
First Onset of Pityriasis Rubra Pilaris following SARS-CoV-2 Booster Vaccination: Case Report and Review of the Literature

 ,
,  ,
,
Abstract
:1. Introduction
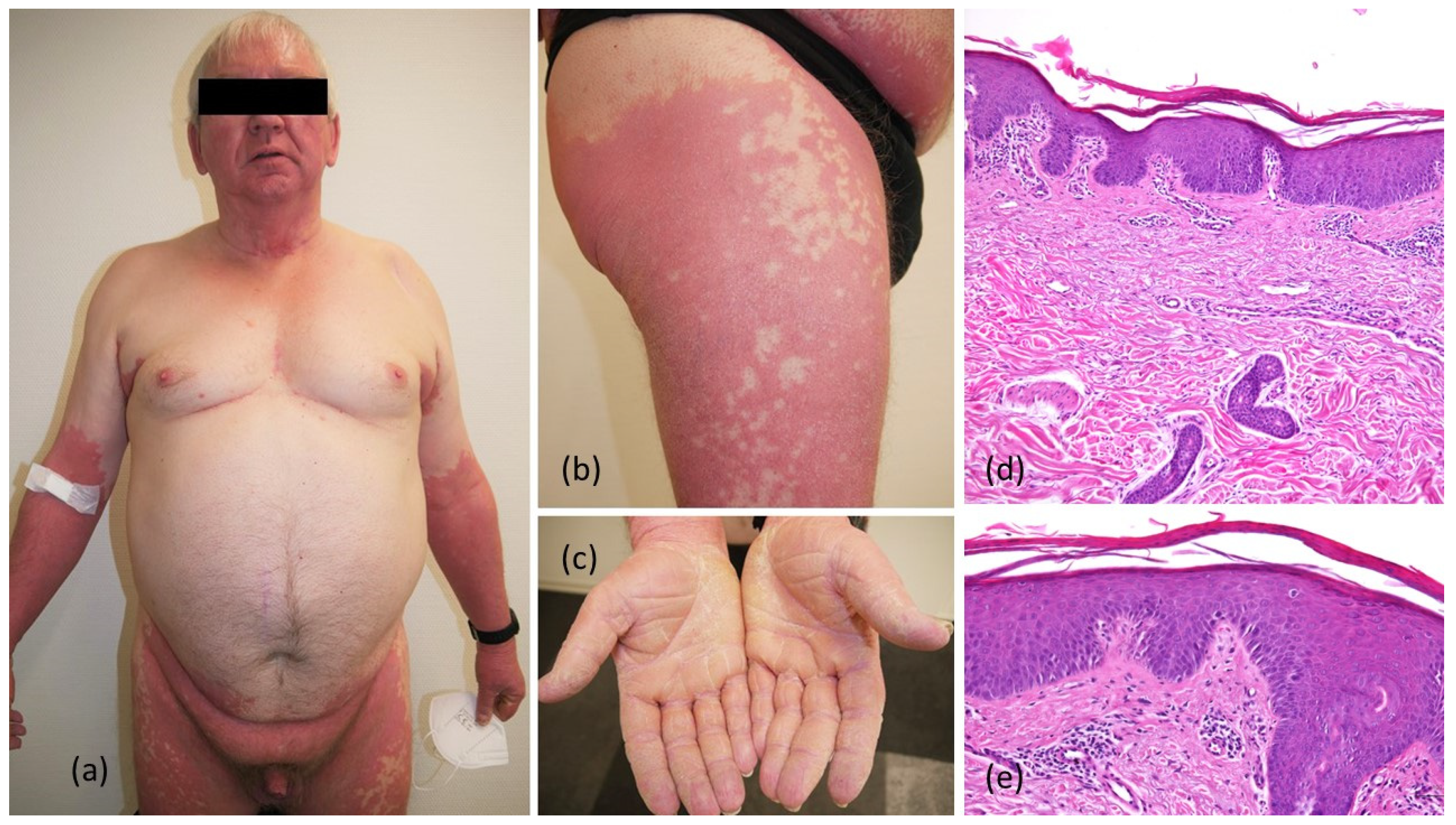
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gambichler, T.; Boms, S.; Susok, L.; Dickel, H.; Finis, C.; Abu Rached, N.; Barras, M.; Stücker, M.; Kasakovski, D. Cutaneous findings following COVID-19 vaccination: Review of world literature and own experience. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.W.; Tam, Y.C.; Oh, C.C. Skin manifestations of COVID-19: A worldwide review. JAAD Int. 2021, 2, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Chong, V.C.; Chong, W.S.; Oon, H.H. A Review on Pityriasis Rubra Pilaris. Am. J. Clin. Dermatol. 2018, 19, 377–390. [Google Scholar] [CrossRef]
- Ajebo, E.M.; Howard, J.D.; Anand, D.; Davis, L.S. Pityriasis rubra pilaris potentially triggered by messenger RNA-1273 COVID vaccine. JAAD Case Rep. 2022, 23, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Scheel, C.H.; Arafat, Y.; Kautz, O.; Boms, S. Erythrodermic pityriasis rubra pilaris after SASRS-CoV-2 vaccination with concomitant COVID-19 infection. J. Eur. Acad. Dermatol. Venereol. 2022. [Google Scholar] [CrossRef]
- Wada, M.; Lee, S.; Curnow, P.; Simpson, I.; Mar, A. A case of pityriasis rubra pilaris following AstraZeneca COVID-19 vaccine. JAAD Case Rep. 2022, 24, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Fernández, L.T.; Pérez-Garza, D.M.; delaO-Escamilla, A.; Yamallel-Ortega, L.A.; Cuellar-Barboza, A.; Ocampo-Candiani, J.; Chavez-Alvarez, S. Pityriasis rubra pilaris in association with inactivated SARS-CoV-2 vaccine (CoronaVac). Dermatol. Ther. 2022, 35, e15455. [Google Scholar] [CrossRef]
- Bramhoff, A.C.; Wesselmann, U.; Bender, S.T.; Berghoff, A.V.; Hofmann, S.C.; Balakirski, G. Pityriasis rubra pilaris nach COVID-19-Impfung: Kausaler Zusammenhang oder Koinzidenz? [Pityriasis rubra pilaris after COVID-19 vaccination: Causal relationship or coincidence?]. Der Hautarzt 2022. (In Germany) [Google Scholar] [CrossRef]
- Criado, P.R.; Ianhez, M.; Rocha, P.S.; Miot, H.A. Pityriasis rubra pilaris (type I) following ChAdOx1 COVID-19 vaccine: A report of two cases with successful treatment with oral isotretinoin. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e508–e510. [Google Scholar] [CrossRef]
- Sechi, A.; Pierobon, E.; Pezzolo, E.; Germi, L.; Trevisan, G.; Zardo, D.; Riva, G.; Mondino, S.; Naldi, L. Abrupt onset of Sweet syndrome, pityriasis rubra pilaris, pityriasis lichenoides et varioliformis acuta and erythema multiforme: Unravelling a possible common trigger, the COVID-19 vaccine. Clin. Exp. Dermatol. 2022, 47, 437–440. [Google Scholar] [CrossRef]
