
The Clinical Characteristics of Immunoglobulin Light Chain Amyloidosis in the Chinese Population: A Systematic Scoping Review
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
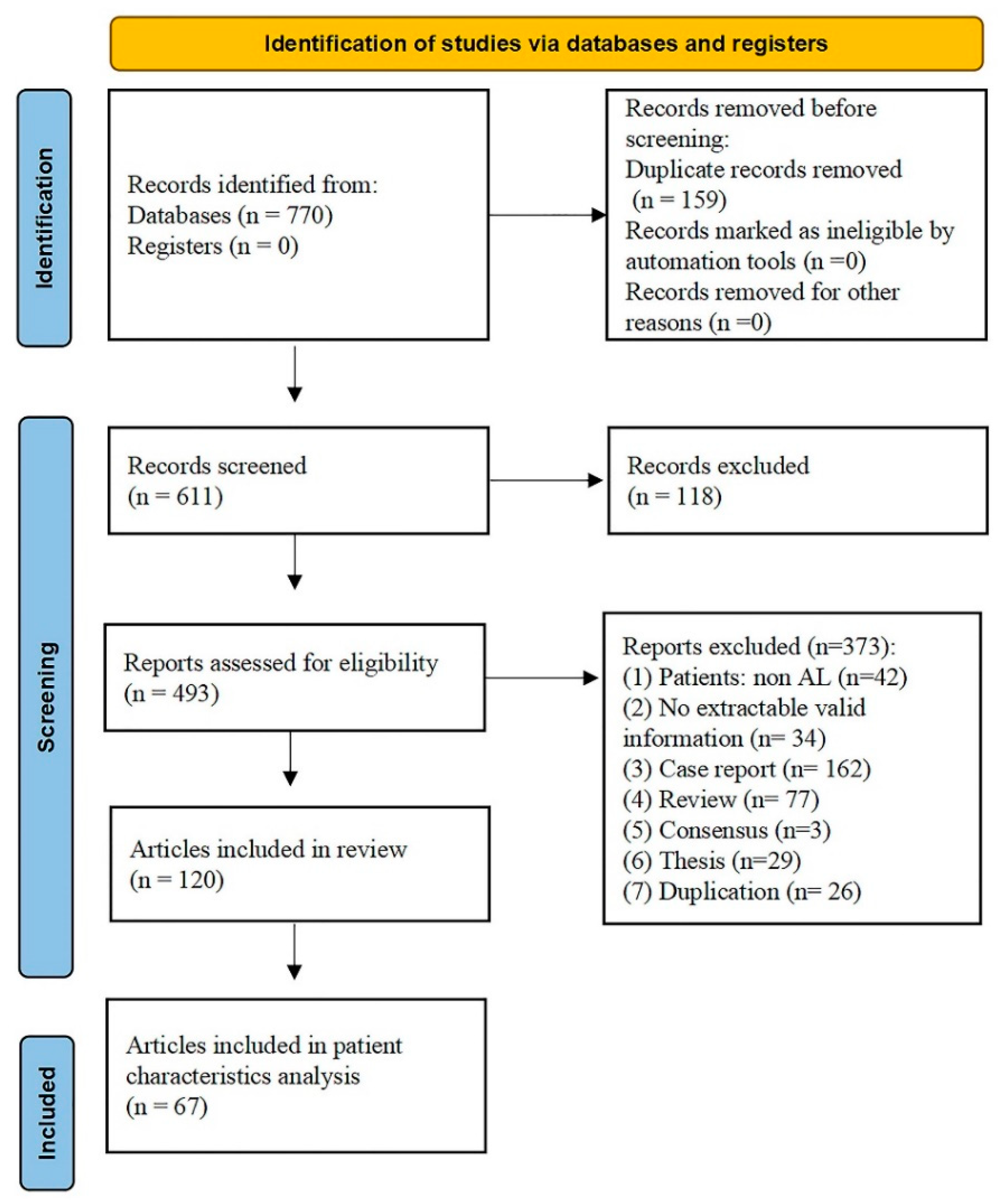
2.2. Eligibility Criteria and Literature Screening
2.3. Data Extraction
2.4. Statistical Analyses
3. Results
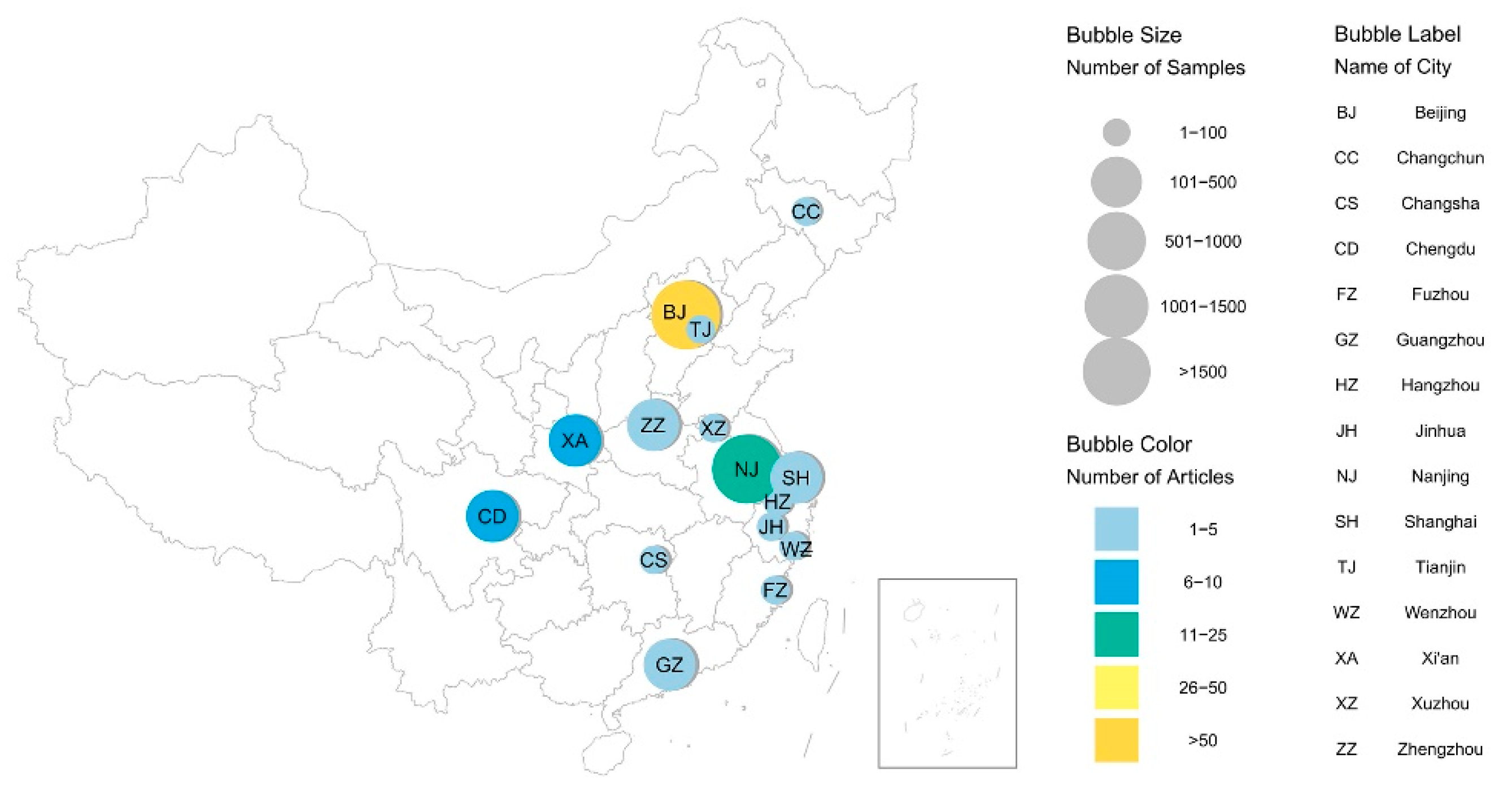
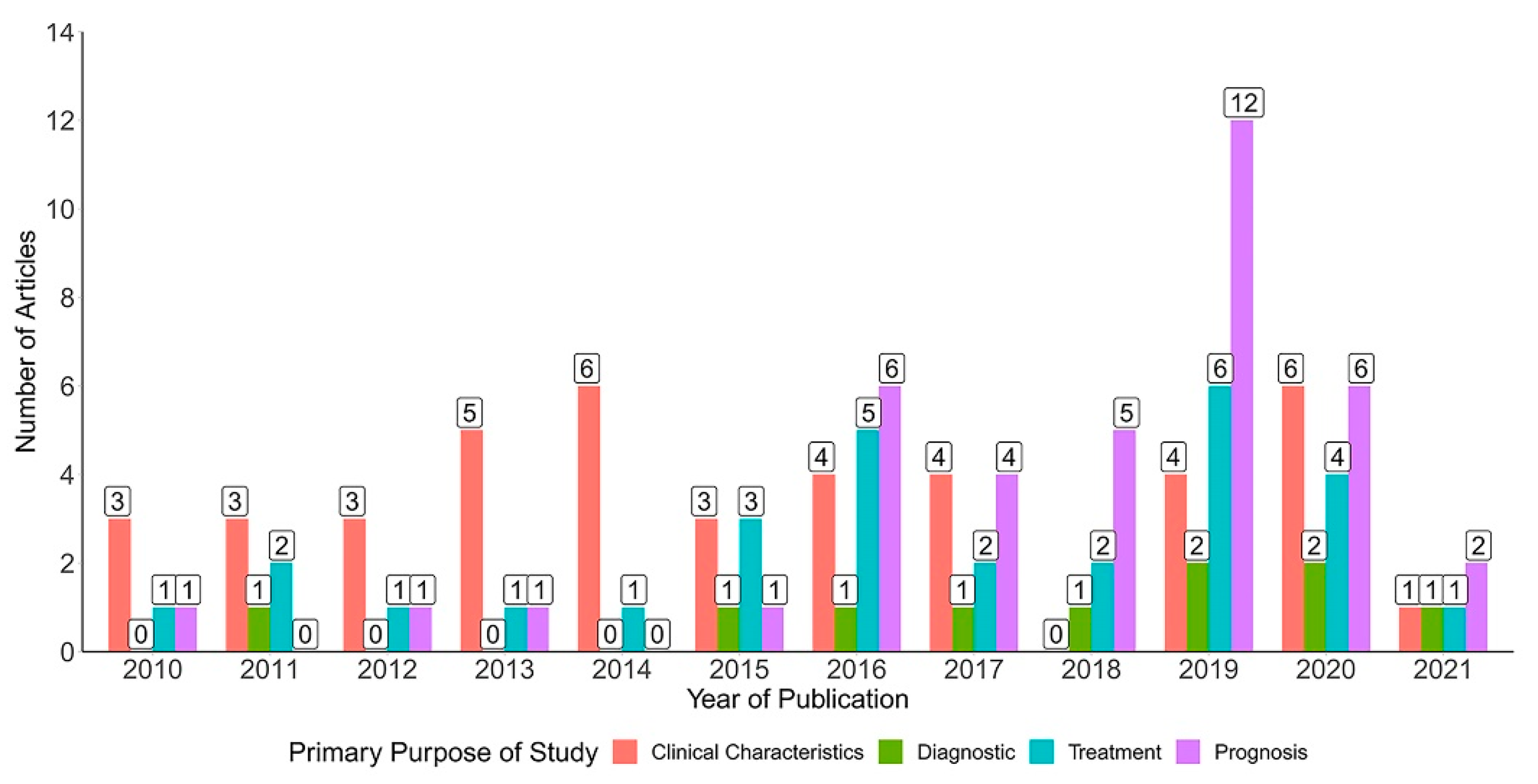
3.1. Description of the Included Studies

3.2. Clinical Characteristics of Patients with AL Amyloidosis
3.3. Organ Involvement
3.4. Proportion of Plasma Cells in Bone Marrow
3.5. Prognostic Indicators
4. Discussion
4.1. Summary of Evidence
4.2. Comparison with Other Studies
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Quock, T.P.; Yan, T.; Chang, E.; Guthrie, S.; Broder, M.S. Epidemiology of AL amyloidosis: A real-world study using US claims data. Blood Adv. 2018, 2, 1046–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merlini, G. AL amyloidosis: From molecular mechanisms to targeted therapies. Hematol. Am. Soc. Hematol. Educ. Program 2017, 2017, 1–12. [Google Scholar] [CrossRef] [PubMed]
- McCausland, K.L.; White, M.K.; Guthrie, S.D.; Quock, T.; Finkel, M.; Lousada, I.; Bayliss, M.S. Light Chain (AL) Amyloidosis: The Journey to Diagnosis. Patient-Patient-Cent. Outcomes Res. 2017, 11, 207–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulman, A.; Connors, L.H.; Weinberg, J.; Mendelson, L.M.; Joshi, T.; Shelton, A.C.; Sanchorawala, V. Patient outcomes in light chain (AL) amyloidosis: The clock is ticking from symptoms to diagnosis. Eur. J. Haematol. 2020, 105, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Gertz, M.A. Immunoglobulin light chain amyloidosis: 2020 update on diagnosis, prognosis, and treatment. Am. J. Hematol. 2020, 95, 848–860. [Google Scholar] [CrossRef]
- Gertz, M.A.; Dispenzieri, A. Systemic Amyloidosis Recognition, Prognosis, and Therapy: A Systematic Review. JAMA 2020, 324, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Desport, E.; Bridoux, F.; Sirac, C.; Delbes, S.; Bender, S.; Fernandez, B.; Quellard, N.; Lacombe, C.; Goujon, J.M.; Lavergne, D.; et al. Al amyloidosis. Orphanet J. Rare Dis. 2012, 7, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.-H.; Liu, Z.-H. The Clinical Presentation and Management of Systemic Light-Chain Amyloidosis in China. Kidney Dis. 2016, 2, 1–9. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, G.E.; Stahl, A.; Voegeler, J.; Quiering, C.; Lorenz, K.; Spital, G.; Liakopoulos, S. Efficacy and safety of ranibizumab with or without panretinal laser photocoagulation versus laser photocoagulation alone in proliferative diabetic retinopathy—NThe PRIDE study. Acta Ophthalmol. 2019, 98. [Google Scholar] [CrossRef]
- An, Y.F.; Wang, X.H.; Cai, B.; Li, L.X. Application value of serum free light chain ratio in diagnosis of myocardial amyloidosis. Int. J. Lab. Med. 2021, 42, 99–102. [Google Scholar]
- Chen, W.C.; Huang, X.H.; Wang, Q.W. Efficacy and safety of lenalidomide with dexamethasone in relapse/refractory light-chain amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2017, 26, 201–205. [Google Scholar]
- Chen, N. Bortezomib in the treatment of kidney light chain amyloidosis. J. Am. Soc. Nephrol. 2018, 29, 478. [Google Scholar]
- Chen, Q.H.; Huang, X.H.; Zhao, L. Factors influencing engraftment after autologus peripheral blood stem cell trans-plantation for light chain amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2019, 28, 301–306. [Google Scholar]
- Cheng, Z.-W.; Tian, Z.; Kang, L.; Chen, T.-B.; Fang, L.-G.; Cheng, K.-A.; Zeng, Y.; Fang, Q. Electrocardiographic and echocardiographic features of patients with primary cardiac amyloidosis. Chin. J. Cardiol. 2010, 38, 606–609. [Google Scholar]
- Cui, Q.; Yu, J.; Shen, W. Late gadolinium enhancement and T1 mapping for the diagnosis of cardiac amyloidosis. Chin. Crit. Care Med. 2019, 31, 1538–1541. [Google Scholar]
- Diao, X.; Li, J.; Ouyang, J.; Liu, J.; Huang, B.; Chen, M.; Gu, J. Flow cytometry-based immunophenotypic analysis of primary systemic light chain amy-loidosis. Oncol. Lett. 2017, 13, 2691–2697. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.J.; Wu, G.; Zhang, S.S. Clinical characteristics and screening indexes of light chain amyloidosis nephropathy. Chin. J. Pract. Med. 2019, 23, 6–10. [Google Scholar]
- Feng, J.; Huang, X.F.; Zhang, C.L.; Shen, K.N.; Sun, J.; Tian, Z.; Cao, X.X.; Zhang, L.; Zhou, D.B.; Li, J. Analysis of clinical characteristics and outcome of patients with very high risk primary immunoglobulin light-chain amyloidosis. Chin. J. Hematol. 2017, 38, 107–111. [Google Scholar]
