4. Discussion
The study of Winburn and Stock [
33] used transition analysis to generate ages at which 90% and 95% of their sample transitioned to exhibiting OA in the TMJ and all appendicular joints. The current study generated similar ages at transition using a more diverse skeletal sample. For the BIPOC subsample, the pooled-sex ages at which 95% of this sample transitioned to having OA in the shoulder, elbow, wrist, hand, hip, knee, and foot were not significantly different from those reported in Winburn and Stock [
33] (See
Table 7). For the white subsample, the pooled-sex ages at which 95% of this sample transitioned to having OA in the shoulder, elbow, wrist, hand, hip, knee, and foot were not significantly different from those reported in Winburn and Stock [
33] (See
Table 8). Therefore, both subsamples from the current study confirm the general pattern of age-correlated OA development reported in the earlier study.
The BIPOC subsample did yield significantly different results in the TMJ and ankle for the 95% transition comparison. The original study also identified issues with the ability of the TMJ and the ankle to correctly predict age—even recommending that the TMJ not be used to estimate age in male individuals, that the ankle not be used for females, and that neither joint be used when combined-sex models are employed [
33]. As such, it is not surprising that these two inconsistent joints, in which correlations between OA and age are more tenuous, produced values that were significantly different between the two studies.
This study also confirmed other patterns discovered by the original study authors. For example, the tendency for the proximally placed appendicular joints to develop OA before the more distally placed joints was generally upheld in the white subsample—aside from a few outliers, such as the male elbow (see
Table 4 and
Table 5). Although certain joints showed earlier transition ages than in Winburn and Stock [
33], the pattern of which joints were the first and last to transition—regardless of age—was very similar to that reported by Winburn and Stock. For the white subsample, what this confirms is that in contrast to the long-held belief that OA is too multifactorial to inform age, OA development in appendicular joints is even more strictly controlled by age than previously thought. Furthermore, if, as once believed, OA were a result of regular “wear and tear” to the joint surfaces, it may be expected that those joint surfaces that undergo the highest biomechanical stresses, such as the knee, would be the first in the body to develop OA. However, this is not the case. Instead, in samples of white Americans, appendicular OA follows a consistent pattern, where the hip is one of the first joints to develop OA and the hand is one of the last. Using OA as an indicator of activity patterns, a traditional approach in the discipline of bioarchaeology, e.g., refs. [
52,
53,
54,
55,
56,
57,
58], is, therefore, unwise for forensic populations. For purposes of forensic age estimation, however, this is excellent news. As posited in the original study, the pattern of ages at which OA develops throughout the body can help to refine other aging methods in forensic anthropology. Existing age-estimation methods for middle- to older-aged adults are limited by their broad ranges, but the additional information provided by joint OA can narrow these ranges. The hips are informative for younger individuals, whereas the hands, feet, and female TMJ can provide information to refine the age ranges for older individuals.
The BIPOC subsample followed the “proximal to distal” pattern of OA development more loosely. The hip was often the first joint to transition, but the elbow and knee sometimes transitioned before the shoulder, and the wrist and ankles sometimes transitioned after the hands and feet (see
Table 2). In addition, the TMJ, which was one of the very last joints to transition in Winburn and Stock [
33], was commonly the second or third joint to transition in the BIPOC subsample. The ankle also transitioned much earlier. However, given the tenuous age-OA correlation in the male TMJ and female ankle, the unexpectedly early transition of these joints in this study is not overly concerning—particularly since the original study authors recommended against using these joints to estimate age.
The earlier transition age of the elbow (significant in the BIPOC male and pooled-sex samples) and the later transition age of the wrist (significantly different in the BIPOC male sample) are noteworthy, however. There are several reasons why OA might be observed earlier in the elbow of BIPOC individuals. It is possible that the first author’s difficulty in recognizing OA in the elbow contributed to these differences. Yet, the elbow joint showed good agreement between the researchers in the interobserver error sample (see
Table 10). An alternate explanation could be that the elbow experienced additional abnormal stressors from occupation-related movements. Since the UTK Donated Skeletal Collection asks donors about their profession as part of their demographic data, this information is often available. Indeed, many of the individuals in the BIPOC subsample for this study reported working as a “laborer”, and other individuals reported jobs such as “knife maker”, “textile worker”, “baker”, or “welder”. In each of these careers, it is possible that these individuals participated in activities causing them to experience repeated abnormal loading of the elbow joint during either flexion and extension and/or pronation and supination. Injurious physical labor could initiate the breakdown of homeostasis in the cartilage of the joint, thereby setting the stage for the osteoarthritic effects of aging. It is important to remember that age, though a primary risk factor for OA, is not the sole risk factor. Age fluidly interacts with lived experiences and genetic predispositions to create a unique combination of OA risk factors for any given individual, but these additional factors do not preclude the ability of age to predict OA development.
