
Retrospective Assessment of The Intestinal Protozoan Distribution in Patients Admitted to The Hospital Aristide Le Dantec in Dakar, Senegal, from 2011 to 2020
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Description of the Study Population
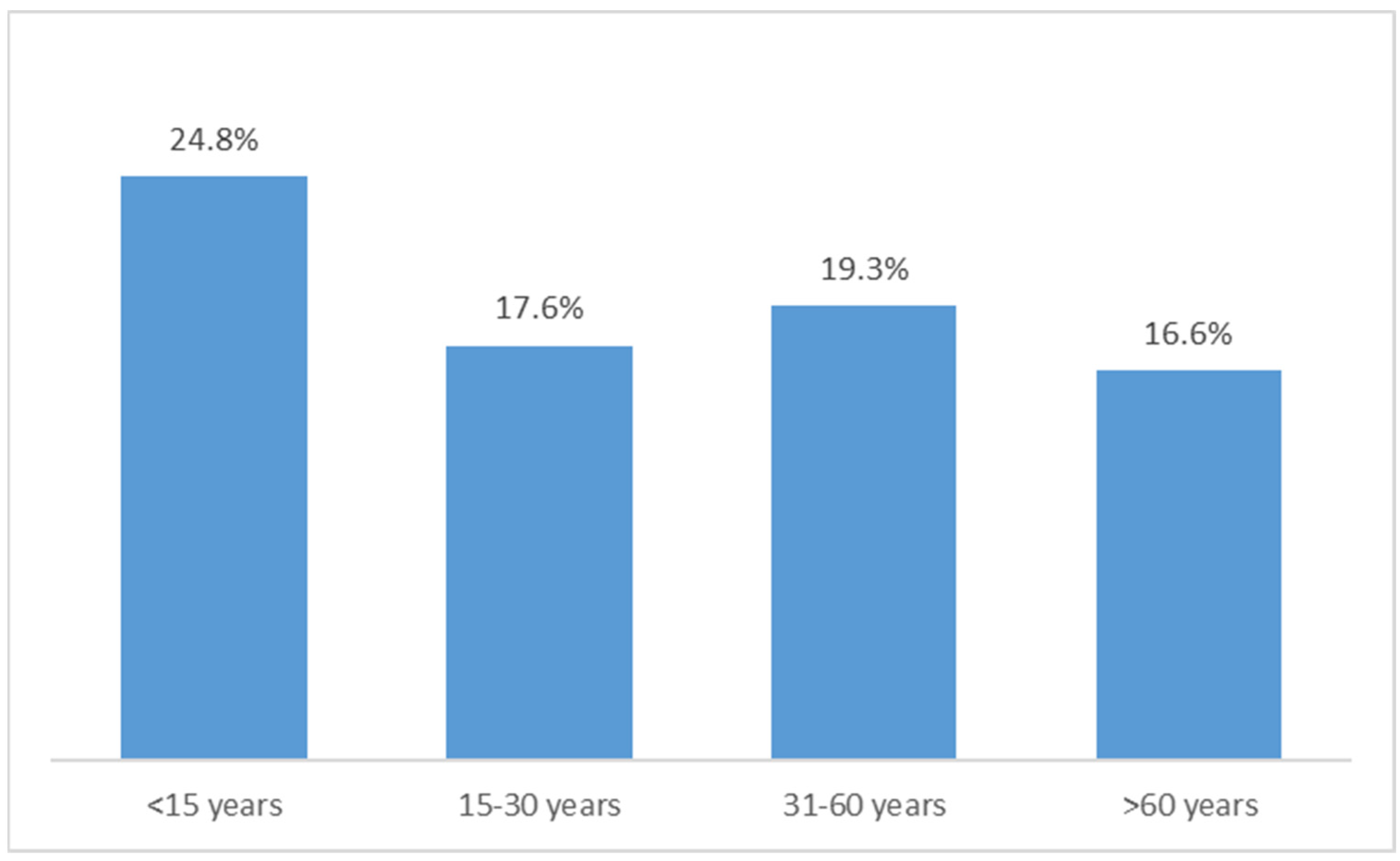
2.2. Indices of Parasites and Variation in Prevalence of Intestinal Protozoan by Study Year and Age Groups
2.3. Pattern of Identified Species
2.4. Factors Associated with Intestinal Protozoan Infections
3. Discussion
4. Methodology
4.1. Area and Population Studied
4.2. Fecal Sample Analysis
4.3. Analysis of the Data
- -(i)
- Simple parasitic index (SPI) is the percentage of subjects parasitized in relation to the total number of fecal parasitological examinations carried out multiplied by one hundred.
