

Postoperative Recovery after TMJ Arthroscopy: Masticatory Improvement and Postoperative Diet

Abstract
:1. Introduction
2. Materials and Methods
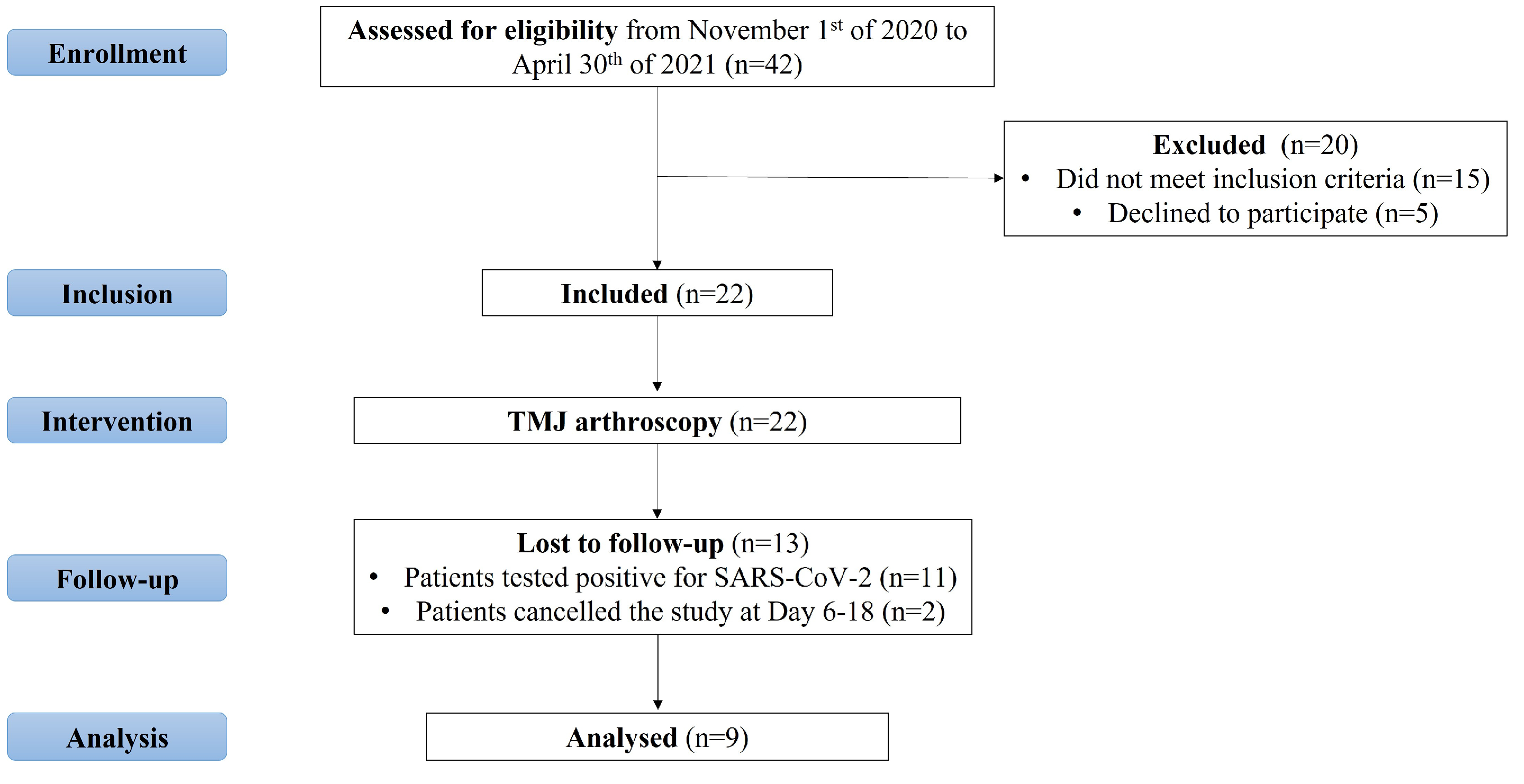
2.1. Study Design
2.2. Study Protocol and Data Collection
2.3. Treatment Protocol
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Discomfort with the Mastication of Different Food Textures | |
| Question 1 | How would you describe your discomfort during the mastication of one cooked potato? (on the left and right sides) |
| Question 2 | How would you describe your discomfort during the mastication of one slice of load bread? (on the left and right sides) |
| Question 3 | How would you describe your discomfort during the mastication of one half of a brioche bread? (on the left and right sides) |
| Question 4 | How would you describe your discomfort during the mastication of one Maria biscuit? (on the left and right sides) |
| Question 5 | How would you describe your discomfort during the mastication of one uncooked and unpeeled almond? (on the left and right sides) |
| TMJ pain during essential functions | |
| Question 6 | How would you describe your TMJ pain during deep breaths? (on the left and right sides) |
| Question 7 | How would you describe your TMJ pain during deglutition? (on the left and right sides) |
| Question 8 | How would you describe your TMJ pain during the speech? (on the left and right sides) |
| Question 9 | How would you describe your TMJ pain during mastication? (on the left and right sides) |
| Discomfort when resuming normal lifestyle | |
| Question 10 | How would you describe your discomfort when restarting professional activity? (on the left and right sides) |
| Question 11 | How would you describe your discomfort when restarting moderate to high-intensity physical activities? (on the left and right sides) |