- Feng, J.; Zhang, C.; Shen, K.; Sun, J.; Fang, Q.; Zhang, L.; Cao, X.; Zhou, D.; Li, J.; Tian, Z. Outcome of Cardiac Light-Chain Amyloidosis in the Era of Novel Therapy―A Single-Center Cohort Study of 227 Patients. Circ. J. 2019, 83, 775–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, L.J.; Chen, H.B.; Xiang, X.J. Analysis of clinical manifestations and immunoglobulin typing of monoclonal immu-noglobulin-related renal injury. Zhejiang Med. J. 2020, 42, 1193–1195. [Google Scholar]
- He, H.; Liu, J.; Jiang, H.; Du, J.; Li, L.; Lu, J.; Fu, W. High Serum Lactate Dehydrogenase adds Prognostic Value to Cardiac Biomarker Staging System for Light Chain Amyloidosis. J. Cancer 2019, 10, 5622–5627. [Google Scholar] [CrossRef]
- Hu, Y.; Zhu, P.; Zhang, Y.; Liang, C.X.; Liu, Q.; Xing, H.Z. Detection of Abnormal Bone Marrow Plasma Cell Clones for the Diagnosis of Systemic Light Chain Amyloidosis. In Proceedings of the 13th National Conference on Experimental Hematology, Wuhan, China, 24 November 2011. [Google Scholar]
- Hu, Y.; Wang, M.; Chen, Y.; Chen, X.; Fang, F.; Shiqin, L.; Zhang, Y.; Wu, X.; Zhu, P. The Significance of Abnormal Plasma Cell Clone In Bone Marrow Of Primary Systemic Light Chain Amyloidosis Patients. Blood 2013, 122, 5342. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, M.; Chen, Y.; Chen, X.; Fang, F.; Liu, S.; Zhang, Y.; Wu, X.; Zhu, P. Immunophenotypic analysis of abnormal plasma cell clones in bone marrow of primary systemic light chain amyloidosis patients. Chin. Med. J. 2014, 127, 2765–2770. [Google Scholar]
- Huang, X.H.; Wang, Q.W.; Shi, M.J.; Chen, W.C.; Jiang, S.; Gong, D.H.; Zeng, C.H.; Zhao, M.; Liu, Z.H. Efficency and safety of autologus stem cell transplantation for primary systemic amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2011, 4, 312–318. [Google Scholar]
- Huang, B.H.; Li, J.; Zhou, Z.H.; Zheng, D.; Gu, J.L. Bortezomib Combined with Dexamethasone in the Treatment of Initial Systemic Light Chain Amyloidosis. In Proceedings of the 13th National Conference on Experimental Hematology, Wuhan, China, 24 November 2011. [Google Scholar]
- Huang, B.; Li, J.; Liu, J.; Zheng, N.; Chen, M.; Zhou, Z.; Xu, D.; Zou, W. Bortezomib with Dexamethasone in Newly Diagnosed Patients with Primary Systemic Light Chain Amyloidosis or Multiple Myeloma-Associated AL Amyloidosis. Blood 2012, 120, 5036. [Google Scholar] [CrossRef]
- Huang, X.H.; Jiang, S.; Shi, M.J.; Chen, W.C.; Wang, Q.W.; Zeng, C.H.; Liu, Z.H. Outcomes and risk factors in patients with idiopathic AL amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2012, 21, 304–310. [Google Scholar]
- Huang, X.; Wang, Q.; Chen, W.; Zeng, C.; Chen, Z.; Gong, D.; Zhang, H.; Liu, Z. Induction therapy with bortezomib and dexamethasone followed by autologous stem cell transplantation versus autologous stem cell transplantation alone in the treatment of renal AL amyloidosis: A randomized controlled trial. BMC Med. 2014, 12, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Jing, X.-C.; Hu, Z.; Chen, X.; Liu, X.-Q. Early Impairment of Cardiac Function and Asynchronization of Systemic Amyloidosis with Preserved Ejection Fraction Using Two-Dimensional Speckle Tracking Echocardiography. Echocardiography 2015, 32, 1832–1840. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Li, J.; Xu, X.; Zheng, D.; Zhou, Z. Successful treatment of renal light chain (AL) amyloidosis with bortezomib and dexamethasone (VD). Pathol. Biol. 2015, 63, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Wang, Q.; Jiang, S.; Chen, W.; Zeng, C.; Liu, Z. The clinical features and outcomes of systemic AL amyloidosis: A cohort of 231 Chinese patients. Clin. Kidney J. 2014, 8, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.H.; Wang, Q.W.; Chen, W.C.; Gong, D.H.; Zeng, C.H.; Liu, Z.H. Bortezomib before, during and after autologous hematopoietic stem cell trans-plantation in patients with newly diagnosed al amyloidosis. Hong Kong J. Nephrol. 2015, 17, 60–61. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Wang, Q.; Chen, W.; Ren, G.; Liu, Z. Bortezomib with dexamethasone as first-line treatment for AL amyloidosis with renal involvement. Amyloid 2016, 23, 51–57. [Google Scholar] [CrossRef]
- Huang, X.; Feng, J.; Zhang, C.; Shen, K.; Sun, J.; Tian, Z.; Cao, X.; Zhang, L.; Zhou, D.; Li, J. The usage of Mayo staging system in Chinese patients with primary light chain amy-loidosis. Chin. J. Hematol. 2016, 37, 278–282. [Google Scholar]
