


Development of the Follow-Up Human 3D Oral Cancer Model in Cancer Treatment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Cell Culture
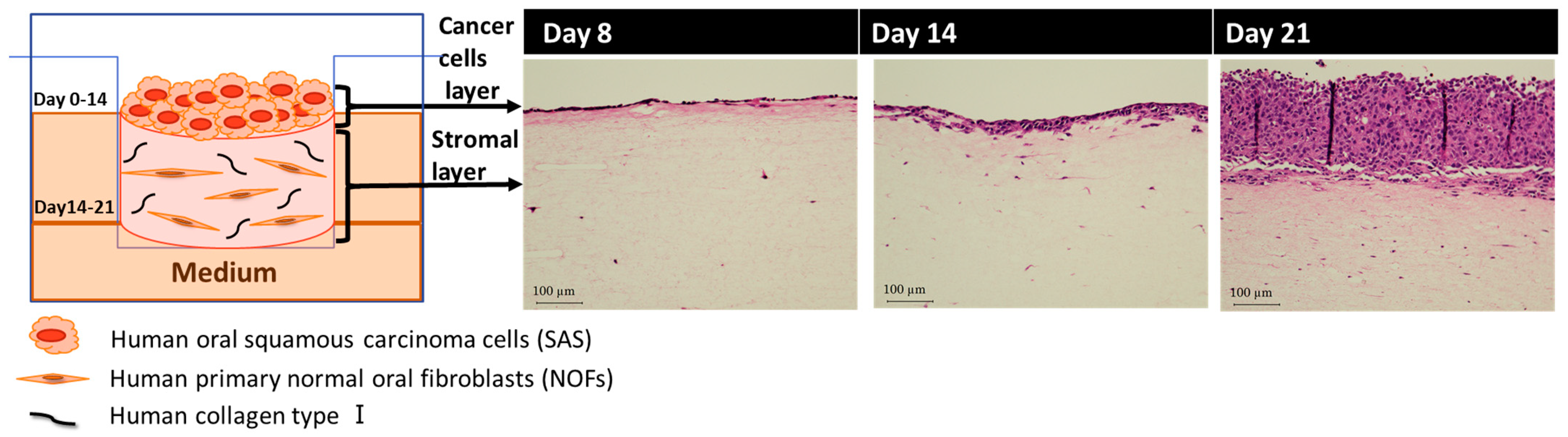
2.2. Fabrication of Human 3D Oral Cancer Model
2.3. Treatment Planning of BNCT for 3D Oral Cancer Model
2.4. BNCT for 3D Oral Cancer Model
2.5. Histological Analysis
2.6. Statistical Analysis
3. Results
3.1. Fabrication of Human 3D Oral Cancer Model
3.2. Treatment Planning of BNCT for 3D Oral Cancer Model
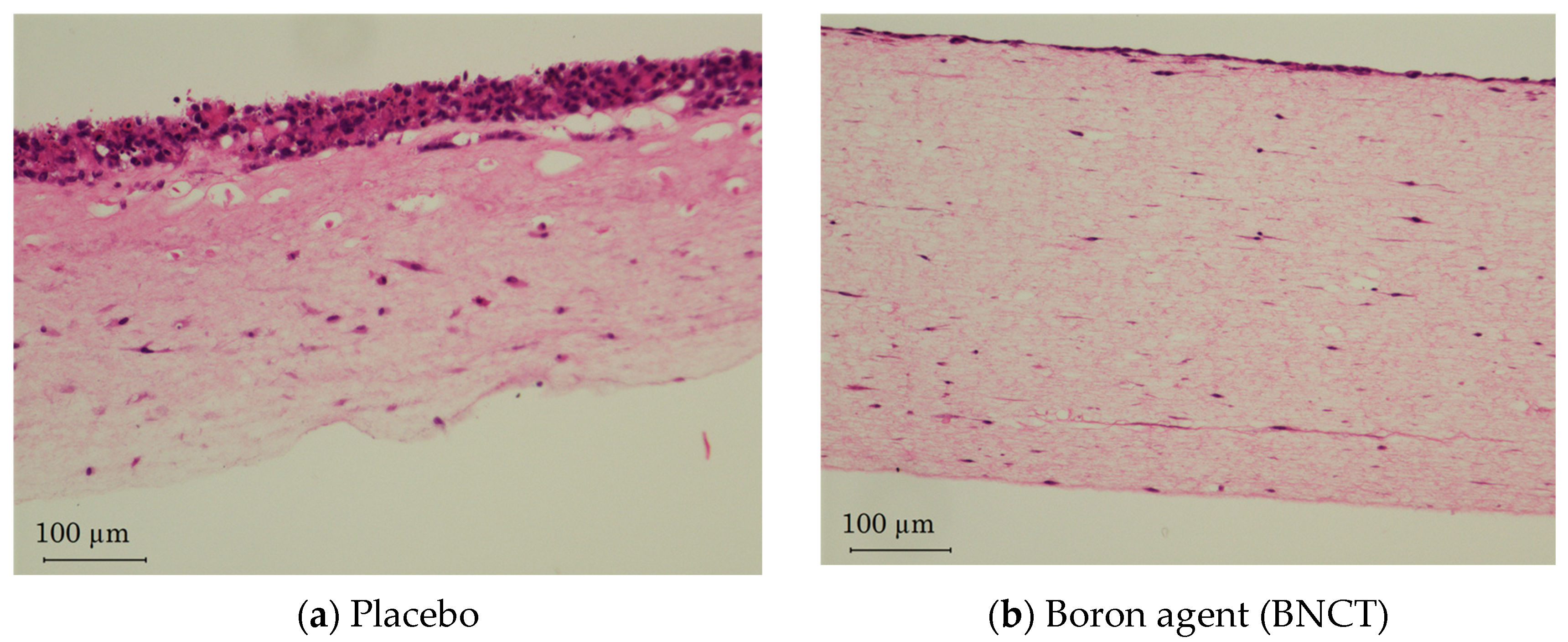
3.3. Evaluation of BNCT for 3D Oral Cancer Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chandra, R.A.; Keane, F.K.; Voncken, F.E.M.; Thomas, C.R., Jr. Contemporary radiotherapy: Present and future. Lancet 2021, 398, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Wakiyama, H.; Furusawa, A.; Choyke, P.L.; Kobayashi, H. Near Infrared Photoimmunotherapy; A Review of Targets for Cancer Therapy. Cancers 2021, 13, 2535. [Google Scholar] [CrossRef] [PubMed]
- Malouff, T.D.; Seneviratne, D.S.; Ebner, D.K.; Stross, W.C.; Waddle, M.R.; Trifiletti, D.M.; Krishnan, S. Boron Neutron Capture Therapy: A Review of Clinical Applications. Front. Oncol. 2021, 11, 601820. [Google Scholar] [CrossRef] [PubMed]
- Van Norman, G.A. Limitations of Animal Studies for Predicting Toxicity in Clinical Trials. J. Am. Coll. Cardiol. Basic Trans. Sci. 2019, 4, 845–854. [Google Scholar] [CrossRef]
- Zhao, Z.; Chen, X.; Dowbaj, A.M.; Sljukic, A.; Bratlie, K.; Lin, L.; Fong, E.L.S.; Balachander, G.M.; Chen, Z.; Soragni, A.; et al. Organoids. Nat. Rev. Methods Prim. 2022, 2, 94. [Google Scholar] [CrossRef]
- Atat, O.E.; Farzaneh, Z.; Pourhamzeh, M.; Taki, F.; Abi-Habib, R.; Vosough, M.; El-Sibai, M. 3D modeling in cancer studies. Hum. Cell 2022, 35, 23–36. [Google Scholar] [CrossRef]
- LeSavage, B.L.; Suhar, R.A.; Broguiere, N.; Lutolf, M.P.; Heilshorn, S.C. Next-generation cancer organoids. Nat. Mater. 2022, 21, 143–159. [Google Scholar] [CrossRef]
- Jensen, C.; Teng, Y. Is It Time to Start Transitioning From 2D to 3D Cell Culture? Front. Mol. Biosci. 2020, 7, 33. [Google Scholar] [CrossRef]
- OECD. Guidance Document on Good In Vitro Method Practices (GIVIMP); OECD Series on Testing and Assessment, No. 286; OECD Publishing: Paris, France, 2018. [Google Scholar] [CrossRef]
- Wishart, G.; Gupta, P.; Schettino, G.; Nisbet, A.; Velliou, E. 3d tissue models as tools for radiotherapy screening for pancreatic cancer. Br. J. Radiol. 2021, 94, 20201397. [Google Scholar] [CrossRef]
