
Merkel Cell Carcinoma in Kidney Transplant Recipients

Abstract
:1. Introduction
2. Etiology and Pathophysiology of Merkel Cell Carcinoma
3. Epidemiology of Merkel Cell Carcinoma in Kidney Transplant Recipients
3.1. Methods of Systematic Search for Epidemiological Data
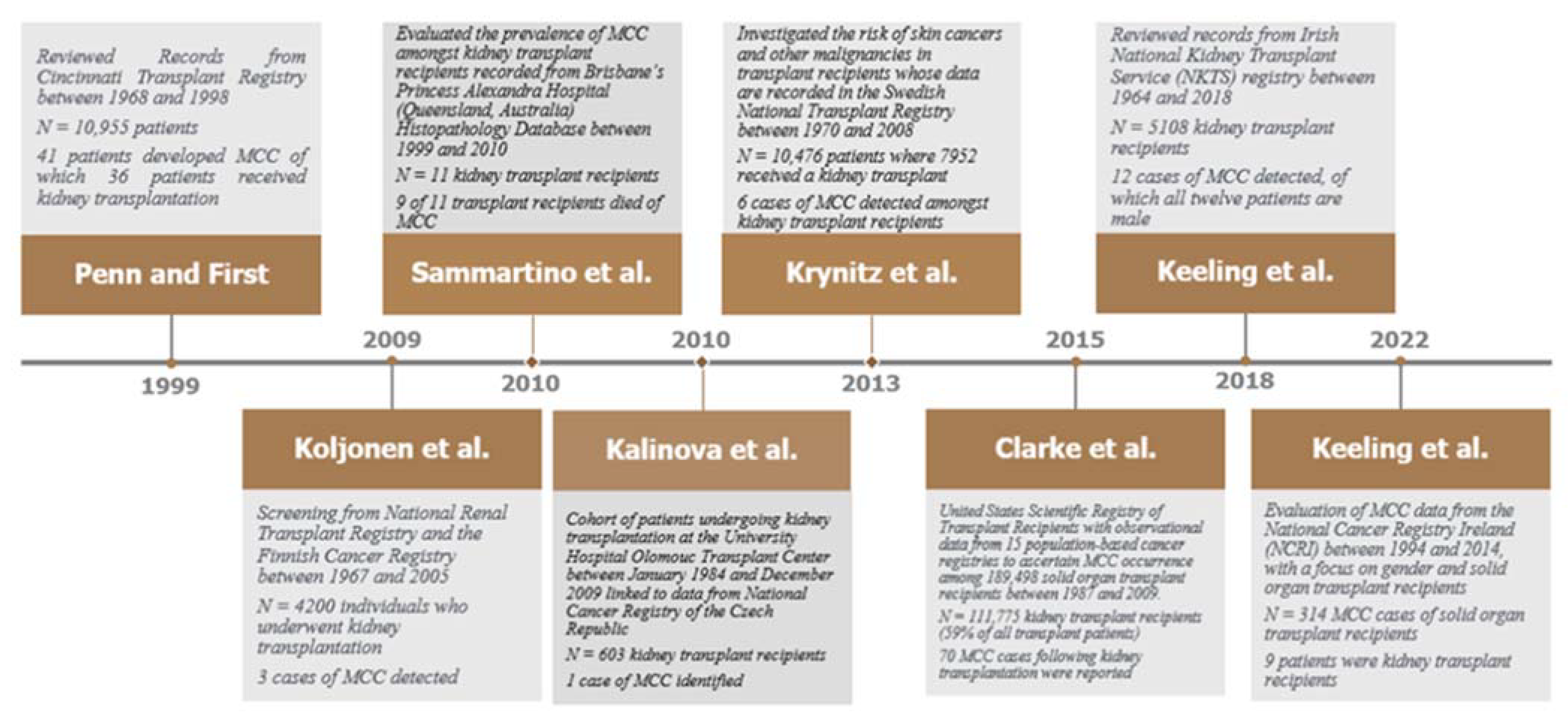
3.2. Epidemiological Cohort Studies
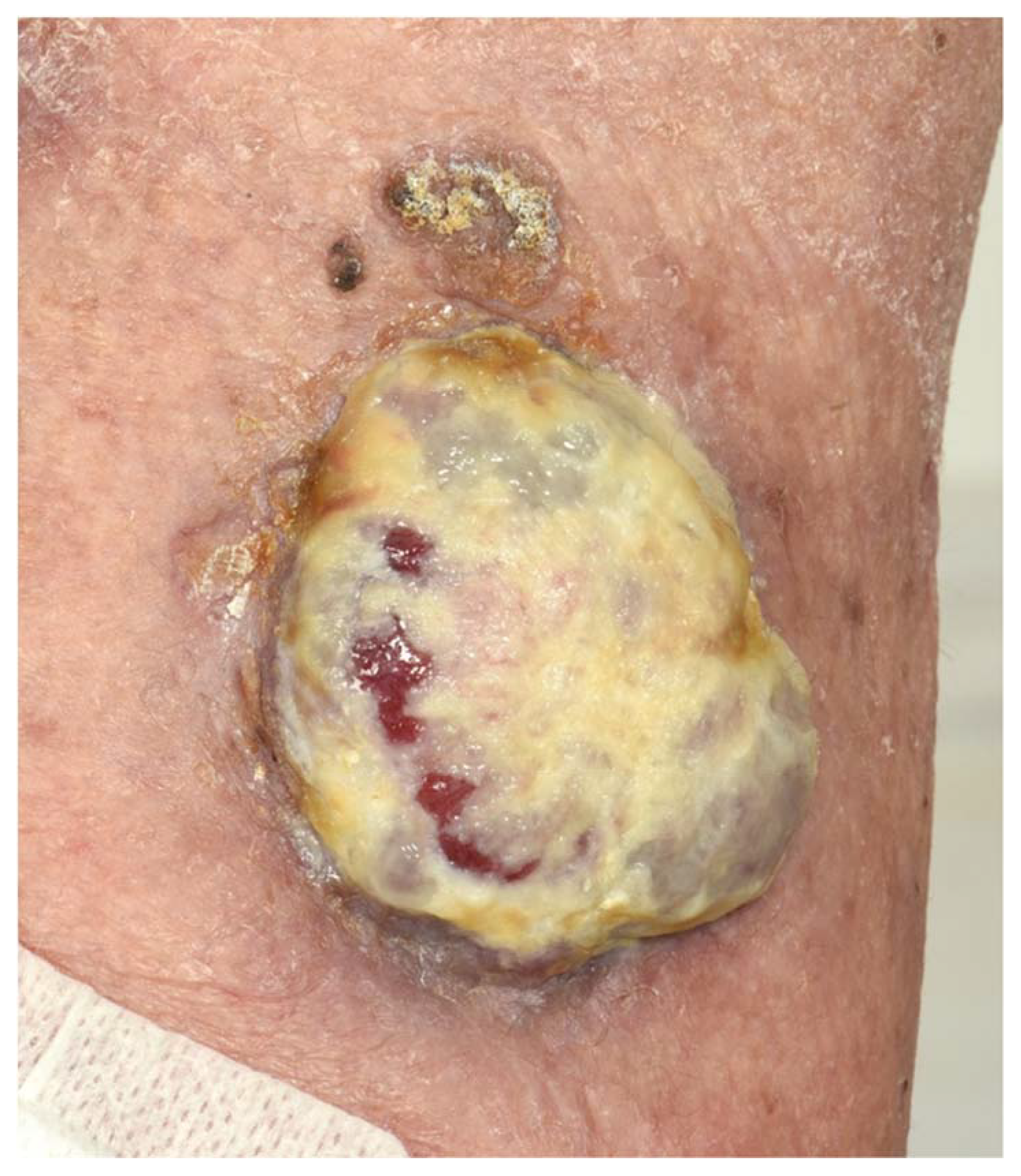
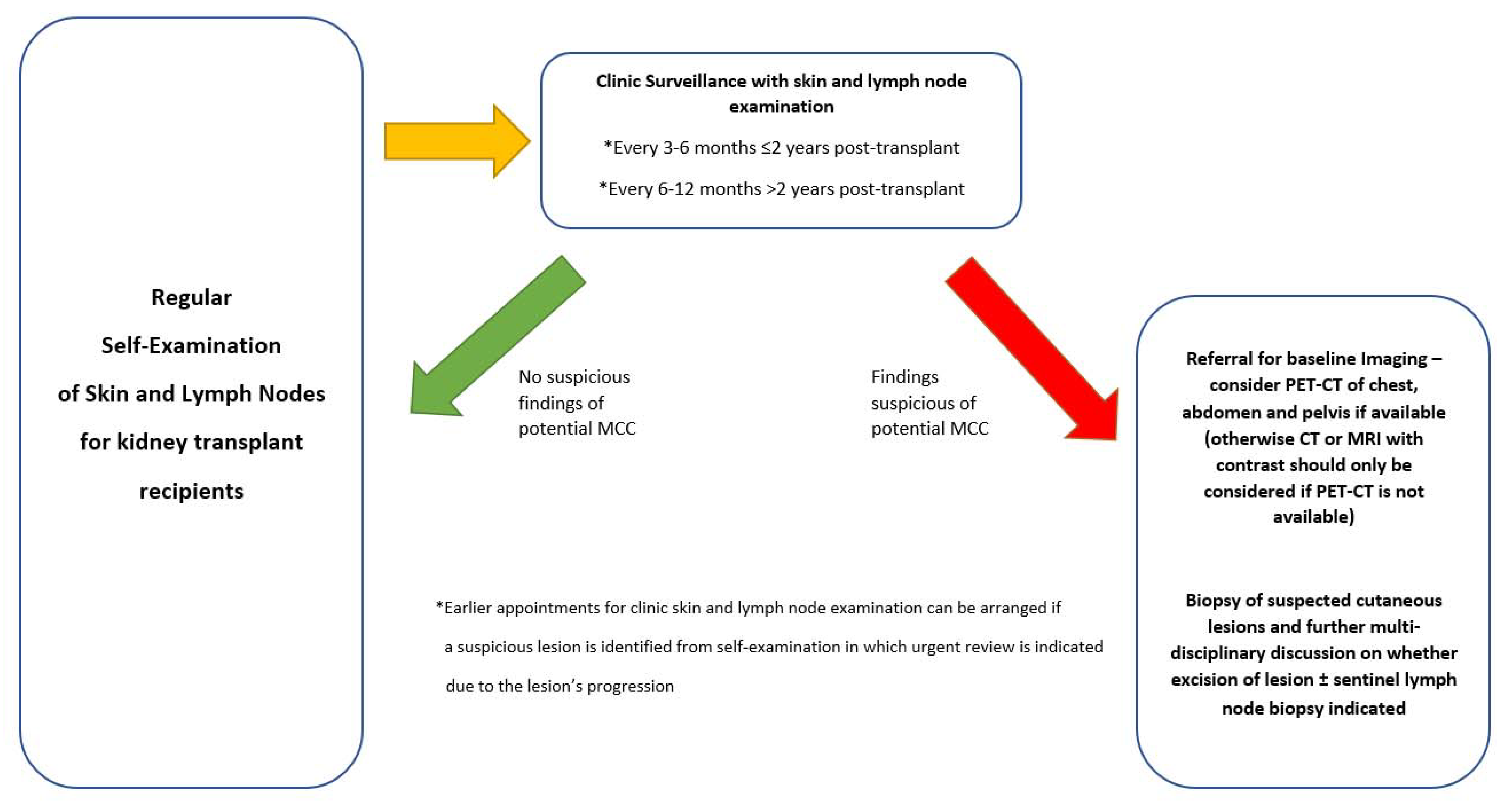
4. Clinical Presentation, Diagnostic Features and Surveillance of Merkel Cell Carcinoma
5. Prevention and Management Options for Merkel Cell Carcinoma
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goessling, W.; McKee, P.H.; Mayer, R.J. Merkel cell carcinoma. J. Clin. Oncol. 2002, 20, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; Lebbé, C.; Zur Hausen, A.; Avril, M.F.; Hariharan, S.; Bharmal, M.; Becker, J.C. Merkel cell carcinoma: Epidemiology, prognosis, therapy and unmet medical needs. Eur. J. Cancer 2017, 71, 53–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albores-Saavedra, J.; Batich, K.; Chable-Montero, F.; Sagy, N.; Schwartz, A.M.; Henson, D.E. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: A population based study. J. Cutan. Pathol. 2010, 37, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Brissett, A.E.; Olsen, K.D.; Kasperbauer, J.L.; Lewis, J.E.; Goellner, J.R.; Spotts, B.E.; Weaver, A.L.; Strome, S.E. Merkel cell carcinoma of the head and neck: A retrospective case series. Head Neck 2002, 24, 982–988. [Google Scholar] [CrossRef]
- Paulson, K.G.; Park, S.Y.; Vandeven, N.A.; Lachance, K.; Thomas, H.; Chapuis, A.G.; Harms, K.L.; Thompson, J.A.; Bhatia, S.; Stang, A.; et al. Merkel cell carcinoma: Current US incidence and projected increases based on changing demographics. J. Am. Acad Dermatol. 2018, 78, 457–463. [Google Scholar] [CrossRef]
- Ezaldein, H.H.; Ventura, A.; DeRuyter, N.P.; Yin, E.S.; Giunta, A. Understanding the influence of patient demographics on disease severity, treatment strategy, and survival outcomes in merkel cell carcinoma: A surveillance, epidemiology, and end-results study. Oncoscience 2017, 4, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Tetzlaff, M.T.; Harms, P.W. Danger is only skin deep: Aggressive epidermal carcinomas. An overview of the diagnosis, demographics, molecular-genetics, staging, prognostic biomarkers, and therapeutic advances in Merkel cell carcinoma. Mod. Pathol. 2020, 33, 42–55. [Google Scholar] [CrossRef]
- Llombart, B.; Monteagudo, C.; Lopez-Guerrero, J.A.; Carda, C.; Jorda, E.; Sanmartín, O.; Almenar, S.; Molina, I.; Martin, J.M.; Llombart-Bosch, A. Clinicopathological and immunohistochemical analysis of 20 cases of Merkel cell carcinoma in search of prognostic markers. Histopathology 2005, 46, 622–634. [Google Scholar] [CrossRef]
- Güler-Nizam, E.; Leiter, U.; Metzler, G.; Breuninger, H.; Garbe, C.; Eigentler, T.K. Clinical course and prognostic factors of Merkel cell carcinoma of the skin. Br. J. Dermatol. 2009, 161, 90–94. [Google Scholar] [CrossRef]
- Koljonen, V.; Sahi, H.; Bohling, T.; Mäkisalo, H. Post-transplant Merkel cell carcinoma. Acta. Dermato Venereol. 2016, 96, 442–447. [Google Scholar] [CrossRef]
- Tarantola, T.I.; Vallow, L.A.; Halyard, M.Y.; Weenig, R.H.; Warschaw, K.E.; Grotz, T.E.; Jakub, J.W.; Roenigk, R.K.; Brewer, J.D.; Weaver, A.L.; et al. Prognostic factors in Merkel cell carcinoma: Analysis of 240 cases. J. Am. Acad Dermatol. 2013, 68, 425–432. [Google Scholar] [CrossRef]
- Muñoz, I.P.; Masferrer, J.P.; Vegas, J.O.; Montalvo, M.S.; Díaz, R.J.; Casas, A.M. Merkel cell carcinoma from 2008 to 2012, reaching a new level of understanding. Cancer Treat. Rev. 2013, 39, 421–429. [Google Scholar] [CrossRef]
- Lemos, B.D.; Storer, B.E.; Iyer, J.G.; Phillips, J.L.; Bichakjian, C.K.; Fang, L.C.; Johnson, T.M.; Liegeois-Kwon, N.J.; Otley, C.C.; Paulson, K.G.; et al. Pathologic nodal evaluation improves prognostic accuracy in Merkel cell carcinoma: Analysis of 5823 cases as the basis of the first consensus staging system. J. Am. Acad Dermatol. 2010, 63, 751–761. [Google Scholar] [CrossRef] [Green Version]
- Lewis, C.W.; Qazi, J.; Hippe, D.S.; Lachance, K.; Thomas, H.; Cook, M.M.; Juhlin, I.; Singh, N.; Thuesmunn, Z.; Takagishi, S.R.; et al. Patterns of distant metastases in 215 Merkel cell carcinoma patients: Implications for prognosis and surveillance. Cancer Med. 2020, 9, 1374–1382. [Google Scholar] [CrossRef]
- Ikawa, F.; Kiya, K.; Uozumi, T.; Yuki, K.; Takeshita, S.; Hamasaki, O.; Arita, K.; Kurisu, K. Brain metastasis of Merkel cell carcinoma. Neurosurg. Rev. 1999, 22, 54–57. [Google Scholar] [CrossRef]
- Kamijo, A.; Koshino, T.; Hirakawa, K.; Saito, T. Merkel cell carcinoma with bone metastasis: A case report. J. Orthop. Sci. 2002, 7, 574–577. [Google Scholar] [CrossRef]
- An, K.P.; Ratner, D. Merkel cell carcinoma in the setting of HIV infection. J. Am. Acad Dermatol. 2001, 45, 309–312. [Google Scholar] [CrossRef]
- Pellitteri, P.K.; Takes, R.P.; Lewis, J.S., Jr.; Devaney, K.O.; Harlor, E.J.; Strojan, P.; Rodrigo, J.P.; Suárez, C.; Rinaldo, A.; Medina, J.E.; et al. Merkel cell carcinoma of the head and neck. Head Neck 2012, 34, 1346–1354. [Google Scholar] [CrossRef]
- Yamana, N.; Sueyama, H.; Hamada, M. Cardiac metastasis from Merkel cell skin carcinoma. Int. J. Clin. Oncol. 2004, 9, 210–212. [Google Scholar] [CrossRef]
- Motaouakil, A.; Boukhannous, I.; Chennoufi, M.; El Moudane, A.; Mokhtari, M.; Barki, A. Kidney metastasis in a case of Merkel cell carcinoma. Urol. Case. Rep. 2021, 37, 101704. [Google Scholar] [CrossRef]
- Krynitz, B.; Edgren, G.; Lindelöf, B.; Baecklund, E.; Brattström, C.; Wilczek, H.; Smedby, K.E. Risk of skin cancer and other malignancies in kidney, liver, heart and lung transplant recipients 1970 to 2008—A Swedish population-based study. Int. J. Cancer 2013, 132, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Penn, I.; First, M.R. Merkel’s cell carcinoma in organ recipients: Report of 41 cases1. Transplantation 1999, 68, 1717–1721. [Google Scholar] [CrossRef] [PubMed]
- Heath, M.; Jaimes, N.; Lemos, B.; Mostaghimi, A.; Wang, L.C.; Peñas, P.F.; Nghiem, P. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: The AEIOU features. J. Am. Acad Dermatol. 2008, 58, 375–381. [Google Scholar] [CrossRef] [Green Version]