- Sahni, M.K.; Roy, K.; Asati, D.P.; Khurana, U. An old entity, a new trigger: Post COVID-19 vaccine pityriasis rubra pilaris. Int. J. Risk Saf. Med. 2021, 32, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Hunjan, M.K.; Roberts, C.; Karim, S.; Hague, J. Pityriasis rubra pilaris-like eruption following administration of the BNT163b2 (Pfizer-BioNTech) mRNA COVID-19 vaccine. Clin. Exp. Dermatol. 2022, 47, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Lladó, I.; Butrón, B.; Sampedro-Ruiz, R.; Fraga, J.; de Argila, D. Pityriasis rubra pilaris after Vaxzevria® COVID-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e833–e835. [Google Scholar] [CrossRef] [PubMed]
- Peña-Rosado, A.; Riera-Martí, N.; Expósito-Serrano, V.; Romaní, J. Autoinflammatory keratinitzation diseases (AIKDs. Actas Dermosifiliogr (Engl. Ed.) 2021, 112, 891–900. [Google Scholar] [CrossRef]
- Akiyama, M. Autoinflammatory Keratinization Diseases (AiKDs): Expansion of Disorders to Be Included. Front. Immunol. 2020, 11, 280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, M.; Belhadjali, H.; Hammedi, F.; Ben Meriem, C.; Zili, J. Pityriasis rubra pilaris occurring after vaccination with diphtheria-pertussis-tetanus and oral poliovirus vaccines. Indian J. Dermatol. Venereol. Leprol. 2015, 81, 618–620. [Google Scholar] [CrossRef] [PubMed]
- Naciri Bennani, B.; Cheikh Rouhou, H.; Waton, J.; Cuny, J.F.; Bassegoda, G.; Trechot, P.; Barbaud, A.; Schmutz, J.L. Pityriasis rubra pilaire après vaccination [Pityriasis rubra pilaris after vaccination]. Ann. Dermatol. Venereol. 2011, 138, 753–756. [Google Scholar] [CrossRef]
- Kadylak, D.; Barańska-Rybak, W. Acute postinfectious pityriasis rubra pilaris as a cutaneous manifestation in COVID-19: A case report and its dermoscopic features. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e622–e624. [Google Scholar] [CrossRef]
- Aguilar-Gamboa, F.R.; Cubas-Alarcon, D.; Villegas-Chiroque, M.; Failoc-Rojas, V.E. Pityriasis rubra pilaris post-infection due COVID-19: Case report. Colomb. Médica (Cali.) 2021, 52, e7014577. [Google Scholar] [CrossRef]
- Arora, A.; Mohta, A.; Ghiya, B.C.; Kumar Jangir, V. Acute postinfectious type III pityriasis rubra pilaris as a cutaneous manifestation in COVID-19: Decoding a possible trigger!! J. Cosmet. Dermatol. 2022. [Google Scholar] [CrossRef]