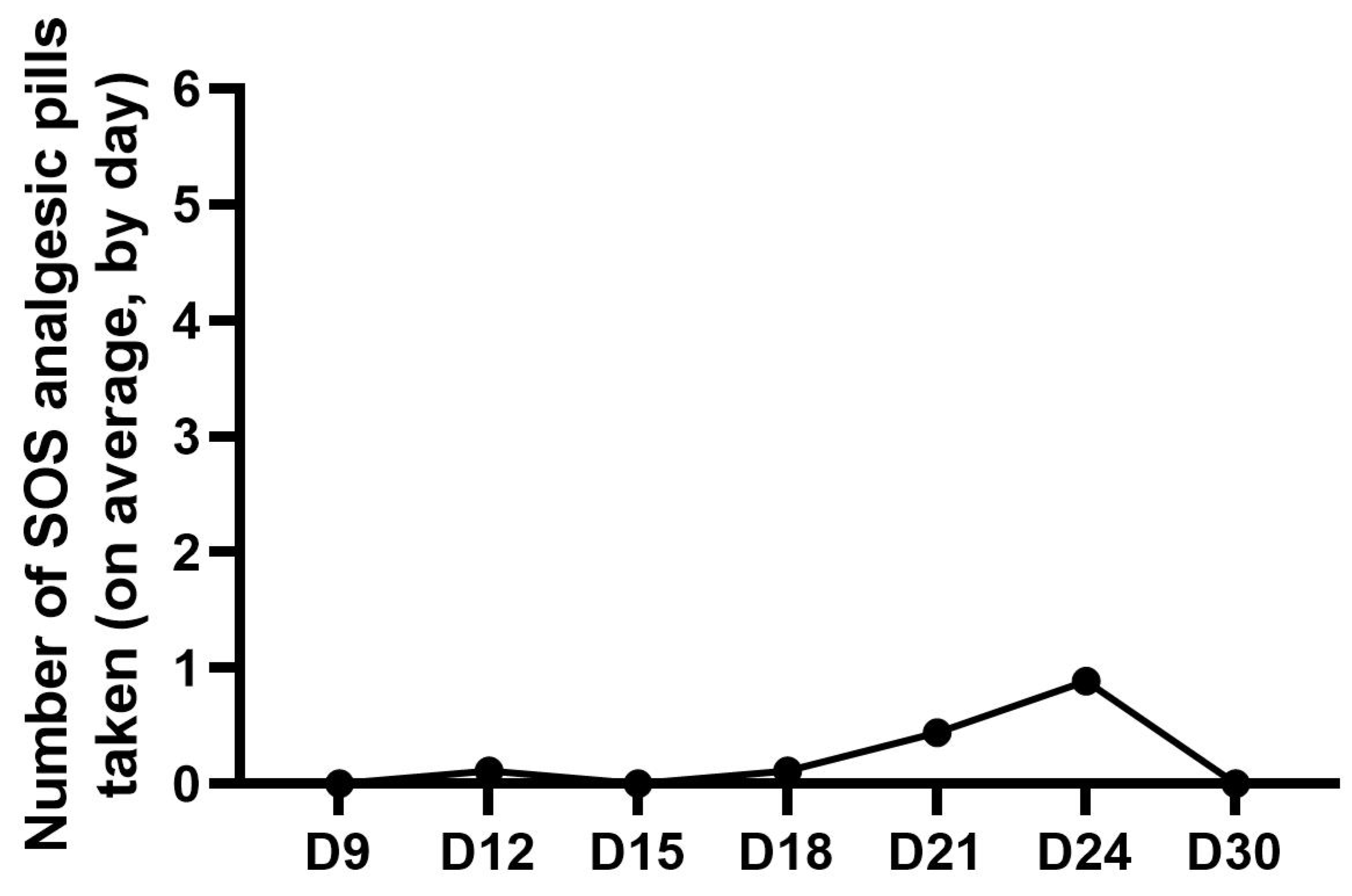
| Number of SOS analgesics needed | |
| Question 12 | Please indicate the average number of SOS analgesic pills taken each day (over the previous 3 days). |
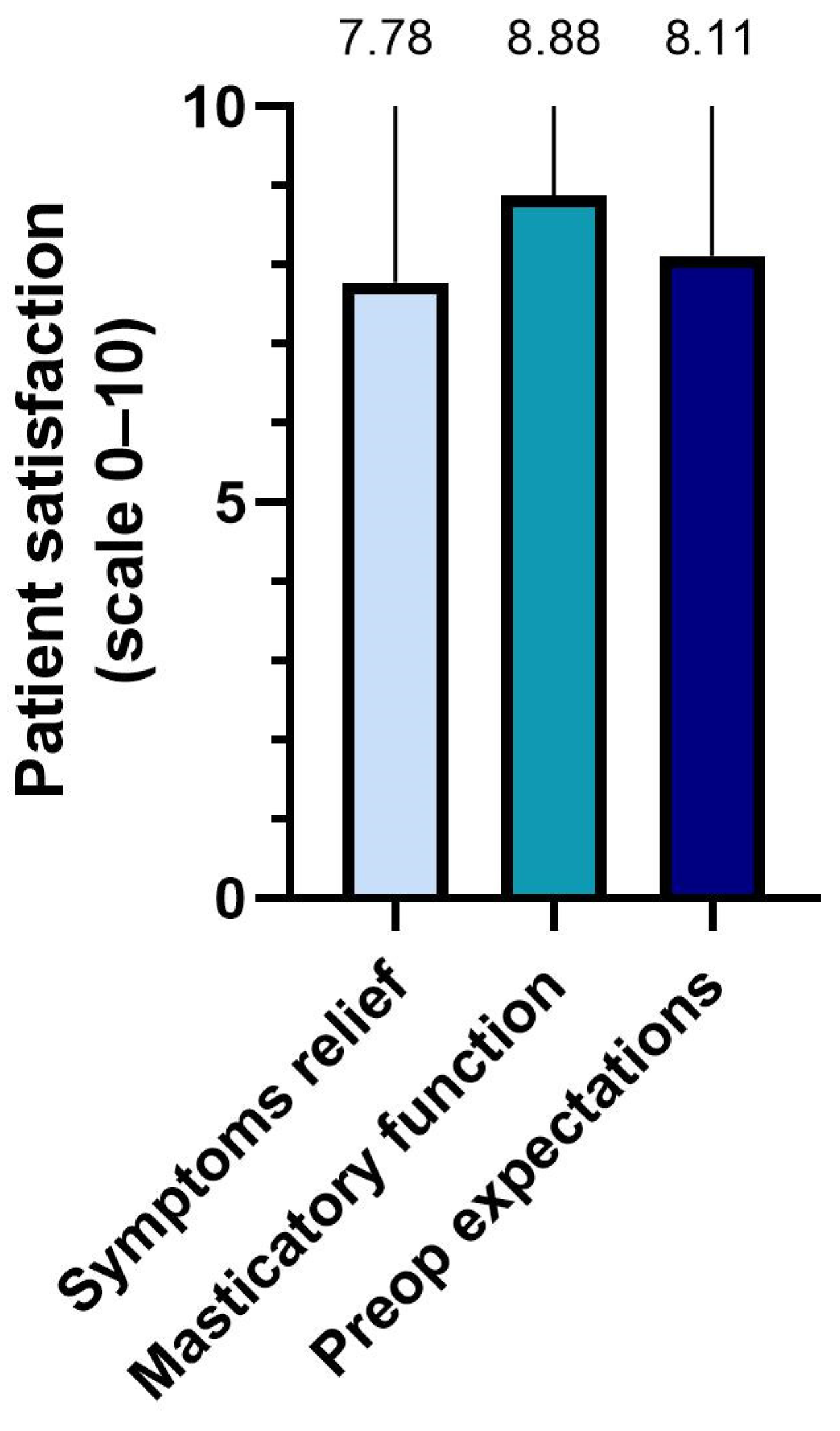
| Participant satisfaction | |
| Question 12 | Are you, overall, satisfied with the relief of your symptoms? |
| Question 13 | Are you satisfied with your masticatory improvement? |
| Question 15 | Were we able to match your preoperative expectations? Are you satisfied with the surgery and your postoperative recovery experiences? |
Appendix B
| Foods | Preparation |
|---|---|
| Potato, of 25–35 mm size (A) | Boil one potato for 15 min and let it cool for another 15 min, before ingestion. |
| Loaf bread (Bimbo® brand) (B) | One slice of loaf bread without crust. |
| Brioche bread, similar to hamburger or hot dog bun (Bimbo® brand) (C) | Break one brioche bread in half. |
| Maria biscuit similar to the Rich Tea biscuit (Vieira® brand) (D) | 1 Maria biscuit. |
| Uncooked almond (E) | Do not cook or peel it. |
 | |
| None of these foods should be broken into smaller pieces (than indicated above) nor be kept inside the mouth too long (softening the food), because these factors might interfere with the results. | |
| The food should be ingested on the days you attend an interview. If you feel any kind of discomfort during the mastication of any of the foods, stop. You should not force the mastication. | |
| Medication/Drug | Dosage | Duration |
|---|---|---|
| Amoxicillin + Clavulanate (875 mg + 125 mg) | 1 pill → 12/12 h | 8 days |
| Clonixin (300 mg) | 1 capsule → 8/8 h | 5 days |
| Paracetamol + Thiocolchicoside (500 mg + 2 mg) | 2 pills → 8/8 h | 5 days |