- Paulson, K.G.; Iyer, J.G.; Blom, A.; Warton, E.M.; Sokil, M.; Yelistratova, L.; Schuman, L.; Nagase, K.; Bhatia, S.; Asgari, M.M.; et al. Systemic immune suppression predicts diminished merkel cell carcinoma–specific survival independent of stage. J. Investig. Dermatol. 2013, 133, 642–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, M.; Baker, K.; Redman, M.; Lachance, K.; Nguyen, M.; Parvathaneni, U.; Bhatia, S.; Nghiem, P.T.; Tseng, Y.D. Differential outcomes among immunosuppressed patients with Merkel cell carcinoma: Impact of immunosuppression type on cancer-specific and overall survival. Am. J. Clin. Oncol. 2019, 42, 82–88. [Google Scholar] [CrossRef]
- Clarke, C.A.; Robbins, H.A.; Tatalovich, Z.; Lynch, C.F.; Pawlish, K.S.; Finch, J.L.; Hernandez, B.Y.; Fraumeni, J.F., Jr.; Madeleine, M.M.; Engels, E.A. Risk of merkel cell carcinoma after solid organ transplantation. J. Natl. Cancer Inst. 2015, 107, dju382. [Google Scholar] [CrossRef] [Green Version]
- Sahi, H.; Kukko, H.; Böhling, T.; Tukiainen, E.; Sihto, H.; Joensuu, H.; Koljonen, V. Unusually young Merkel cell carcinoma patients are Merkel cell polyomavirus positive and frequently immunocompromised. Eur. J. Plast. Surg. 2010, 33, 349–353. [Google Scholar] [CrossRef]
- Ma, J.E.; Brewer, J.D. Merkel cell carcinoma in immunosuppressed patients. Cancers 2014, 6, 1328–1350. [Google Scholar] [CrossRef]
- Rotondo, J.C.; Bononi, I.; Puozzo, A.; Govoni, M.; Foschi, V.; Lanza, G.; Gafà, R.; Gaboriaud, P.; Touzé, F.A.; Selvatici, R.; et al. Merkel Cell Carcinomas Arising in Autoimmune Disease Affected Patients Treated with Biologic Drugs, Including Anti-TNFMCC in Autoimmune Disease Patients. Clin. Cancer. Res. 2017, 23, 3929–3934. [Google Scholar] [CrossRef] [Green Version]
- Schlemeyer, T.; Ohnezeit, D.; Virdi, S.; Körner, C.; Weißelberg, S.; Starzonek, S.; Schumacher, U.; Grundhoff, A.; Indenbirken, D.; Albertini, S.; et al. Merkel cell carcinoma and immune evasion: Merkel cell polyomavirus small T-antigen induced surface changes can be reverted by therapeutic intervention. J. Investig. Dermatol. 2022, 142, 3071–3081.e13. [Google Scholar] [CrossRef]
- D’Angelo, S.P.; Bhatia, S.; Brohl, A.S.; Hamid, O.; Mehnert, J.M.; Terheyden, P.; Shih, K.C.; Brownell, I.; Lebbé, C.; Lewis, K.D.; et al. Avelumab in patients with previously treated metastatic Merkel cell carcinoma: Long-term data and biomarker analyses from the single-arm phase 2 JAVELIN Merkel 200 trial. J. Immunother. Cancer 2020, 8, e000674. [Google Scholar] [CrossRef]
- Nghiem, P.; Bhatia, S.; Lipson, E.J.; Sharfman, W.H.; Kudchadkar, R.R.; Brohl, A.S.; Friedlander, P.A.; Daud, A.; Kluger, H.M.; Reddy, S.A.; et al. Durable tumor regression and overall survival in patients with advanced Merkel cell carcinoma receiving pembrolizumab as first-line therapy. J. Clin. Oncol. 2019, 37, 693–702. [Google Scholar] [CrossRef]
- Kim, S.; Wuthrick, E.; Blakaj, D.; Eroglu, Z.; Verschraegen, C.; Thapa, R.; Mills, M.; Dibs, K.; Liveringhouse, C.; Russell, J.; et al. Combined nivolumab and ipilimumab with or without stereotactic body radiation therapy for advanced Merkel cell carcinoma: A randomised, open label, phase 2 trial. Lancet 2022, 400, 1008–1019. [Google Scholar] [CrossRef]
- Gauci, M.L.; Aristei, C.; Becker, J.C.; Blom, A.; Bataille, V.; Dreno, B.; Del Marmol, V.; Forsea, A.M.; Fargnoli, M.C.; Grob, J.J.; et al. Diagnosis and treatment of Merkel cell carcinoma: European consensus-based interdisciplinary guideline—Update 2022. Eur. J. Cancer. 2022, 171, 203–231. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves First Treatment for Rare form of Skin Cancer. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-rare-form-skin-cancer (accessed on 15 November 2022).
- U.S. Food and Drug Administration. FDA Approves Pembrolizumab for Merkel Cell Carcinoma. Available online: https://www.fda.gov/drugs/fda-approves-pembrolizumab-merkel-cell-carcinoma (accessed on 15 November 2022).
- Song, L.; Bretz, A.C.; Gravemeyer, J.; Spassova, I.; Muminova, S.; Gambichler, T.; Sriram, A.; Ferrone, S.; Becker, J.C. The HDAC Inhibitor domatinostat promotes cell-cycle arrest, induces apoptosis, and increases immunogenicity of Merkel cell carcinoma cells. J. Investig. Dermatol. 2021, 141, 903–912.e4. [Google Scholar] [CrossRef]
- Zur Hausen, A.; Rennspiess, D.; Winnepenninckx, V.; Speel, E.J.; Kurz, A.K. Early B-cell differentiation in Merkel cell carcinomas: Clues to cellular ancestry. Cancer Res. 2013, 73, 4982–4987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tilling, T.; Wladykowski, E.; Failla, A.V.; Houdek, P.; Brandner, J.M.; Moll, I. Immunohistochemical analyses point to epidermal origin of human Merkel cells. Histochem. Cell Biol. 2014, 141, 407–421. [Google Scholar] [CrossRef]
- Tilling, T.; Moll, I. Which are the cells of origin in merkel cell carcinoma? J. Skin Cancer 2012, 2012, 680410. [Google Scholar] [CrossRef] [Green Version]
- Sunshine, J.C.; Jahchan, N.S.; Sage, J.; Choi, J. Are there multiple cells of origin of Merkel cell carcinoma? Oncogene 2018, 37, 1409–1416. [Google Scholar] [CrossRef]
- Becker, J.C.; Stang, A.; DeCaprio, J.A.; Cerroni, L.; Lebbé, C.; Veness, M.; Nghiem, P. Merkel cell carcinoma. Nat. Rev. Dis. Prim. 2017, 3, 1–7. [Google Scholar] [CrossRef]
- Duncavage, E.J.; Zehnbauer, B.A.; Pfeifer, J.D. Prevalence of Merkel cell polyomavirus in Merkel cell carcinoma. Mod. Pathol. 2009, 22, 516–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popp, S.; Waltering, S.; Herbst, C.; Moll, I.; Boukamp, P. UV-B-type mutations and chromosomal imbalances indicate common pathways for the development of Merkel and skin squamous cell carcinomas. Int. J. Cancer 2002, 99, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.; Shuda, M.; Chang, Y.; Moore, P.S. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science 2008, 319, 1096–1100. [Google Scholar] [CrossRef] [Green Version]
- Martel-Jantin, C.; Pedergnana, V.; Nicol, J.T.; Leblond, V.; Trégouët, D.A.; Tortevoye, P.; Plancoulaine, S.; Coursaget, P.; Touzé, A.; Abel, L.; et al. Merkel cell polyomavirus infection occurs during early childhood and is transmitted between siblings. J. Clin. Virol. 2013, 58, 288–291. [Google Scholar] [CrossRef] [Green Version]
- Loyo, M.; Guerrero-Preston, R.; Brait, M.; Hoque, M.O.; Chuang, A.; Kim, M.S.; Sharma, R.; Liégeois, N.J.; Koch, W.M.; Califano, J.A.; et al. Quantitative detection of Merkel cell virus in human tissues and possible mode of transmission. Int. J. Cancer 2010, 126, 2991–2996. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; You, J. Molecular mechanisms of merkel cell polyomavirus transformation and replication. Ann. Rev. Virol. 2020, 7, 289–307. [Google Scholar] [CrossRef]
