

Seroepidemiology of Toxoplasmosis in Hemodialysis Patients in Senegal
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Study Participants
2.2. Toxoplasmosis Seroprevalence
3. Discussion
4. Materials and Methods
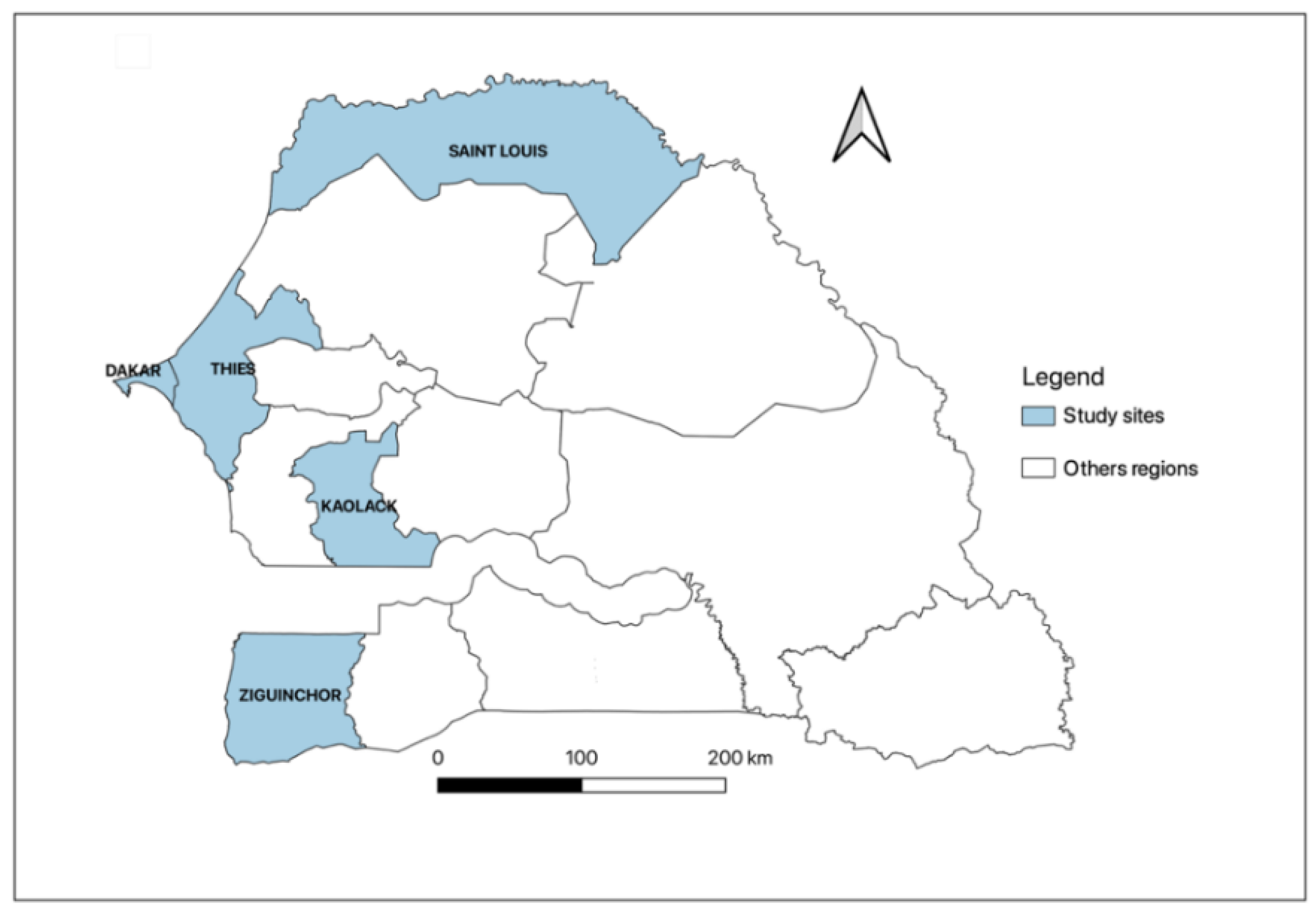
4.1. Study Areas
4.2. Toxoplasma gondii Antibodies Detection
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skariah, S.; McIntyre, M.K.; Mordue, D.G. Toxoplasma gondii: Determinants of tachyzoite to bradyzoite conversion. Parasitol. Res. 2010, 107, 253–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert-Gangneux, F.; Dardé, M.L. Epidemiology of and diagnostic strategies for toxoplasmosis. Clin. Microbiol. Rev. 2012, 25, 264–296. [Google Scholar] [CrossRef] [Green Version]
- Montoya, J.G.; Liesenfeld, O. Toxoplasmosis. Lancet 2004, 363, 1965–1976. [Google Scholar] [CrossRef]
- Pott, H.; Castelo, A. Isolated cerebellar toxoplasmosis as a complication of HIV infection. Int. J. STD AIDS 2013, 24, 70–72. [Google Scholar] [PubMed]
- Agrawal, S.R.; Singh, V.; Ingale, S.; Jain, A.P. Toxoplasmosis of spinal cord in acquired immunodeficiency syndrome patient presenting as paraparesis: A rare entity. J. Glob. Infect. Dis. 2014, 6, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, S.; Ferreira, E.; Ramos, I.; Martins, R.; De Freitas, L.; Borges, J.L. Cerebral toxoplasmosis after renal transplantation. Case report and review. Acta Med. Port. 1994, 7 (Suppl. 1), S61–S66. [Google Scholar]
- AdouBryn, K.D.; Ouhon, J.; Nemer, J.; Yapo, C.G.; Assoumou, A. Serological survey of acquired toxoplasmosis in women of child-bearing age in Yopougon (Abidjan, Côte d’Ivoire). Bull. Soc. Pathol. Exot. 2004, 97, 345–348. [Google Scholar]
- Barratt, J.L.N.; Harkness, J.; Marriott, D.; Ellis, J.T.; Stark, D. Importance of nonenteric protozoan infections in immunocompromised people. Clin. Microbiol. Rev. 2010, 23, 795–836. [Google Scholar] [CrossRef] [Green Version]
- Murat, J.B.; Hidalgo, H.F.; Brenier-Pinchart, M.P.; Pelloux, H. Human toxoplasmosis: Which biological diagnostic tests are best suited to which clinical situations? Expert Rev. Anti Infect. Ther. 2013, 11, 943–956. [Google Scholar] [CrossRef]
- Contini, C. Clinical and diagnostic management of toxoplasmosis in the immunocompromised patient. Parassitologia 2008, 50, 45–50. [Google Scholar]
- Bessières, M.H. Les infections parasitaires chez les transplantés. RFL 2008, 2008, 53–59. [Google Scholar] [CrossRef]
- Patrat-Delon, S.; Gangneux, J.P.; Lavoué, S.; Lelong, B.; Guiguen, C.; Le Tulzo, Y. Correlation of parasite load determined by quantitative PCR to clinical outcome in a heart transplant patient with disseminated toxoplasmosis. J. Clin. Microbiol. 2010, 48, 2541–2545. [Google Scholar] [CrossRef] [Green Version]
