
Recent Trends in the Integrated Management of Cutaneous Squamous Cell Carcinoma


Department of Dermatology, Saudi German Hospital and Clinic, Dubai P.O. Box 391093, United Arab Emirates
Dermato 2022, 2(3), 59-72; https://doi.org/10.3390/dermato2030007
Submission received: 25 May 2022
/
Revised: 17 June 2022
/
Accepted: 23 June 2022
/
Published: 28 June 2022
(This article belongs to the Special Issue Feature Review Papers in Dermato)
Abstract
:Cutaneous squamous cell carcinoma (cSCC) is one of the most prevalent neoplasms worldwide. Important risk factors for cSCC include sun exposure, immunosuppression, pale skin, and aging. White people are more likely to develop cSCC, and men are more affected than women. In advanced cases, surgery and/or radiotherapy are no longer effective. Due to a historical lack of treatment options, some medications have been used in these patients without sufficient recommendation. There is an urgent need to identify patients at an increased risk of recurrence and spread early for timely diagnosis and treatment. Despite extensive data on the high-risk features and prognostication, considerable variation remains globally regarding high-risk cSCC and the delivery of oncology services. The current comprehensive review evaluated and summarized contemporary knowledge of various management options for cSCC to simplify the integrated treatment plans.
1. Introduction
Despite the increasing prevalence of cutaneous squamous cell carcinoma (cSCC), global numbers remain underestimated [1,2]. In the last three decades, the incidence of cSCCs has increased from 50% to 300%, and their prevalence in European countries is projected to double by 2030 [3]. In the Caucasian population, the probability of having cSCC at any point in life is believed to be between 7% and 11% [4]. Five-year cure rates of typical indolent cSCC are >90%. Advanced cSCC is defined as locally advanced or distant cSCC. Metastatic cSCC is a very small part (3–5%) of cSCC [5]. cSCC still carries a considerable burden on overall mortality due to its high frequency [6]. After melanoma, it is the most prevalent cause of skin cancer death, accounting for most skin cancer deaths in individuals aged >85 years [7]. The mechanisms of spread include “shelving” or “skating” along fascial planes (e.g., perichondrium, periosteum, muscle fascia), arteries, or nerves and spreading via lymphatic or hematogenous systems. Most cSCCs occur in the head and neck. Following the typical spread pattern, it commonly involves the ipsilateral submandibular and submental nodes, the parotid gland, and the intraparotid nodes [8].
The majority of cSCCs develop in the sun-damaged skin of older adults with white European ancestry, often in the context of preexisting actinic keratosis lesions. Apart from ultraviolet (UV) radiation exposure, other predisposing factors include chronic immunosuppressed states, chronic skin conditions, exposure to ionizing radiation, inherited genetic conditions, human papillomavirus infection, chronic arsenic exposure, and treatment with BRAF inhibitors (vemurafenib and dabrafenib), among others [9].
Treatment choices depend on the diagnosis and staging. cSCC is most commonly treated with surgery. Radiotherapy is often indicated. Systemic agents are beneficial in locally progressed and metastatic cSCC [10]. In recent decades, the increasing knowledge of the signaling pathways implicated in cSCC has propelled the evolution of novel targeted therapies. Modern immunotherapy has dramatically transformed treatment paradigms [11]. The current comprehensive literature review explores various management and clinical diagnostic options for cSCC to simplify the integrated treatment plans.
2. Histopathologic Subtypes
Keratoacanthoma and verrucous carcinoma are well-differentiated histologic subtypes that have a low propensity for spread. Keratoacanthomas are well-differentiated and usually appear dome-shaped with a radial keratin plug on light microscopy. The verrucous carcinoma subtypes include the Buschkee Lowenstein tumor in the perineum as well as epithelioma cuniculatum on the plantar surface of the foot. Verrucous carcinomas have an internal component with well-differentiated squamous epithelium and pushing boundaries [12]. The prognosis for a few histological cSCC subtypes is poor. Desmoplastic cSCC often invades, recurs, and spreads more frequently than other cSCC types [13]. Desmoplasia has been reported to be a predictor of local recurrence [14]. Another subtype with a high risk of regional recurrence, spread, and mortality is the adenosquamous variant, characterized by secretory tubular structures [15].
3. Clinical Diagnosis
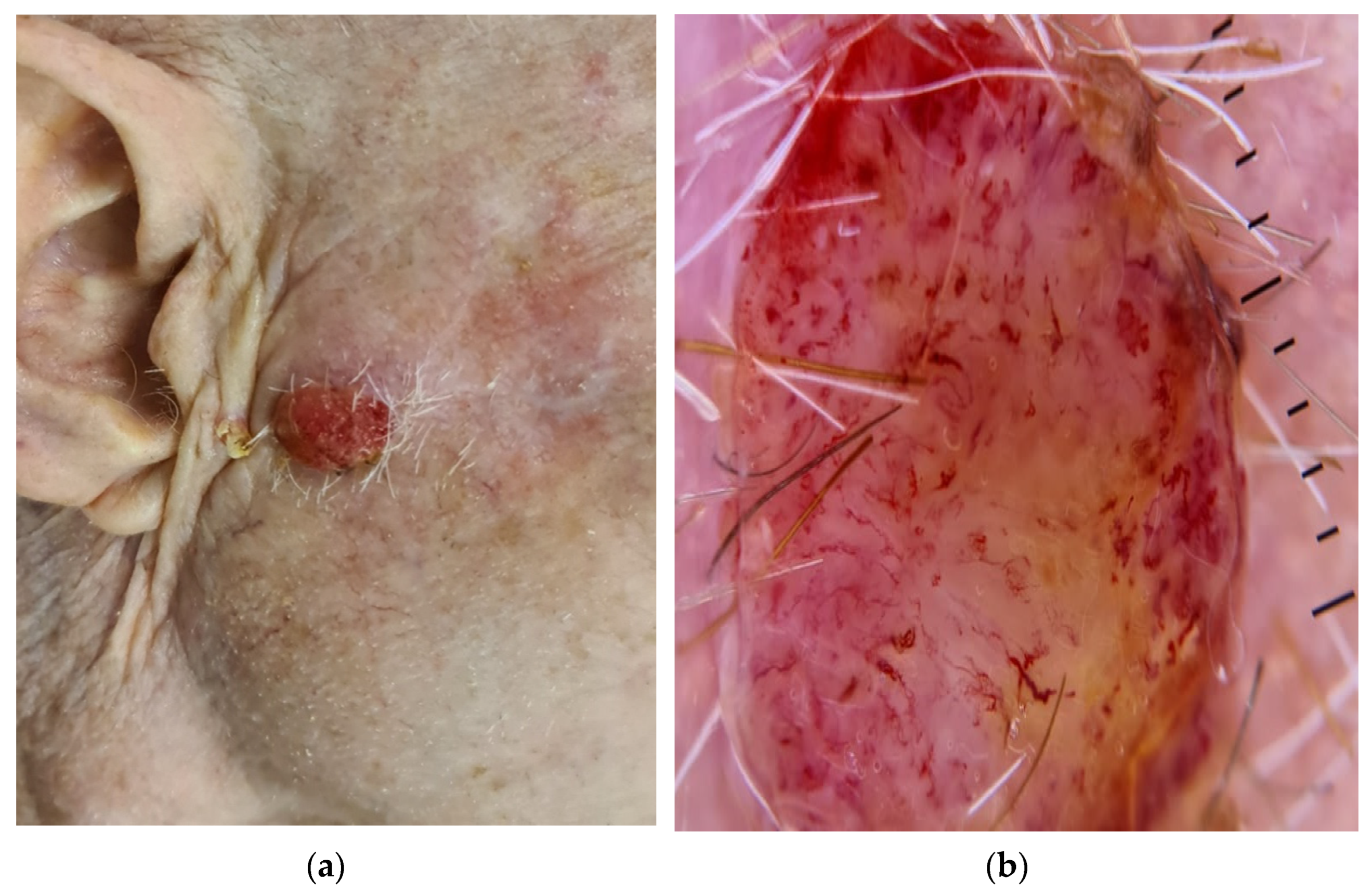
cSCC is most commonly found in chronically sun-exposed body areas. The lesions are described by tumor size, site, cutaneous classification, and pigmentation. In the early stages, the lesions are often small, light pink plaques with or without overlying scaly areas and induration. Gradually, these neoplasms tend to grow and ulcerate. The lesions then become pigmented, ranging from light brown to dark brown. Dermoscopic features, such as white rings, keratin, and blood spots, can help distinguish cSCC from other elevated cutaneous neoplasms (Figure 1) [16,17,18].
