
REBT Integration in Public and Private Outpatient Settings during COVID-19 Pandemic: Perspectives from Indonesia

Abstract
:1. Introduction
2. Methods
3. Results
3.1. Distribution of Anxiety, Depression, and Sleep Quality by Sex and REBT Sessions
3.2. Differences in the Proportion of Characteristics, Anxiety, Depression, and Sleep Quality with REBT Therapy Sessions by Sex
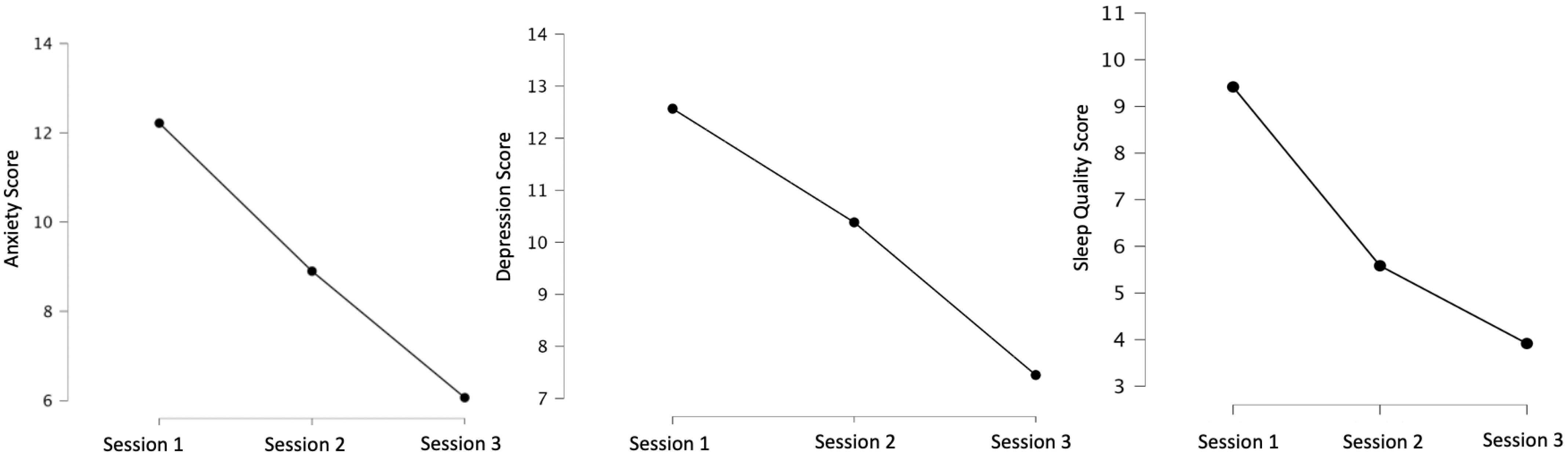
3.3. Repeated Measures ANOVA Analysis
4. Discussion
5. Limitations
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Coronavirus Disease (COVID-19). 2 July 2021. Available online: https://covid19.who.int (accessed on 20 September 2021).
- Corona Jakarta. Pantau COVID-19 Hari Ini. 2 July 2021. Available online: https://corona.jakarta.go.id/id (accessed on 20 September 2021).
- PDSKJI. Masalah Psikologis di Era Pandemi COVID-19. 2 September 2022. Available online: http://www.pdskji.org/home (accessed on 14 September 2022).
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of Mental Health Problems During the COVID-19 Pandemic: A Systematic Review and Meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Karki, P.; Prakash, P.; Chandra, A.; Khadka, S. Impact of COVID-19 Pandemic on Quality of Sleep Among Nepalese Residents. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Puthran, R.; Zhang, M.W.B.; Tam, W.W.; Ho, R.C. Prevalence of Depression Amongst Medical Students: A Meta-analysis. Med. Educ. 2016, 50, 456–468. [Google Scholar] [CrossRef] [PubMed]
- Szentagotai, A. Irrational Beliefs, Thought Suppression and Distress: A Mediation Analysis. J. Cogn. Behav. Psychother. 2006, 6, 119–127. Available online: https://www.proquest.com/docview/201708515 (accessed on 20 April 2021).
