
Bidirectional Association between Psoriasis and Asthma: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Eligibility
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Identified Studies
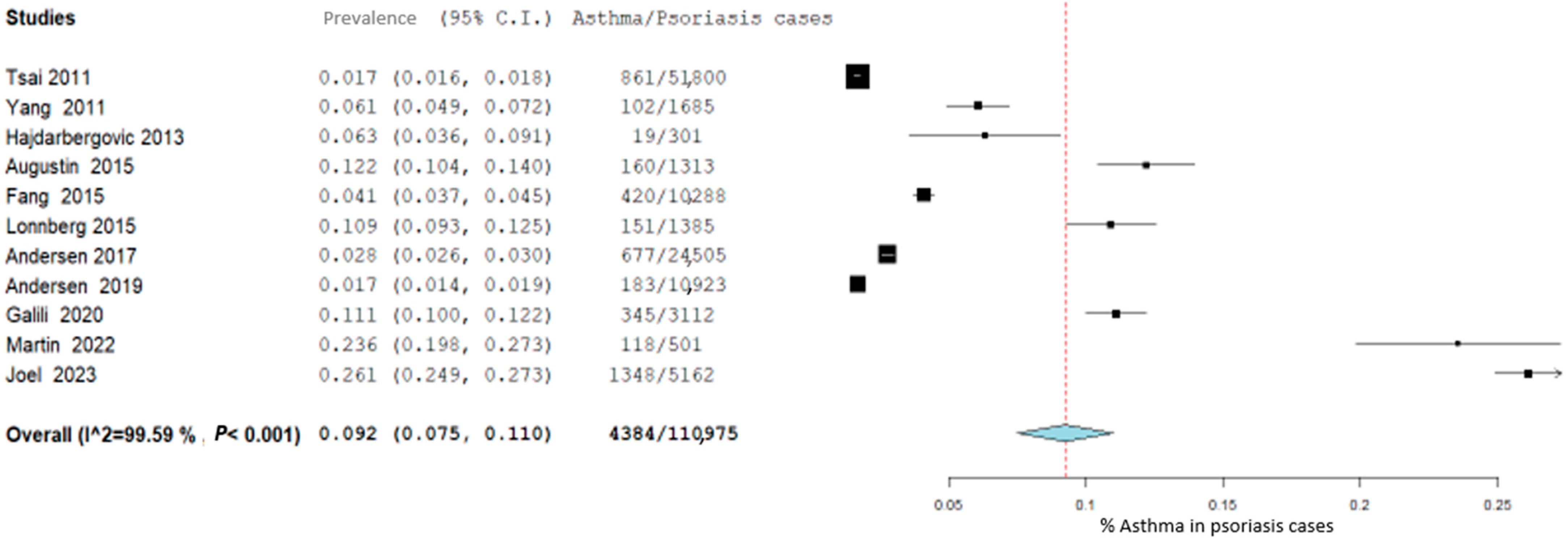
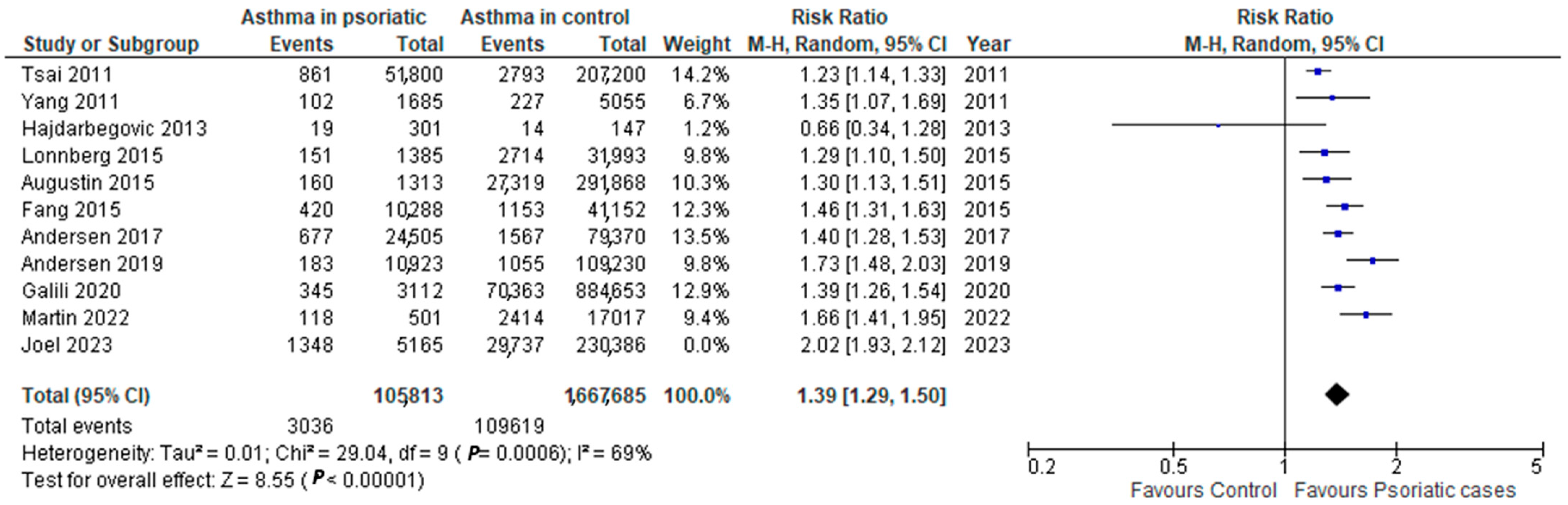
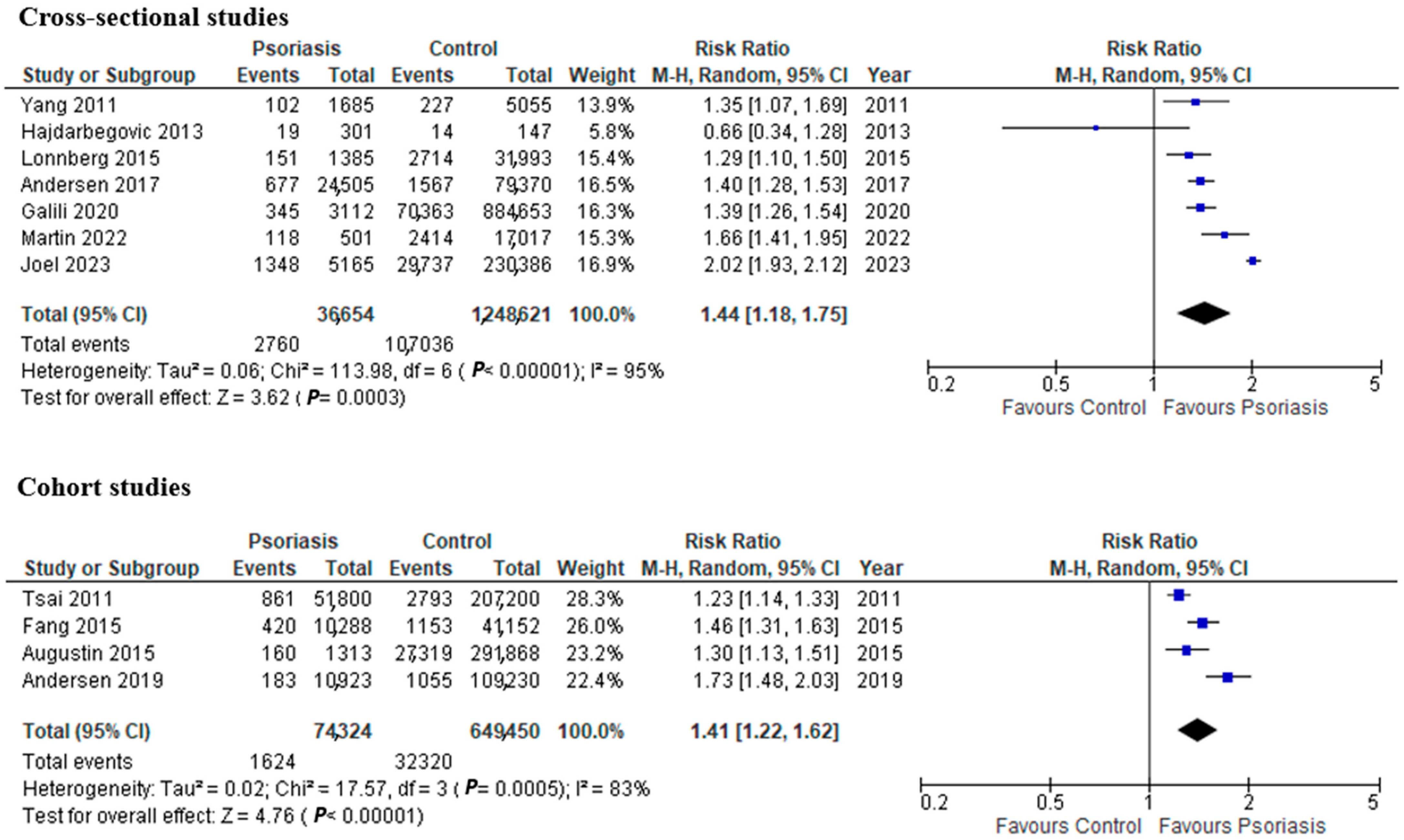
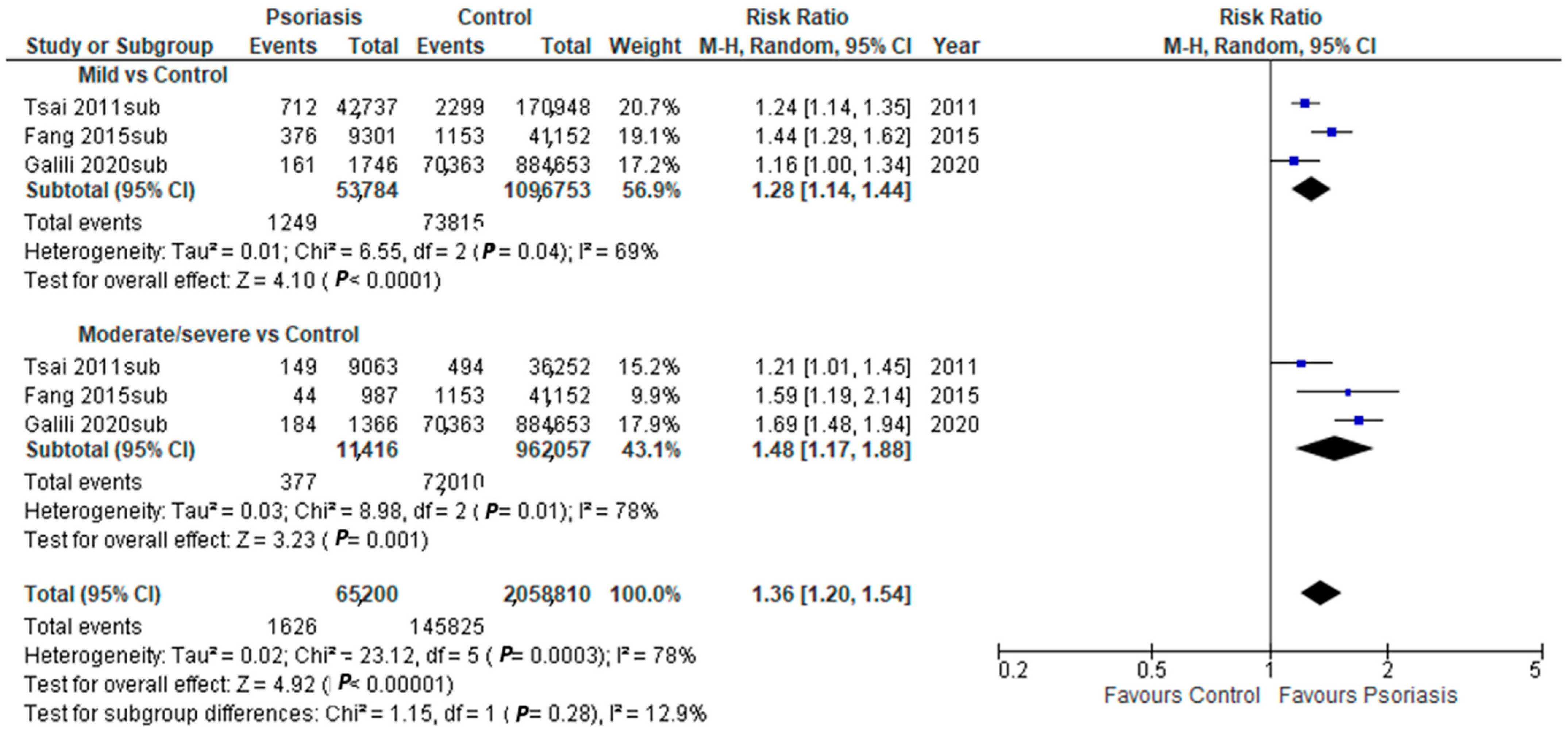
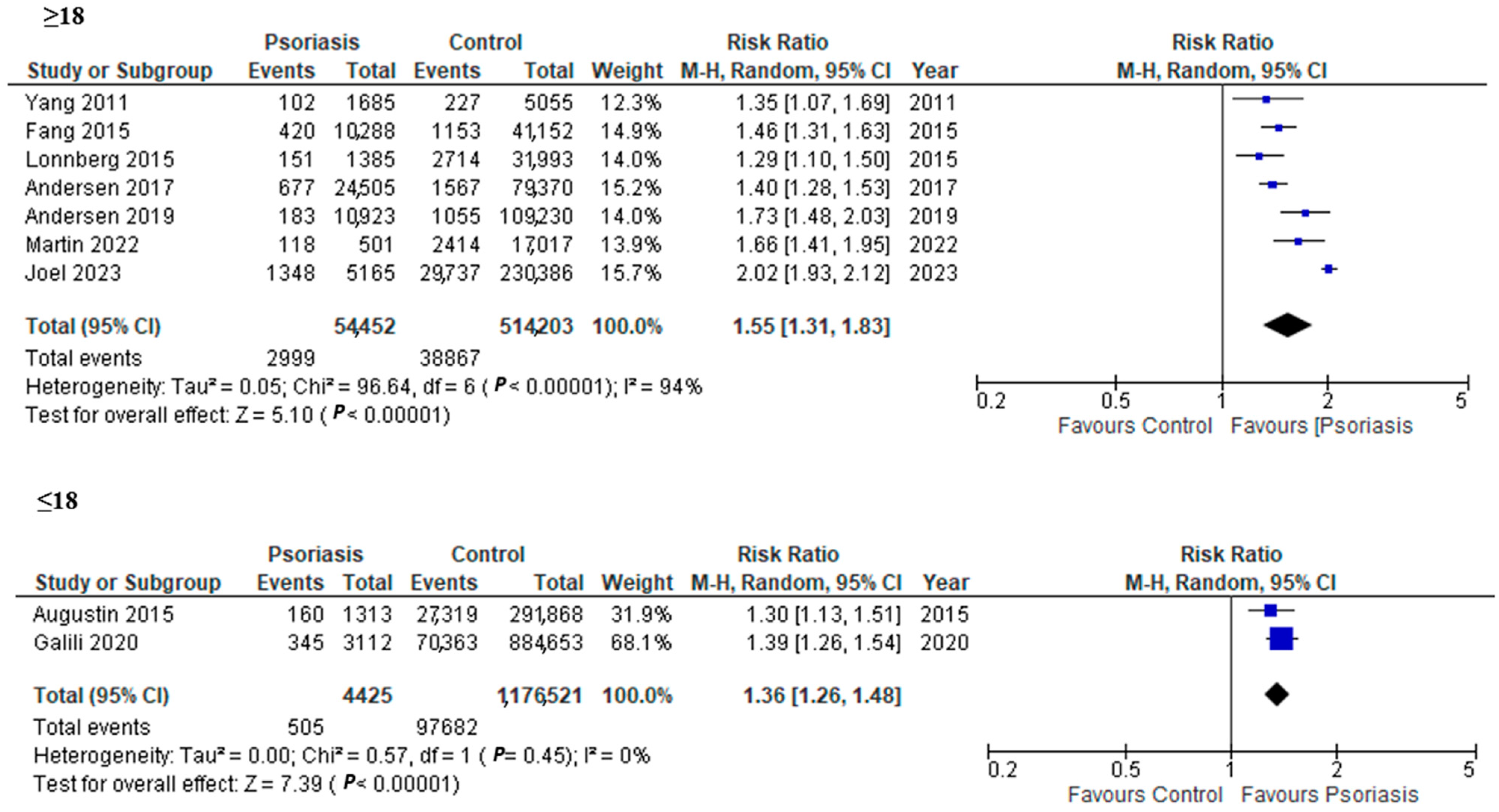
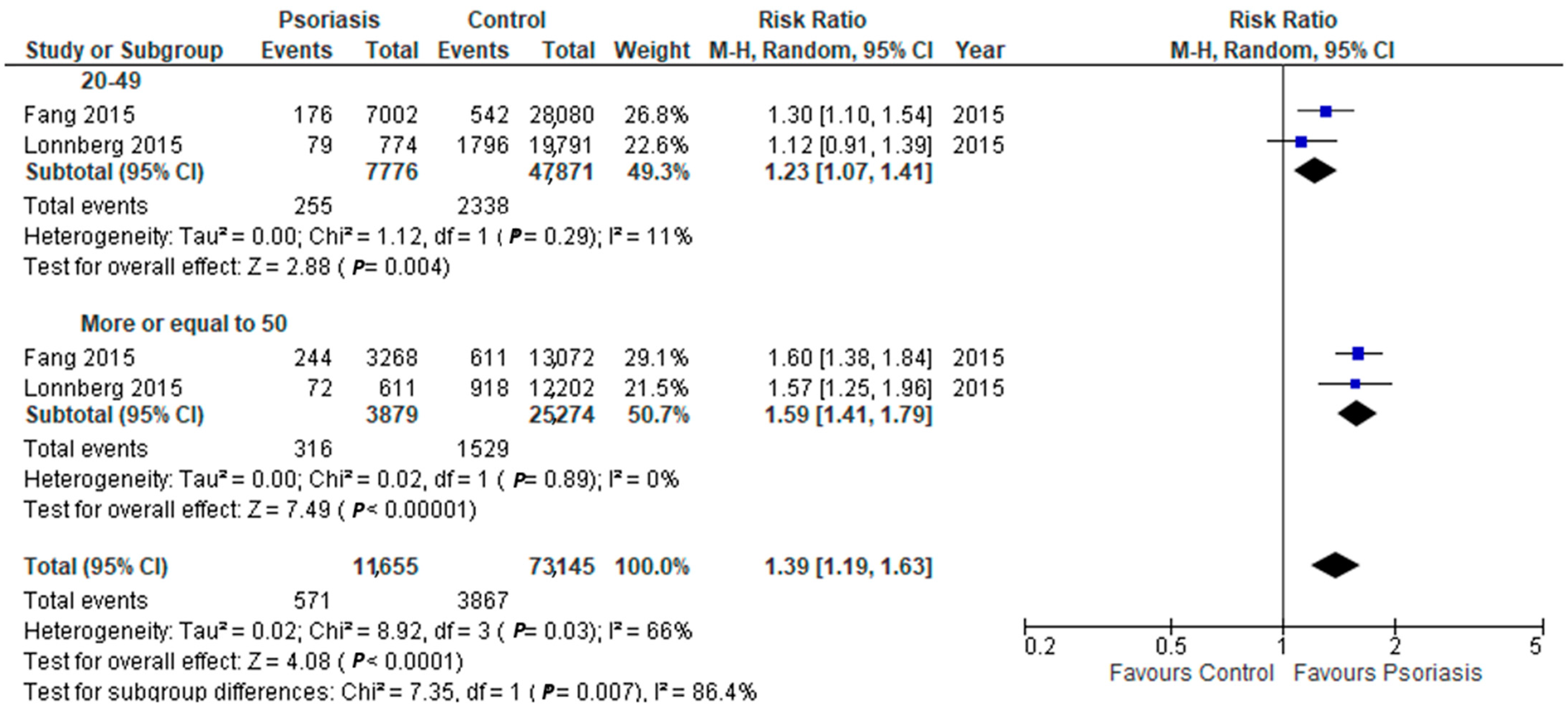
3.2. Asthma in Psoriasis Patients
3.3. Psoriasis in Asthma Patients
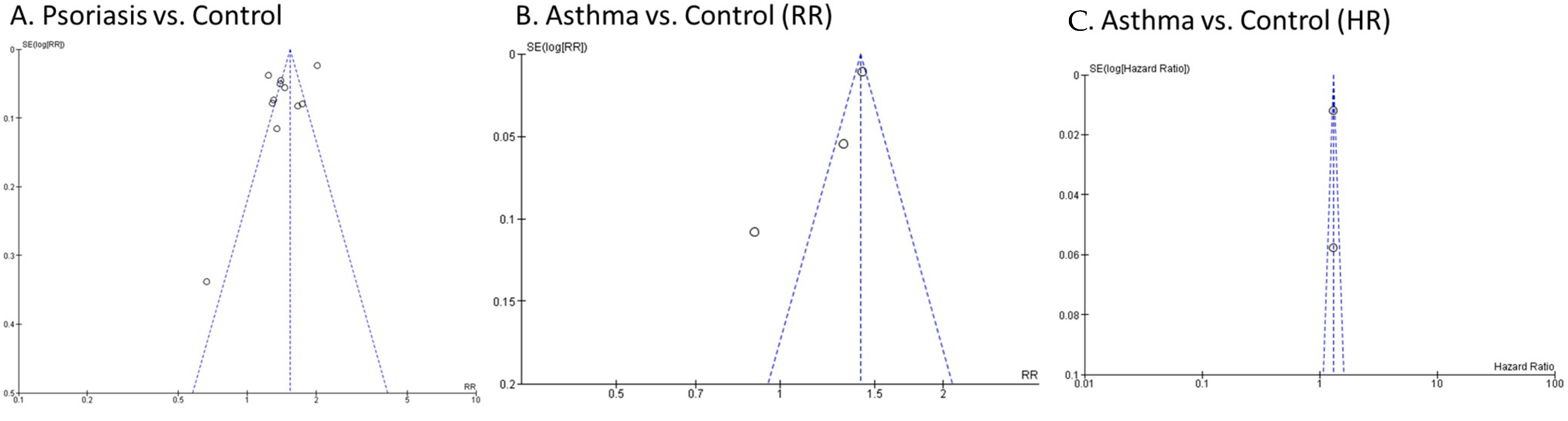
3.4. Quality Assessment and Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korman, N.J. Management of Psoriasis as a Systemic Disease: What Is the Evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Rachakonda, T.D.; Schupp, C.W.; Armstrong, A.W. Psoriasis Prevalence among Adults in the United States. J. Am. Acad. Dermatol. 2014, 70, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Singh, R.; Cloutier, M.; Gauthier-Loiselle, M.; Emond, B.; Guérin, A.; Ganguli, A. Prevalence of Psoriasis in Children and Adolescents in the United States: A Claims-Based Analysis. J. Drugs Dermatol. 2018, 17, 187–194. [Google Scholar]
- World Health Organization. Global Report on Psoriasis; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-156518-9. [Google Scholar]
- Henseler, T.; Christophers, E. Psoriasis of Early and Late Onset: Characterization of Two Types of Psoriasis Vulgaris. J. Am. Acad. Dermatol. 1985, 13, 450–456. [Google Scholar] [CrossRef]
- Schön, M.P.; Boehncke, W.-H. Psoriasis. N. Engl. J. Med. 2005, 352, 1899–1912. [Google Scholar] [CrossRef]
- Oliveira, M.; de, F.S.P.d.; Rocha, B.d.O.; Duarte, G.V. Psoriasis: Classical and Emerging Comorbidities. An. Bras. Dermatol. 2015, 90, 9–20. [Google Scholar] [CrossRef]
- Bu, J.; Ding, R.; Zhou, L.; Chen, X.; Shen, E. Epidemiology of Psoriasis and Comorbid Diseases: A Narrative Review. Front. Immunol. 2022, 13, 880201. [Google Scholar] [CrossRef]
- Tsai, T.-F.; Wang, T.-S.; Hung, S.-T.; Tsai, P.I.-C.; Schenkel, B.; Zhang, M.; Tang, C.