Furthermore, it must be noted that the white subsample also included numerous individuals with listed occupations of “welder” and “laborer” (alongside a variety of frequently listed occupations such as “electrician”, “homemaker”, and “disabled”). Additionally, several individuals in both subsamples reported either having no job or “white-collar” jobs without intense physical labor. Thus, it is not possible to rely on occupation as an explanation for the earlier development of OA in the elbow of BIPOC males and pooled-sex individuals—especially given the limitations of a 60-person subsample. Beyond simply looking at career, however, it is certainly possible that the embodiment of a diverse set of life experiences could be responsible for an earlier age at transition of the elbow if the elbow happens to be a joint surface that is more susceptible to the influence of lived experiences. Although it seems improbable that stress from living as BIPOC in a racialized society would manifest only in a single joint, it cannot be entirely ruled out without a deeper understanding of the way that stress interacts specifically with the elbow joint at a cellular level, for example. The internalization of external stressors can interact with epigenetics to produce different biological results in various individuals, so it would not be surprising if embodiment-related OA presented itself via different channels. Indeed, the activation of the hypothalamic-pituitary-adrenal (HPA) axis from acute or chronic stress can trigger biological disruptions from stress hormone release, which facilitate disease processes, but social stressors can also trigger changes in behavior that can have biological consequences (e.g., smoking, drinking, and exercise) [
8]. On a cellular level, social adversity can contribute to changes in cell structure and sensitivity to stimuli [
8], which larger-scale factors such as differential access to health care (and health insurance; [
9]) can further exacerbate or mitigate. The biological pathways through which social stressors are linked to biological consequences are many, and future research is needed to investigate the specific relationship between OA (specifically in the elbow joint) and social adversity.
In contrast to the elbow, the wrist demonstrated an older age at transition in the BIPOC subsample than in Winburn and Stock [
33] (see
Table 7). A possible explanation as to why the wrist was delayed in transitioning from “OA absent” to “present” could be related to the earlier age at transition of the elbow. To elaborate, if more strain is diverted to the elbow joint rather than the wrist, then perhaps the wrist experienced more protection from injurious loading in these individuals. Alternatively, the wrist may naturally be more resistant to homeostatic disruption, which would explain why it is one of the later joints to transition to “OA present” in all three groups (this study’s BIPOC and white subsamples, as well as the original white American sample studied by Winburn and Stock).
In this study’s white subsample (see
Table 3), the 90% ages of transition were younger than those reported in Winburn and Stock [
33] for the female TMJ, female hand, and male ankle, and the ages at which 95% of the samples transitioned were younger for the female TMJ, female elbow, female knee, female foot, and male ankle. There were no significant differences in the pooled-sex category. Like the BIPOC subsample, it is possible that the injurious loading of these joints contributed to earlier OA development. A few of these significant differences can also potentially be explained by interobserver error discrepancies—particularly in the female hand. The hand showed one of the lowest interobserver agreement rates of all the joints, so if the two studies did not agree on when OA in the hand was present or absent, then this could explain the significantly different ages at transition. It is also noteworthy that for the white subsample (the only cohort as of yet investigated for interobserver error), in each of the joint surfaces that showed disagreement, a younger age at transition was generated in the current study than in the original. This indicates that in the current study, OA was marked more often as “present” in younger individuals in these joints, whereas it was marked as “absent” by Winburn and Stock [
33]. Greater standardization, or stricter adherence to the descriptions of OA in the various joints provided in Winburn and Stock’s [
33] and
Table 3, may be necessary to ensure replicable results in future applications.
In addition to being compared with the ages at transition generated from the Winburn and Stock [
33] data, the BIPOC and iteratively resampled white subsamples were also compared to each other (see
Table 6). The only significant differences were in the ages at which 90% and 95% of BIPOC males transitioned to exhibiting wrist OA and the ages at which 95% of BIPOC males transitioned to exhibiting knee OA. In all three cases, the BIPOC males transitioned at a later age than the iteratively resampled white male subsample. These significant differences in the wrist and knee are notable. As in the above comparisons, the older age at transition of the wrist could indicate its resistance to homeostatic disruption. The knee is interesting, as it is most definitely not an area of the body prone to natural OA resistance. On the contrary, the knee is one of the joints in which OA is most common [
59] and one that commonly undergoes total joint arthroplasty [
60]. Yet, the age at transition is older in the knee of the BIPOC subsample. Since the knee is one of the weight-bearing joints, it is possible that obesity is a risk factor influencing the differing ages at transition, where excess weight is responsible for earlier OA development in the white subsample. Despite significant differences in the joints discussed, however, the BIPOC and white subsamples overall demonstrated clearly similar results. Particularly when the sexes were pooled, significant differences were rare between BIPOC and white individuals from the original study (see
Table 7) and nonexistent between BIPOC and white individuals in the current sample (see
Table 6).
While the TMJ and ankle were consistently poor indicators of age, the shoulder and the hip performed consistently well. In all the samples tested, there were no significant differences involving these two joints. One explanation for this pattern could be the fact that both the hip and the shoulder are ball-and-socket joints that are relatively well protected by soft tissue. This could mean that the presence of OA and, therefore, the ages at transition generated by these joints, result more directly from age-related homeostatic disruptions and are less influenced by outside factors than other joints. Not only are these strong indicators of age, but the hip also had particularly low rates of interobserver error and intraobserver error (between 0 and 5%; see
Table 10), indicating that hip OA can be reliably assessed.