- Magro, C.; Crowson, A.N.; Franks, L.; Schaffer, P.R.; Whelan, P.; Nuovo, G. The histologic and molecular correlates of COVID-19 vaccine-induced changes in the skin. Clin. Dermatol. 2021, 39, 966–984. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.B.; Pham, N.T.U.; Phan, H.N.; Nguyen, H.T. Generalized erythrodermic psoriasis triggered by vaccination against severe acute respiratory syndrome Coronavirus 2. Dermatol. Ther. 2022, 35, e15464. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, K.; Kawakami, Y.; Tokuda, M.; Sato, S.; Sugihara, S.; Miyake, T.; Sugiura, K.; Morizane, S. Flare-up of generalized pustular psoriasis following Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine: Two cases without mutations of IL36RN and CARD14 genes. J. Dermatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Nagai, H.; Jimbo, H.; Matsuura, S.; Tatsuoka, S.; Shiraki, E.; Nishigori, C. Successful treatment of pityriasis rubra pilaris with guselkumab: Serum CCL20 as a potential marker for the disease activity. Dermatol. Ther. 2020, 33, e14403. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, A.; Gambardella, A.; Licata, G.; Alfano, R.; Argenziano, G. Successful treatment of Pityriasis rubra pilaris with brodalumab. Australas. J. Dermatol. 2020, 61, e249–e251. [Google Scholar] [CrossRef] [PubMed]
- Langley, R.G.; Tsai, T.F.; Flavin, S.; Song, M.; Randazzo, B.; Wasfi, Y.; Jiang, J.; Li, S.; Puig, L. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: Results of the randomized, double-blind, phase III NAVIGATE trial. Br. J. Dermatol. 2018, 178, 114–123. [Google Scholar] [CrossRef] [Green Version]
- Ross, N.A.; Chung, H.J.; Li, Q.; Andrews, J.P.; Keller, M.S.; Uitto, J. Epidemiologic, Clinicopathologic, Diagnostic, and Management Challenges of Pityriasis Rubra Pilaris: A Case Series of 100 Patients. JAMA Dermatol. 2016, 152, 670–675. [Google Scholar] [CrossRef] [Green Version]
- Ricar, J.; Cetkovska, P. Successful treatment of refractory extensive pityriasis rubra pilaris with risankizumab. Br. J. Dermatol. 2021, 184, e148. [Google Scholar] [CrossRef]
- Napolitano, M.; Abeni, D.; Didona, B. Biologics for pityriasis rubra pilaris treatment: A review of the literature. J. Am. Acad. Dermatol. 2018, 79, 353–359.e11. [Google Scholar] [CrossRef]
- Haynes, D.; Strunck, J.L.; Topham, C.A.; Ortega-Loayza, A.G.; Kent, G.; Cassidy, P.B.; Hu, R.; Choate, K.; Wang, Z.; Liu, Y.; et al. Evaluation of Ixekizumab Treatment for Patients With Pityriasis Rubra Pilaris: A Single-Arm Trial. JAMA Dermatol. 2020, 156, 668–675. [Google Scholar] [CrossRef]


{kind=link}