- -(ii)
- Corrected parasitic index (CPI) is the ratio of number of parasites identified to the number of total examinations multiplied by one hundred.
- -(iii)
- Polyparasitism index (PPI) is the coexistence in the same individual of two or more parasitic species. The PPI I derived from the difference between the CPI and the SPI.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, W.; Arshad, S.; Khatoon, N.; Khan, I.; Ahmad, N.; Kamal, M.; UlHassan, H.; Khan, N.; Haq, A.U.; Ilyas, M.; et al. Food handlers: An important reservoir of protozoans and helminth parasites of public health importance. Braz. J. Biol. 2021, 82. [Google Scholar] [CrossRef] [PubMed]
- Hailegebriel, T. Prevalence of intestinal parasitic infections and associated risk factors among students at Dona Berber primary school, Bahir Dar. Ethiopia. BMC Infect. Dis. 2017, 17, 362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amer, O.S.O.; Al-Malki, E.S.; Waly, M.; Alageel, A.; Lubbad, M.Y. Prevalence of Intestinal Parasitic Infections among Patients of King Fahd Medical City in Riyadh Region, Saudi Arabia: A 5-Year Retrospective Study. J. Parasitol. Res. 2018, 2018, 8076274. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J.; Brindley, P.J.; Bethony, J.M.; King, C.H.; Pearce, E.J.; Jacobson, J. Helminth infections: The great neglected tropical diseases. J. Clin. Investig. 2008, 118, 1311–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, S.; Stark, D.; Harkness, J.; Ellis, J. Enteric Protozoa in the Developed World: A Public Health Perspective. Clin. Microbiol. Rev. 2012, 25, 420–449. [Google Scholar] [CrossRef] [Green Version]
- Dawson, D. Foodborne protozoan parasites. Int. J. Food Microbiol. 2005, 103, 207–227. [Google Scholar] [CrossRef]
- Giangaspero, A.; Gasser, R.B. Human cyclosporiasis. Lancet Infect. Dis. 2019, 19, e226–e236. [Google Scholar] [CrossRef]
- Ryan, U.; Hijjawi, N.; Xiao, L. Foodborne cryptosporidiosis. Int. J. Parasitol. 2018, 48, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Ryan, U.; Hijjawi, N.; Feng, Y.; Xiao, L. Giardia: An under-reported foodborne parasite. Int. J. Parasitol. 2018, 49, 1–11. [Google Scholar] [CrossRef]
- Levecke, B.; Montresor, A.; Albonico, M.; Ame, S.M.; Behnke, J.M.; Bethony, J.M.; Noumedem, C.D.; Engels, D.; Guillard, B.; Kotze, A.C.; et al. Assessment of anthelmintic effica-cy of mebendazole in school children in six countries where soil-transmitted helminths are endemic. PLoS Negl. Trop Dis. 2014, 8, e3204. [Google Scholar] [CrossRef]
- Gabrielli, A.-F.; Montresor, A.; Chitsulo, L.; Engels, D.; Savioli, L. Preventive chemotherapy in human helminthiasis: Theoretical and operational aspects. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 683–693. [Google Scholar] [CrossRef] [Green Version]
- Loiseau, P.; Le Bras, J. New drugs against parasitic diseases. Rev. Prat. 2007, 57, 175–182. [Google Scholar]