| Esomeprazole (20 mg) | 1 pill → 24/24 h | 5 days |
| Tramadol (50 mg) | 1 pill → 12/12 h | SOS → If pain persists. Take Ondansetron and Tramadol together |
| Ondansetron (4 mg) | 1 pill → 12/12 h |
| Methylprednisolone | Breakfast | Lunch | Dinner |
|---|---|---|---|
| Postoperative D1 | 8 mg | 8 mg | 8 mg |
| Postoperative D2 | 8 mg | 8 mg | 4 mg |
| Postoperative D3 | 8 mg | 4 mg | 4 mg |
| Postoperative D4 | 4 mg | 4 mg | 4 mg |
| Postoperative D5 | 4 mg | 4 mg | 4 mg |
References
- Peyron, M.A.; Lassauzay, C.; Woda, A. Effects of increased hardness on jaw movement and muscle activity during chewing of visco-elastic model foods. Exp. Brain Res. 2002, 142, 41–51. [Google Scholar] [PubMed]
- van der Bilt, A. Assessment of mastication with implications for oral rehabilitation: A review. J. Oral Rehabil. 2011, 38, 754–780. [Google Scholar] [CrossRef] [PubMed]
- Tonni, I.; Riccardi, G.; Piancino, M.G.; Stretti, C.; Costantinides, F.; Paganelli, C. The influence of food hardness on the physiological parameters of mastication: A systematic review. Arch. Oral Biol. 2020, 120, 104903. [Google Scholar] [CrossRef] [PubMed]
- Pematilleke, N.; Kaur, M.; Adhikari, B.; Torley, P.J. Relationship between masticatory variables and bolus characteristics of meat with different textures. J. Texture Stud. 2021, 52, 552–560. [Google Scholar] [CrossRef]
- Park, Y.S.; Hong, H.P.; Ryu, S.R.; Lee, S.; Shin, W.S. Effects of textured food masticatory performance in older people with different dental conditions. BMC Geriatr. 2022, 22, 384. [Google Scholar] [CrossRef]
- Zhao, L.; Monahan, R. Functional assessment of the stomatognathic system. Clin. Plast. Surg. 2007, 34, e1–e9. [Google Scholar] [CrossRef]