- Huang, X.; Fu, C.; Chen, L.; Chen, W.; Ren, G.; Guo, J.; Zhao, L.; Zeng, C.; Zhang, H.; Gong, D.; et al. Combination of bortezomib in the induction, conditioning and consolidation with au-tologous hematopoietic stem cell transplantation in patients with immunoglobulin light chain amyloidosis. Am. J. Hematol. 2019, 94, 101–104. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.-F.; Jian, S.; Lu, J.; Shen, K.-N.; Feng, J.; Zhang, C.-L.; Tian, Z.; Wang, J.-L.; Lei, W.-J.; Cao, X.-X.; et al. Genomic profiling in amyloid light-chain amyloidosis reveals mutation profiles associated with overall survival. Amyloid 2019, 27, 36–44. [Google Scholar] [CrossRef]
- Huang, X.; Ren, G.; Chen, W.; Guo, J.; Zhao, L.; Zeng, C.; Ge, Y.; Liu, Z. The role of induction therapy before autologous stem cell transplantation in low disease burden AL amyloidosis patients. Amyloid 2020, 28, 75–83. [Google Scholar] [CrossRef]
- Ji, J.; Fang, L.G.; Fang, Q.; Zhu, W.L. Clinical analysis of 104 cases with cardiac amyloidosis. Chin. J. Heart Fail. Cardiomyopathy 2017, 1, 98–103. [Google Scholar]
- Lei, C.H.; Zhu, X.L.; Liu, L.W.; Zuo, L.; Yang, F.; Wang, Y.; Ma, Z.L. Value of Echocardiography in Prognosis of Patients with High-risk Primary Light-chain Cardiac Amyloidosis. Chin. J. Ultrasound Med. 2019, 35, 1001–1004. [Google Scholar]
- Lei, C.H.; Zuo, L.; Wang, Y.; Zhu, X.; Zhou, M.; Yang, Q.; Xu, H.; Liu, L. The role of three-dimensional speckle tracking imaging in the diagnosis of immunoglobulin light-chain cardiac amyloidosis with normal leftventricul are jection fraction. Chin. J. Ultrason. 2020, 12, 213–218. [Google Scholar]
- Lei, C.; Zhu, X.; Hsi, D.H.; Wang, J.; Zuo, L.; Ta, S.; Yang, Q.; Xu, L.; Zhao, X.; Wang, Y.; et al. Predictors of cardiac involvement and survival in patients with primary systemic light-chain amyloidosis: Roles of the clinical, chemical, and 3-D speckle tracking echocardiography parameters. BMC Cardiovasc. Disord. 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Li, T.; Huang, X.H.; Chen, W.C.; Zhao, L.; Wang, Q.W.; Zeng, C.H.; Liang, D.D.; Liu, Z.H. The significant of skin fat and rectal mucosal biopsy in the diagnosis of systemic light chain amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2015, 24, 425–428+486. [Google Scholar]
- Li, R.; Yang, Z.-G.; Wen, L.-Y.; Liu, X.; Xu, H.-Y.; Zhang, Q.; Guo, Y.-K. Regional myocardial microvascular dysfunction in cardiac amyloid light-chain amyloidosis: Assessment with 3T cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2016, 18, 16. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Feng, J.; Cao, X.X.; Zhang, C.L.; Shen, K.N.; Huang, X.F.; Zhang, C.L.; Duan, M.H.; Zhang, W.; Zhu, T.N.; et al. Autologous peripheral blood hematopoietic stem cell transplantation for patients with primary light chain amyloidosis: Experience of 31 cases in a single center. Chin. J. Hematol. 2016, 37, 201–204. [Google Scholar]
- Li, T.; Huang, X.; Cheng, S.; Zhao, L.; Ren, G.; Chen, W.; Wang, Q.; Zeng, C.; Liu, Z. Utility of abdominal skin plus subcutaneous fat and rectal mucosal biopsy in the diagnosis of AL amyloidosis with renal involvement. PLoS ONE 2017, 12, e0185078. [Google Scholar] [CrossRef]
- Li, R.; Yang, Z.-G.; Xu, H.-Y.; Shi, K.; Liu, X.; Diao, K.-Y.; Guo, Y.-K. Myocardial Deformation in Cardiac Amyloid Light-chain Amyloidosis: Assessed with 3T Cardiovascular Magnetic Resonance Feature Tracking. Sci. Rep. 2017, 7, 3794. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Duan, X.J.; Sun, Y.; Lu, Y.; Xu, H.Y.; Wang, Q.Z.; Wang, H.Y. Classification of cardiac amyloidosis: An immunohistochemical analysis. Chin. J. Pathol. 2018, 47, 105–109. [Google Scholar]
- Li, T.; Huang, X.; Wang, Q.; Zhao, L.; Ren, G.; Chen, W.; Zheng, C.; Zhou, M.; Jiang, Q.; Yin, R.; et al. A risk stratification for systemic immunoglobulin light-chain amyloidosis with renal involvement. Br. J. Haematol. 2019, 187, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, J.; Lin, L.; Shen, K.; Tian, Z.; Sun, J.; Zhang, C.; An, J.; Jin, Z.; Vliegenthart, R.; et al. Left and right ventricular myocardial deformation and late gadolinium enhancement: Incremental prognostic value in amyloid light-chain amyloidosis. Cardiovasc. Diagn. Ther. 2020, 10, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Li, D.Y.; Liu, D.; Wang, S.X.; Zhao, M.H. Associations between the immunoglobulin germline gene usage and the tropism of organ involvement and renal amyloid deposition patterns in immunoglobulin light-chain amyloidosis by mass spectrometry. J. Am. Soc. Nephrol. 2020, 31, 9–10. [Google Scholar]
- Li, H.; Wang, Y.; Lan, P.; Xie, L.; Zhao, Y.; Lu, W.; Li, G. Electrocardiographic parameters and prognosis of renal light chain amyloidosis. Clin. Cardiol. 2020, 43, 1160–1166. [Google Scholar] [CrossRef]
- Lin, Y.C. Analysis of clinical characteristics of 10 patients with amyloidosis. Guide China Med. 2014, 12, 110–111. [Google Scholar]