- Desoubeaux, G.; Perret-Gallix, K.; MacHet, M.C.; Sirinelli, A.; Bailly, É.; Van Langendonck, N. Toxoplasmic cyst and heart transplant: A case report of serological reactivation in an acute graft rejection context. Ann. Biol. Clin. 2012, 70, 323–328. [Google Scholar] [CrossRef]
- Seck, S.M.; Mbow, M.; Kane, Y.; Cisse, M.M.; Faye, G.; Kama, A. Prevalence of SARS-CoV-2 antibodies in hemodialysis patients in Senegal: A multicenter cross-sectional study. BMC Nephrol. 2021, 22, 384. [Google Scholar] [CrossRef]
- Lo, G.; Diouf, N.N.; Faye, B.; Seck, M.C.; Diawara, P.S.; Ba, I. Toxoplasmosis prevalence among pregnant women attending at the Military hospital of Ouakam Laboratory, Dakar. MAN 2012, 59, 7. [Google Scholar]
- Tine, R.C.K.; Dieng, T.; Sylla, K.; Sow, D.; Lelo, S.; Dia, M. Trends in toxoplasmosis seroprevalence among pregnant women attending the Fann Teaching Hospital in Dakar Senegal. JPVB 2017, 9, 146–152. [Google Scholar]
- Seck, M.C.; Faye, B.; Mbow, M.; Ndiaye, M.; Badiane, A.S.; Diongue, K. Serological study on toxoplasmosis among pregnant women attending at military hospital of Ouakam, Dakar. Dakar Med. 2015, 60, 7. [Google Scholar]
- Nissapatorn, V.; Leong, T.H.; Lee, R.; Init, I.; Ibrahim, J.; Yen, T.S. Seroepidemiology of toxoplasmosis in renal patients. Southeast Asian J. Trop. Med. 2011, 42, 237–247. [Google Scholar]
- Ocak, S.; Duran, N.; Eskiocak, A.F.; Aytac, H. Anti-Toxoplasma gondii antibodies in hemodialysis patients receiving long-term hemodialysis therapy in Turkey. Saudi Med. J. 2005, 26, 1378–1382. [Google Scholar]
- Seyyedpour, S.H.; Afshar, P.; Barzegarnejad, A.; Kalhori, S.; Agah, R. Evaluation of Anti-Toxoplasma gondii Antibodies in Hemodialysis Patients with Chronic Kidney Disease in Sari, Iran. Nephrourol. Mon. 2016, 8, e40182. [Google Scholar] [CrossRef] [Green Version]
- Mpiga Mickoto, B.; Mickoto, B.M.; Akue, J.P.; Bisvigou, U.; Tsonga, S.M.; Nkoghe, D. Étude sérologique de la toxoplasmose chez les femmes enceintes de Franceville, Gabon. Bull. Soc. Pathol. Exot. 2010, 103, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Gamba, E.P.; Nambei, W.S.; Kamandji, L. Integrated screening for HIV, syphilis, and toxoplasmosis among pregnant women in the Central African Republic. Med. Sante Trop. 2013, 23, 421–426. [Google Scholar] [CrossRef] [PubMed]
- El Mansouri, B.; Rhajaoui, M.; Sebti, F.; Amarir, F.; Laboudi, M.; Bchitou, R.; Hamad, M.; Lyagoubi, M. Seroprevalence of toxoplasmosis in pregnant women in Rabat, Morocco. Bull. Soc. Pathol. Exot. 2007, 100, 289–290. [Google Scholar]
- Olusi, T.; Groß, U.; Ajayi, J. High incidence of toxoplasmosis during pregnancy in Nigeria. Scand. J. Infect. Dis. 1996, 28, 645–646. [Google Scholar] [CrossRef]