- Bae, Y.; Park, Y. The effect of relaxation exercises for the masticator muscles on temporomandibular joint dysfunction (TMD). J. Phys. Ther. Sci. 2013, 25, 583–586. [Google Scholar] [CrossRef]
- Roberts, W.E.; Goodacre, C.J. The temporomandibular joint: A critical review of life-support functions, development, articular Surfaces, biomechanics and degeneration. J. Prosthodont. 2020, 29, 772–779. [Google Scholar] [CrossRef]
- Wu, M.; Almeida, F.T.; Friesen, R. A systematic review on the association between clinical symptoms and CBCT findings in symptomatic TMJ degenerative joint disease. J. Oral Facial Pain Headache 2021, 35, 332–345. [Google Scholar] [CrossRef]
- Maini, K.; Dua, A. Temporomandibular Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2022; pp. 1–13. [Google Scholar]
- McCain, J.P.; Hossameldin, R.H.; Srouji, S.; Maher, A. Arthroscopic discopexy is effective in managing temporomandibular joint internal derangement in patients with Wilkes stage II and III. J. Oral Maxillofac. Surg. 2015, 73, 391–401. [Google Scholar] [CrossRef]
- McCain, J.P. Arthroscopy of the human temporomandibular joint. J. Oral Maxillofac. Surg. 1988, 46, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Kinard, B.E.; Bouloux, G.F.; Prahalad, S.; Vogler, L.; Abramowicz, S. Arthroscopy of the temporomandibular joint in patients with juvenile idiopathic arthritis. J. Oral Maxillofac. Surg. 2016, 74, 1330–1335. [Google Scholar] [CrossRef] [PubMed]
- Laskin, D.M. Arthroscopy versus arthrocentesis for treating internal derangements of the temporomandibular joint. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.A.; Wolford, L.M.; Ellis, E., 3rd; Neff, A. The hierarchy of different treatments for arthrogenous temporomandibular disorders: A network meta-analysis of randomized clinical trials. J. Craniomaxillofac. Surg. 2020, 48, 9–23. [Google Scholar] [CrossRef] [PubMed]