- Lin, L.; Li, X.; Feng, J.; Shen, K.-N.; Tian, Z.; Sun, J.; Mao, Y.-Y.; Cao, J.; Jin, Z.-Y.; Li, J.; et al. The prognostic value of T1 mapping and late gadolinium enhancement cardiovascular magnetic resonance imaging in patients with light chain amyloidosis. J. Cardiovasc. Magn. Reson. 2018, 20, 1–11. [Google Scholar] [CrossRef]
- Liu, D.; Liu, G. Analysis of Clinical Characteristics in 20 Patients with AL Amyloidosis. J. Cap. Med. Univ. 2010, 31, 416–419. [Google Scholar]
- Liu, B.; Wang, Y.; Bai, M.; Wang, D.; Zhang, M.; Zhao, J.; Shiren, S. Cyclophosphamide + Thalidomide + Dexamethasone Versus Melphalan + Dexamethasone for the Treatment of Amyloid Light-chain Amyloidosis with Kidney Involvement: A Retrospective Study in Chinese Patients. Clin. Ther. 2019, 41, 1186–1198. [Google Scholar] [CrossRef]
- Liu, Y.X.; Lian, H.; Li, J.; Shen, K.N.; Chen, W.; Lin, X.; Fang, L.G. Single-center experience of diagnosis and strategy in patients with cardiac amyloidosis and cerebral infarction. Chin. J. Interv. Cardiol. 2019, 27, 567–573. [Google Scholar]
- Liu, Y.; Wen, L.; Ma, L.; Kang, Y.; Liu, K.; Huang, X.; Ruan, G.; Lu, J. MAGE genes: Prognostic indicators in AL amyloidosis patients. J. Cell. Mol. Med. 2019, 23, 5672–5678. [Google Scholar] [CrossRef]
- Liu, H.; Fu, H.; Guo, Y.-K.; Yang, Z.-G.; Xu, H.-Y.; Shuai, X.; Xu, R.; Li, Z.-L.; Xia, C.-C.; He, Y.; et al. The prognostic value of right ventricular deformation derived from cardiac magnetic resonance tissue tracking for all-cause mortality in light-chain amyloidosis patients. Cardiovasc. Diagn. Ther. 2020, 10, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Liu, B.; Wang, Y.; Bai, M. P0268A Comparative Study of Cyclophosphamide, Thalidomide and Dexamethasone (CTD) versus Bortezomib and Dexamethasone (BDEX) in Al Amyloidosis: A Real-Word Study in Chinese Patients. Nephrol. Dial. Transplant. 2020, 35. [Google Scholar] [CrossRef]
- Liu, Y.; Lai, Y.; Ma, L.; Wen, L.; Duan, W.; Wang, F.; Kang, Y.; Chen, H.; Chen, Y.; Gao, L.; et al. Fluorescence in situ hybridisation combined with CD138 immunomagnetic sorting is effective to identify cytogenetic abnormalities which play significant prognostic roles in Chinese AL amyloidosis patients. Amyloid 2020, 27, 208–209. [Google Scholar] [CrossRef]
- Lu, J.; Wang, H.; Huang, X.J. Curative effect observation of patients with primary systemic amyloidosis treated by the combin ation of bortezomib with dexmethasone and cyclophosphamide. Chin. J. Hematol. 2013, 345–348. [Google Scholar]
- Mao, X.X.; Zhao, D.C.; Fang, Q.; Tian, Z.; Cheng, Z.W.; Cui, Q.C. Clinicopathological Features of Cardiac Amyloidosis. Med. J. Peking Union Med. Coll. Hosp. 2012, 3, 89–94. [Google Scholar]
- Mao, Y.Y.; Feng, J.; Meng Qi Shen, K.N.; Cao, X.X.; Zhou, D.B.; Li, J. Clinical characteristics and prognostic analysis of monoclonal IgM- related AL amy-loidosis. Chin. J. Hematol. 2017, 38, 989–992. [Google Scholar]
- Mei, J.G.; Shao, L.J.; Cao, H.Q.; Li, H.Q.; Cui, Y.P. Detection and analysis of cytogenetic abnormalities in systemic AL amyloidosis. Lab. Med. Clin. 2016, 13, 3463–3466. [Google Scholar]
- Mu, X.-D.; Xiong, Y.; Chen, J.; Zhang, W.; Qiu, Z.-X.; Hu, Y.; Liu, Y.; Cong, T.-C.; Gao, L.; Ren, Y.-L.; et al. Retrospective analysis of 11 cases of respiratory amyloidosis. Chin. J. Tuberc. Respir. Dis. 2013, 36. [Google Scholar]
- Ni, J.; Yu, D.R.; Zhu, B.; Chen, H.Y. Clinical analysis of 44 cases of renal amyloidosis. Chin. J. Integr. Tradit. West. Nephrol. 2014, 15, 39–40. [Google Scholar]
- Qiu, Y.; Zhang, C.L.; Shen, K.N.; Su, W.; Feng, J.; Zhang, L.; Cao, X.X.; Li, J. Clinical presentation and prognosis of light-chain amyloidosis patients with un-measurable free light-chain levels. Ann. Hematol. 2018, 97, 2465–2470. [Google Scholar] [CrossRef]
- Ren, L.; Liu, H.; Xu, X.H.; Jiang, S.H.; Fang, Y.; Ding, X.Q. Clinicopathology, diagnosis and classification of renal amyloidosis. Chin. J. Nephrol. 2011, 10, 730–734. [Google Scholar]
- Ren, H.Q.; Lv, Y.M.; Cai, Q.; Li, Y.; Han, S.J.; Wang, R.; Hao, X.K. Clinicopathological analysis of 10 cases of renal amyloidosis. Mil. Med. J. Southeast China 2011, 13, 348–349. [Google Scholar]
- Ren, C.; Ren, J.; Tian, Z.; Du, Y.; Hao, Z.; Zhang, Z.; Fang, W.; Li, F.; Zhang, S.; Hsu, B.; et al. Assessment of cardiac amyloidosis with 99mTc-pyrophosphate (PYP) quantitative SPECT. EJNMMI Phys. 2021, 8, 348–349. [Google Scholar] [CrossRef]
- Rui, H.C.; Lv, Y.N.; Yang, F.; Fan, Y.; Li, X.M.; Xu, F.; Cheng, S.Q.; Liang, S.S.; Huang, X.H.; Liu, Z.H.; et al. Clinicopathologic features and outcomes of light-chain amyloidosis(AL)patients based on digital whole slide imaging. Chin. J. Nephrol. Dial. Transplant. 2017, 26, 113–118. [Google Scholar]