That the shoulder and the hip are well-protected, ball-and-socket joints and yet are some of the first to demonstrate OA is a seeming contradiction. If the well-developed joint capsules and surrounding musculature do provide a buffer to external, injurious forces, why would these joints then display OA at an earlier age compared to more distal ones? Perhaps the driving factor is not perturbation by confounding factors, nor an extreme amount of use, but rather the type of use at the joint. The shoulder and hip are capable of abduction and adduction, flexion and extension, or rotational movement [
61]. The wide range of movement permitted at these joints may work in combination with the built-in protection of the muscle and ligaments encasing the joints to produce an age at transition that is truly reflective of age at death.
4.1. Validating Winburn and Stock [33]
In addition to confirming several patterns outlined in Winburn and Stock [
33], this study also validated its application to BIPOC. For both the white and the BIPOC subsamples, the method was able to successfully predict the age at death of a large proportion of all subsamples using both 90% and 95% ages of transition (>88%). Furthermore, accuracies were comparable between the BIPOC and white individuals—ranging from 88 to 92% and 88 to 93%, respectively. These numbers indicate that there are no discrepancies in OA development by social race that would preclude the use of estimating age at death with appendicular OA presence or absence.
It was predicted that the lived experiences and historic inequities faced by BIPOC, which have been demonstrated to accelerate aging and cause other health disparities among the living, would impact the ability of OA to correctly predict age in these individuals or to necessitate a population-specific set of standards for using OA for age estimation. This does not seem to be the case in the current sample. Not only were ages estimated with equivalent accuracy in BIPOC and white individuals, but also there were few significant differences between the BIPOC and iteratively resampled white subsamples, with younger ages at transition for BIPOC only observed in one joint. Interestingly, of the three samples compared—the BIPOC subsample, white subsample, and Winburn and Stock’s [