- González, L.V.; López, J.P.; Díaz-Báez, D.; Orjuela, M.P.; Chavez, M. Clinical outcomes of operative arthroscopy and temporomandibular medical infiltration with platelet-rich fibrin in upper and lower articular space. J. Craniomaxillofac. Surg. 2021, 49, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Guerra, M.F.; Rodríguez-Campo, F.J.; Escorial-Hernández, V.; Sanz-García, A.; Brabyn, P.J.; Fernández-Domínguez, M. Temporomandibular joint arthroscopy in advanced stages of internal derangement: A retrospective cohort study on the influence of age. Int. J. Oral Maxillofac. Surg. 2022, 51, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Locker, D.; Slade, G. Prevalence of symptoms associated with temporomandibular disorders in a Canadian population. Community Dent. Oral Epidemiol. 1988, 16, 310–313. [Google Scholar] [CrossRef]
- Nourallah, H.; Johansson, A. Prevalence of signs and symptoms of temporomandibular disorders in a young male Saudi population. J. Oral Rehabil. 1995, 22, 343–347. [Google Scholar] [CrossRef]
- Yule, P.L.; Durham, J.; Playford, H.; Moufti, M.A.; Steele, J.; Steen, N.; Wassell, R.W.; Ohrbach, R. OHIP-TMDs: A patient-reported outcome measure for temporomandibular disorders. Community Dent. Oral Epidemiol. 2015, 43, 461–470. [Google Scholar] [CrossRef]
- Su, N.; Liu, Y.; Yang, X.; Shen, J.; Wang, H. Correlation between oral health-related quality of life and clinical dysfunction index in patients with temporomandibular joint osteoarthritis. J. Oral Sci. 2016, 58, 483–490. [Google Scholar] [CrossRef]
- Trize, D.M.; Calabria, M.P.; Franzolin, S.O.B.; Cunha, C.O.; Marta, S.N. Is quality of life affected by temporomandibular disorders? Einstein 2018, 16, eAO4339. [Google Scholar] [CrossRef] [PubMed]