- Tine, R.C.K.; Faye, B.; Ndour, C.T.; Sylla, K.; Sow, D.; Ndiaye, M.; Ndiaye, J.L.; Magnussen, P.; Alifrangis, M.; Bygbjerg, I.C.; et al. Parasitic Infections among Children under Five Years in Senegal: Prevalence and Effect on Anaemia and Nutritional Status. ISRN Parasitol. 2013, 2013, 272701. [Google Scholar] [CrossRef] [Green Version]
- Diongue, K.; Ndiaye, M.; Seck, M.C.; Diallo, M.A.; Ndiaye, Y.D.; Badiane, A.S.; Ndiaye, D. Distribution of Parasites Detected in Stool Samples of Patients in Le Dantec University Hospital of Dakar, Senegal, from 2011 to 2015. J. Trop. Med. 2017, 2017, 8296313. [Google Scholar] [CrossRef] [Green Version]
- Lelo, S.; Ly, F.; Lam, A.; Fall, C.B.; Manga, I.; Tairou, F. Detection of Intestinal Parasites in Stool Samples by Mi-croscopy and Real-Time PCR in Children with Vulnerable Living Conditions in Dakar, Senegal. J. Bacteriol. Parasitol. 2021, 12, 398. [Google Scholar]
- Sylla, K.; Tine, R.C.K.; Sow, D. Aspects épidémiologiques des parasitoses intestinales diagnostiquées au la-boratoire de parasitologie-mycologie du centre national hospitalier de Fann, Dakar. Med. Afr. Noire 2013, 60, 339–346. [Google Scholar]
- Khaled, S.; Gantois, N.; Ly, A.T.; Senghor, S.; Even, G.; Dautel, E.; Dejager, R.; Sawant, M.; Baydoun, M.; Benamrouz-Vanneste, S.; et al. Prevalence and Subtype Distribution of Blastocystis sp. in Senegalese School Children. Microorganisms 2020, 8, 1408. [Google Scholar] [CrossRef]
- Ouattara, M.; N’Guéssan, N.A.; Yapi, A.; N’Goran, E.K. Prevalence and Spatial Distribution of Entamoeba histolytica/dispar and Giardia lamblia among Schoolchildren in Agboville Area (Côte d’Ivoire). PLoS Negl. Trop. Dis. 2010, 4, e574. [Google Scholar] [CrossRef]
- Wale, M.; Gedefaw, S. Prevalence of Intestinal Protozoa and Soil Transmitted Helminths Infections among School Children in Jaragedo Town, South Gondar Zone of Ethiopia. J. Trop. Med. 2022, 2022, 5747978. [Google Scholar] [CrossRef]
- Hajissa, K.; Islam, M.A.; Sanyang, A.M.; Mohamed, Z. Prevalence of intestinal proto-zoan parasites among school children in africa: A systematic review and meta-analysis. PLoS Negl. Trop Dis. 2022, 16, e0009971. [Google Scholar] [CrossRef]
- Abu-Madi, M.A.; Behnke, J.M.; Boughattas, S.; Al-Thani, A.; Doiphode, S.H. A decade of intestinal protozoan epidemi-ology among settled immigrants in Qatar. BMC Infect. Dis. 2016, 16, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noor Azian, M.Y.; San, Y.M.; Gan, C.C.; Yusri, M.Y.; Nurulsyamzawaty, Y.; Zuhaizam, A.H.; Maslawaty, M.N.; Norparina, I.; Vythilingam, I. Prevalence of intestinal protozoa in an aborigine community in Pahang, Malaysia. Trop. Biomed. 2007, 24, 55–62. [Google Scholar] [PubMed]
- Dobo, B. Prevalence of intestinal protozoan infection among patients in Hawassa city administration millennium health center, Ethiopia. J. Appl. Biotechnol. Bioeng. 2018, 5, 206–210. [Google Scholar] [CrossRef] [Green Version]