- Bechara, M.; Al-Refaie, W.; El-Taweel, A. The Effectiveness of Rational Emotive behavior therapy (REBT) in Reducing Symptoms of Anxiety and Depression in Patients with COVID-19. J. Clin. Psychol. 2021, 77, 1–13. [Google Scholar] [CrossRef]
- Into the Light Indonesia. Daftar Puskesmas, Rumah Sakit, dan Biro Psikologi Penyedia Layanan Kesehatan Mental di Indonesia. 30 March 2023. Available online: https://www.intothelightid.org/tentang-bunuh-diri/daftar-penyedia-layanan-kesehatan-mental (accessed on 2 April 2023).
- Kemenkes, R.I. Pedoman Penyelenggaraan Kesehatan Jiwa di Fasilitas Kesehatan Tingkat Pertama. Direktorat Pencegahan dan Pengendalian Masalah Kesehatan Jiwa dan Napza, Direktorat Jenderal Pencegahan dan Pengendalian Penyakit, Kementerian Kesehatan RI. 2020. Available online: https://promkes.kemkes.go.id/pub/files/files1241Pedoman_Pelayanan_Kesehatan_Jiwa%20di%20FKTP%20[1].pdf (accessed on 14 September 2021).
- The Jakarta Post. The Underwhelming Search for Good Mental Health Service in Indonesia. 30 March 2023. Available online: https://www.thejakartapost.com/culture/2023/03/29/the-underwhelming-search-for-good-mental-health-service-in-indonesia.html (accessed on 2 April 2023).
- Zahra, A.A. Yuk Cari Tahu Layanan Kesehatan Jiwa Pada Puskesmas dan Lokasinya! PPH UNIKA Atma Jaya. 5 February 2020. Available online: http://pph.atmajaya.ac.id/berita/artikel/yuk-cari-tahu-layanan-kesehatan-jiwa-pada-puskesmas-dan-lokasinya (accessed on 20 September 2021).
- Surilena Ismail, R.I.; Irwanto Djoerban, Z.; Utomo, B.; Sabarinah, I.w.a.n.; Akip, A.A. The Effect of Rational Emotive Behavior therapy (REBT) on Antiretroviral Therapeutic Adherence and Mental Health in Women Infected with HIV/AIDS. Acta Med. Indones. 2014, 46, 283–291. Available online: https://pubmed.ncbi.nlm.nih.gov/25633544/ (accessed on 20 April 2021).
- Wong, D.F.K.; Cheung, Y.C.H.; Huang, Y.-T.; Tam, C.H.L.; Chan, W.M.H.; Yeung, K.K.W. Quasi-experimental Study Comparing CBT, MBCT, Activity-based Supportive Counselling for Hong Kong Delinquent Youth. Res. Soc. Work. Pract. 2022, 32, 567–582. [Google Scholar] [CrossRef]
- Dian, C.N. Validitas dan Reliabilitas the Patient Health Questionnaire (PHQ-9) Versi Bahasa Indonesia. Program Studi Psikiatri Fakultas Kedokteran Universitas Sumatera Utara Medan. 2020. Available online: https://repositori.usu.ac.id/handle/123456789/29791 (accessed on 20 April 2021).
- Sukmawati, N.M.H.; Putra, I.G.S.W. Reliabilitas Kuesioner Pittsburrgh Sleep Quality Index (PSQI) Versi Bahasa Indonesia Dalam Mengukur Kualitas Tidur Lansia. J. Lingkung. Dan Pembang. 2019, 3, 30–38. Available online: https://ejournal.warmadewa.ac.id/index.php/wicaksana (accessed on 20 April 2021).
- Alim, I.Z. Uji Validitas dan Reliabilitas Instrumen Pittsburgh Sleep Quality Index Versi Bahasa Indonesia = Test Validity and Reliability of the Instrument Pittsburgh Sleep Quality Index Indonesia Language Version. UI Tesis. 2015, pp. 71–73. Available online: https://lib.ui.ac.id/detail?id=20404062&lokasi=lokal (accessed on 20 April 2021).
- Laerd Statistics. Repeated Measures ANOVA. 5 June 2021. Available online: https://statistics.laerd.com/statistical-guides/repeated-measures-anova-statistical-guide.php (accessed on 14 September 2022).
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of Stress, Anxiety, Depression Among the General Population During the COVID-19 Pandemic: A Systematic Review and Meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Turner, M.J. Rational Emotive Behavior Therapy (REBT), Irrational and Rational Beliefs, and the Mental Health of Athletes. Front. Psychol. 2016, 7, 1423. [Google Scholar] [CrossRef]
- Srifianti. Pengaruh Rational Emotive Behavior Therapy (REBT) Terhadap Penurunan Gejala Gangguan Cemas Menyeluruh (GAD). J. Psikol. 2018, 16, 92–99. Available online: https://ejurnal.esaunggul.ac.id/index.php/psiko/article/view/2669 (accessed on 20 April 2021).