- Sa, Q.; Ren, G.S.; Xu, X.D. Plasma cell characteristics in patients with systemic light chain amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2019, 28, 401–406. [Google Scholar]
- Sa, Q.; Ren, G.S.; Xu, X.D.; Xu, X.; Chen, W.; Guo, J.; Zhao, L.; Liu, Z.; Huang, X. Genetic characteristics of bone marrow plasma cells in 102 patients with systemic light chain amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2020, 29, 413–419. [Google Scholar]
- Shen, K.-N.; Feng, J.; Huang, X.-F.; Zhang, C.-L.; Zhang, C.-L.; Cao, X.-X.; Zhang, L.; Zhou, D.-B.; Li, J. At least partial hematological response after first cycle of treatment predicts organ response and long-term survival for patients with AL amyloidosis receiving bortezomib-based treatment. Ann. Hematol. 2017, 96, 2089–2094. [Google Scholar] [CrossRef]
- Shen, K.; Dong, Y.; Fu, W.; Wu, Y.; Huang, Z.; Wei, Y.; Li, C.; Sun, C.; Huang, W.; Wang, H.; et al. Doxycycline Combined with Bortezomib-Cyclophosphamide-Dexamethasone Chemotherapy for Newly Diagnosed Patients with Mayo 2004 Stage II-III Light-Chain Amyloidosis: A Randomized Controlled Multicenter Study. Blood 2019, 134, 1870. [Google Scholar] [CrossRef]
- Shen, K.-N.; Zhang, C.-L.; Tian, Z.; Feng, J.; Wang, Y.-N.; Sun, J.; Zhang, L.; Cao, X.-X.; Zhou, D.-B.; Li, J. Bortezomib-based chemotherapy reduces early mortality and improves outcomes in patients with ultra-high-risk light-chain amyloidosis: A retrospective case control study. Amyloid 2019, 26, 66–73. [Google Scholar] [CrossRef]
- Shen, K.-N.; Miao, H.-L.; Zhang, C.-L.; Feng, J.; Zhang, L.; Cao, X.-X.; Zhou, D.-B.; Wei, S.; Li, J. Posttreatment dFLC less than 10 mg/L predicts superior organ response and longer time to next treatment in newly diagnosed light-chain amyloidosis patients treated with bortezomib. Leuk. Lymphoma 2020, 62, 874–882. [Google Scholar] [CrossRef]
- Sui, Y.X.; Jiang, N.; Xie, L.Y.; Zhao, D. Amyloid nephropathy: A clinicopathologic analysis of 31 cases. Chin. J. Clin. Exp. Pathol. 2014, 30, 1379–1382. [Google Scholar]
- Wan, K.; Sun, J.; Han, Y.; Liu, H.; Yang, D.; Li, W.; Wang, J.; Cheng, W.; Zhang, Q.; Zeng, Z.; et al. Increased Prognostic Value of Query Amyloid Late Enhancement Score in Light-Chain Cardiac Amyloidosis. Circ. J. 2018, 82, 739–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, K.; Sun, J.; Han, Y.; Luo, Y.; Liu, H.; Yang, D.; Cheng, W.; Zhang, Q.; Zeng, Z.; Chen, Y. Right ventricular involvement evaluated by cardiac magnetic resonance imaging predicts mortality in patients with light chain amyloidosis. Hear. Vessel. 2017, 33, 170–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, K.; Sun, J.; Yang, D.; Liu, H.; Wang, J.; Cheng, W.; Zhang, Q.; Zeng, Z.; Zhang, T.; Greiser, A.; et al. Left Ventricular Myocardial Deformation on Cine MR Images: Relationship to Severity of Disease and Prognosis in Light-Chain Amyloidosis. Radiology 2018, 288, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Wan, K.; Li, W.; Sun, J.; Xu, Y.; Wang, J.; Liu, H.; Dong, Y.; Cheng, W.; Zhang, Q.; Zeng, Z.; et al. Regional amyloid distribution and impact on mortality in light-chain amyloidosis: A T1 mapping cardiac magnetic resonance study. Amyloid 2019, 26, 45–51. [Google Scholar] [CrossRef]
- Wan, K.; Lin, J.Y.; Guo, X.L.; Song, R.Z.; Wang, J.; Xu, Y.W.; Li, W.H.; Cheng, W.; Sun, J.Y.; Zhang, Q.; et al. Prognostic Value of Right Ventricular Dysfunction in Patients with AL Amyloidosis: Com-parison of Different Techniques by Cardiac Magnetic Resonance. J. Magn. Reson. Imaging 2020, 52, 1441–1448. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H.; Chen, W.F.; Tong, X.Z.; Yan, M.S.; Xu, D.R.; Li, J. Clinical features and survival analys is of light-chain amyloidosis associated renal disease. Chin. J. Postgrad. Med. 2010, 33, 7–10. [Google Scholar]
- Wang, X.X.; Dong, K.; Sun, L.; Song, C.Z.; Lv, F.D. Clinical pathological characteristics of fight chain deposition disease and light chain amyloidosis in liver. Beijing Med. J. 2016, 38, 877–879. [Google Scholar]
- Wang, J.; Yang, F.; Zuo, L.; Lei, C.; Sheng, J.; Sun, C.; Liu, L. P5843Investigation of left ventricular function and biomarkers following treatment in patients with light-chain cardiac amyloidosis. Eur. Hear. J. 2017, 38. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Zhao, H.Y.; Tan, J.B.; Li, Y.J.; Zhang, S.S.; Tian, W.L.; Xie, X.S.; Cao, W.J.; Sun, L.; Yang, Y.L.; et al. The value of urine Bence Jones protein and complement C3 in differential diagnosis of nenal amyloidos is and nephrotic syndrome. Int. J. Transplant. Hemopurif. 2019, 17, 19–22. [Google Scholar]
- Wang, L.M.; Tian, Y.; Zhao, L.; Yang, X. Clinical Analysis of Immunoglobulin Amyloid Light-chain Cardiac Amyloidosis. Chin. Gen. Pract. 2020, 23, 3474–3478. [Google Scholar]