- Flores, A.; Esteban, J.G.; Angles, R.; Mas-Coma, S. Soil transmitted helminthes infection at very high altitude in Bolivia. Trans. R. Soc. Trop. Med. Hyg. 2001, 95, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Omar, M.; Abdelal, H.O. Current status of intestinal parasitosis among patients attending teaching hospitals in Zagazig district, Northeastern Egypt. Parasitol. Res. 2022, 121, 1651–1662. [Google Scholar] [CrossRef]
- Aschale, Y.; Minwuyelet, A.; Akalu, T.Y.; Talie, A. Prevalence of Intestinal Parasite Infections and Associated Factors among Pregnant Women in Northwest Ethiopia. J. Parasitol. Res. 2022, 2022, 9065425. [Google Scholar] [CrossRef]
- Akinbo, F.; Omoregie, R.; Eromwon, R.; Igbenimah, I.; Airueghiomon, U.-E. Prevalence of intestinal parasites among patients of a tertiary hospital in Benin city, Nigeria. N. Am. J. Med. Sci. 2011, 3, 462–464. [Google Scholar] [CrossRef] [Green Version]
- Hailu, G.G.; Ayele, E.T. Assessment of the prevalence of intestinal parasitic infections and associated habit and culture-related risk factors among primary schoolchildren in Debre Berhan town, Northeast Ethiopia. BMC Public Health 2021, 21, 112. [Google Scholar] [CrossRef]
- Hussein, A.H.; Rashed, S.M.; El-Hayawan, I.A.; Ali, N.S.; Ouf, E.A.A.; Ali, A.T. Intestinal Parasite Infections and Accuracy of Direct Thin and Thick Smear, Formol-Ether Sedimentation, Centrifugal Flotation, and Mini-FLOTAC Techniques among Patients with Gastrointestinal Tract Disorders from the Greater Cairo Region, Egypt. Am. J. Trop. Med. Hyg. 2017, 96, 589–594. [Google Scholar] [CrossRef] [Green Version]
- Abbaszadeh Afshar, M.J.; Barkhori Mehni, M.; Rezaeian, M.; Mohebali, M.; Baigi, V.; Amiri, S.; Amirshekari, M.B.; Ha-midinia, R.; Samimi, M. Prevalence and associated risk factors of human intestinal parasitic infections: A popula-tion-based study in the southeast of Kerman province, southeastern Iran. BMC Infect Dis. 2020, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- El Guamri, Y.; Belghyti, D.; Achicha, A.; Tiabi, M.; Aujjar, N.; Barkia, A.; El Kharrim, K.; Barkia, H.; El-Fellaki, E.; Mousahel, R.; et al. Enquête épidémiologique rétrospective sur les parasitoses intes-tinales au Centre hospitalier provincial El Idrissi (Kénitra, Maroc): Bilan de 10 ans (1996–2005). Ann. Biol. Clin. 2009, 67, 191–202. [Google Scholar]
- Baba, O.A.S.C.; Aminetou, B.M.; Ba, O.; Mouhamedou, K.; Elhdj, D.; Samba, H.; Abdallahi, M.O.; Lo, B. Prevalence of intestinal parasites among school children in the Gorgol, Guidimagha and Brakna area (Mauritania). Rev. Francoph. Lab. 2012, 440, 75–78. [Google Scholar]
- Fonseca, R.E.P.D.; Barbosa, M.C.R.; Ferreira, B.R. High prevalence of enteroparasites in children from Ribeirão Preto, São Paulo, Brazil. Rev. Bras. Enferm. 2017, 70, 566–571. [Google Scholar] [CrossRef] [Green Version]
- Eroglu, F.; Koltas, I.S. Evaluation of the transmission mode of B. hominis by using PCR method. Parasitol. Res. 2010, 107, 841–845. [Google Scholar] [CrossRef]
