
Efficacy of Elastodontic Devices vs. Clear Aligners in Lower Intercanine Distance Changes Assessed by Computer-Aided Evaluation

Abstract
:1. Introduction
2. Material and Methods
Study Sample
3. Experimental Settings
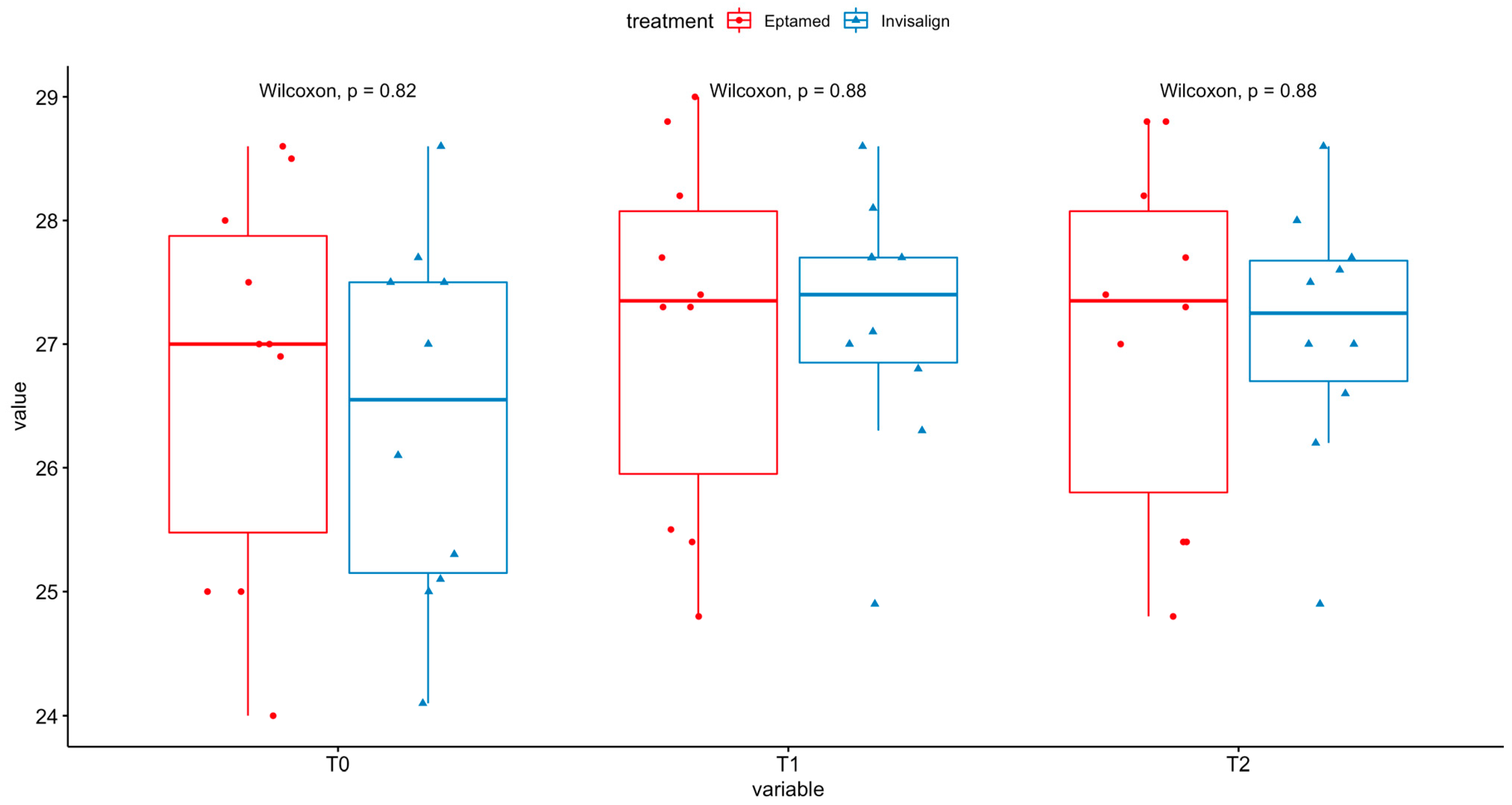
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bishara, S.E.; Treder, J.E.; Jakobsen, J.R. Facial and dental changes in adulthood. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Rapeepattana, S.; Thearmontree, A.; Suntornlohanakul, S. Etiology of Malocclusion and Dominant Orthodontic Problems in Mixed Dentition: A Cross-sectional Study in a Group of Thai Children Aged 8-9 Years. J. Int. Soc. Prev. Community Dent. 2019, 9, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef] [PubMed]
- Ortu, E.; Pietropaoli, D.; Cova, S.; Marci, M.C.; Monaco, A. Efficacy of elastodontic devices in overjet and overbite reduction assessed by computer-aid evaluation. BMC Oral Health 2021, 21, 269. [Google Scholar] [CrossRef] [PubMed]
- Ravera, S.; Rollet, D.; Cugliari, G.; Deregibus, A.; Castroflorio, T. Interceptive treatment effects of EF preformed appliance in pre-pubertal and pubertal skeletal Class II growing patients: A retrospective controlled study. Eur. J. Paediatr. Dent. 2020, 21, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Aprile, G.; Ortu, E.; Cattaneo, R.; Pietropaoli, D.; Giannoni, M.; Monaco, A. Orthodontic management by functional activator treatment: A case report. J. Med. Case Rep. 2017, 11, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caruso, S.; Nota, A.; Ehsani, S.; Maddalone, E.; Ojima, K.; Tecco, S. Impact of molar teeth distalization with clear aligners on occlusal vertical dimension: A retrospective study. BMC Oral Health 2019, 19, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brook, P.H.; Shaw, W.C. The development of an index of orthodontic treatment priority. Eur. J. Orthod. 1989, 11, 309–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, C.; Richmond, S. The development of the index of complexity, outcome and need (ICON). J. Orthod. 2000, 27, 149–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibasaki, W.M.M.; da Silva, L.H.; Fuziy, A.; Trivino, T.; Costa, A.L.F.; Nahas-Scocate, A.C.R. Evaluation of lower anterior dental changes in patients treated with self-ligating brackets. J. Oral Biol. Craniofac. Res. 2019, 9, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Boyd, K.; Saccomanno, S.; Lewis, C.J.; Coceani Paskay, L.; Quinzi, V.; Marzo, G. Myofunctional therapy. Part 1: Culture, industrialisation