- Budikayanti, A.; Larasari, A.; Malik, K.; Syeban, Z.; Indrawati, L.; Octaviana, F. Screening of Generalized Anxiety Disorder in Patients with Epilepsy: Using a Valid and Reliable Indonesian Version of Generalized Anxiety Disorder-7 (GAD-7). Neurol Res. Int. 2019, 2019, 5902610. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and Correlates of PTSD and Depressive Symptoms One Month After the Outbreak of the COVID-19 Epidemic in A Sample of Home-quarantined Chinese University Students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef]
- Abate, K.H. Gender Disparity in Prevalence of Depression Among Patient Population: A Systematic Review. Ethiop. J. Health Sci. 2013, 23, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, M.J.; Kassinove, H.; Miller, N.J. Effects of Rational-Emotive Therapy, Rational Role Reversal, and Rational-Emotive Imagery on the Emotional Adjustment of Community Mental Health Center Patients. J. Consult. Clin. Psychol. 1980, 48, 366–374. [Google Scholar] [CrossRef]
- Solomon, A.; Arnow, B.A.; Gotlib, I.H.; Win, B. Individualized Measurement of Irrational Beliefs in Remitted Depressives. J. Clin. Psychol. 2003, 59, 439–455. [Google Scholar] [CrossRef]
- Odriozola-González, P.; Planchuelo-Gómez, Á.; Irurtia, M.J.; de Luis-García, R. Psychological Effects of the COVID-19 Outbreak and Lockdown Among Students and Workers of a Spanish University. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef] [PubMed]
- Sartorao Filho, C.; Rodrigues, W.; Beauchamp de Castro, R.; Marcal, A.; Pavelqueires, S.; Takano, L.; de Oliveira, W.L.; Neto, C.L.S. Impact of COVID-19 Pandemic on Mental Health of Medical Students: A Cross-sectional Study Using GAD-7 and PHQ-9 questionnaires. medRxiv 2020. [Google Scholar] [CrossRef]
- Zhao, X.; Lan, M.; Li, H.; Yang, J. Perceived Stress and Sleep Quality Among the Non-diseased General Public in China During the 2019 Coronavirus Disease: A Moderated Mediation Model. Sleep Med. 2020, 77, 339–345. [Google Scholar] [CrossRef]
- Manna, G.; Falgares, G.; Ingoglia, S.; Como, M.R.; De Santis, S. The Relationship Between Self-esteem, Depression and Anxiety: Comparing Vulnerability and Scar Model in the Italian Context. Mediterr. J. Clin. Psychol. 2016, 4. Available online: https://cab.unime.it/journals/index.php/MJCP/article/view/1328 (accessed on 20 April 2021).
- Ellis, A. Discomfortanxiety: A New Cognitive Behavioural Contruct. Journal of Psychology. J. Ration.-Emot. Cogn.-Behav. Ther. 2003, 21, 193–202. [Google Scholar] [CrossRef]
- Warren, R.; McLellarn, R.W.; Ponzoha, C. Rational-emotive Therapy vs. General Cognitive BTehavior Therapy in the treatment of Low Self-esteem and Related Emotional Disturbances. Cogn. Ther. Res. 1988, 12, 21–37. [Google Scholar] [CrossRef]
- David, D.; Schnur, J.; Belloiu, A. Another Search for the “Hot” Cognition: Apprasial Irrational Beliefs, Attribution, and Their Relation to Emotion. J. Ration.-Emot. Cogn.-Behav. Ther. 2002, 20, 93–131. [Google Scholar] [CrossRef]