- Machoň, V.; Levorová, J.; Hirjak, D.; Beňo, M.; Drahoš, M.; Foltán, R. Does arthroscopic lysis and lavage in subjects with Wilkes III internal derangement reduce pain? Oral Maxillofac. Surg. 2021, 25, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Dimitroulis, G. A new surgical classification for temporomandibular joint disorders. Int. J. Oral Maxillofac. Surg. 2013, 42, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Ângelo, D.F.; Araújo, R.A.D.; Sanz, D. Surgical complications related to temporomandibular joint arthroscopy: A prospective analysis of 39 single-portal versus 43 double-portal procedures. Int. J. Oral Maxillofac. Surg. 2021, 50, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Ângelo, D.F.; de Barros, R.C.M. Routine ear canal and tympanic membrane inspection after temporomandibular joint arthroscopy-correspondence. Int. J. Surg. 2022, 101, 106646. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Wilk, B.R.; Stenback, J.T.; McCain, J.P. Postarthroscopy physical therapy management of a patient with temporomandibular joint dysfunction. J. Orthop. Sport. Phys. Ther. 1993, 18, 473–478. [Google Scholar] [CrossRef]






| Participant (#) | Age | Profession | Principal Diagnosis | Dimitroulis Classification | TMJ Intervention |
|---|---|---|---|---|---|
| 1 | 39 | Administrative | DDwoR | 3 | Bilateral Arthroscopy |
| 2 | 54 | Security | DDwoR | 3 | Bilateral Arthroscopy |
| 3 | 18 | Student | DDwoR | 3 | Unilateral Arthroscopy |
| 4 | 23 | Student | DDwR | 2 | Bilateral Arthroscopy |
| 5 | 31 | Music Teacher | DDwoR | 3 | Bilateral Arthroscopy |
| 6 | 36 | Business | DDwoR | 3 | Bilateral Arthroscopy |
| 7 | 43 | Beauty Artist | DDwoR | 3 | Unilateral Arthroscopy |
| 8 | 25 | Administrative | DDwR | 3 | Bilateral Arthroscopy |