4. Risk Stratification and Staging of cSCC
Risk stratification of cSCC is a crucial step in the management based on clinical features and pathology features in biopsy [19] (Table 1). Tumors greater than 6 mm with the invasion of subcutaneous fat in microscopy are linked with a high risk of metastasis and local recurrence, which adversely affect the prognosis [14]. Formal staging and molecular pathology with biomarkers are also equally important [19].
Formal tumor staging of cSCC can be done by the American Joint Committee on Cancer (AJCC) classification 8 edition used for cSCC arising from the head and neck region. Another method for formal staging is Brigham and Women’s Hospital (BWH) classification [19]. Both stagings depend on the TNM classification of tumors [19]. A recent survey has demonstrated that dermatologists are more inclined to use BWH staging as advantages of BWH over AJCC staging were published in dermatology journals [20]. A system for cSCC staging and management using NCCN version 2021 has also allowed for a very high-risk category of risk stratification [20]. This category includes all features of the high-risk category and additionally includes >4 cm size of the tumor in any location [20].
Contemporary prognostic elements for recurrence, which will aid in identifying the role of standard or adjuvant treatments, are about clinicopathological aspects portrayed in clinical studies or consensus meetings. The high-risk characteristics are generally observed in approximately 5% of all non-melanoma skin cancers [21,22]. Radiological studies such as CT scan, MRI, ultrasound, and PET–CT can be employed when an extensive disease is suspected [19]. CT scan is advised when bone or lymph node disease is suspected or proven. Perineural spread, central nervous system spread, deep soft tissue spread, and bone marrow disease should be investigated with MRI. Ultrasonography has a role in cSCC to identify superficial lymph node disease and USG- guided FNA or biopsy. PET-CT can also investigate distant metastases, which has additional advantages of function information and differentiation between postoperative scar and recurrence [19]. Aggressive characteristics of metastatic cSCC lead to significant morbidity, escalated mortality, and individuals who require systemic treatments [5]. Metastatic cSCC and locally advanced cSCC occur more frequently (up to 35%) in high cSCCs [5].
The treatment of cSCC has long been a significant part of dermatologists’ clinical practice, and they are well-versed in the various therapeutic options available. Treatment choice depends primarily on risk stratification and formal staging. The diagnosis and treatment of cSCC among elderly adults with a short life expectancy has recently become a highly debated issue. This issue requires a clear differentiation between advanced age and reduced life expectancy, as they are not identical. Every dermatologist has seen robust, active nonagenarians who want and deserve to have their cSCC treated with a technique that offers the best cure rate and quality of life [23].
5. Management
5.1. Surgical Options
5.1.1. Excisional Surgery
Surgical excision is the most effective option for removing the tumor entirely. It is an outpatient procedure in low-risk cases with a faster recovery time. It allows for tissue histologic assessment and cure rates of up to 95% for some primary cSCCs [24]. The recommended free margin of normal skin is 6–10 mm for high-risk cSCC and 4–6 mm for low-risk cSCC [25,26]. To ensure complete tumor removal, extirpated specimens must be forwarded to an experienced surgical dermatopathologist for meticulous margin evaluation. For lesions with high-risk characteristics or those regarded as very high-risk, doctors recommend broader margins of at least 15 mm [27] to ensure complete tumor elimination. Such enormous margins are only possible in a few body regions with sufficient cutaneous laxity to tolerate such enormous defects. In addition, instead of routine surgical excision, high-risk tumors should be referred to Mohs surgeons for Mohs micrographic surgery (MMS), which allows for proven tumor removal without the requirement of extensive wide margins of normal cutaneous areas.
5.1.2. Mohs Micrographic Surgery
Mohs micrographic surgery (MMS) is a surgical procedure that enables a complete microscopic view of the tissue, the accurate determination of positive tumor margins, and total tumor clearance. Because surgical excision with negative margins is linked to considerably reduced recurrence rates, MMS is the benchmark for the surgical eradication of high-risk cSCC as it offers high cure rates and low recurrence rates [19,28,29]. MMS cure rates for primary cSCCs are 97%, and 94% for recurrent cSCCs [28,30]. Recent studies have demonstrated that MMS is highly effective in treating high-risk cSCCs and avoiding local recurrence [31,32]. A multidisciplinary team may be required to ensure total clearance in complex advanced cases with bony infiltration, parotid gland involvement, perineural spread, or metastases. MMS is a more precise and efficient method as compared with conventional surgical excision [33]. The fixed formalin paraffin embedded (FFPE) technique involves the storage of tissue samples to preserve tissue morphology and cellular integrity. Despite the usage of formalin, a toxic and time-consuming protocol that precludes the widespread application of the technique, the combination of MMS with FFPE provides more reliable results [34]. Restaging with data acquired by Mohs surgery is far superior to staging with biopsy data alone, as the surgeon performing the surgery can recognize high-risk features not identified on focal biopsy specimens [35]. Low-risk cases of cSCC can also be offered the option of MMS, where it is available after considering the cost. Patients of cSCC who undergo conventional surgical excision and in turn have positive margins can be referred to a Mohs surgeon for further surgical planning. If margins are positive on Mohs surgery, then this should be discussed in a multidisciplinary board meeting. If the perineural invasion is observed during MMS, then additional radiotherapy should be added to the post-operative care plan [19].
5.1.3. Sentinel Lymph Node Biopsy
Sentinel lymph node biopsy (SNLB) can potentially improve screening for metastasis, prognostication, and patient selection for early therapy and adjuvant clinical trials. However, most international standards do not endorse SNLB. In a meta-analysis of 19 studies, a positive sentinel lymph node was found in 12.3% of the 130 patients with cSCC who underwent SLNB, and the false-negative incidence was 2.6%. In those with a positive node, the primary cSCC diameter was >2 cm. Sentinel lymph nodes were negative in all nine patients with T1 lesions in whom the tumor had been confined to the mucosa (0%) as per American Joint Committee on Cancer (AJCC) criteria. Positive nodes were present in 3 of 5 patients with T4 lesions in whom the tumor had spanned through all layers of the tissue (60.0%), and in 13 of 116 patients with T2 lesions in whom the tumor had spread into the submucosa (11.2%). No patients with T3 lesions were enrolled in the study [36]. A recent systematic evaluation reported an SLNB positivity of 13.9% with a false-negative rate of 4.6% [17]. In another review of 23 studies with 566 patients examined, the proportion of patients with cSCC and positive SLNB was 8% [24], which was lower than that observed in previous analyses [36,37]. There were insufficient numbers of participants in the investigations to confidently establish the determinants of SLN positivity [38]. The actual clinical value of applying SLNB in patients with cSCC has not been clearly defined. In addition, information on the prognostic value of SNLB remains insufficient for recommending its routine use in patients with cSCC. Surgery could still be offered after a multidisciplinary consultation with a restricted group of patients. More effort should be made to identify the predictors of sentinel lymph node involvement for effective patient selection.
5.2. Targeted Therapies
5.2.1. PD-1 Inhibitors
Neoplastic cells can interact with some immune cells and alter their activity. Co-receptors operate as both activators and inhibitors of the host response when a host body identifies the antigen produced by the human leukocyte antigen (HLA) complex in the tumor cell [39]. cSCC has one of the most significant mutational defects of any cancer, making it a favorable candidate for immunotherapy [40]. Immune checkpoint inhibitors are effective against tumors with a high mutational burden [39,40]. The higher risk of cSCC in immunocompromised patients emphasizes the important role of the immune system in the growth of cSCC [41,42]. Therefore, clinical trials of these remedies for the treatment of cSCC have been conducted.
Immune checkpoint receptors include inhibitory receptors like programmed cell death 1 protein (PD-1) and cytotoxic T-lymphocyte antigen 4 (CTLA4). T-cells, B-cells, natural killer cells, monocytes, and dendritic cells express the inhibitor co-receptor PD-1 [43]. This transmembrane protein interacts with receptors on the surface of tumor cells, PD-L1 and PD-L2. Binding triggers a signal that suppresses active T-cells and results in immunological enervation via anergy and T-cell apoptosis [44,45]. Using monoclonal antibodies to target immunological checkpoint proteins has resulted in therapeutic benefits for cancer patients [46,47,48]. Proliferating cells and the tumor microenvironment make up an established tumor. Both the tumor stroma and the inflammatory infiltrate constitute the latter. To improve the immune response, most immune checkpoint inhibitors target lymphocytes in the TME [43,44,45,46,47,48,49].