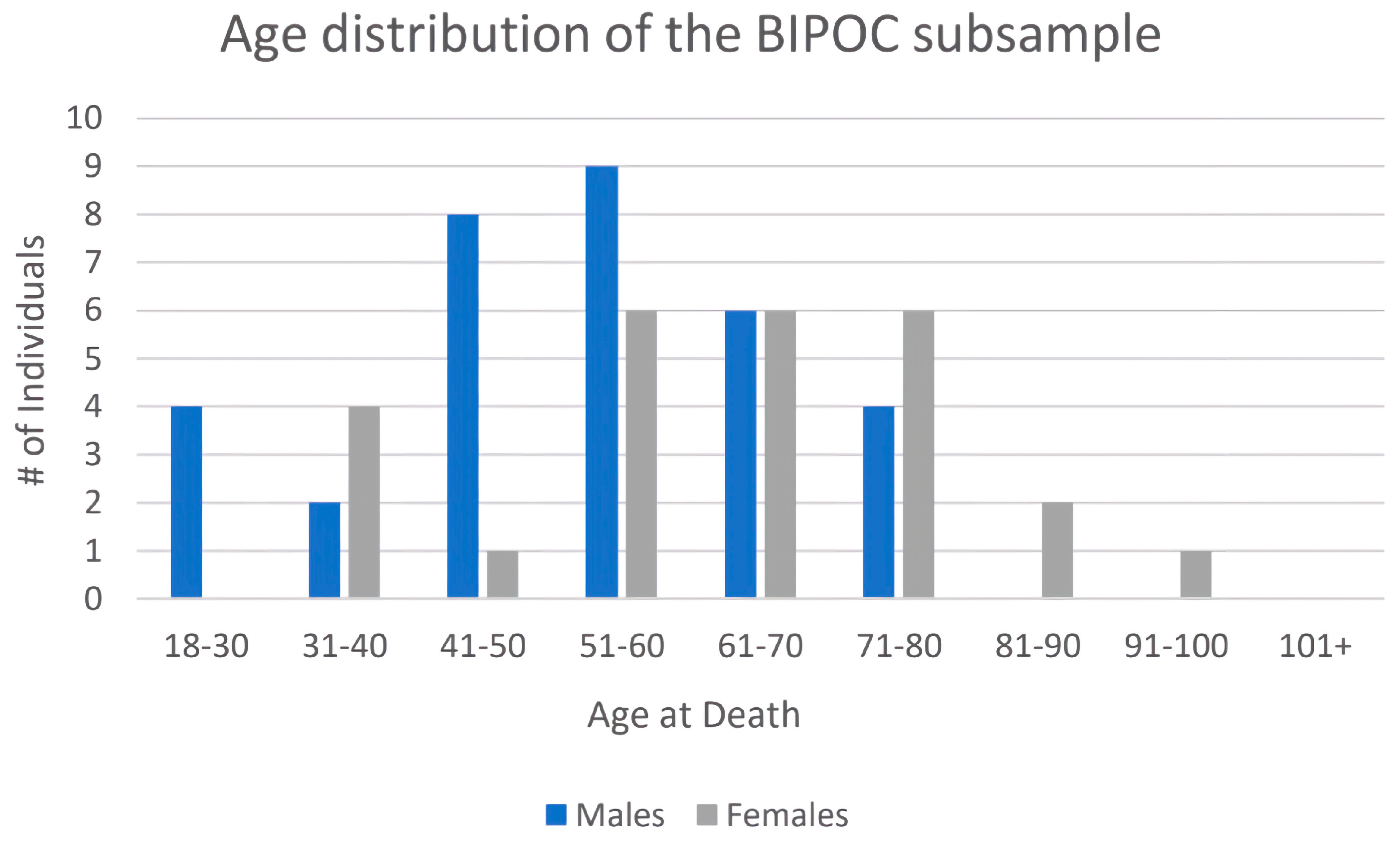
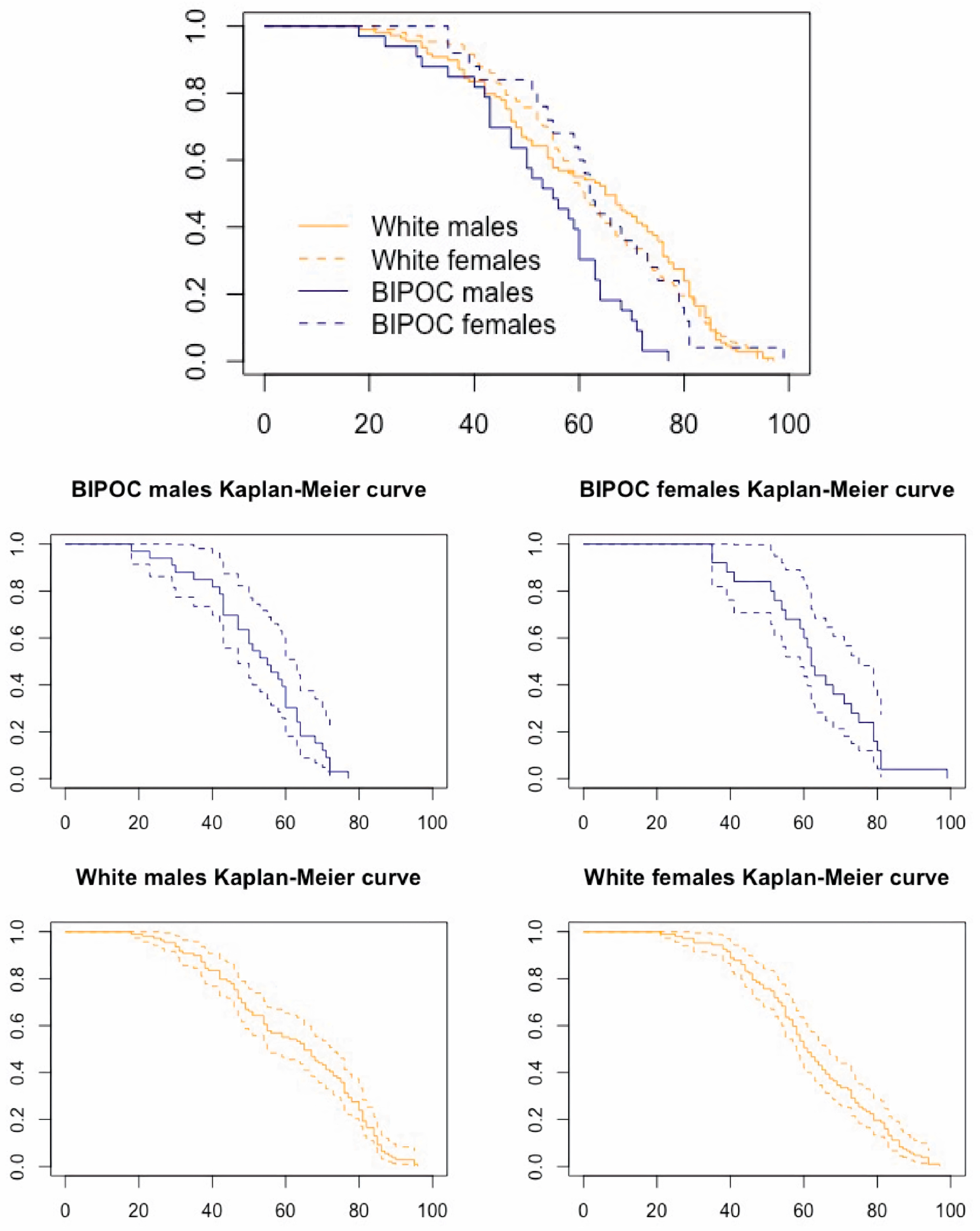
33] white sample—it was the two white subsamples that showed the most significant differences. The idea that embodied experiences of social inequity are driving the slight differences noted in the BIPOC subsample is inconsistent with the observed pattern, in which the elbow is the only area in the body where advanced aging is observed, and only when the BIPOC subsample is compared with the original Winburn and Stock sample (not when this study’s subsamples are compared with each other). Rather, if embodied inequity were the driving factor, many—or all—of the joints would be expected to produce lower ages at transition in more of a systemic pattern, consistently throughout the body. Instead, the results of this study indicate that the ability of OA to predict age at death among U.S. residents of eastern Tennessee is not significantly impacted by differing lived experiences in individuals of differing self-reported social races. This is not to say that OA development is not affected by experiences of living as BIPOC in a racialized society, but rather that the variations that do occur are localized rather than systemic and, therefore, do not prevent OA from accurately assessing age at death. Additionally, the average age at death is an important factor to consider when comparing multiple populations. The mortality curve (age distribution) of BIPOC males was the only group that indicated a lower average age at death in this subsample than the white subsample, and this younger age at death has the potential to artificially drive the ages at transition down. Even if the mortality curve did drive the ages at transition down to an earlier age, they were still not systematically younger, which further reinforces the conclusion that lived experiences of social race did not impact OA development in this sample, or suggests that any existing experiences of inequity were tempered by resilience [
62].