- Wang, Y.; Xu, L.; Liu, Y.; Hu, Y.; Shi, Q.; Jin, L.; Yang, L.; Wang, P.; Zhang, K.; Huang, X.; et al. Transcriptional heterogeneity of clonal plasma cells and immune evasion in immunoglobulin light chain amyloidosis. Int. J. Hematol. 2020, 113, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.M.; Wang, T.T.; Tian, Y.; Zhao, L.; Yang, X.C.; Chen, W.M. The prognostic value of baseline serum free light chain in immunoglobulin light- chain cardiac amyloidosis. Chin. J. Hematol. 2020, 01, 47–53. [Google Scholar]
- Wei, W.; Zhou, F.; Shi, H.T.; Li, L.; Hou, J. Clinical features of multiple myleloma-associated amyloidosis: A report of 33 cases. J. Clin. Hematol. 2015, 28, 584–588. [Google Scholar]
- Wei, Y.; Chen, D.D.; Tang, P.; Xie, X.S. Comparison of efficacy and safety of VTD regimen and CTD regimen in the treatment of primary systemic amyloidosis. J. Basic Clin. Oncol. 2020, 33, 191–195. [Google Scholar]
- Wu, X.; Miao, H.-L.; Zhu, T.-N.; Feng, J.; Zhang, L.; Mao, Y.-Y.; Zhou, D.-B.; Cao, X.-X.; Li, J. Bortezomib-based treatment can improve factor X activity in immunoglobulin light-chain amyloidosis with factor X deficiency. Amyloid 2019, 26, 255–256. [Google Scholar] [CrossRef]
- Xiao, H.B.; Liu, R.H.; Yuan, S.G.; Ling, G.H.; Xia, Y.C.; Xu, X.Q.; Wang, J.; Bi, H.X.; Chen, N.L. Analysis of clinical and pathological characteristics of 20 patients with renal amyloidosis. Int. J. Pathol. Clin. Med. 2010, 30, 43–47. [Google Scholar]
- Xu, T.H.; Wei, Z.; Chen, C.; Shen, Y.Q.; Ge, X.F.; Liu, P. The value of abdominal fat aspiration and labial salivary gland biopsy in diagnosing immunoglobulin light chain amyloidosis. Chin. J. Clin. Med. 2019, 26, 37–42. [Google Scholar]
- Yang, Y.G. Clinical Study of Elder and Elder Early Renal Amyloidosis and Skin Amyloidosis. China Contin. Med. Educ. 2015, 7, 78–79. [Google Scholar]
- Yang, J.; Shi, H.; Xu, J.; Li, X.; Shen, P.Y.; Wang, C.H. Clinicopathological analysis of 33 cases of primary renal amyloidosis. Mod. Pract. Med. 2016, 28, 998–999. [Google Scholar]
- Yang, F.; Liu, L.W.; Wang, J.; Zhang, M.; Zuo, L.; Lei, C.; Ta, S. Investigation of left ventricular function and biomarkers following chemotherapy in pa-tients with light-chain cardiac amyloidosis. Chin. J. Ultrason. 2017, 26, 928–933. [Google Scholar]
- Yang, T.; Wan, K.; Song, R.; Guo, X.; Xu, Y.; Wang, J.; Zhang, Q.; Alexander, K.M.; Liao, R.; Chen, Y. Serum high-density lipoprotein cholesterol serves as a prognostic marker for light-chain cardiac amyloidosis. Int. J. Cardiol. 2020, 325, 96–102. [Google Scholar] [CrossRef]
- Yao, Y.; Wang, S.X.W.; Zhang, Y.K.; Liu, G.; Qu, Z.; Zou, W.Z. lmmunohistochemical classification of amyioid in kidney biopsy and clinical characteristics of renal amyloidosis in Chinese patients. Beijing Med. J. 2012, 34, 267–270. [Google Scholar]
- Yao, Y.; Wang, S.X.W.; Zhang, Y.K.; Qu, Z.; Liu, G.; Zou, W.Z. Clinicopathological correlation analysis of AL renal amyloidosis. Chin. J. Nephrol. 2013, 29, 216–218. [Google Scholar]
- Yao, Y.; Wang, S.X.W.; Zhang, Y.K.; Qu, Z.; Liu, G.; Zou, W.Z. Associations between pathological features and clinical manifestations of immu-noglobulin light-chain renal amyloidosis. Chin. J. Clin. 2013, 7, 6344–6348. [Google Scholar]
- Yao, Y.; Wang, S.-X.; Zhang, Y.-K.; Qu, Z.; Liu, G.; Zou, W.-Z. A clinicopathological analysis in a large cohort of Chinese patients with renal amyloid light-chain amyloidosis. Nephrol. Dial. Transplant. 2012, 28, 689–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Huang, Z.; Hu, W.; Li, X.; Shen, M.; Zhang, J.; Tang, R.; Chen, S.; Chen, W. Clinical Analysis of Cardiac Involvement in 53 Patients with Multiple Myeloma Coexistent with Light Chain Amyloidosis. Clin. Lymphoma Myeloma Leuk. 2020, 20, 519–525.e1. [Google Scholar] [CrossRef] [Green Version]
- Yuan, X.F.; Liu, L.L. Study on the characteristics of cardiac echocardiography and electrocardiogram of cardiac amyloidosis. Chin. J. Mod. Drug Appl. 2015, 9, 34–35. [Google Scholar]
- Yuan, F.F.; Jiang, Y. Clinicopathological characteristics of renal amyloidosis and its relationship with TCM syndromes. Chin. J. Integr. Tradit. West. Nephrol. 2019, 20, 408–410. [Google Scholar]
- Zhai, Y.-P.; Liu, H.-N.; Yu, Y.-P.; Zhou, X.-G.; Song, P.; Li, F.; Wang, X.-W. Treatment of primary systemic amyloidosis with the combination of bortezomib and dexamethasone. Zhonghua Xue Ye Xue Za Zhi 2010, 31, 319–322. [Google Scholar]
- Zhai, Y.-P.; Song, P.; Li, F.; Liu, H.-N.; Yu, Y.-P.; Shi, P.; An, Z.-M.; Zhou, X.; Zhang, C.-N. The clinical significance of serum free light chain in primary systemic amyloidosis. Zhonghua nei ke za zhi 2011, 50, 404–407. [Google Scholar] [PubMed]