The PD-L1/PD-1 axis is a fundamental modus operandi of malignant immune circumvention and has been the main concept behind developing novel treatments in recent years. PD-1 inhibitors have been developed for a variety of cancers. However, because of the limited response of cSCC to other systemic treatments, medications targeting this axis are effective in some patients [50,51]. These preliminary findings require a more thorough investigation of this approach and its possible therapeutic significance in cSCC. Surface PD-1/PD-L1 has been found in several malignancies. Its expression has been associated with poor clinical outcomes [52,53], including cSCC [54,55,56,57].
Cemiplimab was the first drug approved by the FDA and EMA to treat advanced cSCC. The FDA approved cemiplimab on 28 September 2018 for patients with metastatic cutaneous squamous cell carcinoma or locally advanced cutaneous squamous cell carcinoma [58]. Cemiplimab also received conditional marketing authorization for the same indications valid throughout the European Union on 28 June 2019 [59]. It is a PD-1-targeting human monoclonal antibody. It has been proven successful in immunocompetent patients with metastatic disease (RR 47%) and advanced cSCC (RR 50%) [58]. Cemiplimab is now being investigated as neoadjuvant therapy in patients with recurrent stage III-IV head and neck cSCC before surgery (NCT03565783) and as a preoperative intralesional injection in patients with recurrent cSCC (NCT03889912).
Pembrolizumab was also authorized by the FDA on 24 June 2020 for advanced cSCC as it showed encouraging clinical benefit and durable responses. Pembrolizumab efficacy was investigated in the KEYNOTE-629 trial, and it was approved for metastatic or recurrent cases of squamous cell carcinoma that are not curable by surgery or radiation [60]. Presently, immune checkpoint inhibitors are the standard of care in metastatic and locally advanced cSCC. Several clinical trials are also ongoing to manage advanced cases of cSCC with intra-lesional instillation of cemiplimab or in neoadjuvant or adjuvant scenarios after surgery and radiotherapy, as well as research on pembrolizumab. In culmination, the anti-PD1 agents cemiplimab and pembrolizumab are approved by the FDA for the treatment of advanced cSCC. Presently, immune checkpoint inhibitors are the standard of care in locally advanced and metastatic cSCC [58,59,60,61].
The most common adverse effects of immune checkpoint inhibitor (ICI) are diarrhea and fatigue, both of which are relatively minor adverse reactions. Immune checkpoint inhibitors are known to cause minor inflammation; therefore, in patients with pneumonitis, colitis, hepatitis, thyroiditis, or hypophysitis, it is necessary to take them carefully. These unwanted reactions can be severe in some instances, requiring termination. Dermatitis and pruritus are other possible side effects [62].
In addition to clinical trial evidence, multiple case reports of immunotherapy effectiveness in immunocompetent cSCC patients have been published [63,64,65,66]. The utilization of checkpoint inhibitors is an obstacle for transplant patients because increased T-cell activation can galvanize allograft rejection [67]. As transplant cases are frequently omitted from clinical studies, data are scarce, and only data from isolated cases are accessible [65,67,68].
On 21 January 2021, cemiplimab was removed from France’s list of reimbursable medicine specialties in view of the absence of phase III randomized trials demonstrating comparative or higher efficacy of cemiplimab versus other systemic treatments [69]. However, patient support programs are available in the United States of America. These programs assist eligible patients with medicine-related out-of-pocket expenses and reimbursements. They also provide cemiplimab free of cost to eligible patients who are uninsured [70]. Nonetheless, a research study has even observed that cemiplimab is a cost-effective use of payer resources for treating advanced cSCC and provides value for money from a healthcare payer’s outlook [71].
5.2.2. EGFR Inhibitors
EGFR inhibitors have been documented for advanced cSCC, with most trials focusing on cetuximab, which has a lot of heterogeneity and a small number of patients. Cetuximab can be used in combination with radiotherapy or chemotherapy [72]. Contemporary international clinical guidelines recommend cetuximab in cases that fail to respond to or have contraindications for immune checkpoint inhibitors [61]. EGFR has been identified as a key therapeutic target in various tumor types. Blocking EGFR signaling using monoclonal antibodies or small compounds is effective. In cSCC, EGFR expression is frequently dysregulated [73]. In contrast, gefitinib and other EGFR tyrosine kinase inhibitors have demonstrated only a limited therapeutic effect in patients with cSCC [74].
5.2.3. Cytotoxic Agents—Chemotherapy
Polychemotherapy with cytotoxic agents such as carboplatin, 5-fluorouracil, methotrexate, bleomycin, and gemcitabine have been employed as off-label chemotherapy in advanced cSCC. Recent guidelines state that these systemic chemotherapies can be used only in cases that fail to respond or are intolerant to anti-PD-1 immunotherapy [61].
5.2.4. Novel and Upcoming Treatment Agents and Targets in Development
Antibody-drug conjugates are a new type of anticancer treatment that combines the selectivity of targeted therapy with the deadly efficacy of chemotherapy medicines [75]. Another interesting way to target antigens is to go after cancer stem cells or tumor-initiating cells [76].
MicroRNAs (miRNAs) are a group of RNAs that have a crucial gene-regulatory role. Many studies have proved that dysregulation of these microRNAs is linked with developing many neoplasms. Flotillin-2 is an essential lipid raft component that is usually positively associated with oncogenesis. Nevertheless, a recent study has demonstrated that Flotillin-2 expression cSCC was low. In addition, Flotillin-2 is a direct target gene of microRNA. Flotillin-2 plays an anti-oncogenesis role in cSCC. MicroRNA miR-486-3P acts as an oncogene in cSCC through the mitigation of Flotillin-2. This is an exciting novel target for the treatment of cSCC [77].
5.3. Adjuvant Treatment for High-Risk Patients
Adjuvant treatment is recommended for high-risk cSCC because of recurrence, metastasis, and disease-specific mortality. While there are several alternatives for therapy before surgery, there is little agreement on the appropriate perioperative management [78]. For local or high-risk cSCC with negative margins, substantial perineural, more extensive, or identified nerve involvement or other high-risk characteristics, the National Comprehensive Cancer Network guidelines advocate for multidisciplinary consultation and adjuvant radiotherapy (RT). Its use is justified by the prospect of lowering the risk of local recurrences. In patients who have repeated excisions that are not feasible after surgical excision for cSCC with positive margins, European guidelines propose postoperative RT [79]. According to a previous study, the benefits of adjuvant RT following cSCC resection with negative surgical margins are questionable [80].
According to the British Association of Dermatologists (BAD) guidelines, adjuvant RT should be offered to patients with incompletely excised cSCC who cannot undergo further surgery and have an increased risk of local recurrence. Adjuvant RT is recommended for T3 tumors that have been completely excised and meet the high-risk criteria. Post-operative RT should be avoided in patients with completely resected T1 or T2 cSCC [81].
5.4. Radiation Therapy
For high-risk cSCC, radiation therapy is employed as a primary therapeutic option because of its noninvasive nature [82]. It cures a broad spectrum of cSCC types, including aggressive ones with lower cure rates. Radiation therapy is as effective as surgery for malignancies in the lips and eyelids [83,84]. A rigorous treatment regimen requires dedication. At the same time, it allows for the histological confirmation of tumor margins [85]. Furthermore, radiation therapy is recommended in individuals who are poor surgical candidates, who have tumors in inoperable locations, or whose reconstruction may have cosmetic or functional ramifications. In tumors that have failed to respond to other treatments, radiation therapy alone is most commonly employed as salvage or palliative therapy [86].