- Bessho, T.; Takagi, T.; Igawa, K.; Sato, K. Gelatin-based cell culture device for construction and X-ray irradiation of a three-dimensional oral cancer model. Anal. Sci. 2023. [Google Scholar] [CrossRef]
- Haga, K.; Yamazaki, M.; Maruyama, S.; Kawaharada, M.; Suzuki, A.; Hoshikawa, E.; Chan, N.N.; Funayama, A.; Mikami, T.; Kobayashi, T.; et al. Crosstalk between oral squamous cell carcinoma cells and cancer-associated fibroblasts via the TGF-β/SOX9 axis in cancer progression. Transl. Oncol. 2021, 14, 101236. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Igawa, K.; Ogawara, R.; Suda, M.; Hamano, T.; Ibaragi, S.; Hanafusa, T.; Ichikawa, Y.; Sasaki, A. The accelerator-based boron neutron capture reaction evaluation system for head and neck cancer. Appl. Radiat. Isot. 2020, 165, 109271. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, Y.; Kobayashi, T. Characteristics of the KUR Heavy Water Neutron Irradiation Facility as a neutron irradiation field with variable energy spectra. Nucl. Instr. Meth Res. Sect. A 2000, A453, 569–596. [Google Scholar] [CrossRef]
- Suzuki, M.; Kato, I.; Aihara, T.; Hiratsuka, J.; Yoshimura, K.; Niimi, M.; Kimura, Y.; Ariyoshi, Y.; Haginomori, S.; Sakurai, Y.; et al. Boron neutron capture therapy outcomes for advanced or recurrent head and neck cancer. J. Radiat. Res. 2014, 55, 146–153. [Google Scholar] [CrossRef]
- Coleman, C.N.; Blakely, W.F.; Fike, J.R.; MacVittie, T.J.; Metting, N.F.; Mitchell, J.B.; Moulder, J.E.; Preston, R.J.; Seed, T.M.; Stone, H.B.; et al. Molecular and cellular biology of moderate-dose (1–10 Gy) radiation and potential mechanisms of radiation protection: Report of a workshop at Bethesda, Maryland. Radiat. Res. 2003, 159, 812–833. [Google Scholar] [CrossRef] [PubMed]
- Jaschke, W.; Schmuth, M.; Trianni, A.; Bartal, G. Radiation-Induced Skin Injuries to Patients: What the Interventional Radiologist Needs to Know. Cardiovasc. Interv. Radiol. 2017, 40, 1131–1140. [Google Scholar] [CrossRef]
- Naidu, M.U.; Ramana, G.V.; Rani, P.U.; Mohan, I.K.; Suman, A.; Roy, P. Chemotherapy-induced and/or radiation therapy-induced oral mucositis—Complicating the treatment of cancer. Neoplasia 2004, 6, 423–431. [Google Scholar] [CrossRef]
- Report on the Deliberation Results. Available online: https://www.pmda.go.jp/files/000237993.pdf (accessed on 1 March 2020).
- eBioMedicine. The 3Rs of Animal Research. eBioMedicine 2022, 76, 103900. [Google Scholar]
- Suzuki, M. Boron neutron capture therapy (BNCT): A unique role in radiotherapy with a view to entering the accelerator-based BNCT era. Int. J. Clin. Oncol. 2020, 25, 43–50. [Google Scholar] [CrossRef]