- Tolstov, Y.L.; Pastrana, D.V.; Feng, H.; Becker, J.C.; Jenkins, F.J.; Moschos, S.; Chang, Y.; Buck, C.B.; Moore, P.S. Human Merkel cell polyomavirus infection II. MCV is a common human infection that can be detected by conformational capsid epitope immunoassays. Int. J. Cancer 2009, 125, 1250–1256. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Liu, F.; He, Z.; Deng, Q.; Pan, Y.; Liu, Y.; Zhang, C.; Ning, T.; Guo, C.; Liang, Y.; et al. Seroprevalence of Merkel cell polyomavirus in the general rural population of Anyang, China. PLoS ONE 2014, 9, e106430. [Google Scholar] [CrossRef]
- Vahabpour, R.; Aghasadeghi, M.R.; Salehi-Vaziri, M.; Mohajel, N.; Keyvani, H.; Nasimi, M.; Esghaei, M.; Monavari, S.H. Prevalence of Merkel cell polyomavirus in Tehran: An age-specific serological study. Iran Red. Crescent Med. J. 2016, 18, e26097. [Google Scholar] [CrossRef] [Green Version]
- Van der Meijden, E.; Bialasiewicz, S.; Rockett, R.J.; Tozer, S.J.; Sloots, T.P.; Feltkamp, M.C. Different serologic behavior of MCPyV, TSPyV, HPyV6, HPyV7 and HPyV9 polyomaviruses found on the skin. PloS ONE 2013, 8, e81078. [Google Scholar] [CrossRef] [PubMed]
- Iyer, J.G.; Afanasiev, O.K.; McClurkan, C.; Paulson, K.; Nagase, K.; Jing, L.; Marshak, J.O.; Dong, L.; Carter, J.; Lai, I.; et al. Merkel Cell Polyomavirus-Specific CD8+ and CD4+ T-cell Responses Identified in Merkel Cell Carcinomas and Blood T-cell Responses against Merkel Cell Polyomavirus. Clin. Cancer Res. 2011, 17, 6671–6680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulson, K.G.; Carter, J.J.; Johnson, L.G.; Cahill, K.W.; Iyer, J.G.; Schrama, D.; Becker, J.C.; Madeleine, M.M.; Nghiem, P.; Galloway, D.A. Antibodies to merkel cell polyomavirus T antigen oncoproteins reflect tumor burden in merkel cell carcinoma patients. Cancer Res. 2010, 70, 8388–8397. [Google Scholar] [CrossRef] [Green Version]
- Afanasiev, O.K.; Yelistratova, L.; Miller, N.; Nagase, K.; Paulson, K.; Iyer, J.G.; Ibrani, D.; Koelle, D.M.; Nghiem, P. Merkel Polyomavirus-Specific T Cells Fluctuate with Merkel Cell Carcinoma Burden and Express Therapeutically Targetable PD-1 and Tim-3 Exhaustion Markers Fluctuating and Exhausted CD8 T Cells in MCC. Clin. Cancer Res. 2013, 19, 5351–5360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harms, P.W.; Patel, R.M.; Verhaegen, M.E.; Giordano, T.J.; Nash, K.T.; Johnson, C.N.; Daignault, S.; Thomas, D.G.; Gudjonsson, J.E.; Elder, J.T.; et al. Distinct gene expression profiles of viral-and nonviral-associated merkel cell carcinoma revealed by transcriptome analysis. J. Investig. Dermatol. 2013, 133, 936–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sihto, H.; Joensuu, H. Tumor-infiltrating lymphocytes and outcome in Merkel cell carcinoma, a virus-associated cancer. Oncoimmunology 2012, 1, 1420–1421. [Google Scholar] [CrossRef] [Green Version]
- Paulson, K.G.; Iyer, J.G.; Tegeder, A.R.; Thibodeau, R.; Schelter, J.; Koba, S.; Schrama, D.; Simonson, W.T.; Lemos, B.D.; Byrd, D.R.; et al. Transcriptome-wide studies of merkel cell carcinoma and validation of intratumoral CD8+ lymphocyte invasion as an independent predictor of survival. J. Clin. Oncol. 2011, 29, 1539–1546. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, L.E.; Mohsin, N.; Yaghi, M.; Frech, F.S.; Dreyfuss, I.; Nouri, K. Merkel cell carcinoma: An updated review of pathogenesis, diagnosis, and treatment options. Dermatol. Ther. 2022, 35, e15292. [Google Scholar] [CrossRef]
- Afanasiev, O.K.; Nagase, K.; Simonson, W.; Vandeven, N.; Blom, A.; Koelle, D.M.; Clark, R.; Nghiem, P. Vascular E-selectin expression correlates with CD8 lymphocyte infiltration and improved outcome in Merkel cell carcinoma. J. Investig. Dermatol. 2013, 133, 2065–2073. [Google Scholar] [CrossRef] [Green Version]
- Dowlatshahi, M.; Huang, V.; Gehad, A.E.; Jiang, Y.; Calarese, A.; Teague, J.E.; Dorosario, A.A.; Cheng, J.; Nghiem, P.; Schanbacher, C.F.; et al. Tumor-specific T cells in human Merkel cell carcinomas: A possible role for Tregs and T-cell exhaustion in reducing T-cell responses. J. Investig. Dermatol. 2013, 133, 1879–1889. [Google Scholar] [CrossRef] [Green Version]
- Theiss, J.M.; Günther, T.; Alawi, M.; Neumann, F.; Tessmer, U.; Fischer, N.; Grundhoff, A. A comprehensive analysis of replicating Merkel cell polyomavirus genomes delineates the viral transcription program and suggests a role for mcv-miR-M1 in episomal persistence. PLoS Pathog. 2015, 11, e1004974. [Google Scholar] [CrossRef]
- Harms, P.W.; Vats, P.; Verhaegen, M.E.; Robinson, D.R.; Wu, Y.M.; Dhanasekaran, S.M.; Palanisamy, N.; Siddiqui, J.; Cao, X.; Su, F.; et al. The distinctive mutational spectra of polyomavirus-negative Merkel cell carcinoma. Cancer Res. 2015, 75, 3720–3727. [Google Scholar] [CrossRef] [Green Version]
- Goh, G.; Walradt, T.; Markarov, V.; Blom, A.; Riaz, N.; Doumani, R.; Stafstrom, K.; Moshiri, A.; Yelistratova, L.; Levinsohn, J.; et al. Mutational landscape of MCPyV-positive and MCPyV-negative Merkel cell carcinomas with implications for immunotherapy. Oncotarget 2016, 7, 3403–3415. [Google Scholar] [CrossRef] [Green Version]
- Starrett, G.J.; Marcelus, C.; Cantalupo, P.G.; Katz, J.P.; Cheng, J.; Akagi, K.; Thakuria, M.; Rabinowits, G.; Wang, L.C.; Symer, D.E.; et al. Merkel cell polyomavirus exhibits dominant control of the tumor genome and transcriptome in virus-associated Merkel cell carcinoma. MBio 2017, 8, e02079-16. [Google Scholar] [CrossRef] [Green Version]
- Del Carmen Gonzalez-Vela, M.; Curiel-Olmo, S.; Derdak, S.; Beltran, S.; Santibanez, M.; Martinez, N.; Castillo-Trujillo, A.; Gut, M.; Sanchez-Pacheco, R.; Almaraz, C.; et al. Shared oncogenic pathways implicated in both virus-positive and UV-induced Merkel cell carcinomas. J. Investig. Dermatol. 2017, 137, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.Q.; Waldeck, K.; Vergara, I.A.; Schröder, J.; Madore, J.; Wilmott, J.S.; Colebatch, A.J.; De Paoli-Iseppi, R.; Li, J.; Lupat, R.; et al. UV-associated mutations underlie the etiology of MCV-negative Merkel cell carcinomas. Cancer Res. 2015, 75, 5228–5234. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.M.; Cushman, C.H.; DeCaprio, J.A. Merkel cell polyomavirus: Oncogenesis in a stable genome. Viruses 2021, 14, 58. [Google Scholar] [CrossRef]