6. Drug Molecules, Special Scenarios, and cSCC
6.1. BRAF Inhibitors and cSCC
The BRAF inhibitors can suppress tumor growth by interfering with the MAPK pathway [87,88,89]. Similarly, MEK inhibition was also found to be effective in reducing cSCC; therefore, to reduce these side effects, BRAF inhibitors were combined with MEK inhibitors. In particular, vemurafenib is combined with cobimetinib [90] and dabrafenib with trametinib [91]. Recent trials [92] showed that trametinib, which inhibits both BRAF and MEK, decreases the risk of cSCC compared with BRAF monotherapy [92]. However, BRAF inhibitors have been shown to generate RAS mutations that upregulate the RAS/MAPK pathway. After BRAF inhibitor treatment, RAS mutations were found in 21–60% of lesions, compared with 3–30% in normal cSCCs [93]. In squamous carcinomas, BRAF inhibitor-induced mutations differ from the mutations in spontaneous cases [94]. Human papillomaviruses (HPVs) have also been discovered periodically in BRAF inhibitor-induced cSCCs, suggesting that HPV may expedite tumor growth in the exposed population [95].
In addition to MEK inhibitors, cyclooxygenase (COX)-2 inhibition has been tested as a technique to prevent the BRAF inhibitor-induced cSCC. Anti-COX-2 drugs (celecoxib and diclofenac) have been demonstrated to reduce prostaglandin synthesis, thereby preventing cSCC formation in experiments that induced cSCC carcinogenesis via ultraviolet radiation [96,97].
6.2. Sonic Hedgehog Inhibitors and cSCC
Sonic hedgehog (SHH) signaling pathway activation, the Ptch1 gene, and the GLI1 transcription factors (the primary target of the hedgehog pathway) have all been reported to be expressed in cSCC [98]. Typical effects include loss-of-function changes in pathway suppressors like Ptch1 and gain-of-function changes in promoters. These are also common in BCC, in which 73% have a gene-inactivating mutation, and 20% have a genetic activation of smoothened protein [99].
Previous research has shown that cSCCs can develop from a BCC lesion because the two stem from the same cells. In two studies, Ptch1 was discovered to play a new role in the connection between BCC and cSCC development in two studies [100]. Ptch1 determines whether a cell is basal or squamous, and its polymorphisms influence cell-fate determination. Although Ptch1 absence activates the SHH pathway in BCC, Ptch1 overexpression augments recourse, thereby increasing the risk of cSCC [101]. Arsenic trioxide was the first drug approved for targeting SHH by the Food and Drug Administration (FDA) [102]. Vismodegib and Sonidegib were the other two drugs approved in 2013 by the FDA for the SHH pathway. Drugs like 5E1, robotnikinin, RU-SKI3, and cyclopamine are under preclinical studies in cancer treatment. Other drugs like saridegib, glasdegib, taladegib, itraconazole, and genistein are under phase II trials against various cancers [103].
6.3. Immunosuppression and cSCC
Solid organ transplant recipients are at peril of developing cSCC due to immunosuppressive medications. Earlier immunosuppressive medications like azathioprine and cyclosporine have a very high risk of developing cSCC in these transplant cases. However, newer immunosuppressants such as mycophenolate mofetil, tacrolimus, sirolimus, and everolimus have reduced the risk of cSCC compared with previous immunosuppressants [104].
6.4. Genodermatoses and cSCC
cSCC in genodermatoses also requires individual case-specific risk stratification and management. Multiple squamous cell carcinoma or hereditary squamous cell carcinoma is associated with genodermatoses such as xeroderma pigmentosum, Muir-Torre syndrome, Ferguson-Smith syndrome, Mibelli-type hereditary porokeratosis, keratitis-ichthyosis-deafness syndrome, Rothmund-Thomson syndrome, Bloom syndrome, recessive dystrophic epidermolysis bullosa, and epidermodysplasia verruciformis [105]. The cSCCs arising from recessive dystrophic epidermolysis bullosa are far more aggressive and lead to poor outcomes. Primary cSCC and genodermatoses-induced cSCC have significantly different tumor microenvironments, and peritumoral cell infiltrates [106]. Further disease-specific research in immune dysregulation would create a disease-specific risk stratification strategy in the future.
7. Novel Genetic Research in Management of cSCC
Although clinicopathological factor-based risk assessment and formal staging systems are helpful, they have their limitations, such as a lack of a standardized reporting system, the subjective nature of histopathological reporting, and oversight to record risk at the molecular level. Combining molecular profiling, the 40-gene expression profile (40-GEP) test, and clinicopathological risk assessment has demonstrated significant prognostic value for stratifying metastatic risk. This approach will promote individualized risk identification and improve outcomes [107].
8. Unmet Medical Needs in the Management of cSCC
Most cSCC patients have localized neoplasm, and treatment is straightforward. However, many cases are metastatic and inoperable, which is an unmet need despite all the advances. Contemporary research has widened the comprehension of the mutational landscape and paved the way to identifying biomarkers for characterization, prognostication, and disease monitoring. Nonetheless, it is still challenging to recognize crucial driver mutations of advanced cSCC. Precision medicine using liquid biomarker analysis of circulating tumor cells, circulating tumor DNA, proteomic plasma profiling, or miRNA can potentially improve the risk-stratification strategies in these problematic cases. The future focus should be on this novel biomarker’s analysis to supplement the current tissue-based diagnostic standards [108].
9. Conclusions
The effective management of cSCC starts from clinical examination and dermoscopy, followed by an individual risk stratification strategy. Clinicians can then manage the patient according to formal staging. Surgical management in conventional excision or MMS is the first-line treatment regardless of the patient’s age and location. The selection of the surgical option, i.e., conventional vs. MMS and surgical excision margins, depends on risk stratification. Positive margins on conventional excision can be addressed with MMS and RT. RT can be used as first-line treatment in cases unable to undergo surgical resection. Understanding the molecular foundations of cSCC has aided the development of novel treatments in recent years. The anti-PD1 agents cemiplimab and pembrolizumab are approved by the FDA for the treatment of advanced cSCC. Presently, immune checkpoint inhibitors are the standard of care in locally advanced and metastatic cSCC. Contemporary international guidelines recommend cetuximab or cytotoxic chemotherapy in cases that fail to respond to or have contraindications for immune checkpoint inhibitors. A multidisciplinary board’s role is crucial in managing high-risk cases and positive margins. Other novel targets are being investigated and are still under development.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The author would like to thank Parth Naik (FRANZCR, MD) for editing the English of the manuscript.
Conflicts of Interest
The author declares no conflict of interest.