| 9 | 18 | Student | DDwR | 2 | Bilateral Arthroscopy |
| Mean (±SD) | 31.67 (±12.51) |
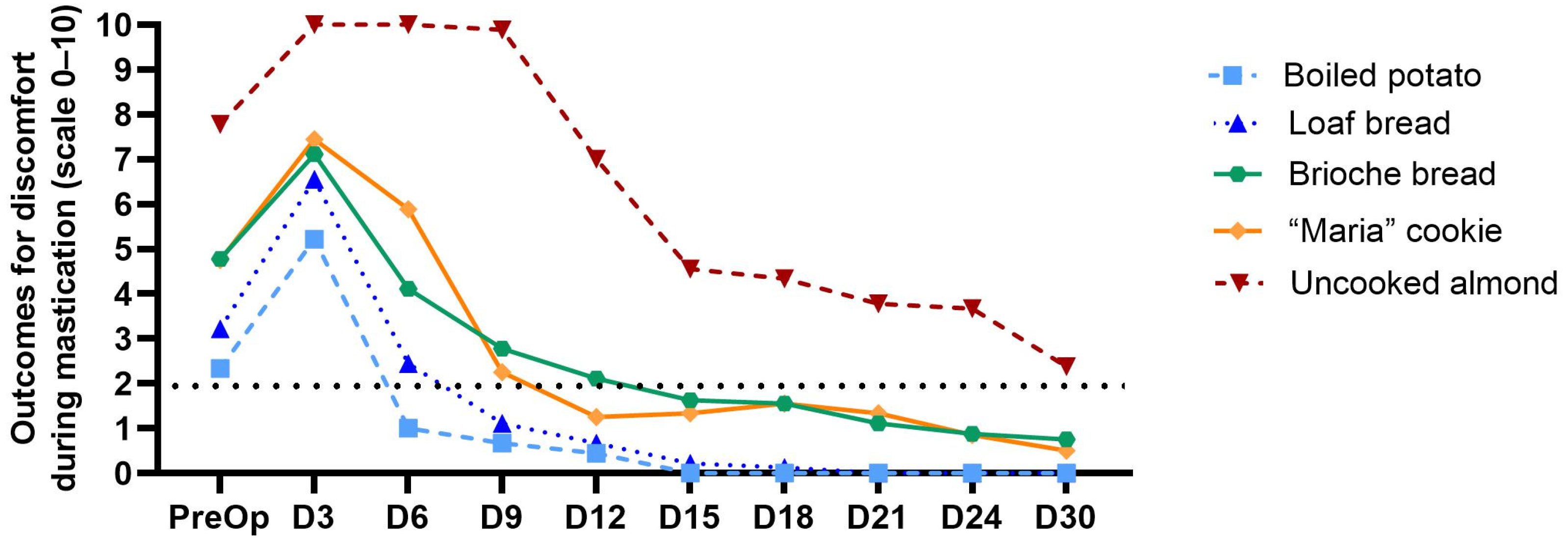
| Discomfort in the Mastication | |||||
|---|---|---|---|---|---|
| Soft Texture | Medium Texture | Hard Texture | |||
| Boiled Potato | Loaf Bread Slice | Brioche Bread | “Maria” Biscuit | Uncooked Almond | |
| (Mean ± SD) | |||||
| Preoperative | 2.33 ± 1.58 | 3.22 ± 2.39 | 4.78 ± 2.53 | 4.75 ± 2.66 | 7.78 ± 2.44 |
| D3 | 5.22 ± 4.49 | 6.56 ± 4.28 | 7.11 ± 3.52 | 7.44 ± 3.84 | 10.00 ± 0.00 |
| D6 | 1.00 ± 1.51 | 2.44 ± 2.96 | 4.11 ± 3.10 | 5.89 ± 3.92 | 10.00 ± 0.00 |
| D9 | 0.67 ± 1.12 | 1.11 ± 1.36 | 2.78 ± 2.17 | 2.25 ± 1.75 | 10.00 ± 0.00 |
| D12 | 0.44 ± 0.88 | 0.67 ± 1.12 | 2.11 ± 1.69 | 1.25 ± 1.83 | 7.00 ± 3.74 |
| D15 | 0.00 ± 0.00 * | 0.22 ± 0.44 * | 1.63 ± 1.77 | 1.33 ± 1.94 | 4.56 ± 4.07 |
| D18 | 0.00 ± 0.00 * | 0.13 ± 0.35 * | 1.56 ± 1.94 | 1.56 ± 1.81 | 4.33 ± 3.71 |
| D21 | 0.00 ± 0.00 * | 0.00 ± 0.00 * | 1.11 ± 1.83 * | 1.33 ± 1.73 * | 3.78 ± 4.02 |
| D24 | 0.00 ± 0.00 * | 0.00 ± 0.00 * | 0.88 ± 1.25 * | 0.85 ± 1.46 * | 3.67 ± 4.18 |
| D30 | 0.00 ± 0.00 * | 0.00 ± 0.00 * | 0.75 ± 1.17 * | 0.50 ± 1.07 * | 2.38 ± 3.78 |
| X2(9) | 32.72 | 41.54 | 38.26 | 39.02 | 42.08 |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Kendall’s W | 0.52 | 0.58 | 0.53 | 0.62 | 0.58 |
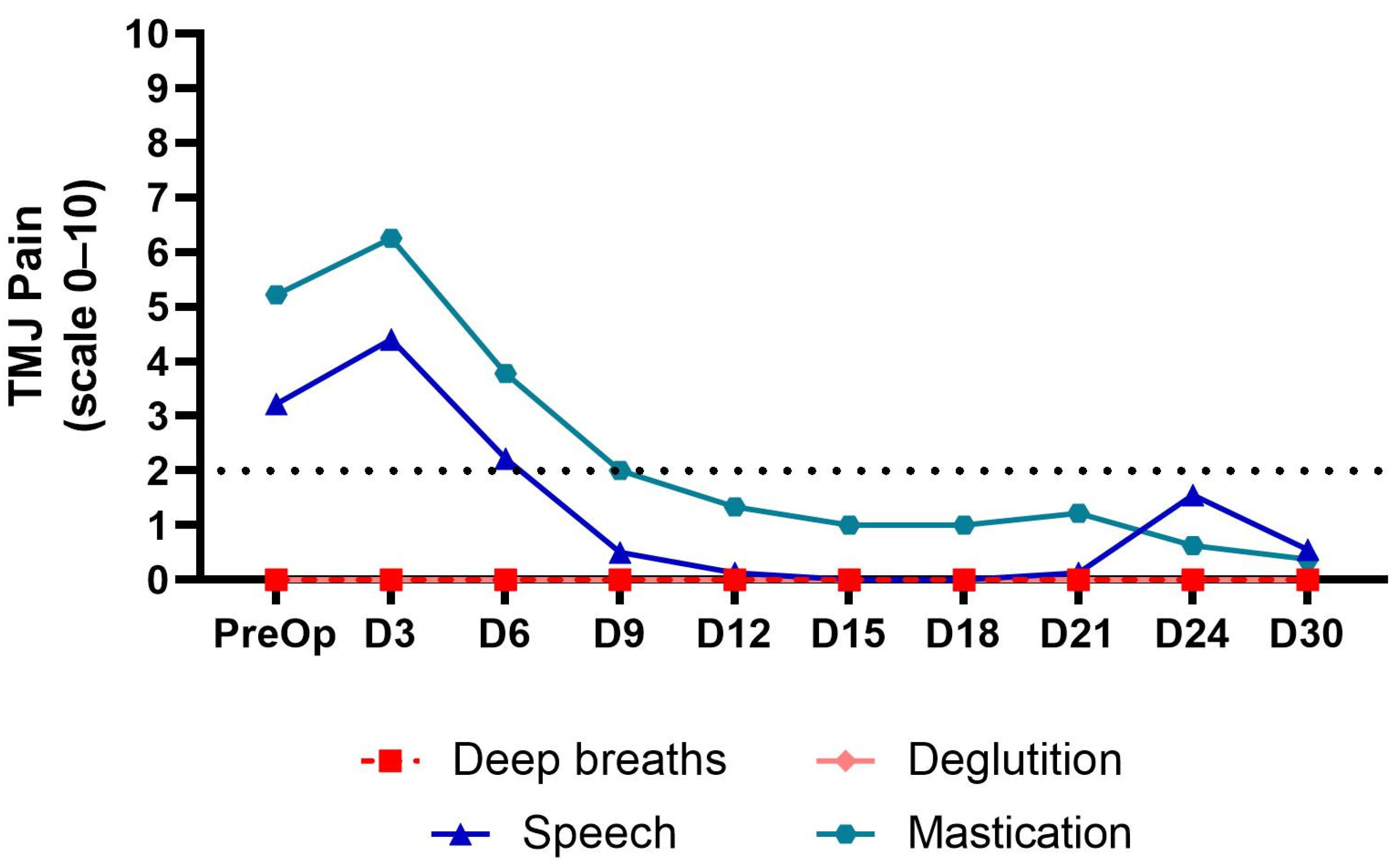
| TMJ Pain | ||||
|---|---|---|---|---|
| During Deep Breaths | During Speech | During Mastication | During Deglutition | |
| (Mean ± SD) | ||||
| Preoperative | 0.00 ± 0.00 | 3.22 ± 3.11 | 5.22 ± 2.99 | 0.00 ± 0.00 |
| D3 | 0.00 ± 0.00 | 4.40 ± 2.19 | 4.11 ± 2.57 | 0.00 ± 0.00 |
| D6 | 0.00 ± 0.00 | 2.22 ± 2.64 | 3.78 ± 2.77 | 0.00 ± 0.00 |
| D9 | 0.00 ± 0.00 | 0.50 ± 0.76 | 2.00 ± 1.94 | 0.00 ± 0.00 |