- Messerer, L.; Bouzbid, S.; Gourbdji, E.; Mansouri, R.; Bachi, F. Seroprevalence of toxoplasmosis in pregnant women in Annaba, Algeria. Rev. Epidemiol. Sante Publique 2014, 62, 160–165. [Google Scholar] [CrossRef]
- Rostami, M.N.; Eskandari, E.; Garoosi, Z.; Mohajeri, N.; Rezaian, M.; Keshavarz, H. Serological Study of Toxoplasma gondii Infection Using IFA Method in Renal Transplant Recipients. IJP 2006, 1, 31–39. [Google Scholar]
- Mostafa, N.E.S.; Abdel Hamed, E.F.; Rashed, H.E.S.; Mohamed, S.Y.; Abdelgawad, M.S.; Elasbali, A.M. The relationship between toxoplasmosis and different types of human tumors. J. Infect. Dev. Ctries. 2018, 12, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Alvarado-Esquivel, C.; Pacheco-Vega, S.J.; Hernández-Tinoco, J.; Sánchez-Anguiano, L.F.; Berumen-Segovia, L.O.; Rodríguez-Acevedo, F.J.I.; Beristain-García, I.; Rábago-Sánchez, E.; Liesenfeld, O.; Campillo-Ruiz, F.; et al. Seroprevalence of Toxoplasma gondii infection and associated risk factors in Huicholes in Mexico. Parasites Vectors 2014, 7, 301. [Google Scholar] [CrossRef] [Green Version]
- Saadat, F.; Mahmoudi, M.R.; Rajabi, E.; Roshan, Z.A.; Shad, B.M.; Karanis, P. Seroepidemiology and Associated Risk Factors of Toxoplasma gondii in Hemodialysis Patients. Acta Parasitol. 2020, 65, 906–912. [Google Scholar] [CrossRef]
- Soltani, S.; Kahvaz, M.S.; Soltani, S.; Maghsoudi, F.; Foroutan, M. Seroprevalence and associated risk factors of Toxoplasma gondii infection in patients undergoing hemodialysis and healthy group. BMC Res. Notes 2020, 13, 551. [Google Scholar] [CrossRef]
- Frimpong, C.; Makasa, M.; Sitali, L.; Michelo, C. Seroprevalence and determinants of toxoplasmosis in pregnant women attending antenatal clinic at the university teaching hospital, Lusaka, Zambia. BMC Infect. Dis. 2017, 17, 10. [Google Scholar] [CrossRef] [Green Version]
- Al-Malki, E.S. Toxoplasmosis: Stages of the protozoan life cycle and risk assessment in humans and animals for an enhanced awareness and an improved socio-economic status. Saudi J. Biol. Sci. 2021, 28, 962–969. [Google Scholar] [CrossRef]
- Yasodhara, P.; Ramalakshmi, B.; Lakshmi, V.; Krishna, T. Socioeconomic status and prevalence of toxoplasmosis during pregnancy. IJMM 2004, 22, 241–243. [Google Scholar] [CrossRef]
- Oakes, J.M.; Rossi, P.H. The measurement of SES in health research: Current practice and steps toward a new approach. Soc. Sci. Med. 2003, 56, 769–784. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| % (n) | 95% CI | |
|---|---|---|
| Age group (years) | ||
| 18–30 | 23% (48) | 17–29 |
| 31–45 | 38% (80) | 31–45 |
| 46–60 | 27% (58) | 22–34 |