References
- Rogers, H.W.; Weinstock, M.A.; Feldman, S.R.; Coldiron, B.M. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the US Population, 2012. JAMA Dermatol. 2015, 151, 1081. [Google Scholar] [CrossRef] [PubMed]
- Muzic, J.G.; Schmitt, A.R.; Wright, A.C.; Alniemi, D.T.; Zubair, A.S.; Olazagasti Lourido, J.M.; Sosa Seda, I.M.; Weaver, A.L.; Baum, C.L. Incidence and Trends of Basal Cell Carcinoma and Cutaneous Squamous Cell Carcinoma. Mayo Clin. Proc. 2017, 92, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Leiter, U.; Keim, U.; Eigentler, T.; Katalinic, A.; Holleczek, B.; Martus, P.; Garbe, C. Incidence, Mortality, and Trends of Nonmelanoma Skin Cancer in Germany. J. Investig. Dermatol. 2017, 137, 1860–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, D.L.; Weinstock, M.A. Nonmelanoma skin cancer in the United States: Incidence. J. Am. Acad. Dermatol. 1994, 30, 774–778. [Google Scholar] [CrossRef]
- Dessinioti, C.; Pitoulias, M.; Stratigos, A.J. Epidemiology of advanced cutaneous squamous cell carcinoma. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 39–50. [Google Scholar] [CrossRef]
- Schmults, C.D.; Karia, P.S.; Carter, J.B.; Han, J.; Qureshi, A.A. Factors Predictive of Recurrence and Death From Cutaneous Squamous Cell Carcinoma. JAMA Dermatol. 2013, 149, 541. [Google Scholar] [CrossRef] [Green Version]
- Brougham, N.D.L.; Tan, S.T. The incidence and risk factors of metastasis for cutaneous squamous cell carcinoma-implications on the T-classification system. J. Surg. Oncol. 2014, 110, 876–882. [Google Scholar] [CrossRef]
- Parekh, V.; Seykora, J.T. Cutaneous Squamous Cell Carcinoma. Clin. Lab. Med. 2017, 37, 503–525. [Google Scholar] [CrossRef]
- Weinberg, A.S.; Ogle, C.A.; Shim, E.K. Metastatic Cutaneous Squamous Cell Carcinoma: An Update. Dermatol. Surg. 2007, 33, 885–899. [Google Scholar] [CrossRef]
- Alam, M.; Armstrong, A.; Baum, C.; Bordeaux, J.S.; Brown, M.; Busam, K.J.; Eisen, D.B.; Iyengar, V.; Lober, C.; Margolis, D.J. Guidelines of care for the management of cutaneous squamous cell carcinoma. J. Am. Acad. Dermatol. 2018, 78, 560–578. [Google Scholar]
- Bottomley, M.J.; Thomson, J.; Harwood, C.; Leigh, I. The Role of the Immune System in Cutaneous Squamous Cell Carcinoma. Int. J. Mol. Sci. 2019, 20, 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calonje, J.E.; Brenn, T.; Lazar, A.J.; McKee, P.H. Pathology of the Skin E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011; ISBN 0723437181. [Google Scholar]
- Breuninger, H.; Schaumburg Lever, G.; Holzschuh, J.; Horny, H.P. Desmoplastic squamous cell carcinoma of skin and vermilion surface: A highly malignant subtype of skin cancer. Cancer 1997, 79, 915–919. [Google Scholar] [CrossRef]
- Brantsch, K.D.; Meisner, C.; Schonfisch, B.; Trilling, B.; Wehner-Caroli, J.; Rocken, M.; Breuninger, H. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: A prospective study. Lancet Oncol. 2008, 9, 713–720. [Google Scholar] [CrossRef]
- Azorín, D.; López-Ríos, F.; Ballestín, C.; Barrientos, N.; Rodríguez-Peralto, J.L. Primary cutaneous adenosquamous carcinoma: A case report and review of the literature. J. Cutan. Pathol. 2001, 28, 542–545. [Google Scholar] [CrossRef]
- Rosendahl, C.; Cameron, A.; Argenziano, G.; Zalaudek, I.; Tschandl, P.; Kittler, H. Dermoscopy of Squamous Cell Carcinoma and Keratoacanthoma. Arch. Dermatol. 2012, 148, 1386. [Google Scholar] [CrossRef]
- Lallas, A.; Pyne, J.; Kyrgidis, A.; Andreani, S.; Argenziano, G.; Cavaller, A.; Giacomel, J.; Longo, C.; Malvestiti, A.; Moscarella, E.; et al. The clinical and dermoscopic features of invasive cutaneous squamous cell carcinoma depend on the histopathological grade of differentiation. Br. J. Dermatol. 2015, 172, 1308–1315. [Google Scholar] [CrossRef]
- Zalaudek, I.; Giacomel, J.; Schmid, K.; Bondino, S.; Rosendahl, C.; Cavicchini, S.; Tourlaki, A.; Gasparini, S.; Bourne, P.; Keir, J.; et al. Dermatoscopy of facial actinic keratosis, intraepidermal carcinoma, and invasive squamous cell carcinoma: A progression model. J. Am. Acad. Dermatol. 2012, 66, 589–597. [Google Scholar] [CrossRef]
- García-Foncillas, J.; Tejera-Vaquerizo, A.; Sanmartín, O.; Rojo, F.; Mestre, J.; Martín, S.; Azinovic, I.; Mesía, R. Update on Management Recommendations for Advanced Cutaneous Squamous Cell Carcinoma. Cancers 2022, 14, 629. [Google Scholar] [CrossRef]
- Patel, V.A.; McCullum, C.; Sparks, A.D.; Schmults, C.D.; Arron, S.T.; Jambusaria-Pahlajani, A. Cutaneous squamous cell carcinoma staging may influence management in users: A survey study. Cancer Med. 2022, 11, 94–103. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Center. NCCN Clinical Practice Guidelines in Oncology; Squamous Cell Carcinoma (V2. 2018). Available online: https://oncolife.com.ua/doc/nccn/Squamous_Cell_Skin_Cancer.pdf (accessed on 1 May 2020).
- Porceddu, S.V.; Bressel, M.; Poulsen, M.G.; Stoneley, A.; Veness, M.J.; Kenny, L.M.; Wratten, C.; Corry, J.; Cooper, S.; Fogarty, G.B.; et al. Post-operative Concurrent Chemoradiotherapy Versus Postoperative Radiotherapy in High-Risk Cutaneous Squamous Cell Carcinoma of the Head and Neck: The Randomized Phase III TROG 05.01 Trial. J. Clin. Oncol. 2018, 36, 1275–1283. [Google Scholar] [CrossRef]
- Mellerio, J.E.; Robertson, S.J.; Bernardis, C.; Diem, A.; Fine, J.D.; George, R.; Goldberg, D.; Halmos, G.B.; Harries, M.; Jonkman, M.F.; et al. Management of cutaneous squamous cell carcinoma in patients with epidermolysis bullosa: Best clinical practice guidelines. Br. J. Dermatol. 2016, 174, 56–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, N.A. Mohs Surgery. Arch. Dermatol. 1983, 119, 761–773. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.J. Defining, Treating, and Studying Very High-Risk Cutaneous Squamous Cell Carcinomas. Arch. Dermatol. 2010, 146, 1292–1295. [Google Scholar] [CrossRef] [PubMed]
- Brodland, D.G.; Zitelli, J.A. Surgical margins for excision of primary cutaneous squamous cell carcinoma. J. Am. Acad. Dermatol. 1992, 27, 241–248. [Google Scholar] [CrossRef]
- Skulsky, S.L.; O’Sullivan, B.; McArdle, O.; Leader, M.; Roche, M.; Conlon, P.J.; O’Neill, J.P. Review of high-risk features of cutaneous squamous cell carcinoma and discrepancies between the American Joint Committee on Cancer and NCCN Clinical Practice Guidelines In Oncology. Head Neck 2017, 39, 578–594. [Google Scholar] [CrossRef]
- Leibovitch, I.; Huilgol, S.C.; Selva, D.; Hill, D.; Richards, S.; Paver, R. Cutaneous squamous cell carcinoma treated with Mohs micrographic surgery in Australia I. Experience over 10 years. J. Am. Acad. Dermatol. 2005, 53, 253–260. [Google Scholar] [CrossRef]
- Jambusaria-Pahlajani, A.; Miller, C.J.; Quon, H.; Smith, N.; Klein, R.Q.; Schmults, C.D. Surgical Monotherapy Versus Surgery Plus Adjuvant Radiotherapy in High-Risk Cutaneous Squamous Cell Carcinoma. Dermatol. Surg. 2009, 35, 574–584. [Google Scholar] [CrossRef]
- Rowe, D.E.; Carroll, R.J.; Day, C.L. Prognostic factors for local recurrence, metastasis, and survival rates in squamous cell carcinoma of the skin, ear, and lip. J. Am. Acad. Dermatol. 1992, 26, 976–990. [Google Scholar] [CrossRef]
- Belkin, D.; Carucci, J.A. Mohs Surgery for Squamous Cell Carcinoma. Dermatol. Clin. 2011, 29, 161–174. [Google Scholar] [CrossRef]
- Pugliano-Mauro, M.; Goldman, G. Mohs Surgery Is Effective for High-Risk Cutaneous Squamous Cell Carcinoma. Dermatol. Surg. 2010, 36, 1544–1553. [Google Scholar] [CrossRef]
- Prickett, K.A.; Ramsey, M.L. Mohs Micrographic Surgery; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Clayton, B.D.; Leshin, B.; Hitchcock, M.G.; Marks, M.; White, W.L. Utility of Rush Paraffin-Embedded Tangential Sections in the Management of Cutaneous Neoplasms. Dermatol. Surg. 2000, 26, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Canavan, T.N.; Celen, A.B.; Frazzette, N.J.; Carucci, J.A.; Doudican, N.; Stevenson, M.L. A cohort study to determine factors associated with upstaging cutaneous squamous cell carcinoma during Mohs surgery. J. Am. Acad. Dermatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, A.R.; Brewer, J.D.; Bordeaux, J.S.; Baum, C.L. Staging for Cutaneous Squamous Cell Carcinoma as a Predictor of Sentinel Lymph Node Biopsy Results. JAMA Dermatol. 2014, 150, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarrete-Dechent, C.; Veness, M.J.; Droppelmann, N.; Uribe, P. High-risk cutaneous squamous cell carcinoma and the emerging role of sentinel lymph node biopsy: A literature review. J. Am. Acad. Dermatol. 2015, 73, 127–137. [Google Scholar] [CrossRef]