An alternate explanation of the unexpectedly similar results between the BIPOC and white subsamples explored the topic of a shared sociocultural environment. In the Southern/Central U.S., communities of color and white populations alike are exposed to a combination of stressors, including infection (e.g., whipworm), environmental toxins, and the effects of extreme poverty, with a resulting higher mortality rate than the rest of the nation [
63]. One of the assumptions in this study was that the white subsample would be afforded a degree of biological buffering from living in a racialized society where “whiteness” is privileged. If this was not the case for this study’s white subsample because the donors were from the Southern/Central U.S., it stands to reason that similar exposure to inequities by both the white and BIPOC subsamples may provide an explanation for the similar age-at-transition results. However, although the white subsample in this study may very well have experienced atypical levels of hardship, the concept of intersectionality [
64] argues that the BIPOC subsample would face the same universal stressors from the shared environment
in addition to the potential strain associated with structural violence and systemic racism [
65,
66]. Thus, similar experiences of inequity, such as poverty, are not a satisfactory explanation for similarities in the age-at-transition between BIPOC and white subsamples, unless differing mechanisms that are protective of joint health were at work during the lives of the BIPOC subsample (e.g., greater resilience [
67] or more non-injurious physical activity). Otherwise, it seems that any intersectional inequity experienced by this sample’s BIPOC donors did not translate to earlier or more advanced joint aging in the form of OA.
4.2. Inter- and Intraobserver Error
Though the overall rates of inter- and intraobserver agreement range from good (11–20% error) to excellent (0–10% error), for certain joints and individuals, they were poor (21%+). This can be attributed to several different factors. For the intraobserver error, changes in opinion from the beginning to the end of the data collection can be attributed to increasing familiarity with the method. As time goes on and a researcher sees more variation, it would make sense that their comfort with classifying OA into one category or the other would increase over time. This is likely what happened with the shoulder joint. The left shoulder had an error rate of 15%, while the right had a rate of 25%. An initial difficulty in recognizing shoulder OA, which was later clarified as more variation was observed, is definitely possible.
Aside from the right shoulder, the right wrist demonstrated the highest rate of intraobserver error, at 21.05% (see
Table 10). This value is difficult to explain, as the left wrist has a much lower error rate, at 10.53% (see
Table 10). Values that were initially marked as absent were more often marked as present during the second round of observations, which could reflect a greater familiarity with identifying true OA absence toward the end of the study. The high intraobserver error rate of the right wrist stands as a cautionary tale, which reminds practitioners that OA can present differently on various joint surfaces. Familiarity with the detailed descriptions of OA in each joint surface presented in Winburn and Stock (Table 3 of [
33]) is essential but, in terms of application, there still appear to be certain joint surfaces (such as the wrist) that researchers become more familiar with over time. The range of variation observed throughout the entire sample helped to solidify examples of true OA absence, which is likely why the values were different at the beginning and the end of the study.
The individuals who had the highest overall percentage of interobserver agreement were older individuals, whereas the individual with the lowest interobserver error score (35.48%; see
Table 11) was a younger individual. This could indicate high interobserver agreement about OA when present, but more difficulty identifying and agreeing on instances where it is entirely absent. The shoulder could be one of these cases, as the interobserver error was fairly high for this joint surface—10.87% for the left and 13.04% for the right (see
Table 10). This is also consistent with the age-at-transition findings for this study, as OA was marked more often as “present” in younger individuals in a number of joints, whereas it was marked as “absent” by Winburn and Stock [
33], creating younger ages-at-transition overall. A final line of evidence supporting this finding is when the OA-aging method was applied to the current sample to estimate age at death, roughly 75% of the individuals that were incorrectly aged were “young” individuals (under 40 years old). Therefore, it is likely that deciding on the “absence” of OA is an aspect of this methodology with considerable interobserver disagreement. For OA to be marked “OA absent”, every single surface of bone had to be present and intact enough for observation; otherwise, it would be marked as “NA”. If two researchers had differing opinions on when bone was too fragmentary, eroded, or otherwise damaged to evaluate it for OA, then this could also explain some discrepancies. Finally, the level of osteological experience could also have played a role in the discrepancies.
In addition to being poor indicators of age, the ankle and the TMJ both demonstrated poor interobserver agreement. The left and right TMJ had the highest interobserver error rate of any joint surface, at 19.57% (see
Table 10). The ankle was close behind, at 18.60% error for the left and 15.38% for the right (see
Table 10). Beyond the fact that these joints provide poor age estimates, their high error values reinforce that the ankle and TMJ are problematic joints for this method, further supporting recommendations for their use only as a last resort.