- Zhang, J.F.; Sun, J.; Wu, M.; Liu, S.J.; Lou, Y.; Wang, Y.W. Clinicopathological study of renal amyloidosis. Chin. J. Lab. Diagn. 2012, 16, 131–133. [Google Scholar]
- Zhang, L.; Wang, Y.; Cheng, L.; Cheng, L.; Wang, J.; Zhou, X.; Liu, M.; Zhang, W.; Zhang, M.; Zhang, B.; et al. Value of assessing left ventricular longitudinal systolic peak strain in differential di-agnosis of primary cardiac amyloidosis from hypertrophic cardiomyopathy. J. South. Med. Univ. 2014, 34, 609–616. [Google Scholar]
- Zhang, L.; Wang, Y.; Cheng, L.Q.; Wang, J.; Zhou, X.; Liu, M.; Zhang, B.; Chen, Y.D.; Zhi, G. The characters of myocardial mechanics in Chinese patients with primary cardiac amyloidosis and hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2014, 64, C197. [Google Scholar]
- Zhang, C.L.; Feng, J.; Shen, K.N.; Su, W.; Zhang, C.L.; Huang, X.F.; Cao, X.X.; Zhang, L.; Zhou, D.B.; Li, J. The diagnostic and prognostic values of serum free light chain in patients with primary light chain amyloidosis. Chin. J. Hematol. 2016, 37, 942–945. [Google Scholar]
- Zhang, L.; Zhou, X.; Wang, J.; Mu, Y.; Liu, B.; Lv, W.; Wang, Y.; Liu, H.; Liu, H.; Zhi, G. Differentiation of light-chain cardiac amyloidosis from hypertrophic cardiomyopathy using myocardial mechanical parameters by velocity vector imaging echocardiography. Int. J. Cardiovasc. Imaging 2016, 33, 499–507. [Google Scholar] [CrossRef]
- Zhang, C.L.; Shen, K.N.; Feng, J.; Cao, X.X.; Mao, Y.Y.; Zhang, L.; Su, W.; Zhou, D.B.; Li, J. Oral melphalan plus high-dose dexamethasone as first-line therapy for patients with primary light chain amyloidosis. Chin. J. Hematol. 2018, 39, 641–644. [Google Scholar]
- Zhang, L.-L.; Shen, K.-N.; Zhang, C.-L.; Qiu, Y.; Miao, H.-L.; Feng, J.; Cao, X.-X.; Zhang, L.; Zhou, D.-B.; Li, J. Clinical presentation and prognostic analysis of Chinese patients with systemic light chain amyloidosis with liver involvement. Leuk. Res. 2019, 86, 106226. [Google Scholar] [CrossRef]
- Zhang, C.-L.; Qiu, Y.; Shen, K.-N.; Miao, H.-L.; Feng, J.; Cao, X.-X.; Zhang, L.; Jiang, X.-Y.; Zhou, D.-B.; Li, J. Clinical presentation and prognosis of immunoglobulin light-chain amyloidosis with high percentage of bone marrow plasma cells. Leuk. Res. 2019, 81, 19–24. [Google Scholar] [CrossRef]
- Zhang, B.; Sun, W.; Zhou, L.; Chen, L. Individualized Nursing Care of 13 Cases of Multiple Myeloma Accompanied by Light Chain Amyloidosis. Chin. J. Rural. Med. Pharm. 2020, 27, 70–71. [Google Scholar]
- Zhang, F.; Yu, X.J.; Wang, S.X.; Qu, L.; Ma, Y.Y.; Liu, G.; Yang, L. A Comparison of Immunopathological Methods in the Classification of Light Chain Renal Amyloidosis. Labeled Immunoass. Clin. Med. 2020, 27, 818–822. [Google Scholar]
- Zhao, Q.; Li, F.; Song, P.; Zhou, X.; Wang, L.; Yu, Y.; An, Z.; Wang, X.; Zhai, Y. Clinical Characteristics and Treatment Outcome of Chinese Patients with Systemic Amyloid Light-Chain Amyloidosis: A Retrospective Single-Center Analysis. Clin. Lymphoma Myeloma Leuk. 2015, 16, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Tian, Z.; Fang, Q. The prognostic value of baseline serum free light chain in cardiac amyloidosis. Zhonghua nei ke za zhi 2016, 55, 186–190. [Google Scholar] [PubMed]
- Zhao, L.; Tian, Z.; Fang, Q. Risk Factors and Prognostic Role of Left Atrial Enlargement in Patients with Cardiac Light-Chain Amyloidosis. Am. J. Med Sci. 2016, 351, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Li, J.; Tian, Z.; Fang, Q. Clinical correlates and prognostic values of pseudoinfarction in cardiac light-chain amyloidosis. J. Cardiol. 2016, 68, 426–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.; Zhuang, T.; Quan, F. Cardiac amyloidosis with normal interventricular septal thickness: A great pretender. J. Am. Coll. Cardiol. 2016, 68, C157. [Google Scholar]
- Zhao, L.; Huang, X.H.; Li, T. Efficiency and safety of thalidomide combined with dexamethasone in patients with primary systemic amyloidosis. J. Nephrol. Dialy Transplant. 2016, 25, 409–414. [Google Scholar]
- Zhao, Q.; Wang, L.P.; Song, P.; Li, F.; Zhou, X.; Yu, Y.; An, Z.; Wang, X.; Zhai, Y. Comparison analysis of outcomes in primary light chain amyloidosis patients treated by auto peripheral blood stem cell transplantation or bortezomib plus dexamethasone. Chin. J. Hematol. 2016, 37, 283–287. [Google Scholar]
- Zhao, L.; Ren, G.S.; Guo, J.Z. Clinical manifestation and prognosis of liver systemic light chain amyloidosis. Chin. J. Nephrol. Dial. Transplant. 2019, 28, 318–323. [Google Scholar]
- Zhou, F.-D.; Zhang, L.-X.; Yao, Y.; Wang, S.-X.; Zou, W.-Z.; Liu, G.; Chen, M.; Zhao, M.-H. Immunofixation Electrophoresis Was Highly Specific for the Diagnosis of Renal Light-Chain Amyloidosis. Am. J. Med Sci. 2013, 345, 18–21. [Google Scholar] [CrossRef]