- Bottomley, M.J.; Thomson, J.; Harwood, C.; Leigh, I. The role of the immune system in cutaneous squamous cell carcinoma. Int. J. Mol. Sci. 2019, 20, 2009. [Google Scholar] [CrossRef] [Green Version]
- Harwood, C.A.; Mesher, D.; McGregor, J.M.; Mitchell, L.; Leedham-Green, M.; Raftery, M.; Cerio, R.; Leigh, I.M.; Sasieni, P.; Proby, C.M. A surveillance model for skin cancer in organ transplant recipients: A 22-year prospective study in an ethnically diverse population. Am. J. Transplant. 2013, 13, 119–129. [Google Scholar] [CrossRef]
- Kuschal, C.; Thoms, K.M.; Schubert, S.; Schäfer, A.; Boeckmann, L.; Schön, M.P.; Emmert, S. Skin cancer in organ transplant recipients: Effects of immunosuppressive medications on DNA repair. Exp. Dermatol. 2012, 21, 2–6. [Google Scholar] [CrossRef]
- Muirhead, R.; Ritchie, D.M. Partial regression of Merkel cell carcinoma in response to withdrawal of azathioprine in an immunosuppression-induced case of metastatic Merkel cell carcinoma. Clin. Oncol. 2007, 19, 96. [Google Scholar] [CrossRef]
- Friedlaender, M.M.; Rubinger, D.; Rosenbaum, E.; Amir, G.; Siguencia, E. Temporary regression of Merkel cell carcinoma metastases after cessation of cyclosporine. Transplantation 2002, 73, 1849–1850. [Google Scholar] [CrossRef] [PubMed]
- Formica, M.; Basolo, B.; Funaro, L.; Mazzucco, G.; Segoloni, G.P.; Piccoli, G. Merkel cell carcinoma in renal transplant recipient. Nephron 1994, 68, 399. [Google Scholar] [CrossRef] [PubMed]
- Douds, A.C.; Mellotte, G.J.; Morgan, S.H. Fatal Merkel-cell tumour (cutaneous neuroendocrine carcinoma) complicating renal transplantation. Nephrol. Dial. Transplant. 1995, 10, 2346–2348. [Google Scholar] [CrossRef] [PubMed]
- Gooptu, C.; Woollons, A.; Ross, J.; Price, M.; Wojnarowska, F.; Morris, P.J.; Wall, S.; Bunker, C.B. Merkel cell carcinoma arising after therapeutic immunosuppression. Br. J. Dermatol. 1997, 137, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.H.; Morgan, M.B.; Mathieson, I.M.; Rabb, H. Merkel cell carcinoma in a renal transplant patient: Increased incidence? Transplantation 1998, 65, 1396–1397. [Google Scholar] [CrossRef]
- Urbatsch, A.; Sams, W.M., Jr.; Urist, M.M.; Sturdivant, R. Merkel cell carcinoma occurring in renal transplant patients. J. Am. Acad Dermatol. 1999, 41, 289–291. [Google Scholar] [CrossRef]
- Silvestris, N.; D’Elia, F.; Tarantino, G.; Lucarelli, A. Merkel cell carcinoma in a renal transplant patient. J. Exp. Clin. Cancer Res. 2000, 19, 399–400. [Google Scholar]
- Bartsch, C.; Mechtersheimer, G.; Helmchen, B.; Krempien, B. Merkel-Zell-Karzinom nach Nierentransplantation. Extreme Lebensumstände als mittelbare Todesursache. Pathologe 2002, 23, 308–312. [Google Scholar] [CrossRef]
- Bucci, J.; Popovsky, J.; Wikas, S. Merkel Cell Carcinoma in a Renal-Transplant Patient. J. Resi. Dermatol. 2003, 7, 19–22. [Google Scholar]
- Morris, K.L.; Williams, B.; Kennedy, G.A. Images in haematology. Heavy bone marrow involvement with metastatic Merkel cell tumour in an immunosuppressed renal transplant recipient. Br. J. Haematol. 2005, 128, 133. [Google Scholar] [CrossRef]
- Ferreira, P.; Pinho, C.; Cardoso, A.; Pereira, J.M.; Cunha, R.; Rodrigues, J.; Amarante, J. Unusual Merkel cell carcinoma in a renal transplant recipient: Case report and review of the literature. Eur. J. Plast. Surg. 2006, 28, 426–431. [Google Scholar] [CrossRef]
- Kanitakis, J.; Euvrard, S.; Chouvet, B.; Butnaru, A.C.; Claudy, A. Merkel cell carcinoma in organ-transplant recipients: Report of two cases with unusual histological features and literature review. J. Cutan. Pathol. 2006, 33, 686–694. [Google Scholar] [CrossRef]
- Lau, P.P.; Lui, P.C. Fine needle aspiration diagnosis of metastatic Merkel cell carcinoma with multinucleated bizarre tumour cells in a post-renal transplant patient. Pathology 2006, 38, 456–458. [Google Scholar] [CrossRef]
- Kaisar, M.O.; Mahadevan, K.; Faull, R.J. Primary presentation with metastatic merkel cell carcinoma in a renal transplant recipient. Nephrology 2007, 12, 420–421. [Google Scholar] [CrossRef]
- Kurnatowska, I.; Zawiasa, A.; Narbutt, J.; Wagrowska-Danielewicz, M.; Stempien, M.; Nowicki, M. Merkel cell carcinoma in a kidney transplant patient: Case report and update on management. Ann. Transplant. 2010, 15, 66–70. [Google Scholar]
- Krejci, K.; Tichy, T.; Horak, P.; Ciferska, H.; Hajduch, M.; Srovnal, J.; Trojanec, R.; Zezulová, M.; Zlevorová, M.; Kalinová, L.; et al. Merkel cell carcinoma of the gluteal region with ipsilateral metastasis into the pancreatic graft of a patient after combined kidney-pancreas transplantation. Onkologie 2010, 33, 520–524. [Google Scholar] [CrossRef]
- Singh, P.; Von, J.V.; Prosek, J.; Rovin, B.; Pesavento, T.E.; Olencki, T.; Pandey, D. Preserved renal allograft function and successful treatment of metastatic Merkel cell cancer post nivolumab therapy. Transplantation 2019, 103, e52–e53. [Google Scholar] [CrossRef]
- Bystrup Boyles, T.; Schødt, M.; Hendel, H.W.; Krarup-Hansen, A.; Junker, N. Pembrolizumab as first line treatment of Merkel cell carcinoma patients—A case series of patients with various co-morbidities. Acta Oncol. 2020, 59, 793–796. [Google Scholar] [CrossRef]
- Rizzo, J.M.; Harms, P.W.; Harms, K.L.; Plaska, A.; Brenner, C.; Durham, A.B. Unknown primary Merkel cell carcinoma in the immunosuppressed patient: Case series. JAAD Case Rep. 2021, 8, 19–22. [Google Scholar] [CrossRef]
- Wu, H.H.L.; Jeyalan, V.; Ponnusamy, A. An Unusual Cause of AKI in a Kidney Transplant Patient with Merkel Cell Cancer. Kidney360 2021, 2, 2040–2041. [Google Scholar] [CrossRef]
- Koljonen, V.; Kukko, H.; Tukiainen, E.; Böhling, T.; Sankila, R.; Pukkala, E.; Sihto, H.; Joensuu, H.; Kyllönen, L.; Mäkisalo, H. Incidence of Merkel cell carcinoma in renal transplant recipients. Nephrol. Dial. Transplant. 2009, 24, 3231–3235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sammartino, C.; Edey, M.; Barraclough, K.; Bialasiewicz, S.; Rockett, R.; Sloots, T.; Oliver, K.; Strutton, G.; Griffin, A.; Campell, S.; et al. Outcome of Merkel cell carcinoma in renal transplant recipients. Nephrology 2010, 15, 63–64. [Google Scholar]