and the shrinking human face. Eur. J. Paediatr. Dent. 2021, 22, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Nota, A.; Caruso, S.; Severino, M.; Gatto, R.; Meuli, S.; Mattei, A.; Tecco, S. Mandibular advancement with clear aligners in the treatment of skeletal Class II. A retrospective controlled study. Eur. J. Paediatr. Dent. 2021, 22, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Kassas, W.; Al-Jewair, T.; Preston, C.B.; Tabbaa, S. Assessment of Invisalign treatment outcomes using the ABO Model Grading System. J. World Fed. Orthod. 2013, 2, e61–e64. [Google Scholar] [CrossRef]
- Yıldırım, A. A Prospective Study to Determine the Efficiency of Clear Aligner Appliance. Ph.D. Thesis., Istanbul University Institute of Health Sciences Orthodontics Department, Istanbul, Turkey, 2013. [Google Scholar]
- Ortu, E.; Barrucci, G.; Aprile, G.; Guerrini, L.; Pietropaoli, D.; Monaco, A. Electromyographic evaluation during orthodontic therapy: Comparison of two elastodontic devices. J. Biol. Regul. Homeost. Agents 2020, 34, 1935–1939. [Google Scholar] [CrossRef] [PubMed]
- Marra, P.M.; Fiorillo, L.; Cervino, G.; Cardarelli, F.; Cicciu, M.; Laino, L. Elastodontic treatment with oral bio-activators in young children. Minerva Dent. Oral Sci. 2022, 71, 270–276. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Stratified by Treatment | |||
|---|---|---|---|
| Eptamed | Invisalign | ||
| n | 10 | 10 | p |
| sex = M (%) | 5 (50.0) | 5 (50.0) | 1.000 |
| age (mean (SD)) | 10.40 (1.58) | 10.80 (1.62) | 0.583 |
| T0 (mean (SD)) | 26.75 (1.58) | 26.39 (1.47) | 0.605 |
| T1 (mean (SD)) | 27.14 (1.45) | 27.19 (1.05) | 0.931 |
| T2 (mean (SD)) | 27.08 (1.44) | 27.11 (1.04) | 0.958 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortu, E.; Pietropaoli, D.; Cova, S.; Giannoni, M.; Monaco, A. Efficacy of Elastodontic Devices vs. Clear Aligners in Lower Intercanine Distance Changes Assessed by Computer-Aided Evaluation. Oral 2023, 3, 31-37. https://doi.org/10.3390/oral3010003
Ortu E, Pietropaoli D, Cova S, Giannoni M, Monaco A. Efficacy of Elastodontic Devices vs. Clear Aligners in Lower Intercanine Distance Changes Assessed by Computer-Aided Evaluation. Oral. 2023; 3(1):31-37. https://doi.org/10.3390/oral3010003
Chicago/Turabian StyleOrtu, Eleonora, Davide Pietropaoli, Samuele Cova, Mario Giannoni, and Annalisa Monaco. 2023. "Efficacy of Elastodontic Devices vs. Clear Aligners in Lower Intercanine Distance Changes Assessed by Computer-Aided Evaluation" Oral 3, no. 1: 31-37. https://doi.org/10.3390/oral3010003