- Parkar, U.; Traub, R.J.; Vitali, S.; Elliot, A.; Levecke, B.; Robertson, I.; Geurden, T.; Steele, J.; Drake, B.; Thompson, R.A. Molecular characterization of Blastocystis iso-lates from zoo animals and their animal- keepers. Vet. Parasitol. 2010, 169, 8–17. [Google Scholar] [CrossRef]
- Polis, M.A.; Tuazon, C.U.; Alling, D.W.; Talmanis, E. Transmission of Giardia lamblia from a day care center to the community. Am. J. Public Health 1986, 76, 1142–1144. [Google Scholar] [CrossRef] [Green Version]
- Gendrel, D.; Treluyer, J.M.; Richard-Lenoble, D. Parasitic diarrhea in normal and malnourished children. Fundam. Clin. Pharmacol. 2003, 17, 189–197. [Google Scholar] [CrossRef]
- Wahdini, S.; Putra, V.P.; Sungkar, S. The Prevalence of Intestinal Protozoan Infections among Children in Southwest Sumba Based on the Type of Water Sources. Infect. Chemother. 2021, 53, 519–527. [Google Scholar] [CrossRef]
- McHardy, I.H.; Wu, M.; Shimizu-Cohen, R.; Couturier, M.R.; Humphries, R.M. Detection of Intestinal Protozoa in the Clinical Laboratory. J. Clin. Microbiol. 2014, 52, 712–720. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Number | Percentage | CI 95% | |
|---|---|---|---|
| Years | |||
| 2011 | 408 | 11.98 | (10.93–13.11) |
| 2012 | 437 | 12.83 | (11.74–13.99) |
| 2013 | 344 | 10.1 | (09.13–11.15) |
| 2014 | 313 | 9.19 | (08.26–10.20) |
| 2015 | 292 | 8.57 | (07.68–09.56) |
| 2016 | 416 | 12.21 | (11.15–13.35) |
| 2017 | 414 | 12.15 | (11.10–13.29) |
| 2018 | 343 | 10.07 | (09.10–11.12) |
| 2019 | 252 | 7.4 | (06.56–08.33) |
| 2020 | 188 | 5.52 | (04.80–06.34) |
| Age group | |||
| <15 yrs | 302 | 8.86 | (07.95–09.87) |
| 15–30 yrs | 1139 | 33.43 | (31.87–35.03) |
| 31–60 yrs | 1562 | 45.85 | (44.18–47.52) |
| >60 yrs | 404 | 11.86 | (10.81–12.99) |
| Gender | |||
| Male | 1735 | 50.92 | (49.24–52.60) |
| Female | 1672 | 49.08 | (47.40–50.76) |
| Service | |||
| Hospitalized | 896 | 26.3 | (24.85–27.8) |
| Non-hospitalized | 2511 | 73.7 | (72.2–75.15) |
| Seasons | |||
| Dry | 2814 | 82.59 | (81.28–83.83) |
| Rainy | 593 | 17.41 | (16.17–18.72) |
| Intestinal parasites | |||
| Negative | 2762 | 81.07 | (79.72–82.35) |
| Positive | 645 | 18.93 | (17.65–20.28) |
| Species | Frequency | Percentage | CI 95% |
|---|---|---|---|
| Negative | 2762 | 81.07 | (79.72–82.35) |
| Monoparasitism | 579 | 16.99 | (15.77–18.29) |
| Entamoeba coli | 234 | 6.87 | (06.07–07.77) |
| Blastocystis hominis | 194 | 5.69 | (04.96–06.52) |
| Entamoeba histolytica/dispar | 79 | 2.31 | (01.86–02.88) |
| Giardia intestinalis | 45 | 1.32 | (0.99–01.76) |
| Trichomonas intestinalis | 18 | 0.53 | (0.33–0.84) |
| Endolimax nana | 4 | 0.12 | (0.04–0.31) |
| Cystoisospora belli | 4 | 0.12 | (0.04–0.31) |
| Cryptosporidium spp. | 1 | 0.03 | (0.00–0.21) |
| Biparasitism | 64 | 1.88 | (01.47–02.39) |
| G.intestinalis–E. coli | 2 | 0.06 | (0.01–0.23) |
| B. hominis–E. nana | 1 | 0.03 | (0.00–0.21) |
| C. belli–B. hominis | 1 | 0.03 | (0.00–0.21) |
| E.coli–B.hominis | 26 | 0.76 | (0.52–01.12) |
| E.histolytica/dispar–B.hominis | 7 | 0.21 | (0.10–0.43) |
| E.histolytica/dispar–E. coli | 16 | 0.47 | (0.29–0.77) |