| Patients (Present Case) | Gender | Age (Years) | SARS-CoV-2 Vaccine | PRP Onset Following (Dose) | Onset of PRP after Vaccination (Days) | Re-Exposed to SARS-CoV-2 Vaccines | Systemic Treatment |
|---|---|---|---|---|---|---|---|
| #1 | m | 67 | Comirnaty/Pfizer-BioNTech, 1st 2nd Vaxzevria/AstraZeneca | 3rd | 14 | - | brodalumab, risankizumab, ustekinumab |
| #2 [4] | m | 75 | Spikevax/Moderna | 1st | 5 | yes, exacerbation | acitretin, guselkumab |
| #3 [5] | m | 51 | Spikevax/Moderna, 1st Vaxzevria/AstraZeneca, 2nd Comirnaty/Pfizer- BioNTech (concomittant COVID-19 infection) | 3rd | 10 | - | guselkumab |
| #4 [6] | m | 65 | Vaxzevria/AstraZeneca | 1st | 60 | - | acitretin |
| #5 [7] | m | 59 | CoronaVac/Sinovac | 2nd | 4 | - | none * |
| #6 [7] | m | 56 | CoronaVac/Sinovac | 2nd | 30 | - | none * |
| #7 [8] | m | 50 | Vaxzevria/AstraZeneca | 1st | 9 | yes, no exacerbation | acitretin |
| #8 [8] | m | 58 | Comirnaty/Pfizer-BioNTech | 2nd | 20 | - | corticosteroids, allotretinoin |
| #9 [8] | f | 60 | Vaxzevria/AstraZeneca | 1st | 30 | yes, no exacerbation | acitretin, methotrexate |
| #10 [9] | m | 31 | Vaxzevria/AstraZeneca | 1st | 15 | - | isotretinoin |
| #11 [9] | m | 42 | Vaxzevria/AstraZeneca | 2nd | 8 | - | isotretinoin |
| #12 [10] | f | 62 | Spikevax/Moderna | 1st | 5 | - | corticosteroids |
| #13 [10] | f | 82 | Comirnaty/Pfizer-BioNTech | 1st | 7 | - | methotrexate |
| #14 [11] | m | 72 | Covishield/AstraZeneca | 1st | 21 | yes, no exacerbation | none * |
| #15 [12] | m | 51 | Comirnaty/Pfizer-BioNTech | 1st | 3 | yes, exacerbation | acitretin |
| #16 [13] | f | 63 | Vaxzevria/AstraZeneca | 1st | 9 | - | acitretin |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambichler, T.; Scheel, C.H.; Arafat, Y.; Heinzer, E.; Noldes, K.; Bulic, Z.; Boms, S. First Onset of Pityriasis Rubra Pilaris following SARS-CoV-2 Booster Vaccination: Case Report and Review of the Literature. Dermato 2022, 2, 73-78. https://doi.org/10.3390/dermato2030008
Gambichler T, Scheel CH, Arafat Y, Heinzer E, Noldes K, Bulic Z, Boms S. First Onset of Pityriasis Rubra Pilaris following SARS-CoV-2 Booster Vaccination: Case Report and Review of the Literature. Dermato. 2022; 2(3):73-78. https://doi.org/10.3390/dermato2030008
Chicago/Turabian StyleGambichler, Thilo, Christina H. Scheel, Yousef Arafat, Ekaterina Heinzer, Kathrin Noldes, Zenaida Bulic, and Stefanie Boms. 2022. "First Onset of Pityriasis Rubra Pilaris following SARS-CoV-2 Booster Vaccination: Case Report and Review of the Literature" Dermato 2, no. 3: 73-78. https://doi.org/10.3390/dermato2030008