- Kalinova, L.; Majek, O.; Stehlik, D.; Krejci, K.; Bachleda, P. Skin cancer incidence in renal transplant recipients-a single center study. Biomed. Pap. Med. Fac. Univ. Palacky. Olomouc. Czech. Repub. 2010, 154, 257–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keeling, E.; Murray, S.L.; Williams, Y.; Sexton, D.J.; O’Kelly, P.; Deady, S.; O’Leary, E.; Dorman, A.; Roche, M.; Ni Raghallaigh, S.; et al. Merkel cell carcinoma in kidney transplant recipients in Ireland 1964–2018. Br. J. Dermatol. 2019, 181, 1314–1315. [Google Scholar] [CrossRef] [PubMed]
- Keeling, E.; O’Leary, E.; Deady, S.; ONeill, J.P.; Conlon, P.J.; Moloney, F.J. Gender and immunosuppression impact on Merkel cell carcinoma diagnosis and prognosis. A population based cohort study. Skin. Health Dis. 2022, 2, e80. [Google Scholar] [CrossRef]
- Becker, J.C.; Kauczok, C.S.; Ugurel, S.; Eib, S.; Bröcker, E.B.; Houben, R. Merkel cell carcinoma: Molecular pathogenesis, clinical features and therapy. J. Dtsch. Dermatol. Ges. 2008, 6, 709–719. [Google Scholar] [CrossRef]
- Lien, M.H.; Baldwin, B.T.; Thareja, S.K.; Fenske, N.A. Merkel cell carcinoma: Clinical characteristics, markers, staging and treatment. J. Drugs. Dermatol. 2010, 9, 779–784. [Google Scholar]
- Llombart, B.; Requena, C.; Cruz, J. Update on Merkel cell carcinoma: Epidemiology, etiopathogenesis, clinical features, diagnosis, and staging. Actas Dermosifiliogr. 2017, 108, 108–119. [Google Scholar] [CrossRef]
- Sparks, J.; Sparks, M.; Malone, J.C. Cutaneous Merkel cell carcinoma: Multiple asynchronous primary lesions in a patient on immunosuppressive therapy. J. Cutan. Pathol. 2017, 44, 309–312. [Google Scholar] [CrossRef]
- Fried, I.; Cerroni, L. Merkel cell carcinoma. Pathologe 2014, 35, 467–475. [Google Scholar] [CrossRef]
- Calder, K.B.; Smoller, B.R. New insights into merkel cell carcinoma. Adv. Anat. Pathol. 2010, 17, 155–161. [Google Scholar] [CrossRef]
- Narisawa, Y.; Koba, S.; Inoue, T.; Nagase, K. Histogenesis of pure and combined Merkel cell carcinomas: An immunohistochemical study of 14 cases. J. Dermatol. 2015, 42, 445–452. [Google Scholar] [CrossRef]
- Iacocca, M.V.; Abernethy, J.L.; Stefanato, C.M.; Allan, A.E.; Bhawan, J. Mixed Merkel cell carcinoma and squamous cell carcinoma of the skin. J. Am. Acad. Dermatol. 1998, 39, 882–887. [Google Scholar] [CrossRef]
- Lai, J.H.; Fleming, K.E.; Ly, T.Y.; Pasternak, S.; Godlewski, M.; Doucette, S.; Walsh, N.M. Pure versus combined Merkel cell carcinomas: Immunohistochemical evaluation of cellular proteins (p53, Bcl-2, and c-kit) reveals significant overexpression of p53 in combined tumors. Human. Pathol. 2015, 46, 1290–1296. [Google Scholar] [CrossRef]
- Sakata, Y.; Inaba, Y.; Kunimoto, K.; Kaminaka, C.; Yamamoto, Y.; Iwahashi, Y.; Murata, S.I.; Asamura, S.; Jinnin, M. The clinical significance of cytokeratin 20 staining pattern in Merkel cell carcinoma. Drug. Discov. Ther. 2021, 15, 162–165. [Google Scholar] [CrossRef]
- Pasternak, S.; Carter, M.D.; Ly, T.Y.; Doucette, S.; Walsh, N.M. Immunohistochemical profiles of different subsets of Merkel cell carcinoma. Human. Pathol. 2018, 82, 232–238. [Google Scholar] [CrossRef]
- Miller, N.J.; Church, C.D.; Dong, L.; Crispin, D.; Fitzgibbon, M.P.; Lachance, K.; Jing, L.; Shinohara, M.; Gavvovidis, I.; Willimsky, G.; et al. Tumor-Infiltrating Merkel Cell Polyomavirus-Specific T Cells Are Diverse and Associated with Improved Patient Survival A02-Restricted T-cell Receptors in Merkel Cell Carcinoma. Cancer Immunol. Res. 2017, 5, 137–147. [Google Scholar] [CrossRef] [Green Version]
- Ames, H.M.; Bichakjian, C.K.; Liu, G.Y.; Oravecz-Wilson, K.I.; Fullen, D.R.; Verhaegen, M.E.; Johnson, T.M.; Dlugosz, A.A.; Ross, T.S. Huntingtin-interacting protein 1, a Merkel cell carcinoma marker that interacts with c-Kit. J. Investig. Dermatol. 2011, 131, 2113–2120. [Google Scholar] [CrossRef] [Green Version]
- Fleming, K.E.; Ly, T.Y.; Pasternak, S.; Godlewski, M.; Doucette, S.; Walsh, N.M. Support for p63 expression as an adverse prognostic marker in Merkel cell carcinoma: Report on a Canadian cohort. Human. Pathol. 2014, 45, 952–960. [Google Scholar] [CrossRef]
- Stetsenko, G.Y.; Malekirad, J.; Paulson, K.G.; Iyer, J.G.; Thibodeau, R.M.; Nagase, K.; Schmidt, M.; Storer, B.E.; Argenyi, Z.B.; Nghiem, P. p63 expression in Merkel cell carcinoma predicts poorer survival yet may have limited clinical utility. Am. J. Clin. Pathol. 2013, 140, 838–844. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.G.; Wang, L.C.; Penas, P.F.; Gellenthin, M.; Lee, S.J.; Nghiem, P. Sentinel lymph node biopsy for evaluation and treatment of patients with Merkel cell carcinoma: The Dana-Farber experience and meta-analysis of the literature. Arch. Dermatol. 2006, 142, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Concannon, R.; Larcos, G.S.; Veness, M. The impact of 18F-FDG PET-CT scanning for staging and management of Merkel cell carcinoma: Results from Westmead Hospital, Sydney, Australia. J. Am. Acad. Dermatol. 2010, 62, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Harms, K.L.; Healy, M.A.; Nghiem, P.; Sober, A.J.; Johnson, T.M.; Bichakjian, C.K.; Wong, S.L. Analysis of prognostic factors from 9387 Merkel cell carcinoma cases forms the basis for the new 8th edition AJCC staging system. Ann. Surg. Oncol. 2016, 23, 3564–3571. [Google Scholar] [CrossRef] [PubMed]
- Walsh, N.M. Complete spontaneous regression of Merkel cell carcinoma (1986–2016): A 30 year perspective. J. Cutan. Pathol. 2016, 43, 1150–1154. [Google Scholar] [CrossRef]
- Bichakjian, C.K.; Olencki, T.; Aasi, S.Z.; Alam, M.; Andersen, J.S.; Blitzblau, R.; Bowen, G.M.; Contreras, C.M.; Daniels, G.A.; Decker, R.; et al. Merkel cell carcinoma, version 1.2018, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 2018, 16, 742–774. [Google Scholar] [CrossRef]
- Hawryluk, E.B.; O’Regan, K.N.; Sheehy, N.; Guo, Y.; Dorosario, A.; Sakellis, C.G.; Jacene, H.A.; Wang, L.C. Positron emission tomography/computed tomography imaging in Merkel cell carcinoma: A study of 270 scans in 97 patients at the Dana-Farber/Brigham and Women’s Cancer Center. J. Am. Acad Dermatol. 2013, 68, 592–599. [Google Scholar] [CrossRef]
- Locke, F.L.; Rollison, D.E.; Sondak, V.K. Merkel cell carcinoma and immunosuppression: What we still need to know. J. Natl. Cancer Inst. 2015, 107, dju422. [Google Scholar] [CrossRef] [Green Version]
- Paulson, K.G.; Lewis, C.W.; Redman, M.W.; Simonson, W.T.; Lisberg, A.; Ritter, D.; Morishima, C.; Hutchinson, K.; Mudgistratova, L.; Blom, A.; et al. Viral oncoprotein antibodies as a marker for recurrence of Merkel cell carcinoma: A prospective validation study. Cancer 2017, 123, 1464–1474. [Google Scholar] [CrossRef] [Green Version]