| E.histolytica/dispar–T.intestinalis | 1 | 0.03 | (0.00–0.21) |
| G. intestinalis–B. hominis | 1 | 0.03 | (0.00–0.21) |
| G. intestinalis–E. coli | 7 | 0.21 | (0.10–0.43) |
| T. intestinalis–E. coli | 1 | 0.03 | (0.00–0.21) |
| T. intestinalis–B. hominis | 1 | 0.03 | (0.00–0.21) |
| Polyparasitism | 2 | 0.06 | (0.01–0.23) |
| E. histolytica/dispar–B. hominis–Chilomastix Mesnili | 1 | 0.03 | (0.00–0.21) |
| E.histolytica/dispar–B. hominis–E. coli | 1 | 0.03 | (0.00–0.21) |
| Frequency %) | OR * (95% CI) | p Value | |
|---|---|---|---|
| Years | |||
| 2011 | 16 (3.92) | 1 | |
| 2012 | 70 (16.02) | 4.75 (02.70–08.34) | 0.000 |
| 2013 | 35 (10.17) | 2.89 (01.57–05.34) | 0.001 |
| 2014 | 58 (18.53) | 6.51 (03.64–11.65) | 0.000 |
| 2015 | 62 (21.23) | 6.38 (03.59–11.35) | 0.000 |
| 2016 | 107 (25.72) | 8.19 (04.72–14.24) | 0.000 |
| 2017 | 117 (28.26) | 8.88 (05.13–15.37) | 0.000 |
| 2018 | 85 (24.78) | 7.76 (04.42–13.64) | 0.000 |
| 2019 | 69 (27.38) | 8.84 (04.97–15.72) | 0.000 |
| 2020 | 26 (13.83) | 3.75 (01.95–07.21) | 0.000 |
| Age Group | |||
| <15 Years | 75 (24.83) | 1 | |
| 15–30 Years | 201 (17.65) | 0.98 (00.70–01.33) | 0.841 |
| 31–60 Years | 302 (19.33) | 1.03 (00.76–01.40) | 0.850 |
| >60 Years | 67 (16.58) | 0.84 (00.57–01.23) | 0.378 |
| Gender | |||
| Male | 311 (17.93) | 1 | |
| Female | 334 (19.98) | 1.11 (00.93–01.33) | 0.233 |
| Service | |||
| Hospitalized | 113 (12.61) | 1 | |
| Non-Hospitalized | 532 (21.19) | 1.68 (01.33–02.13) | 0.000 |
| Season | |||
| Dry | 517 (18.37) | 1 | |
| Rainy | 128 (21.59) | 1.16 (00.92–01.47) | 0.207 |
| Species | Age Group (Years) | Gender | Service | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| <15 Years | 13–30 Years | 31–60 Years | >60 Years | p Value | Male | Female | p Value | Hospitalized | Non-Hospitalized | p Value | |
| (N = 302) | (N = 1139) | (N = 1562) | (N = 404) | (N = 1735) | (N = 1672) | (N = 896) | (N = 2511) | ||||
| Giardiaintestinalis | 18 (6.0%) | 12 (1.1%) | 21 (1.3%) | 4 (1.0%) | 0.000 | 27 (1.6%) | 28 (1.7%) | 0.784 | 14 (1.6%) | 41 (1.6) | 0.886 |
| Entamoeba coli | 29 (9.6%) | 87 (7.6%) | 140 (9.0%) | 31 (7.7%) | 0.505 | 139 (8.0%) | 148 (7.9%) | 0.377 | 47 (5.2%) | 240 (9.6%) | 0.000 |
| Blastocystis hominis | 32 (10.60%) | 79 (6.94%) | 100 (6.40%) | 22 (5.44%) | 0.038 | 116 (6.69%) | 117 (7.00%) | 0.719 | 28 (3.13%) | 205 (8.16%) | 0.000 |
| Endolimax nana | 0 | 1 (0.09%) | 3 (0.19%) | 1 (0.24%) | 0.750 | 3 (0.17%) | 2 (1.20%) | 0.685 | 2 (0.22%) | 3 (0.12%) | 0.486 |
| Cryptosporidium spp. | 0 | 0 | 1 (0.06%) | 0 | 0.757 | 0 | 1 (0.06%) | 0.308 | 1 (0.11%) | 0 | 0.094 |
| Cystoisospora belli | 0 | 1 (0.09%) | 4 (0.26%) | 0 | 0.461 | 1 (0.06%) | 4 (0.24%) | 0.461 | 2 (0.22%) | 3 (0.12%) | 0.486 |
| Entamoeba histolytica:dispar | 8 (2.65%) | 34 (2.99%) | 50 (3.20%) | 13 (3.22%) | 0.955 | 52 (3.00%) | 53 (3017%) | 0.771 | 22 (2.46%) | 83 (3.31%) | 0.206 |
| Chilomastix mesnili | 1 (0.33%) | 0 | 0 | 0 | 0.016 | 0 | 1 (0.06%) | 0.308 | 0 | 1 (0.04%) | 0.550 |
