brace and back extensor strengthening exercise in a patient with Parkinson disease. Ann. Rehabil. Med. 2015, 39, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Abe, T.; Shibao, Y.; Takeuchi, Y.; Mataki, Y.; Amano, K.; Hioki, S.; Miura, K.; Noguchi, H.; Funayama, T.; Koda, M.; et al. Initial hospitalization with rigorous bed rest followed by bracing and rehabilitation as an option of conservative treatment for osteoporotic vertebral fractures in elderly patients: A pilot one arm safety and feasibility study. Arch. Osteoporos. 2018, 13, 134. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.W.; Yang, H.S.; Kim, Y.B.; Yang, J.C.; Kang, K.B.; Kim, T.W.; Park, K.H.; Jeon, K.S.; Shin, H.D.; Kim, Y.E.; et al. Comparison of the Effectiveness of Three Lumbosacral Orthoses on Early Spine Surgery Patients: A Prospective Cohort Study. Ann. Rehabil. Med. 2021, 45, 24–32. [Google Scholar] [CrossRef]
- Azadinia, F.; Ebrahimi, E.T.; Kamyab, M.; Parnianpour, M.; Cholewicki, J.; Maroufi, N. Can lumbosacral orthoses cause trunk muscle weakness? A systematic review of literature. Spine J. 2017, 17, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Cholewicki, J.; McGill, K.C.; Shah, K.R.; Lee, A.S. The effects of a three-week use of lumbosacral orthoses on trunk muscle activity and on the muscular response to trunk perturbations. BMC Musculoskelet. Disord. 2010, 11, 154. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.C.; Lin, H.H.; Chang, M.C. Bracing Following Transforaminal Lumbar Interbody Fusion is not Necessary for Patients with Degenerative Lumbar Spine Disease: A Prospective, Randomized Trial. Clin. Spine Surg. 2018, 31, E441–E445. [Google Scholar] [CrossRef] [PubMed]
- Yee, A.; Yoo, J.; Marsolais, E.; Carlson, G.; Poe-Kochert, C.; Bohlman, H.; Emery, S. Use of a postoperative lumbar corset after lumbar spinal arthrodesis for degenerative conditions of the spine. A prospective randomized trial. J. Bone Jt. Surg. Am. 2008, 90, 2062–2068. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Stegall, P.R.; Roye, D.P.; Agrawal, S.K. Robotic Spine Exoskeleton (RoSE): Characterizing the 3-D Stiffness of the Human Torso in the Treatment of Spine Deformity. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1026–1035. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Fontanari, V.; Schmölz, W.; Agrawal, S.K. Active Soft Brace for Scoliotic Spine: A Finite Element Study to Evaluate in-Brace Correction. Robotics 2022, 11, 37. [Google Scholar] [CrossRef]
- Rozek, K.; Jasiewicz, B. Effect of Preoperative SpineCor(R) Treatment on Surgical Outcome in Idiopathic Scoliosis: An Observational Study. Med. Sci. Monit. 2019, 25, 754–759. [Google Scholar] [CrossRef]
- Zeh, A.; Planert, M.; Klima, S.; Hein, W.; Wohlrab, D. The flexible Triac-Brace for conservative treatment of idiopathic scoliosis. An alternative treatment option? Acta Orthop. Belg. 2008, 74, 512–521. [Google Scholar] [PubMed]
- Guo, J.; Lam, T.P.; Wong, M.; Ng, B.K.W.; Lee, K.M.; Liu, K.L.; Hung, L.H.; Lau, A.H.Y.; Sin, S.W.; Kwok, W.K.; et al. A prospective randomized controlled study on the treatment outcome of SpineCor brace versus rigid brace for adolescent idiopathic scoliosis with follow-up according to the SRS standardized criteria. Eur. Spine J. 2014, 23, 2650–2657. [Google Scholar] [CrossRef] [PubMed]
- Norbury, J.W.; Mehta, S.K.; Danison, A.; Felsen, G.S. Braddom’s Physical Medicine and Rehabilitation, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Trauner, K.B. The Emerging Role of 3D Printing in Arthroplasty and Orthopedics. J. Arthroplast. 2018, 33, 2352–2354. [Google Scholar] [CrossRef] [PubMed]
- Barrios-Muriel, J.; Romero-Sanchez, F.; Alonso-Sanchez, F.J.; Rodriguez Salgado, D. Advances in Orthotic and Prosthetic Manufacturing: A Technology Review. Materials 2020, 13, 295. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Imaging of the Cervical Spine Is Recommended with Any of the Following NEXUS Criteria Present |
|---|
|
| Imaging of the Cervical Spine Is Recommended with Any of the Following CCR Criteria Present |
|---|
|
| Mechanism of Injury/Fracture Morphology | |
|
|
| Posterior Ligamentous Complex Integrity | |
|
|
| Neurologic Status | |
|
|
| Management | |
|
|
| Fracture Morphology | |
|
|
| Discoligamentous Complex | |
|
|
| Neurologic Status | |
|
|
| Continuous Cord Compression | |
|
|
| Management | |
|
|
| Types of Orthoses | Vertebral Regions Treated | Conditions Targeted | Subtypes |
|---|---|---|---|
| Cervical orthoses | C1-C6 | Whiplash related injures | Soft collars, rigid collars |
| Cervicothoracic orthoses | C6-T5 | Cranial, vertebral fractures, post-op care, scoliosis | SOMI, Halo, Minerva braces |
| Cervico-thoracic-lumbar-sacral orthoses | C2-L5 | Scoliosis | Milwaukee device |
| Thoraco-lumbo-sacral orthoses | T6-L4 | Idiopathic scoliosis, OVF, camptocormia | Boston, Charleston, Providence, Jewett, and CASH braces |
| Lumbosacral orthoses | L3-S1 | Degenerative lumbar vertebral conditions, lower back pain | Soft braces, rigid braces |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerillo, J.L.; Becsey, A.N.; Sanghadia, C.P.; Root, K.T.; Lucke-Wold, B. Spine Bracing: When to Utilize—A Narrative Review. Biomechanics 2023, 3, 136-154. https://doi.org/10.3390/biomechanics3010013
Cerillo JL, Becsey AN, Sanghadia CP, Root KT, Lucke-Wold B. Spine Bracing: When to Utilize—A Narrative Review. Biomechanics. 2023; 3(1):136-154. https://doi.org/10.3390/biomechanics3010013
Chicago/Turabian StyleCerillo, John L., Alexander N. Becsey, Chai P. Sanghadia, Kevin T. Root, and Brandon Lucke-Wold. 2023. "Spine Bracing: When to Utilize—A Narrative Review" Biomechanics 3, no. 1: 136-154. https://doi.org/10.3390/biomechanics3010013