- Calzavara-Pinton, P.; Monari, P.; Manganoni, A.M.; Ungari, M.; Rossi, M.; Gualdi, G.; Venturini, M.; Sala, R. Merkel cell carcinoma arising in immunosuppressed patients treated with high-dose ultraviolet A1 (320–400 nm) phototherapy: A report of two cases. Photodermatol. Photoimmunol. Photomed. 2010, 26, 263–265. [Google Scholar] [CrossRef]
- Harms, P.W.; Collie, A.; Hovelson, D.H.; Cani, A.K.; Verhaegen, M.E.; Patel, R.M.; Fullen, D.R.; Omata, K.; Dlugosz, A.A.; Tomlins, S.A.; et al. Next generation sequencing of Cytokeratin 20-negative Merkel cell carcinoma reveals ultraviolet-signature mutations and recurrent TP53 and RB1 inactivation. Modern. Pathol. 2016, 29, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Mancebo, S.E.; Hu, J.Y.; Wang, S.Q. Sunscreens: A review of health benefits, regulations, and controversies. Dermatol. Clin. 2014, 32, 427–438. [Google Scholar] [CrossRef]
- Samimi, M.; Touzé, A.; Laude, H.; Le Bidre, E.; Arnold, F.; Carpentier, A.; Gardair, C.; Carlotti, A.; Maubec, E.; Dupin, N.; et al. Vitamin D deficiency is associated with greater tumor size and poorer outcome in Merkel cell carcinoma patients. J. Eur. Acad Dermatol. Venereol. 2014, 28, 298–308. [Google Scholar] [CrossRef]
- Sahi, H.; Koljonen, V.; Böhling, T.; Neuvonen, P.J.; Vainio, H.; Lamminpää, A.; Kyyrönen, P.; Pukkala, E. Increased incidence of Merkel cell carcinoma among younger statin users. Cancer Epidemiol. 2012, 36, 421–424. [Google Scholar] [CrossRef]
- Lebbe, C.; Becker, J.C.; Grob, J.J.; Malvehy, J.; Del Marmol, V.; Pehamberger, H.; Peris, K.; Saiag, P.; Middleton, M.R.; Bastholt, L.; et al. Diagnosis and treatment of Merkel Cell Carcinoma. European consensus-based interdisciplinary guideline. Eur. J. Cancer 2015, 51, 2396–2403. [Google Scholar] [CrossRef]
- Ellis, D.L.; Davis, R.S. Evidence-based management of primary and localized Merkel cell carcinoma: A review. Int. J. Dermatol. 2013, 52, 1248–1258. [Google Scholar] [CrossRef]
- Kline, L.; Coldiron, B. Mohs micrographic surgery for the treatment of Merkel cell carcinoma. Dermatol. Surg. 2016, 42, 945–951. [Google Scholar] [CrossRef]
- Terushkin, V.; Brodland, D.G.; Sharon, D.J.; Zitelli, J.A. Mohs surgery for early-stage Merkel cell carcinoma (MCC) achieves local control better than wide local excision ± radiation therapy with no increase in MCC-specific death. Int. J. Dermatol. 2021, 60, 1010–1012. [Google Scholar] [CrossRef]
- Gunaratne, D.A.; Howle, J.R.; Veness, M.J. Sentinel lymph node biopsy in Merkel cell carcinoma: A 15-year institutional experience and statistical analysis of 721 reported cases. Br. J. Dermatol. 2016, 174, 273–281. [Google Scholar] [CrossRef]
- Bhatia, S.; Storer, B.E.; Iyer, J.G.; Moshiri, A.; Parvathaneni, U.; Byrd, D.; Sober, A.J.; Sondak, V.K.; Gershenwald, J.E.; Nghiem, P. Adjuvant radiation therapy and chemotherapy in Merkel cell carcinoma: Survival analyses of 6908 cases from the National Cancer Data Base. J. Natl. Cancer. Inst. 2016, 108, djw042. [Google Scholar] [CrossRef] [Green Version]
- Nugent, S.T.; Lukowiak, T.M.; Cheng, B.; Stull, C.; Miller, C.J.; Aizman, L.; Perz, A.M.; Etzkorn, J.; Sobanko, J.F.; Shin, T.M.; et al. High compliance with National Comprehensive Cancer Network guidelines and no local recurrences for patients receiving Mohs micrographic surgery for Merkel cell carcinoma: A single-center retrospective case series. J. Am. Acad Dermatol. 2022. [Google Scholar] [CrossRef]
- Veness, M.; Howle, J. Radiotherapy alone in patients with Merkel cell carcinoma: The Westmead Hospital experience of 41 patients. Australas. J. Dermatol. 2015, 56, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Iyer, J.G.; Parvathaneni, U.; Gooley, T.; Miller, N.J.; Markowitz, E.; Blom, A.; Lewis, C.W.; Doumani, R.F.; Parvathaneni, K.; Anderson, A.; et al. Single-fraction radiation therapy in patients with metastatic Merkel cell carcinoma. Cancer. Med. 2015, 4, 1161–1170. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, P.; Kaufman, H.L.; Bharmal, M.; Mahnke, L.; Phatak, H.; Becker, J.C. Systematic literature review of efficacy, safety and tolerability outcomes of chemotherapy regimens in patients with metastatic Merkel cell carcinoma. Future. Oncol. 2017, 13, 1263–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voog, E.; Biron, P.; Martin, J.P.; Blay, J.Y. Chemotherapy for patients with locally advanced or metastatic Merkel cell carcinoma. Cancer 1999, 85, 2589–2595. [Google Scholar] [CrossRef]
- Tello, T.L.; Coggshall, K.; Yom, S.S.; Siegrid, S.Y. Merkel cell carcinoma: An update and review: Current and future therapy. J. Am. Acad Dermatol. 2018, 78, 445–454. [Google Scholar] [CrossRef]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune checkpoint blockade: A common denominator approach to cancer therapy. Cancer Cell. 2015, 27, 450–461. [Google Scholar] [CrossRef] [Green Version]
- Lyngaa, R.; Pedersen, N.W.; Schrama, D.; Thrue, C.A.; Ibrani, D.; Met, Ö.; Nghiem, P.; Becker, J.C.; Hadrup, S.R. T-cell Responses to Oncogenic Merkel Cell Polyomavirus Proteins Distinguish Patients with Merkel Cell Carcinoma from Healthy DonorsT-cell Epitopes in MCPyV-Encoded Proteins. Clin. Cancer Res. 2014, 20, 1768–1778. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, H.L.; Russell, J.S.; Hamid, O.; Bhatia, S.; Terheyden, P.; D’Angelo, S.P.; Shih, K.C.; Lebbé, C.; Milella, M.; Brownell, I.; et al. Updated efficacy of avelumab in patients with previously treated metastatic Merkel cell carcinoma after ≥1 year of follow-up: JAVELIN Merkel 200, a phase 2 clinical trial. J. Immunother. Cancer 2018, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, S.; Lebbé, C.; Mortier, L.; Brohl, A.; Fazio, N.; Grob, J.J.; Prinzi, N.; Hanna, G.; Hassel, J.; Kiecker, F.; et al. 604 First-line avelumab treatment in patients with metastatic Merkel cell carcinoma: 4-year follow-up from the JAVELIN Merkel 200 trial. J. Immunother. Cancer 2022, 10, 604. [Google Scholar]
- Walker, J.W.; Lebbé, C.; Grignani, G.; Nathan, P.; Dirix, L.; Fenig, E.; Ascierto, P.A.; Sandhu, S.; Munhoz, R.; Benincasa, E.; et al. Efficacy and safety of avelumab treatment in patients with metastatic Merkel cell carcinoma: Experience from a global expanded access program. J. Immunother. Cancer 2020, 8, e000313. [Google Scholar] [CrossRef] [Green Version]