- Zhu, Z.; Yue, C.; Sun, Y.; Li, X.; Li, M. Light-chain amyloidosis with renal involvement: Renal outcomes and validation of two renal staging systems in the Chinese population. Amyloid 2019, 26, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Zampieri, M.; Cappelli, F.; Allinovi, M.; Olivotto, I.; Antonioli, E.; Tassetti, L.; Zocchi, C.; Andrei, V.; Di Mario, C.; Nozzoli, C.; et al. Incidence of light chain amyloidosis in Florence metropolitan area, Italy: A population-based study. Amyloid 2021, 28, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, C. Current diagnosis and treatment of AL amyloidosis in Japan: A nationwide epidemiological survey. J. Comp. Eff. Res. 2019, 60, 973–978. [Google Scholar]
- Jun, H.J.; Kim, K.; Kim, S.J.; Mun, Y.-C.; Bang, S.-M.; Won, J.-H.; Kim, C.S.; Lee, J.H.; Korean Multiple Myeloma Working Party (KMMWP). Clinical features and treatment outcome of primary systemic light-chain amyloidosis in Korea: Results of multicenter analysis. Am. J. Hematol. 2012, 88, 52–55. [Google Scholar] [CrossRef]
- Quock, T.P.; Yan, T.; Chang, E.; Guthrie, S.; Broder, M.S. Healthcare resource utilization and costs in amyloid light-chain amyloidosis: A real-world study using US claims data. J. Comp. Eff. Res. 2018, 7, 549–559. [Google Scholar] [CrossRef]
- Lousada, I.; Comenzo, R.L.; Landau, H.; Guthrie, S.; Merlini, G. Light Chain Amyloidosis: Patient Experience Survey from the Amyloidosis Research Consortium. Adv. Ther. 2015, 32, 920–928. [Google Scholar] [CrossRef] [Green Version]
- Hwa, Y.L.; Fogaren, T.; Sams, A.; Faller, D.V.; Stull, D.M.; Thuenemann, S.; Mendelson, L. Immunoglobulin Light-Chain Amyloidosis: Clinical Presentations and Diagnostic Approach. J. Adv. Pract. Oncol. 2019, 10, 470–481. [Google Scholar]
- Bianchi, G.; Zhang, Y.; Comenzo, R.L. AL Amyloidosis: Current Chemotherapy and Immune Therapy Treatment Strategies: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncology 2021, 3, 467–487. [Google Scholar] [CrossRef]
- Hong, L.Z. Guidelines for the diagnosis and treatment of systemic light chain amyloidosis (revised in 2021). Natl. Med. J. China 2021, 101, 1646–1656. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Toal Number (n) | Positive Number (n) | Percentage (%) |
|---|---|---|---|
| Type of light chains | |||
| Lambda | 3610 | 2890 | 80.0 |
| Kappa | 508 | 14.1 | |
| Unclear * | 212 | 5.9 | |
| Disease course | |||
| Newly diagnosed | 2020 | 2010 | 99.5 |
| Relapsed/Refractory | 10 | 0.5 | |
| Mayo 2004 cardiac staging system | |||
| I | 1559 | 383 | 24.6 |
| II | 535 | 34.3 | |
| III | 641 | 41.1 | |
| Mayo 2012 cardiac staging system | |||
| I | 1585 | 532 | 33.6 |
| II | 391 | 24.7 | |
| III | 399 | 25.2 | |
| IV | 263 | 16.6 | |
| NYHA functional class | |||
| I–II | 929 | 638 | 68.7 |
| III–IV | 291 | 31.3 | |
| Organ involvement | |||
| Renal | 3798 | 3202 | 84.3 |
| Cardiac | 4070 | 2542 | 62.5 |
| Soft tissue | 807 | 335 | 41.5 |
| Gastrointestinal tract | 2174 | 747 | 34.4 |
| Liver | 3190 | 578 | 18.1 |
| Nerves | 2381 | 268 | 11.3 |
| Renal | 3798 | 3202 | 84.3 |
| Number of involved organs | |||
| 1 | 382 | 79 | 20.7 |
| 2 | 122 | 31.9 | |
| 3 | 121 | 31.7 | |
| ≥4 | 60 | 15.7 | |
| dFLC (median, mg/L) | |||
| 19.1–250.3 | 2044 | ||
| <50 | 312 | 15.3 | |
| ≥50 | 1732 | 84.7 | |
| <180 | 1404 | 68.7 | |
| ≥180 | 640 | 31.3 | |
| NT-proBNP (median, ng/L) | |||
| 222–14,213 | 2928 | ||
| <332 | 512 | 17.5 | |
| ≥332 | 2416 | 82.5 | |
| <1800 | 1392 | 47.5 | |
| ≥1800 | 1536 | 52.5 | |
| TNT (median, μg/L) | |||
| 0.016–0.21 | 1545 | ||
| <0.035 | 1038 | 67.2 | |
| ≥0.035 | 507 | 32.8 | |
| eGFR (median, mL/min/1.73 m2) | |||
| 70–115.3 | 1259 | ||
| <50 | 764 ‡ | 140 | 18.4 |
| ≥50 | 624 | 81.6 | |
| 24 h urine protein (median, g/24 h) | |||
| 0.9–6.64 | 2423 | ||
| <5 | 2140 | 83.3 | |
| ≥5 | 283 | 11.7 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, C.; Wang, X.; Cao, X.; Xu, L.; Liu, W.; Pi, J.; Wang, B.; Chen, W. The Clinical Characteristics of Immunoglobulin Light Chain Amyloidosis in the Chinese Population: A Systematic Scoping Review. Hemato 2023, 4, 12-25. https://doi.org/10.3390/hemato4010002
Fu C, Wang X, Cao X, Xu L, Liu W, Pi J, Wang B, Chen W. The Clinical Characteristics of Immunoglobulin Light Chain Amyloidosis in the Chinese Population: A Systematic Scoping Review. Hemato. 2023; 4(1):12-25. https://doi.org/10.3390/hemato4010002
Chicago/Turabian StyleFu, Chengcheng, Xiaohong Wang, Xian Cao, Lingjie Xu, Wang Liu, Jingnan Pi, Bin Wang, and Wenming Chen. 2023. "The Clinical Characteristics of Immunoglobulin Light Chain Amyloidosis in the Chinese Population: A Systematic Scoping Review" Hemato 4, no. 1: 12-25. https://doi.org/10.3390/hemato4010002