4.3. Methodological Recommendations
This study confirmed that OA is effective in estimating age of BIPOC and white individuals from eastern Tennessee and that the Winburn and Stock [
33] OA-aging method can essentially be applied without modification. However, one issue identified by the current study was the difficulty in applying the method to individuals with patterns of OA development that did not fit the ages at transition reported by Winburn and Stock (Table 9 of [
33]). To elaborate, the appendicular joints and the TMJ transition from “no OA” to “OA present” in a somewhat regular pattern. The hip should transition before the hand, according to this pattern—a finding first reported by Winburn and Stock [
33] and confirmed in the current study. Yet, when trying to predict age at death based on the OA of the individuals in the current study, some individuals showed a contradictory patterning of OA. For example, some individuals were coded “OA present” in the hand (a region typically slow to develop OA), but “OA absent” in the hip (a region where OA typically develops early). In these instances, the joints provide conflicting age estimates, with one providing a relatively young maximum age and the other providing a much older minimum age. Obviously, both cannot be correct, but it is the recommendation of the current study—following the approach of Winburn and Stock [
33]—that the
absence of OA should be preferenced. Emphasizing absence over presence is a more conservative methodology because, while it is possible (due to occupational injury, for example) for a joint to develop OA prior to the age at which 90% of the population has transitioned, it is less likely that OA will be absent after that age. In other words, it is possible that a 26-year-old has slight OA developing in their hands while still having no OA in the hip. Therefore, in instances where OA development does not follow the generalized pattern of development presented in Winburn and Stock (Table 9 of [
33]), the best practice is to rely on the absence of OA rather than the presence as the indicator of age.
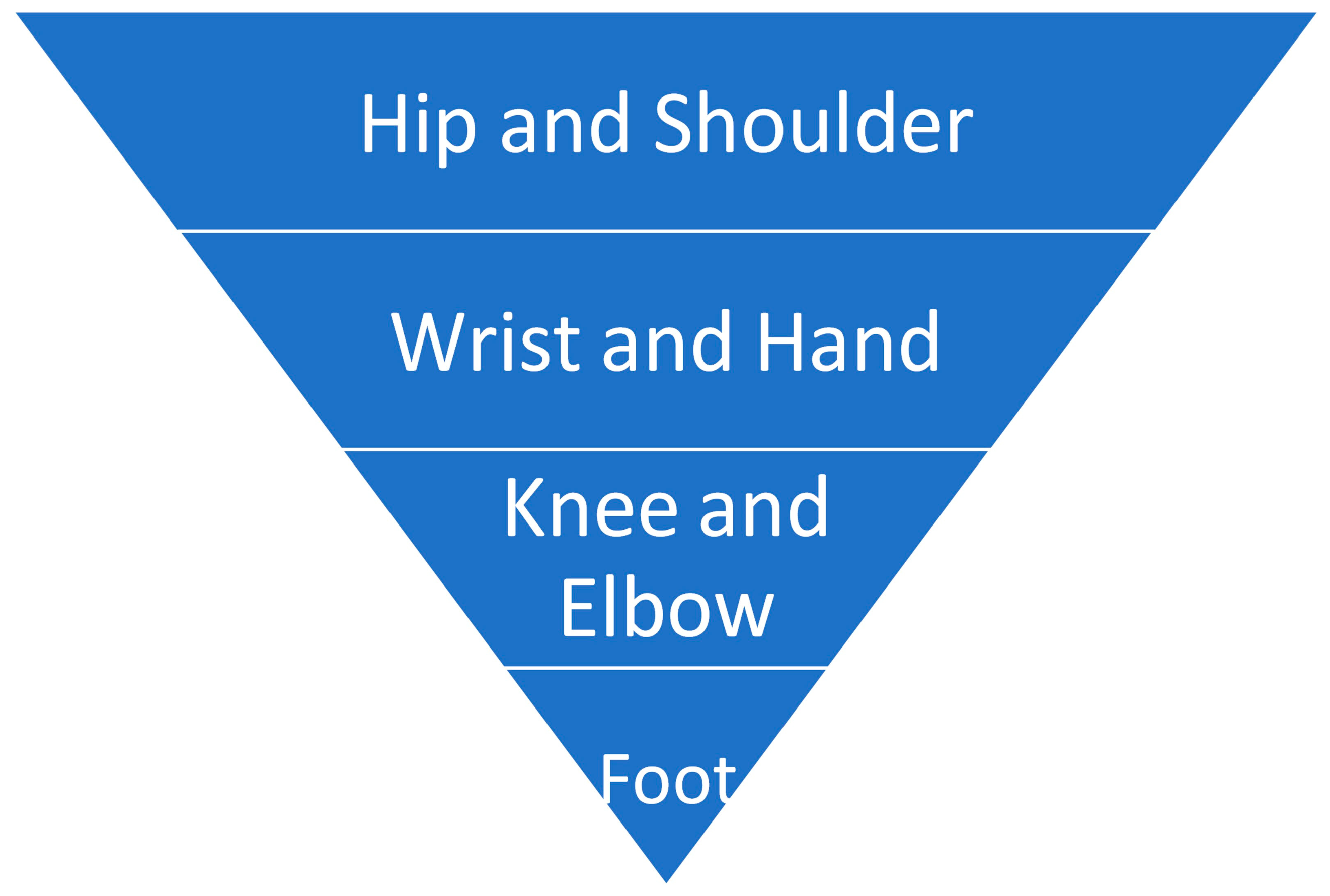
This study’s findings indicate a hierarchy of joints in terms of their age-estimation utility and the reliability of their assessment (
Figure 6). The TMJ and the ankle should not be used for age estimation. In contrast, the hip and the shoulder are strong age indicators that, if present in a case, should be given preference over the other joints in a case where OA patterning is unexpected. Methodologically, this is significant, as if even a single, complete femoral head is present in a case assemblage, this can refine an age estimate generated from other indicators (e.g., pubic symphysis) in a meaningful way. It is recommended that if all the joint surfaces in a skeleton are present, they are used to estimate age in the order in which they are presented in
Figure 6.