- Topalian, S.L.; Bhatia, S.; Hollebecque, A.; Awada, A.; Boer, J.P.; Kudchadkar, R.R.; Goncalves, A.; Delord, J.P.; Martens, U.M.; Picazo, J.M.; et al. Abstract CT074, Non-comparative, open-label, multiple cohort, phase 1/2 study to evaluate nivolumab (NIVO) in patients with virus-associated tumors (CheckMate 358): Efficacy and safety in Merkel cell carcinoma (MCC). Cancer Res. 2017, 77, CT074. [Google Scholar] [CrossRef]
- Becker, J.C.; Hassel, J.C.; Menzer, C.; Kähler, K.C.; Eigentler, T.K.; Meier, F.E.; Berking, C.; Gutzmer, R.; Mohr, P.; Kiecker, F.; et al. Adjuvant ipilimumab compared with observation in completely resected Merkel cell carcinoma (ADMEC): A randomized, multicenter DeCOG/ADO study. J. Clin. Oncol. 2018, 36, 9527. [Google Scholar] [CrossRef]
- Topalian, S.L.; Bhatia, S.; Amin, A.; Kudchadkar, R.R.; Sharfman, W.H.; Lebbé, C.; Delord, J.P.; Dunn, L.A.; Shinohara, M.M.; Kulikauskas, R.; et al. Neoadjuvant nivolumab for patients with resectable Merkel cell carcinoma in the CheckMate 358 trial. J. Clin. Oncol. 2020, 38, 2476–2487. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s), Country of Report, Journal and Year of Publication | Age (Years) and Sex of Patient(s) | Previous Malignancies | Post-Transplant Immunosuppression Received | Location and Spread of MCC | Time from Transplantation to MCC Diagnosis | Treatment Received | Clinical Outcome |
|---|---|---|---|---|---|---|---|
| Formica et al., Italy Nephron, 1994 [74] | 54, Male | Prostatic highly differentiated in situ adenocarcinoma | Prednisolone Cyclosporine A | Chest Skin Region, Contralateral supraclavicular lymph node metastases, Left subcostal area MCC | 3 years | Regional Lymphadenectomy followed by radiotherapy; Eventual tapering of immunosuppressant dose as disease spread increases | Not specified |
| Douds et al., United Kingdom Nephrol. Dial. Transplant., 1995 [75] | 67, Male | Nil | Prednisolone Cyclosporine A | Upper Left Thigh Skin Region Metastatic MCC at the mediastinum | 2 years | Wide surgical Excision followed by radiotherapy initially; Further radiotherapy given when metastatic MCC diagnosed | Passed away 2 weeks following diagnosis of large mediastinal mass suggestive of metastatic MCC |
| Gooptu et al., United Kingdom Br. J. Dermatol. 1997 [76] | Case 1: 56, Female Case 2: 55, Male | Case 1: Nil Case 2: Numerous episodes of Squamous Cell Carcinoma post-transplant | Case 1: Cyclosporine, Azathioprine Case 2: Cyclosporine, Azathioprine | Case 1: Skin area over left shin and enlarged lymph node at left groin. Pelvic and para-aortic lymphadenopathy confirmed Case 2: Skin area at back of neck initially, axillary and cervical lymphadenopathy prior to spine and brain metastases | Case 1: 4 years Case 2: 15 years | Case 1: Six courses of chemotherapy (etoposide and vincristine) Case 2: Surgical excision followed by radiotherapy | Case 1: Patient died 1 year after presentation Case 2: Patient died 6 months after presentation |
| Williams et al., United States Transplantation, 1998 [77] | 65, Male | Nil | Prednisolone Cyclosporine Azathioprine | Left lower back Skin Region | 6 years | Wide surgical Excision followed by radiotherapy and two cycles of chemotherapy (carboplatin and etoposide); Modification of immunosuppression regime to Prednisolone and Cyclosporine only | At 13 months after treatment, the patient continued to be in good health, without evidence of either allograft rejection or MCC recurrence |
| Urbatsch et al., United States J. Am. Acad. Dermatol., 1999 [78] | Case 1: 40, Male Case 2: 48, Male Case 3: 60, Male | Case 1: SCC in upper extremities, neck, back and face Case 2: Multiple BCC and SCCs of arms and neck Case 3: Multiple BCC and SCCs in various sites | Case 1: Prednisolone Cyclosporine Azathioprine Case 2: Prednisolone Cyclosporine Azathioprine Case 3: Prednisolone Cyclosporine | Case 1: Skin area of right parotid gland Case 2: Skin area of AV fistula at right arm. SCC overlying MCC at this site. Right axillary lymphadenopathy found Case 3: Skin area over left forearm. Left axillary lymphadenopathy suggestive of metastatic MCC | Case 1: 3 years Case 2: 4 years Case 3: 7 years | Case 1: Radiotherapy to affected areas administered Case 2: Wide surgical excisions and right axillary lymphadenectomy, prior to radiotherapy and 3 cycles of chemotherapy (cyclophosphamide, Adriamycin and Vincristine) Case 3: Wide surgical excision initially performed to excise lesion. Due to metastatic spread, patient referred to oncology. Radiotherapy and Chemotherapy deemed unsuitable, for palliative treatment | Case 1: Achieved remission. No evidence of recurrence Case 2: Achieved remission. No evidence of recurrence Case 3: Not specified |
| Silvestris et al., Italy J. Exp. Clin. Cancer Res., 2000 [79] | 90, Female | Resected Colorectal Cancer | Prednisolone | Skin area over the left anterior thigh. Sentinel lymph node biopsy negative. | Not specified | Wide surgical excision performed. Patient declined post-operative radiotherapy | 6 months follow-up did reveal patient was in remission, with no MCC recurrence |
| Bartsch et al., Germany Pathologe, 2002 [80] | 59, Male | Post-transplant urinary bladder adenocarcinoma Multiple metachronic pre-/neoplastic skin lesions | Prednisolone Cyclosporine | Skin area over the Left Auricular Helix | 27 years | Surgical treatment of lesion was performed, but patient died 6 months later before further treatment could be initiated | Patient died of hematogenous spread of MCC 6 months following surgical excision of MCC lesion |
| Morris et al., Australia Br. J. Haematol., 2005 [81] | 72, Male | Not specified | Prednisolone Cyclosporine Mycophenolate Mofetil | Skin area over Right Shoulder with Right Axillary Lymphadenopathy | 4 years | Surgical excision of primary lesion. By the time metastatic MCC was identified, the patient was considered for palliative chemotherapy | Patient died before palliative chemotherapy was instituted |
| Bucci et al., United States J. Resid. Dermatol., 2006 [82] | 55, Male | Multiple SCCs | Not specified. MCC diagnosed 4 weeks after kidney transplantation | Skin area over Central Forehead, with multiple satellite nodules and spread to right cheek and metastatic disease to head and neck regions | 4 weeks | Mohs micrographic surgery was initially performed to clear tumor burden, and the patient also went through bilateral, radical neck dissections | Tumor recurrence occurred months after initial resection and lymph node dissection. Disease advanced quickly and the patient died 6 months following diagnosis |