- Moncrieff, M.D.; Shah, A.K.; Igali, L.; Garioch, J.J. False-negative rate of intraoperative frozen section margin analysis for complex head and neck nonmelanoma skin cancer excisions. Clin. Exp. Dermatol. 2015, 40, 834–838. [Google Scholar] [CrossRef]
- Flies, D.B.; Sandler, B.J.; Sznol, M.; Chen, L. Blockade of the B7-H1/PD-1 pathway for cancer immunotherapy. Yale J. Biol. Med. 2011, 84, 409–421. [Google Scholar]
- Pickering, C.R.; Zhou, J.H.; Lee, J.J.; Drummond, J.A.; Peng, S.A.; Saade, R.E.; Tsai, K.Y.; Curry, J.L.; Tetzlaff, M.T.; Lai, S.Y.; et al. Mutational Landscape of Aggressive Cutaneous Squamous Cell Carcinoma. Clin. Cancer Res. 2014, 20, 6582–6592. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Xu, J.; Du, C.; Wu, Y.; Xia, D.; Lv, W.; Hu, J. The Predictive Value of Tumor Mutation Burden on Efficacy of Immune Checkpoint Inhibitors in Cancers: A Systematic Review and Meta-Analysis. Front. Oncol. 2019, 9, 748674. [Google Scholar] [CrossRef] [Green Version]
- Chan, T.A.; Yarchoan, M.; Jaffee, E.; Swanton, C.; Quezada, S.A.; Stenzinger, A.; Peters, S. Development of tumor mutation burden as an immunotherapy biomarker: Utility for the oncology clinic. Ann. Oncol. 2019, 30, 44–56. [Google Scholar] [CrossRef]
- Mittal, A.; Colegio, O.R. Skin Cancers in Organ Transplant Recipients. Am. J. Transplant. 2017, 17, 2509–2530. [Google Scholar] [CrossRef]
- Bauer, C.; Abdul Pari, A.A.; Umansky, V.; Utikal, J.; Boukamp, P.; Augustin, H.G.; Goerdt, S.; Géraud, C.; Felcht, M. T-lymphocyte profiles differ between keratoacanthomas and invasive squamous cell carcinomas of the human skin. Cancer Immunol. Immunother. 2018, 67, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, D.L.; Wherry, E.J.; Masopust, D.; Zhu, B.; Allison, J.P.; Sharpe, A.H.; Freeman, G.J.; Ahmed, R. Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 2006, 439, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Chikuma, S.; Terawaki, S.; Hayashi, T.; Nabeshima, R.; Yoshida, T.; Shibayama, S.; Okazaki, T.; Honjo, T. PD-1-Mediated Suppression of IL-2 Production Induces CD8 + T Cell Anergy In Vivo. J. Immunol. 2009, 182, 6682–6689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, J.; Zeitouni, N.; Fan, W.; Samie, F.H. Immune checkpoint inhibitor therapy in solid organ transplant recipients: A patient-centered systematic review. J. Am. Acad. Dermatol. 2020, 82, 1490–1500. [Google Scholar] [CrossRef]
- Long, J.; Qi, Z.; Rongxin, Z. PD-1/PD-L1 pathway blockade works as an effective and practical therapy for cancer immunotherapy. Cancer Biol. Med. 2018, 15, 116. [Google Scholar] [CrossRef] [Green Version]
- Nixon, N.A.; Blais, N.; Ernst, S.; Kollmannsberger, C.; Bebb, G.; Butler, M.; Smylie, M.; Verma, S. Current Landscape of Immunotherapy in the Treatment of Solid Tumours, with Future Opportunities and Challenges. Curr. Oncol. 2018, 25, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Tang, H.; Qiao, J.; Fu, Y.-X. Immunotherapy and tumor microenvironment. Cancer Lett. 2016, 370, 85–90. [Google Scholar] [CrossRef]
- Falchook, G.S.; Leidner, R.; Stankevich, E.; Piening, B.; Bifulco, C.; Lowy, I.; Fury, M.G. Responses of metastatic basal cell and cutaneous squamous cell carcinomas to anti-PD1 monoclonal antibody REGN2810. J. Immunother. Cancer 2016, 4, 70. [Google Scholar] [CrossRef] [Green Version]
- Slater, N.A.; Googe, P.B. PD-L1 expression in cutaneous squamous cell carcinoma correlates with risk of metastasis. J. Cutan. Pathol. 2016, 43, 663–670. [Google Scholar] [CrossRef]
- Wang, Y.; Kim, T.H.; Fouladdel, S.; Zhang, Z.; Soni, P.; Qin, A.; Zhao, L.; Azizi, E.; Lawrence, T.S.; Ramnath, N.; et al. PD-L1 Expression in Circulating Tumor Cells Increases during Radio(chemo)therapy and Indicates Poor Prognosis in Non-small Cell Lung Cancer. Sci. Rep. 2019, 9, 566. [Google Scholar] [CrossRef] [Green Version]
- Gu, X.; Dong, M.; Liu, Z.; Mi, Y.; Yang, J.; Zhang, Z.; Liu, K.; Jiang, L.; Zhang, Y.; Dong, S.; et al. Elevated PD-L1 expression predicts poor survival outcomes in patients with cervical cancer. Cancer Cell Int. 2019, 19, 146. [Google Scholar] [CrossRef] [PubMed]
- García-Pedrero, J.M.; Martínez-Camblor, P.; Diaz-Coto, S.; Munguia-Calzada, P.; Vallina-Alvarez, A.; Vazquez-Lopez, F.; Rodrigo, J.P.; Santos-Juanes, J. Tumor programmed cell death ligand 1 expression correlates with nodal metastasis in patients with cutaneous squamous cell carcinoma of the head and neck. J. Am. Acad. Dermatol. 2017, 77, 527–533. [Google Scholar] [CrossRef]
- García-Díez, I.; Hernández-Ruiz, E.; Andrades, E.; Gimeno, J.; Ferrándiz-Pulido, C.; Yébenes, M.; García-Patos, V.; Pujol, R.M.; Hernández-Muñoz, I.; Toll, A. PD-L1 Expression is Increased in Metastasizing Squamous Cell Carcinomas and Their Metastases. Am. J. Dermatopathol. 2018, 40, 647–654. [Google Scholar] [CrossRef]
- Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-cemiplimab-rwlc-metastatic-or-locally-advanced-cutaneous-squamous-cell-carcinoma (accessed on 10 June 2022).
- Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/libtayo (accessed on 17 June 2022).
- Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-cutaneous-squamous-cell-carcinoma (accessed on 17 June 2022).
- Peris, K.; Piccerillo, A.; Del Regno, L.; Di Stefani, A. Treatment approaches of advanced cutaneous squamous cell carcinoma. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.T.; Ahmed, S.R.; Chen, L.; Silapunt, S.; Migden, M.R. Review of systemic agents in the treatment of advanced cutaneous squamous cell carcinoma. Futur. Oncol. 2019, 15, 3171–3184. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, P.; Mehta, A.; Ragab, O.; Lin, S.; In, G.K. Concurrent radiation therapy with programmed cell death protein 1 inhibition leads to a complete response in advanced cutaneous squamous cell carcinoma. JAAD Case Reports 2019, 5, 763–766. [Google Scholar] [CrossRef]
- Vanhakendover, L.; Lebas, E.; Libon, F.; Wauters, O.; Dezfoulian, B.; Marchal, N.; Rorive, A.; Piret, P.; Quatresooz, P.; Jacquemin, D.; et al. Locally advanced and metastatic cutaneous squamous cell carcinoma treated with cemiplimab. Rev. Med. Liege 2019, 74, 436–440. [Google Scholar]
- Chang, A.L.S.; Kim, J.; Luciano, R.; Sullivan-Chang, L.; Colevas, A.D. A Case Report of Unresectable Cutaneous Squamous Cell Carcinoma Responsive to Pembrolizumab, a Programmed Cell Death Protein 1 Inhibitor. JAMA Dermatol. 2016, 152, 106. [Google Scholar] [CrossRef] [Green Version]
- Lipson, E.J.; Bagnasco, S.M.; Moore, J.; Jang, S.; Patel, M.J.; Zachary, A.A.; Pardoll, D.M.; Taube, J.M.; Drake, C.G. Tumor Regression and Allograft Rejection after Administration of Anti–PD-1. N. Engl. J. Med. 2016, 374, 896–898. [Google Scholar] [CrossRef] [Green Version]
- Borradori, L.; Sutton, B.; Shayesteh, P.; Daniels, G.A. Rescue therapy with anti-programmed cell death protein 1 inhibitors of advanced cutaneous squamous cell carcinoma and basosquamous carcinoma: Preliminary experience in five cases. Br. J. Dermatol. 2016, 175, 1382–1386. [Google Scholar] [CrossRef] [PubMed]
- Kacew, A.J.; Harris, E.J.; Lorch, J.H.; Haddad, R.I.; Chau, N.G.; Rabinowits, G.; LeBoeuf, N.R.; Schmults, C.D.; Thakuria, M.; MacConaill, L.E.; et al. Chromosome 3q arm gain linked to immunotherapy response in advanced cutaneous squamous cell carcinoma. Eur. J. Cancer 2019, 113, 1–9. [Google Scholar] [CrossRef]
- Pham, F.; Reynaud, B.; Favier, B.; Darnis, S.; Amini-Adle, M. Cemiplimab removed from reimbursable drugs in France. Eur. J. Cancer 2021, 149, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.sanofi.us/en/products-and-resources/patient-services/libtayo-injection-support (accessed on 17 June 2022).