| 61–77 | 12% (25) | 8.0–17 |
| Region | ||
| Dakar | 41% (87) | 35–48 |
| Kaolack | 17% (36) | 12–23 |
| Saint-Louis | 13% (27) | 8.7–18 |
| Thies | 16% (34) | 12–22 |
| Ziguinchor | 13% (27) | 8.7–18 |
| Sex | ||
| Female | 45% (94) | 38–52 |
| Male | 55% (117) | 48–62 |
| Education level | ||
| Illiterate | 26% (54) | 20–32 |
| Primary | 33% (69) | 27–40 |
| Secondary | 27% (58) | 22–34 |
| University | 14% (30) | 9.9–20 |
| Socioeconomic status | ||
| High | 23.2% (49) | 18–30 |
| Low | 41.7% (88) | 35–49 |
| Moderate | 35.1% (74) | 29–42 |
| Cat with contact | ||
| No | 71.6% (151) | 65–77 |
| Yes | 28.4% (60) | 23–35 |
| Positive IgG, n (%, (95%CI)) | Overall, N = 211 | p-Value | |
|---|---|---|---|
| Age group | |||
| 18–30 | 17 (35.4, (23–51)) | 48 (100%) | 0.4 |
| 31–45 | 33 (41.2, (31–53)) | 80 (100%) | |
| 46–60 | 24 (41.4, (29–55)) | 58 (100%) | |
| 61–77 | 14 (56.0, (35–75)) | 25 (100%) | |
| Region | |||
| Dakar | 38 (43.7, (33–55)) | 87 (100%) | >0.9 |
| Kaolack | 16 (44.4, (28–62)) | 36 (100%) | |
| Saint-Louis | 9 (33.3, (17–54)) | 27 (100%) | |
| Thies | 14 (41.2, (25–59)) | 34 (100%) | |
| Ziguinchor | 11 (40.7, (23–61)) | 27 (100%) | |
| Sex | |||
| Female | 36 (38.3, (29–49)) | 94 (100%) | 0.4 |
| Male | 52 (44.4, (35–54)) | 117 (100%) | |
| Education level | |||
| Illiterate | 31 (57.4, (43–70)) | 54 (100%) | 0.036 |
| Primary | 28 (40.6, (29–53)) | 69 (100%) | |
| Secondary | 18 (31.0, (20–45)) | 58 (100%) | |
| University | 11 (36.7, (21–56)) | 30 (100%) | |
| Socioeconomic status | |||
| High | 18 (36.7, (24–52)) | 49 (100%) | 0.7 |
| Low | 38 (43.1, (33–54)) | 88 (100%) | |
| Moderate | 32 (43.2, (32–55)) | 74 (100%) | |
| Conctact with cat | |||
| No contact | 63 (41.7, (34–50)) | 151 (100%) | >0.9 |
| Contact | 25 (41.6, (29–55)) | 60 (100%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seck, M.C.; Mbow, M.; Seck, S.M.; Dia, Y.A.; Diallo, I.; Cisse, M.; Gningue, M.; Daou, V.; Coundoul, B.; Kane, Y.; et al. Seroepidemiology of Toxoplasmosis in Hemodialysis Patients in Senegal. Parasitologia 2023, 3, 142-150. https://doi.org/10.3390/parasitologia3020015
Seck MC, Mbow M, Seck SM, Dia YA, Diallo I, Cisse M, Gningue M, Daou V, Coundoul B, Kane Y, et al. Seroepidemiology of Toxoplasmosis in Hemodialysis Patients in Senegal. Parasitologia. 2023; 3(2):142-150. https://doi.org/10.3390/parasitologia3020015
Chicago/Turabian StyleSeck, Mame Cheikh, Moustapha Mbow, Sidy Mohamed Seck, Yacine Ameth Dia, Ibrahima Diallo, Marouba Cisse, Moctar Gningue, Victoria Daou, Baratou Coundoul, Yaya Kane, and et al. 2023. "Seroepidemiology of Toxoplasmosis in Hemodialysis Patients in Senegal" Parasitologia 3, no. 2: 142-150. https://doi.org/10.3390/parasitologia3020015