| Ferreira et al., Portugal Eur. J. Plastic Surg., 2006 [83] | 72, Female | Forehead BCC removed 8 months prior to MCC presentation | Prednisolone Cyclosporine Azathioprine | Primary lesion over the Medial Canthus of the Right and Left Eyes. Stage II lymphatic and distant metastasis was identified initially, before liver metastases was found | 11 years | Surgical removal to the level of the periosteum of the nasal bone initially. Plan for adjuvant radiotherapy and chemotherapy following diagnosis of liver metastases | Rapid clinical deterioration with advancing liver metastases before radiotherapy and chemotherapy could be initiated. Patient died 10 months following initial diagnosis |
| Kanitakis et al., France J. Cutan. Pathol., 2006 [84] | 47, Male | Nil | Steroids Cyclosporine | Skin area over Left Shoulder. Patient also had an atypical lentiginous junctional nevus of the chest | 5 years | Lesion surgically excised. Progressive discontinuation of immunosuppression medications | Achieved remission, but patient developed chronic graft rejection and therefore required HD. Lost to follow-up |
| Lau et al., China (Hong Kong) Pathology, 2006 [85] | 57, Female | Nil | Prednisolone Cyclosporine A | Skin area over Right Temporal Region. Later developed two enlarged lymph nodes over the ipsilateral Head and Neck region, one over the preauricular region and one over level II of the Cervical lymphatic chain | 7 years | Wide local clear excision of the primary lesion was performed, followed by fine needle biopsy of the enlarged lymph nodes. Further treatment received, if any, was not specified. | Not specified |
| Kaisar et al., Australia Nephrology (Carlton), 2007 [86] | 67, Female | Frequent occurrences of SCC and BCC post-transplant | Prednisolone Cyclophosphamide | No primary skin lesions detected, axillary lymphadenopathy and Hepatic metastases identified from initial diagnosis | 6 years | Patient opted for palliation due to the extent of metastatic disease | Died soon after diagnosis |
| Kurnatowska et al., Poland Ann. Transplant., 2010 [87] | 62, Male | Nil | Prednisolone Cyclosporine A | Primary lesion at the buttock, eventually developing disseminating skin lesions and multiple metastases | 5 years | Surgical excision of lesions and adjuvant radiotherapy received. Switch from Cyclosporine A to mTOR inhibitor | Patient eventually died due to advancement of disease with multiple metastases |
| Krejci et al., Czech Republic Onkologie, 2010 [88] | 62, Male | Nil | Prednisolone Tacrolimus Mycophenolate Mofetil | Skin area over Right Gluteal Region, eventual inguinal lymph node spread and Head of Pancreas metastasis | 8 years | Wide surgical excision of initial skin lesion, and sentinel lymph node biopsy/lymph node dissection performed. Adjuvant radiotherapy given. Immunosuppressive regime was adjusted (Mycophenolate Mofetil was discontinued, and Tacrolimus treatment was changed to Sirolimus with a low dose of prednisone). 3 cycles of chemotherapy (doxorubicin and cyclophosphamide) were administered when metastatic disease was identified | Patient died of complicating obstructive ileus caused by the tumor mass and pneumonia 9 months after the primary diagnosis. |
| Singh et al., United States Transplantation, 2019 [89] | 71, Female | Nil | Anti-thymoglobulin Glucocorticoid Tacrolimus Mycophenolate Mofetil | Skin area over Left Neck, with MCC then metastasizing to Liver and Spine | 12 years | Initially underwent left lateral neck dissection and radiotherapy. Adjustment of immunosuppression regime (discontinued Tacrolimus, halved Mycophenolate Mofetil dose, and reduced Prednisolone dose to 5mg/day). Eventual commencement on PD-1 therapy (Nivolumab) with 13 cycles of treatment | Significant improvement in quality of life outcomes after commencement of PD-1 therapy. No further progression of MCC and kidney function was stabilized |
| Brystrup Boyles et al., Denmark Acta Oncologica, 2020 [90] | 72, Female | Not specified | Not specified, though noted patient was on long-term immunosuppressive therapy | Primary lesion is arm. AJCC IV grade MCC noted, though area affected by metastases not specified | Not specified | PD-1 therapy (Pembrolizumab) administered as first-line treatment for MCC | Had stable disease and partial response whilst receiving Pembrolizumab, but this was discontinued after four doses and disease progressed again. Mortality outcome not specified. |
| Rizzo et al., United States JAAD Case Rep., 2021 [91] | 48, Male | Not specified | Not specified, though noted patient was on immunosuppressive therapy | Primary lesion over skin area in Right Groin, leading to Right Groin Adenopathy. Liver and then brain metastases eventually diagnosed | Not specified | Treated with chemotherapy (carboplatin and etoposide) followed by PD-1 therapy (Pembrolizumab). When brain metastases were identified, stereotactic surgery was performed and the patient then continued with Pembrolizumab | The patient’s condition deteriorated despite active and aggressive treatment. He was transitioned into hospice care and died of the disease 9 months following diagnosis |
| Wu et al., United Kingdom Kidney360 2021 [92] | 64, Female | Not specified | Not specified, though noted patient was on immunosuppressive therapy | Primary lesion over skin area over Right Anteromedial Thigh. Metastases to the right transplanted kidney was identified | 10 years | Palliative care as patient deemed unsuitable for immunotherapy treatment | Patient passed away during the same hospital admission in which the diagnosis was made |
| PD-1/PD-L1 Inhibitor | Current Developments |
|---|---|
| Avelumab [31,140,141,142] |
|
| Pembrolizumab [32] |
|
| Nivolumab [143] |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, H.H.L.; Pye, I.; Chinnadurai, R. Merkel Cell Carcinoma in Kidney Transplant Recipients. Dermato 2023, 3, 25-50. https://doi.org/10.3390/dermato3010003
Wu HHL, Pye I, Chinnadurai R. Merkel Cell Carcinoma in Kidney Transplant Recipients. Dermato. 2023; 3(1):25-50. https://doi.org/10.3390/dermato3010003
Chicago/Turabian StyleWu, Henry H. L., Isobel Pye, and Rajkumar Chinnadurai. 2023. "Merkel Cell Carcinoma in Kidney Transplant Recipients" Dermato 3, no. 1: 25-50. https://doi.org/10.3390/dermato3010003