| D12 | 0.00 ± 0.00 | 0.13 ± 0.35 * | 1.33 ± 1.32 | 0.00 ± 0.00 |
| D15 | 0.00 ± 0.00 | 0.00 ± 0.00 * | 1.00 ± 1.41 * | 0.00 ± 0.00 |
| D18 | 0.00 ± 0.00 | 0.00 ± 0.00 * | 1.00 ± 1.32 ** | 0.00 ± 0.00 |
| D21 | 0.00 ± 0.00 | 0.13 ± 0.35 * | 1.22 ± 1.99 * | 0.00 ± 0.00 |
| D24 | 0.00 ± 0.00 | 1.56 ± 2.46 | 0.63 ± 1.19 ** | 0.00 ± 0.00 |
| D30 | 0.00 ± 0.00 | 0.56 ± 0.88 * | 0.38 ± 0.74 ** | 0.00 ± 0.00 |
| X2(9) | 25.85 | 39.82 | ||
| p | 0.002 | <0.001 | ||
| Kendall’s W | 0.479 | 0.553 | ||
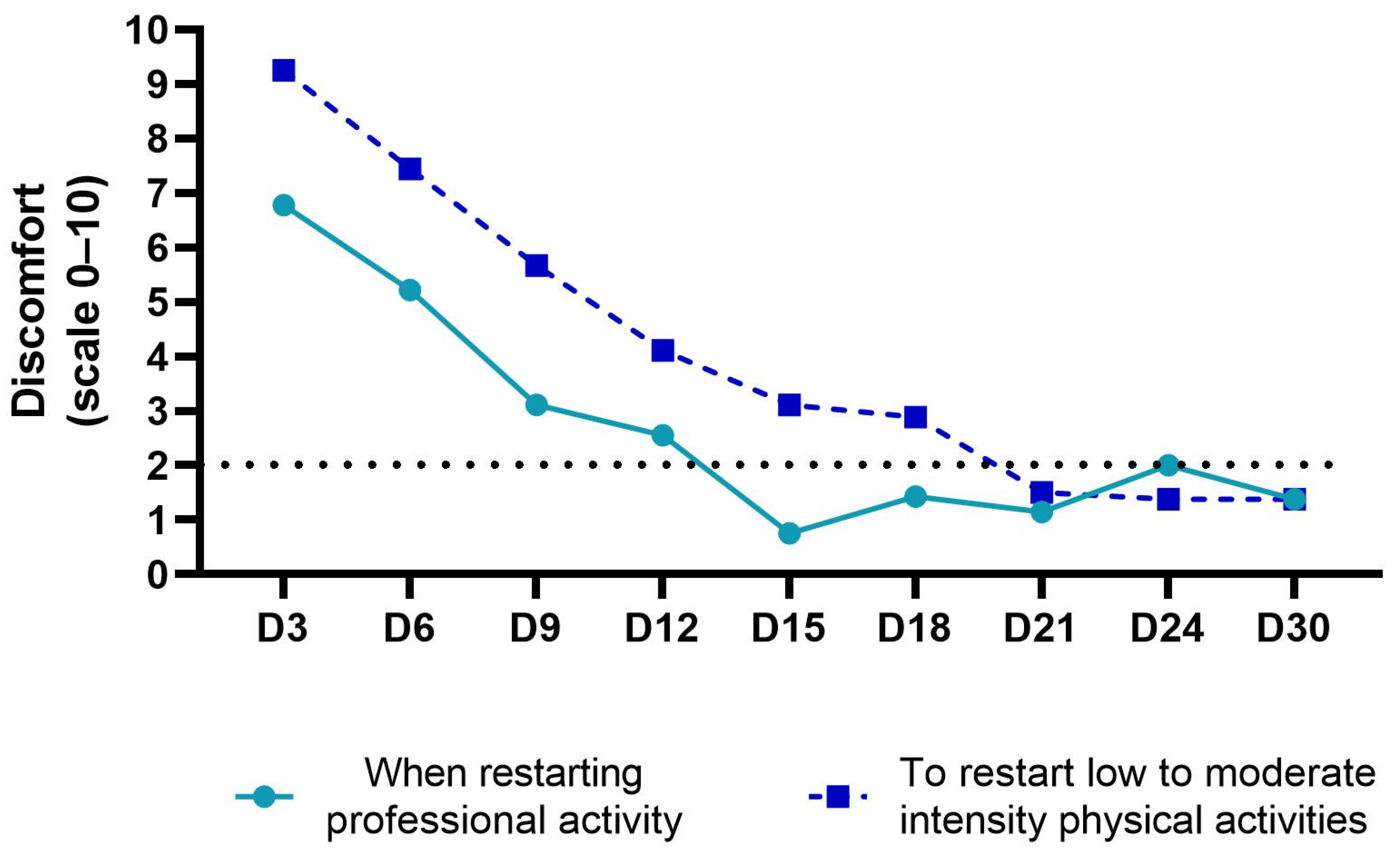
| Discomfort when Restarting Professional Activity | Discomfort when Restarting Moderate to High-Intensity Physical Activities | |
|---|---|---|
| Mean ± SD | ||
| D3 | 6.78 ± 2.68 | 9.25 ± 1.49 |
| D6 | 5.22 ± 3.31 | 7.44 ± 3.4 |
| D9 | 3.11 ± 3.55 | 5.67 ± 3.2 |
| D12 | 2.56 ± 2.40 | 4.11 ± 3.2 |
| D15 | 0.75 ± 1.39 ** | 3.11 ± 3.86 |
| D18 | 1.43 ± 2.3 * | 2.89 ± 3.98 |
| D21 | 1.14 ± 2.19 * | 1.50 ± 3.46 * |
| D24 | 2.00 ± 3.70 * | 1.38 ± 3.50 * |
| D30 | 1.38 ± 3.50 * | 1.38 ± 3.50 * |
| X2(8) | 28.08 | 28.38 |
| p | <0.001 | <0.001 |
| Kendall’s W | 0.44 | 0.44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ângelo, D.F.; Prior, A.; Cardoso, H.J. Postoperative Recovery after TMJ Arthroscopy: Masticatory Improvement and Postoperative Diet. Oral 2023, 3, 191-202. https://doi.org/10.3390/oral3020017
Ângelo DF, Prior A, Cardoso HJ. Postoperative Recovery after TMJ Arthroscopy: Masticatory Improvement and Postoperative Diet. Oral. 2023; 3(2):191-202. https://doi.org/10.3390/oral3020017
Chicago/Turabian StyleÂngelo, David Faustino, André Prior, and Henrique José Cardoso. 2023. "Postoperative Recovery after TMJ Arthroscopy: Masticatory Improvement and Postoperative Diet" Oral 3, no. 2: 191-202. https://doi.org/10.3390/oral3020017