Furthermore, users of this method must thoroughly understand the traits indicative of OA in the various joints, as its appearance is not uniform. In the original paper, Winburn and Stock (Table 3 of [
33]) provide extensive descriptions detailing the appearance and characteristics of OA in the various joints. Familiarity with the contents of this table is essential to the effective application of this method. Along those lines, future research might standardize the percentage of the joint which needs to be present for the evaluation to proceed. If 80% of the joint is present and exhibits no OA but 20% of the margins are eroded, is it safe to say that the joint is free of OA, or does the entire joint surface need to be present? Is perfect preservation a realistic expectation, given the often fragmentary and damaged nature of bone in forensic cases? Each of these questions were outside the scope of the current study, but they deserve attention in future research.
Finally, while the method was accurate, this does not mean that it was precise. Rather, the estimates provided were always broad, often consisting merely of a lower or upper age terminus. For the individuals who have OA in every joint, for example, age estimates based on ages-at-transition for 90% of the original sample are 29.7+ years for males and 37.2+ years for females. While this is somewhat informative, other aging methods should be preferenced, or used in combination with OA, in a casework scenario where a decedent exhibits extensive OA. If a full skeleton is present, then this aging method alone is unlikely to produce a precise age interval. As the original authors noted, the method is most powerful in cases of few or fragmentary remains, where the application of traditional age-estimation methods is not possible.
4.4. Study Limitations
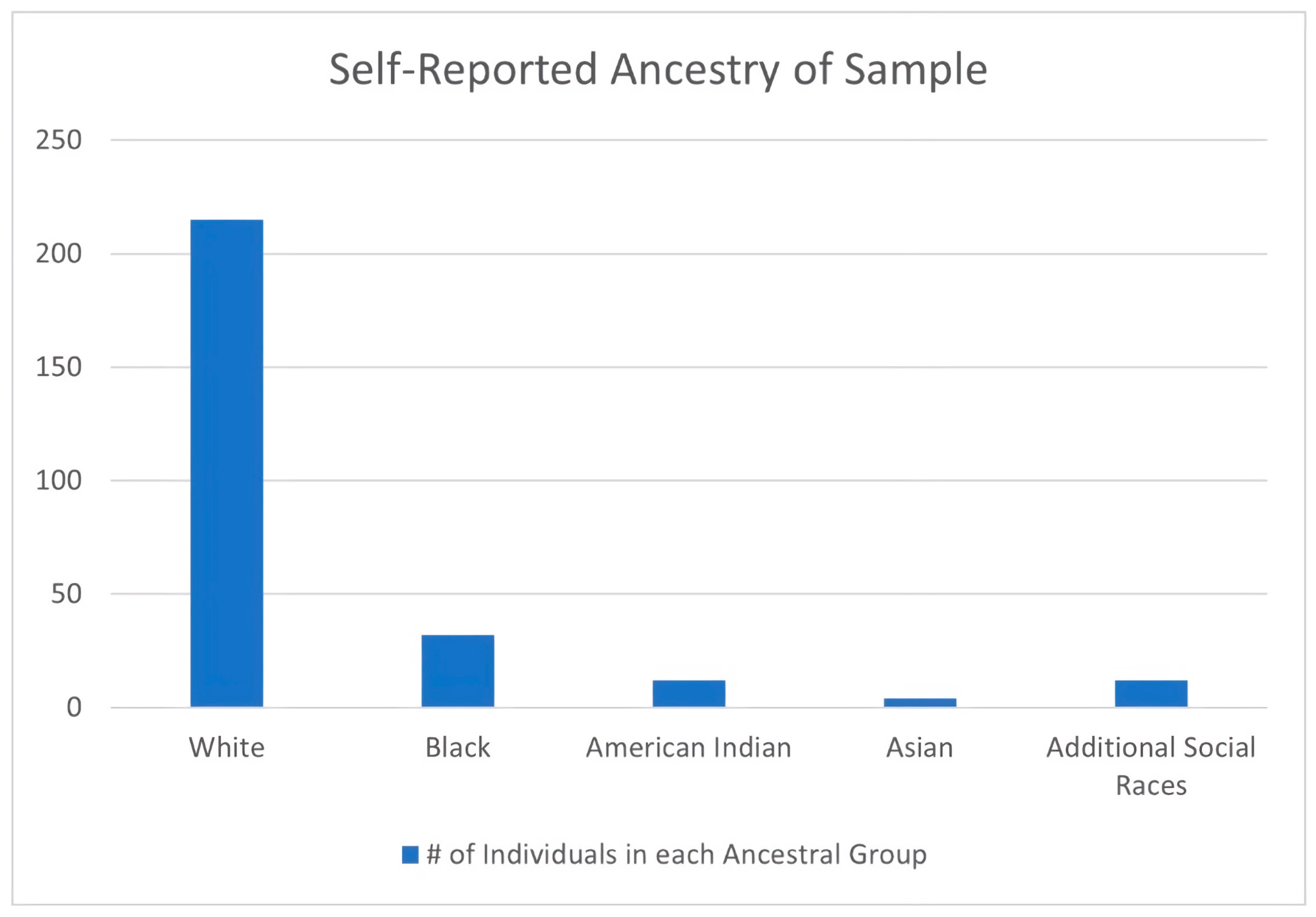
Although this study was the first to apply the OA aging method to donors of color, the small size of the BIPOC subsample (n = 60) was a limitation. Despite the ability of repeated iterative sampling (bootstrapping) to enable direct comparisons with this subsample, a larger sample size with greater variation would have been desirable and should be pursued in future research. Furthermore, in order to combat small sample sizes and to enable a statistical comparison, this study’s BIPOC subsample had to be treated as a singular category, despite being composed of individuals from numerous social races. It is unrealistic to assume that all social races have universal experiences with inequity or marginalization, and treating all communities of color as a single homogenous entity should be avoided. This small sample of BIPOC donors cannot be interpreted as representative of the diverse demographic makeup of the U.S., nor can it be assumed that their lived experiences were shared by other Americans of color. As such, it may be dangerous to extrapolate from this data and apply the OA-aging method to communities of color more broadly.