- Ellis, A. Similarities and Differences Between Rational Emotive Behavior Therapy and Cognitive Therapy. J. Cogn. Psychother. 2003, 17, 225–240. Available online: https://www.proquest.com/openview/88d5a3408af7b18e6909828b8481ba3d/1?pq-origsite=gscholar&cbl=28723 (accessed on 20 April 2021). [CrossRef]
- Engels, G.I.; Garnefski, N.; Diekstra, R.F.W. Efficacy of Rational-Emotive Therapy: A Quantitative Analysis. J. Consult. Clin. Psychol. 1993, 61, 1083–1090. [Google Scholar] [CrossRef]
- Finlay, A.J.F.; Jeffrey, C.L.L. Public and Private Mental Healthcare for the Population Mental Health Effects of COVID-19 Measures. Aust. N. Z. J. Psychiatry 2020, 54, 1138. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Weitz, E.; Twisk, J.; Kuehner, C.; Cristea, I.; David, D.; DeRubeis, R.J.; Dimidjian, S.; Dunlop, B.W.; Faramarzi, M.; et al. Gender as Predictor and Moderator of Outcome in Cognitive Behavior Therapy and Pharmacotherapy for Adult Depression: An “Individual Patient Data” Meta-analysis. Depress. Anxiety 2014, 31, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.; Varker, T.; Kartal, D.; Hetrick, S.; O’Donnell, M.; Forbes, D. Gender Difference in Outcomes Following Trauma-focused Interventions for Posttraumatic Stress Disorder: Systematic Review and Meta-analysis. Psychol. Trauma Theory Res. Pract. Policy 2016, 8, 356–364. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Female | Male | ||
|---|---|---|---|---|
| N | % | N | % | |
| Anxiety Session 1 | ||||
| Normal | 0 | 0 | 0 | 0 |
| Mild | 11 | 50 | 11 | 50 |
| Moderate | 6 | 54.55 | 5 | 45.45 |
| Severe | 18 | 66.67 | 9 | 33.33 |
| Anxiety Session 3 | ||||
| Normal | 5 | 71.43 | 2 | 28.57 |
| Mild | 12 | 46.15 | 14 | 53.85 |
| Moderate | 18 | 66.67 | 9 | 33.33 |
| Severe | 0 | 0 | 0 | 0 |
| Very Severe | 0 | 0 | 0 | 0 |
| Anxiety Session 6 | ||||
| Normal | 17 | 60.71 | 11 | 39.29 |
| Mild | 16 | 57.14 | 12 | 42.86 |
| Moderate | 2 | 50 | 2 | 50 |
| Depression Session 1 | ||||
| Normal | 1 | 100 | 0 | 2.86 |
| Mild | 13 | 54.17 | 11 | 45.83 |
| Moderate | 4 | 80 | 1 | 20 |
| Severe | 10 | 76.92 | 3 | 23.08 |
| Depression Session 3 | ||||
| Normal | 9 | 56.25 | 7 | 43.75 |
| Mild | 8 | 61.54 | 5 | 38.46 |
| Moderate | 11 | 73.33 | 4 | 26.67 |
| Severe | 7 | 46.67 | 8 | 53.33 |
| Very Severe | 0 | 0 | 1 | 100 |
| Depression Session 6 | ||||
| Normal | 18 | 62.07 | 11 | 37.93 |
| Mild | 13 | 68.42 | 6 | 31.58 |
| Moderate | 4 | 40 | 6 | 60 |
| Severe | 0 | 0 | 2 | 100 |
| Sleep Quality Session 1 | ||||
| Good | 4 | 50 | 4 | 50 |
| Poor | 31 | 59.62 | 21 | 40.38 |
| Sleep Quality Session 3 | ||||
| Good | 21 | 47.73 | 23 | 52.27 |
| Poor | 14 | 87.50 | 2 | 12.50 |
| Sleep Quality Session 6 | ||||
| Good | 35 | 58.33 | 25 | 41.67 |
| Variables | Female | Male | x2 | p | ||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Age | ||||||
| <40 yo | 18 | 56.25 | 14 | 43.75 | 0.12 | 0.73 |
| ≥40 yo | 17 | 60.71 | 11 | 39.29 | ||
| Work Status | ||||||
| Unemployed | 11 | 52.38 | 10 | 47.62 | 2.69 | 0.44 |
| Private Employee | 12 | 70.59 | 5 | 29.41 | ||
| Public Employee | 5 | 71.43 | 2 | 28.57 | ||
| Entrepreneur | 7 | 46.67 | 8 | 53.33 | ||