- Konidaris, G.; Paul, E.; Kuznik, A.; Keeping, S.; Chen, C.I.; Sasane, M.; Xu, Y.; Atsou, K.; Ayers, D.; Ruiz, E.S.; et al. Assessing the value of cemiplimab for adults with advanced cutaneous squamous cell carcinoma: A cost-effectiveness analysis. Value Health 2021, 24, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Joseph, K.; Alkaabi, K.; Warkentin, H.; Ghosh, S.; Jha, N.; Smylie, M.; Walker, J. Cetuximab-radiotherapy combination in the management of locally advanced cutaneous squamous cell carcinoma. J. Med. Imaging Radiat. Oncol. 2019, 63, 257–363. [Google Scholar] [CrossRef] [PubMed]
- Alter, M.; Satzger, I.; Mattern, A.; Kapp, A.; Gutzmer, R. Treatment of Advanced Cutaneous Squamous Cell Carcinomas with Epidermal Growth Factor Receptor Inhibitors. Dermatology 2013, 227, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Inoue, J.; Fujiwara, K.; Hamamoto, H.; Kobayashi, K.; Inazawa, J. Improving the Efficacy of EGFR Inhibitors by Topical Treatment of Cutaneous Squamous Cell Carcinoma with miR-634 Ointment. Mol. Ther. Oncolytics 2020, 19, 294–307. [Google Scholar] [CrossRef]
- Diamantis, N.; Banerji, U. Antibody-drug conjugates—An emerging class of cancer treatment. Br. J. Cancer 2016, 114, 362–367. [Google Scholar] [CrossRef]
- Visvader, J.E.; Lindeman, G.J. Cancer stem cells in solid tumours: Accumulating evidence and unresolved questions. Nat. Rev. Cancer 2008, 8, 755–768. [Google Scholar] [CrossRef]
- Li, X.; Yuan, Y.; Wang, Y.; Xie, K.; Lu, S.; Chen, F.; Zhou, M.; Zhen, P. MicroRNA-486–3p promotes the proliferation and metastasis of cutaneous squamous cell carcinoma by suppressing flotillin-2. J. Dermatol. Sci. 2022, 105, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Jambusaria-Pahlajani, A.; Hess, S.D.; Katz, K.A.; Berg, D.; Schmults, C.D. Uncertainty in the Perioperative Management of High-Risk Cutaneous Squamous Cell Carcinoma Among Mohs Surgeons. Arch. Dermatol. 2010, 146, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Stratigos, A.J.; Garbe, C.; Dessinioti, C.; Lebbe, C.; Bataille, V.; Bastholt, L.; Dreno, B.; Fargnoli, M.C.; Forsea, A.M.; Frenard, C.; et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 1. epidemiology, diagnostics and prevention. Eur. J. Cancer 2020, 128, 60–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmults, C.D.; Blitzblau, R.; Aasi, S.Z.; Alam, M.; Andersen, J.S.; Baumann, B.C.; Bordeaux, J.; Chen, P.-L.; Chin, R.; Contreras, C.M. NCCN Guidelines® Insights: Squamous Cell Skin Cancer, Version 1.2022: Featured Updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2021, 19, 1382–1394. [Google Scholar] [CrossRef]
- Keohane, S.G.; Botting, J.; Budny, P.G.; Dolan, O.M.; Fife, K.; Harwood, C.A.; Mallipeddi, R.; Marsden, J.R.; Motley, R.J.; Newlands, C. British Association of Dermatologists guidelines for the management of people with cutaneous squamous cell carcinoma 2020. Br. J. Dermatol. 2021, 184, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Muto, P.; Pastore, F. Radiotherapy in the Adjuvant and Advanced Setting of CSCC. Dermatol. Pract. Concept. 2021, 11, e2021168S. [Google Scholar] [CrossRef]
- Veness, M.J.; Ong, C.; Cakir, B.; Morgan, G. Squamous cell carcinoma of the lip. Patterns of relapse and outcome: Reporting the Westmead Hospital experience, 1980–1997. Australas. Radiol. 2001, 45, 195–199. [Google Scholar] [CrossRef]
- Caccialanza, M.; Piccinno, R.; Gaiani, F.; Contini, D. Relevance of dermatologic radiotherapy in the therapeutic strategy of skin epithelial neoplasms: Excellent results in the treatment of lesions localized on eyelids and skin overlying the cartilage of the nose. G. Ital. Dermatol. Venereol. 2013, 148, 83–88. [Google Scholar]
- Veness, M.; Richards, S. Role of modern radiotherapy in treating skin cancer. Australas. J. Dermatol. 2003, 44, 159–168. [Google Scholar] [CrossRef]
- Al-Othman, M.O.F.; Mendenhall, W.M.; Amdur, R.J. Radiotherapy alone for clinical T4 skin carcinoma of the head and neck with surgery reserved for salvage. Am. J. Otolaryngol. 2001, 22, 387–390. [Google Scholar] [CrossRef]
- Su, F.; Viros, A.; Milagre, C.; Trunzer, K.; Bollag, G.; Spleiss, O.; Reis-Filho, J.S.; Kong, X.; Koya, R.C.; Flaherty, K.T.; et al. RAS Mutations in Cutaneous Squamous-Cell Carcinomas in Patients Treated with BRAF Inhibitors. N. Engl. J. Med. 2012, 366, 207–215. [Google Scholar] [CrossRef] [Green Version]
- Gibney, G.T.; Messina, J.L.; Fedorenko, I.V.; Sondak, V.K.; Smalley, K.S.M. Paradoxical oncogenesis—The long-term effects of BRAF inhibition in melanoma. Nat. Rev. Clin. Oncol. 2013, 10, 390–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatzivassiliou, G.; Song, K.; Yen, I.; Brandhuber, B.J.; Anderson, D.J.; Alvarado, R.; Ludlam, M.J.C.; Stokoe, D.; Gloor, S.L.; Vigers, G.; et al. RAF inhibitors prime wild-type RAF to activate the MAPK pathway and enhance growth. Nature 2010, 464, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, J.; Ascierto, P.A.; Dréno, B.; Atkinson, V.; Liszkay, G.; Maio, M.; Mandalà, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Combined Vemurafenib and Cobimetinib in BRAF -Mutated Melanoma. N. Engl. J. Med. 2014, 371, 1867–1876. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, K.T.; Infante, J.R.; Daud, A.; Gonzalez, R.; Kefford, R.F.; Sosman, J.; Hamid, O.; Schuchter, L.; Cebon, J.; Ibrahim, N.; et al. Combined BRAF and MEK Inhibition in Melanoma with BRAF V600 Mutations. N. Engl. J. Med. 2012, 367, 1694–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, L.; Wang, Y.; Hong, Y.; Ye, X.; Shi, P.; Zhang, J.; Zhao, Q. Incidence and relative risk of cutaneous squamous cell carcinoma with single-agent BRAF inhibitor and dual BRAF/MEK inhibitors in cancer patients: A meta-analysis. Oncotarget 2017, 8, 83280–83291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberholzer, P.A.; Kee, D.; Dziunycz, P.; Sucker, A.; Kamsukom, N.; Jones, R.; Roden, C.; Chalk, C.J.; Ardlie, K.; Palescandolo, E.; et al. RAS Mutations Are Associated With the Development of Cutaneous Squamous Cell Tumors in Patients Treated With RAF Inhibitors. J. Clin. Oncol. 2012, 30, 316–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clynick, B.; Tabone, T.; Fuller, K.; Erber, W.; Meehan, K.; Millward, M.; Wood, B.A.; Harvey, N.T. Mutational Analysis of BRAF Inhibitor–Associated Squamoproliferative Lesions. J. Mol. Diagn. 2015, 17, 644–651. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.N.; Lawson, S.K.; Shaver, A.C.; Du, L.; Nguyen, H.P.; He, Q.; Johnson, D.B.; Lumbang, W.A.; Moody, B.R.; Prescott, J.L.; et al. Contribution of Beta-HPV Infection and UV Damage to Rapid-Onset Cutaneous Squamous Cell Carcinoma during BRAF-Inhibition Therapy. Clin. Cancer Res. 2015, 21, 2624–2634. [Google Scholar] [CrossRef] [Green Version]