On the other hand, testing the method on large and diverse samples is currently precluded by the documented racial disparities in the demographics of modern U.S. donated skeletal collections [
3]. In the UTK Donated Collection, for example, over 90% of curated donors identified as white [
3,
40]. The underrepresentation of people of color in donated skeletal collections may reflect cultural preferences (e.g., a desire for intact interment as a means of final disposition) or a lack of familiarity with body donation processes [
68]. Reluctance on the part of potential donors of color may also be influenced by the long history of their non-consensual
anatomization sensu [
69] into the anatomical collections of the past [
70]. Combined with other abuses enacted by the U.S. biomedical and scientific communities (e.g., The U.S. Public Health Service Syphilis Study at Tuskegee), these collection practices established a longstanding relationship of distrust between scientists/medical providers and, in particular, black Americans [
71]. A combination of disinterest, lack of information, and distrust may thus interact with family wishes, religious ideals, and accessibility to result in the problematic dearth of donors of color in donated skeletal collections. Until these myriad issues begin to be addressed, the use of self-consented CT data from living individuals, or kin-consented imagery from deceased individuals e.g., [
72], may represent avenues for future testing of the Winburn and Stock [
33] aging method to large and diverse samples of individuals of color.
Regardless, the fact that the OA-based age estimation was confirmed to be effective in this small sample of BIPOC individuals is an improvement over the original method, which was only tested on a white sample—both limiting the method’s applicability and implicitly upholding the dangerous idea that there are inherent and meaningful differences between U.S. social races.
5. Conclusions
This study validated the OA-based age-estimation method of Winburn and Stock [
33] and showed that it predicts age with equivalent accuracy in both BIPOC and white individuals from eastern Tennessee. These findings reject the hypothesis that the experience of living in a racialized society would lead to skeletally discernible differences in rates of osteoarthritis-based aging between the study’s two subsamples while acknowledging high poverty and mortality rates potentially contributed to the particular experience of social race in this region [
11,
63]. As such, this method can be used as published on the general U.S. population—although with caution, until supported by multiple additional regional studies.
The generalized progression of proximal-to-distal OA development reported in Winburn and Stock [
33] was largely confirmed, with the elbow as an exception. The ages at transition for 90% and 95% of the population to convert from “OA absent” to “OA present” were also reproduced in the current study, despite certain joints that did demonstrate significant differences between the original and the current studies. The two problematic joints in the original OA study—the TMJ and the ankle—were similarly problematic in the current study, reinforcing the conclusion that they should not be used for age estimation.
There were also points of variation between the two studies. Where ages at transition generated by this study’s white and BIPOC subsamples were statistically different from those generated by Winburn and Stock [
33], they were generally younger in the current study. Along with other lines of evidence, such as the poor intraobserver agreement for younger individuals, this led to the conclusion that OA absence is less likely to be agreed upon than OA presence. This has significant implications for the application of the OA-aging method, as it is essential that researchers agree on what constitutes the absence, not just the presence, of OA.
In cases of fragmentary or incomplete forensic remains, Winburn and Stock [
33] is an age-estimation technique that can provide an accurate—albeit broad—age range if any appendicular joint is present. The method is easy to apply, requires no technology, equipment, or calculations, and does not require a population-specific approach. It can also be used in conjunction with other age-estimation methods to provide a minimum or maximum age to help narrow the overall range for an unknown decedent. If multiple joints are present, then they should be interpreted in tandem with one another but, in cases of conflicting conclusions, the hip and shoulder should be emphasized, and OA absence should be preferenced over OA presence.
Overall, this study confirmed that while OA is multifactorial, its strong age correlation renders it a suitable age indicator. It is hoped that future research will continue to illuminate the many ways in which OA can contribute to the estimation of age in skeletal individuals.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}