| Trichomonas intestinalis | 2 (0.66%) | 4 (0.35%) | 12 (0.77%) | 3 (0.74%) | 0.570 | 9 (0.52%) | 12 (0.72%) | 0.458 | 8 (0.89%) | 13 (0.52%) | 0.218 |
| Species | Season | Years | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dry | Rainy | p Value | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | p Value | |
| (N = 2814) | (N = 593) | (N = 408) | (N = 437) | (N = 344) | (N = 313) | (N = 292) | (N = 416) | (N = 414) | (N = 343) | (N = 252) | (N = 188) | |||
| Giardia intestinalis | 49 (1.7%) | 6 (1.0%) | 0.200 | 1 (0.3%) | 7 (1.6%) | 2 (0.6%) | 4 (1.3%) | 3 (1.0%) | 13 (3.1%) | 7 (1.7%) | 10 (2.9%) | 6 (2.4%) | 2 (1.1%) | 0.026 |
| Entamoeba coli | 239 (8.5%) | 48 (8.1%) | 0.751 | 12 (2.9%) | 41 (9.4%) | 25 (7.3%) | 42 (13.4%) | 29 (9.9%) | 31 (7.5%) | 41 (9.9%) | 34 (9.9%) | 25 (9.9%) | 7 (3.7%) | 0.000 |
| Blastocystis hominis | 176 (6.25%) | 57 (9.61%) | 0.003 | 0 | 0 | 0 | 2 (0.64%) | 16 (5.48%) | 60 (14.42%) | 67 (16.18%) | 39 (11.37%) | 35 (13.89%) | 14 (7.45%) | 0.000 |
| Endolimax nana | 5 (0.18%) | 0 | 0.304 | 0 | 0 | 0 | 1 (0.32%) | 1 (0.34%) | 0 | 1 (0.24%) | 2 (0.58%) | 0 | 0 | 0.427 |
| Cryptosporidium spp. | 0 | 1 (0.17%) | 0.029 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.24%) | 0 | 0 | 0 | 0.613 |
| Cystoisospora belli | 3 (0.11%) | 2 (0.34%) | 0.182 | 0 | 1 (0.23%) | 0 | 1 (0.32%) | 0 | 0 | 1 (0.24%) | 0 | 0 | 2 (1.06%) | 0.094 |
| Entamoeba histolytica/dispar | 85 (3.02%) | 20 (3.37%) | 0.652 | 1 (0.25%) | 22 (5.03%) | 6 (1.74%) | 9 (2.88%) | 13 (4.45%) | 12 (2.88%) | 18 (4.35%) | 6 (1.75%) | 12 (4.76%) | 6 (3.19%) | 0.001 |
| Chilomastix Mesnili | 1 (0.03%) | 0 | 0.646 | 0 | 0 | 0 | 0 | 0 | 1 (0.24%) | 0 | 0 | 0 | 0 | 0.617 |
| Trichomonas intestinalis | 14 (0.50%) | 7 (1.18%) | 0.053 | 2 (0.49%) | 1 (0.23%) | 3 (0.87%) | 3 (0.96%) | 3 (1.03%) | 3 (0.72%) | 4 (0.97%) | 1 (0.29%) | 1 (0.40%) | 0 | 0.759 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndiaye, M.; Diongue, K.; Seck, M.C.; Diallo, M.A.; Kouevidjin, E.; Badiane, A.S.; Ndiaye, D. Retrospective Assessment of The Intestinal Protozoan Distribution in Patients Admitted to The Hospital Aristide Le Dantec in Dakar, Senegal, from 2011 to 2020. Parasitologia 2023, 3, 1-12. https://doi.org/10.3390/parasitologia3010001
Ndiaye M, Diongue K, Seck MC, Diallo MA, Kouevidjin E, Badiane AS, Ndiaye D. Retrospective Assessment of The Intestinal Protozoan Distribution in Patients Admitted to The Hospital Aristide Le Dantec in Dakar, Senegal, from 2011 to 2020. Parasitologia. 2023; 3(1):1-12. https://doi.org/10.3390/parasitologia3010001
Chicago/Turabian StyleNdiaye, Mouhamadou, Khadim Diongue, Mame Cheikh Seck, Mamadou Alpha Diallo, Ekoué Kouevidjin, Aida Sadikh Badiane, and Daouda Ndiaye. 2023. "Retrospective Assessment of The Intestinal Protozoan Distribution in Patients Admitted to The Hospital Aristide Le Dantec in Dakar, Senegal, from 2011 to 2020" Parasitologia 3, no. 1: 1-12. https://doi.org/10.3390/parasitologia3010001