- Hu, N.; Tanaka, H.; Kakino, R.; Yoshikawa, S.; Miyao, M.; Akita, K.; Isohashi, K.; Aihara, T.; Nihei, K.; Ono, K. Evaluation of a treatment planning system developed for clinical boron neutron capture therapy and validation against an independent Monte Carlo dose calculation system. Radiat. Oncol. 2021, 16, 243. [Google Scholar] [CrossRef]
- Takeno, S.; Tanaka, H.; Ono, K.; Mizowaki, T.; Suzuki, M. Analysis of boron neutron capture reaction sensitivity using Monte Carlo simulation and proposal of a new dosimetry index in boron neutron capture therapy. J. Radiat. Res. 2022, 63, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Sunavala-Dossabhoy, G.; Abreo, F.; Timiri Shanmugam, P.S.; Caldito, G. Histopathologic grading of oral mucositis. Oral Dis. 2015, 21, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Klausner, M.; Handa, Y.; Aizawa, S. In vitro three-dimensional organotypic culture models of the oral mucosa. In Vitro Cell. Dev. Biol. Anim. 2021, 57, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei, F.; Moharamzadeh, K.; Tayebi, L. Three-Dimensional In Vitro Oral Mucosa Models of Fungal and Bacterial Infections. Tissue Eng. Part B Rev. 2020, 26, 443–460. [Google Scholar] [CrossRef] [PubMed]
- Chitturi Suryaprakash, R.T.; Kujan, O.; Shearston, K.; Farah, C.S. Three-Dimensional Cell Culture Models to Investigate Oral Carcinogenesis: A Scoping Review. Int. J. Mol. Sci. 2020, 21, 9520. [Google Scholar] [CrossRef]
- Huang, J.; Hwang, A.Y.M.; Jia, Y.; Kim, B.; Iskandar, M.; Mohammed, A.I.; Cirillo, N. Experimental Chemotherapy-Induced Mucositis: A Scoping Review Guiding the Design of Suitable Preclinical Models. Int. J. Mol. Sci. 2022, 23, 15434. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Oral Cancer Model | Boron Concentration [ppm] | Thermal Neutron Fluence [cm−2] | * Total Dose [Gy-Eq] |
|---|---|---|---|
| Cancer cell layer | 26.2 ± 0.3 | 1.52× 1012 | 13 |
| Stromal cell layer | 5.9 ± 0.8 | 1.16× 1012 | 3.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Igawa, K.; Izumi, K.; Sakurai, Y. Development of the Follow-Up Human 3D Oral Cancer Model in Cancer Treatment. BioTech 2023, 12, 35. https://doi.org/10.3390/biotech12020035
Igawa K, Izumi K, Sakurai Y. Development of the Follow-Up Human 3D Oral Cancer Model in Cancer Treatment. BioTech. 2023; 12(2):35. https://doi.org/10.3390/biotech12020035
Chicago/Turabian StyleIgawa, Kazuyo, Kenji Izumi, and Yoshinori Sakurai. 2023. "Development of the Follow-Up Human 3D Oral Cancer Model in Cancer Treatment" BioTech 12, no. 2: 35. https://doi.org/10.3390/biotech12020035