- Pentland, A.P.; Schoggins, J.W.; Scott, G.A.; Khan, K.N.M.; Han, R. Reduction of UV-induced skin tumors in hairless mice by selective COX-2 inhibition. Carcinogenesis 1999, 20, 1939–1944. [Google Scholar] [CrossRef] [Green Version]
- Burns, E.M.; Tober, K.L.; Riggenbach, J.A.; Schick, J.S.; Lamping, K.N.; Kusewitt, D.F.; Young, G.S.; Oberyszyn, T.M. Preventative topical diclofenac treatment differentially decreases tumor burden in male and female Skh-1 mice in a model of UVB-induced cutaneous squamous cell carcinoma. Carcinogenesis 2013, 34, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Tanese, K.; Emoto, K.; Kubota, N.; Fukuma, M.; Sakamoto, M. Immunohistochemical visualization of the signature of activated Hedgehog signaling pathway in cutaneous epithelial tumors. J. Dermatol. 2018, 45, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Pyczek, J.; Khizanishvili, N.; Kuzyakova, M.; Zabel, S.; Bauer, J.; Nitzki, F.; Emmert, S.; Schön, M.P.; Boukamp, P.; Schildhaus, H.-U.; et al. Regulation and Role of GLI1 in Cutaneous Squamous Cell Carcinoma Pathogenesis. Front. Genet. 2019, 10, 1185. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, Y.; Mao, J.-H.; Brown, K.; Girardi, M.; Balmain, A. Promotion of Hras-induced squamous carcinomas by a polymorphic variant of the Patched gene in FVB mice. Nature 2007, 445, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.C.; Wakabayashi, Y.; Jen, K.-Y.; Mao, J.-H.; Zoumpourlis, V.; Del Rosario, R.; Balmain, A. Ptch1 Overexpression Drives Skin Carcinogenesis and Developmental Defects in K14Ptch Mice. J. Investig. Dermatol. 2013, 133, 1311–1320. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.H.; Hirschfeld, S.; Honig, S.F.; Ibrahim, A.; Johnson, J.R.; O’Leary, J.J.; White, R.M.; Williams, G.A.; Pazdur, R. Drug Approval Summaries: Arsenic Trioxide, Tamoxifen Citrate, Anastrazole, Paclitaxel, Bexarotene. Oncologist 2001, 6, 4–11. [Google Scholar] [CrossRef]
- Carpenter, R.L.; Ray, H. Safety and Tolerability of Sonic Hedgehog Pathway Inhibitors in Cancer. Drug Saf. 2019, 42, 263–279. [Google Scholar] [CrossRef]
- Plasmeijer, E.I.; Sachse, M.M.; Gebhardt, C.; Geusau, A.; Bouwes Bavinck, J.N. Cutaneous squamous cell carcinoma (cSCC) and immunosurveillance—The impact of immunosuppression on frequency of cSCC. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Schierbeck, J.; Vestergaard, T.; Bygum, A. Skin Cancer Associated Genodermatoses: A Literature Review. Acta Derm. Venereol. 2019, 99, 360–369. [Google Scholar] [CrossRef] [Green Version]
- Filoni, A.; Cicco, G.; Cazzato, G.; Bosco, A.; Lospalluti, L.; Tucci, M.; Cimmino, A.; Foti, C.; Marzullo, A.; Bonamonte, D. Immune Disregulation in Cutaneous Squamous Cell Carcinoma of Patients with Recessive Dystrophic Epidermolysis Bullosa: A Single Pilot Study. Life 2022, 12, 213. [Google Scholar] [CrossRef]
- Ibrahim, S.F.; Kasprzak, J.M.; Hall, M.A.; Fitzgerald, A.L.; Siegel, J.J.; Kurley, S.J.; Covington, K.R.; Goldberg, M.S.; Farberg, A.S.; Trotter, S.C.; et al. Enhanced metastatic risk assessment in cutaneous squamous cell carcinoma with the 40-gene expression profile test. Futur. Oncol. 2022, 18, 833–847. [Google Scholar] [CrossRef]
- Geidel, G.; Heidrich, I.; Kött, J.; Schneider, S.W.; Pantel, K.; Gebhardt, C. Emerging precision diagnostics in advanced cutaneous squamous cell carcinoma. NPJ Precis. Oncol. 2022, 6, 17. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) Clinical picture in an 81-year-old male with histopathological diagnosis of squamous cell carcinoma on the right pre-auricular region, 15 mm nodular reddish-pink lesion that shows surface lobulations with chief complaints of bleeding on-and-off from the lesion and (b) dermoscopic features consists of irregular surface, variable areas of angiogenesis with the cork-screw pattern of vessels, microthrombi, keratinization, and an erythematous surface with adherent clots.
Figure 1.
(a) Clinical picture in an 81-year-old male with histopathological diagnosis of squamous cell carcinoma on the right pre-auricular region, 15 mm nodular reddish-pink lesion that shows surface lobulations with chief complaints of bleeding on-and-off from the lesion and (b) dermoscopic features consists of irregular surface, variable areas of angiogenesis with the cork-screw pattern of vessels, microthrombi, keratinization, and an erythematous surface with adherent clots.


{kind=link}
Table 1.
Risk stratification of cutaneous squamous cell carcinoma [19].
Table 1.
Risk stratification of cutaneous squamous cell carcinoma [19].
| Low-Risk cSCC | High-Risk cSCC | |
|---|---|---|
| Clinical Parameters | ||
| Location and size | Lesion on trunk and extremities (excluding hands, nail units, pretibial, ankles, and feet) <20 mm; Lesion on cheeks, forehead, scalp, neck, and pretibial area <10 mm | Lesion on trunk and extremities (excluding hands, nail units, pretibial, ankles, and feet) ≥20 mm; Lesion on cheeks, forehead, scalp, neck, and pretibial area ≥10 mm; Lesion on mask areas” of the face (central face, eyelids, eyebrows, periorbital, nose, lips (cutaneous and vermilion), chin, mandible, preauricular and postauricular skin/sulci, temple, and ear), genitalia, hands, and feet |
| Borders | Well-defined | Poorly defined |
| Primary vs. Recurrent | Primary | Recurrent |
| Immunosuppression | − | + |
| Prior RT or chronic inflammatory process | − | + |
| Rapidly growing tumor | − | + |
| Neurologic symptoms | − | + |
| Pathology | ||
| Differentiation | Well or moderately defined | Poorly defined |
| Acantholytic (adenoid), adenosquamous, desmoplastic, or metaplastic (carcinosarcomatous) subtypes | − | + |
| Depth (thickness or level of invasion) | ≤6 mm, no invasion beyond subcutaneous fat | >6 mm or invasion of subcutaneous fat |
| Perineural, lymphatic, or vascular involvement | − | + |
cSCC: Cutaneous squamous cell carcinoma; RT: Radiotherapy.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Naik, P.P. Recent Trends in the Integrated Management of Cutaneous Squamous Cell Carcinoma. Dermato 2022, 2, 59-72. https://doi.org/10.3390/dermato2030007
AMA Style
Naik PP. Recent Trends in the Integrated Management of Cutaneous Squamous Cell Carcinoma. Dermato. 2022; 2(3):59-72. https://doi.org/10.3390/dermato2030007
Chicago/Turabian StyleNaik, Piyu Parth. 2022. "Recent Trends in the Integrated Management of Cutaneous Squamous Cell Carcinoma" Dermato 2, no. 3: 59-72. https://doi.org/10.3390/dermato2030007