| Education | ||||||
| Junior High School | 3 | 37.50 | 5 | 62.50 | 2.91 | 0.23 |
| High School and Vocational Education | 14 | 53.85 | 12 | 46.15 | ||
| Higher Education (Diploma and Bachelor’s) | 18 | 69.23 | 8 | 30.77 | ||
| Marital Status | ||||||
| Married | 22 | 64.71 | 12 | 35.29 | 1.31 | 0.25 |
| Unmarried | 13 | 50 | 13 | 50 | ||
| Anxiety Session 1 | ||||||
| Normal | 0 | 0 | 0 | 0 | 1.46 | 0.48 |
| Mild | 11 | 50 | 11 | 50 | ||
| Moderate | 6 | 54.55 | 5 | 45.45 | ||
| Severe | 18 | 66.67 | 9 | 33.33 | ||
| Anxiety Session 3 | ||||||
| Normal | 5 | 71.43 | 2 | 28.57 | 2.85 | 0.24 |
| Mild | 12 | 46.15 | 14 | 53.85 | ||
| Moderate | 18 | 66.67 | 9 | 33.33 | ||
| Severe | 0 | 0 | 0 | 0 | ||
| Very Severe | 0 | 0 | 0 | 0 | ||
| Anxiety Session 6 | ||||||
| Normal | 17 | 60.71 | 11 | 39.29 | 0.20 | 0.91 |
| Mild | 16 | 57.14 | 12 | 42.86 | ||
| Moderate | 2 | 50 | 2 | 50 | ||
| Depression Session 1 | ||||||
| Normal | 1 | 100 | 0 | 2.86 | 5.76 | 0.22 |
| Mild | 13 | 54.17 | 11 | 45.83 | ||
| Moderate | 4 | 80 | 1 | 20 | ||
| Severe | 10 | 76.92 | 3 | 23.08 | ||
| Depression Session 3 | ||||||
| Normal | 9 | 56.25 | 7 | 43.75 | 3.71 | 0.45 |
| Mild | 8 | 61.54 | 5 | 38.46 | ||
| Moderate | 11 | 73.33 | 4 | 26.67 | ||
| Severe | 7 | 46.67 | 8 | 53.33 | ||
| Very Severe | 0 | 0 | 1 | 100 | ||
| Depression Session 6 | ||||||
| Normal | 18 | 62.07 | 11 | 37.93 | 5.14 | 0.16 |
| Mild | 13 | 68.42 | 6 | 31.58 | ||
| Moderate | 4 | 40 | 6 | 60 | ||
| Severe | 0 | 0 | 2 | 100 | ||
| Sleep Quality Session 1 | ||||||
| Good | 4 | 50 | 4 | 50 | 0.26 | 0.61 |
| Poor | 31 | 59.62 | 21 | 40.38 | ||
| Sleep Quality Session 3 | ||||||
| Good | 21 | 47.73 | 23 | 52.27 | 7.64 | 0.01 * |
| Poor | 14 | 87.50 | 2 | 12.50 | ||
| Sleep Quality Session 6 | ||||||
| Good | 35 | 58.33 | 25 | 41.67 | ||
| REBT Session 1 | REBT Session 3 | REBT Session 6 | x2(df) | p | Kendall’s W | ||||
|---|---|---|---|---|---|---|---|---|---|
| Median | Min–Max | Median | Min–Max | Median | Min–Max | ||||
| Anxiety | 12.50 | 6–19 | 9 | 3–14 | 5.5 | 2–10 | 118.56 (2) | <0.001 * | 0.99 |
| Depression | 14.50 | 4–23 | 10 | 3–21 | 6.5 | 3–19 | 108.18 (2) | <0.001 * | 0.90 |
| Sleep Quality | 9 | 2–16 | 5 | 3–14 | 4 | 2–5 | 75.95 (2) | <0.001 * | 0.63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surilena; Wolter, A.; Vincentius, M.; Teresa, A. REBT Integration in Public and Private Outpatient Settings during COVID-19 Pandemic: Perspectives from Indonesia. Psychiatry Int. 2023, 4, 79-89. https://doi.org/10.3390/psychiatryint4020011
Surilena, Wolter A, Vincentius M, Teresa A. REBT Integration in Public and Private Outpatient Settings during COVID-19 Pandemic: Perspectives from Indonesia. Psychiatry International. 2023; 4(2):79-89. https://doi.org/10.3390/psychiatryint4020011
Chicago/Turabian StyleSurilena, Alegra Wolter, Michael Vincentius, and Adela Teresa. 2023. "REBT Integration in Public and Private Outpatient Settings during COVID-19 Pandemic: Perspectives from Indonesia" Psychiatry International 4, no. 2: 79-89. https://doi.org/10.3390/psychiatryint4020011