-H. Epidemiology and Comorbidities of Psoriasis Patients in a National Database in Taiwan. J. Dermatol. Sci. 2011, 63, 40–46. [Google Scholar] [CrossRef]
- Andersen, Y.M.F.; Wu, J.J.; Thyssen, J.P.; Egeberg, A. Chronologic Order of Appearance of Immune-Mediated Inflammatory Diseases Relative to Diagnosis of Psoriasis. J. Am. Acad. Dermatol. 2019, 81, 1283–1291. [Google Scholar] [CrossRef]
- Elloso, M.M.; Gomez-Angelats, M.; Fourie, A.M. Targeting the Th17 Pathway in Psoriasis. J. Leukoc. Biol. 2012, 92, 1187–1197. [Google Scholar] [CrossRef]
- Diani, M.; Altomare, G.; Reali, E. T Helper Cell Subsets in Clinical Manifestations of Psoriasis. J. Immunol. Res. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ke, R.; Shi, W.; Yan, X.; Wang, Q.; Zhang, Q.; Chai, L.; Li, M. Association between Psoriasis and Asthma Risk: A Meta-Analysis. Allergy Asthma Proc. 2018, 39, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Fahy, J.V. Type 2 Inflammation in Asthma—Present in Most, Absent in Many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Habib, N.; Pasha, M.A.; Tang, D.D. Current Understanding of Asthma Pathogenesis and Biomarkers. Cells 2022, 11, 2764. [Google Scholar] [CrossRef] [PubMed]
- Israel, E.; Reddel, H.K. Severe and Difficult-to-Treat Asthma in Adults. N. Engl. J. Med. 2017, 377, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Gurczynski, S.J.; Moore, B.B. IL-17 in the Lung: The Good, the Bad, and the Ugly. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2018, 314, L6–L16. [Google Scholar] [CrossRef]
- Roos, A.B.; Sethi, S.; Nikota, J.; Wrona, C.T.; Dorrington, M.G.; Sandén, C.; Bauer, C.M.T.; Shen, P.; Bowdish, D.; Stevenson, C.S.; et al. IL-17A and the Promotion of Neutrophilia in Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2015, 192, 428–437. [Google Scholar] [CrossRef]
- Alnahas, S.; Hagner, S.; Raifer, H.; Kilic, A.; Gasteiger, G.; Mutters, R.; Hellhund, A.; Prinz, I.; Pinkenburg, O.; Visekruna, A.; et al. IL-17 and TNF-α Are Key Mediators of Moraxella Catarrhalis Triggered Exacerbation of Allergic Airway Inflammation. Front. Immunol. 2017, 8, 1562. [Google Scholar] [CrossRef]
- Ricciardolo, F.L.M.; Sorbello, V.; Folino, A.; Gallo, F.; Massaglia, G.M.; Favatà, G.; Conticello, S.; Vallese, D.; Gani, F.; Malerba, M.; et al. Identification of IL-17F/Frequent Exacerbator Endotype in Asthma. J. Allergy Clin. Immunol. 2017, 140, 395–406. [Google Scholar] [CrossRef]
- Östling, J.; van Geest, M.; Schofield, J.P.R.; Jevnikar, Z.; Wilson, S.; Ward, J.; Lutter, R.; Shaw, D.E.; Bakke, P.S.; Caruso, M.; et al. IL-17–High Asthma with Features of a Psoriasis Immunophenotype. J. Allergy Clin. Immunol. 2019, 144, 1198–1213. [Google Scholar] [CrossRef]
- Choy, D.F.; Hart, K.M.; Borthwick, L.A.; Shikotra, A.; Nagarkar, D.R.; Siddiqui, S.; Jia, G.; Ohri, C.M.; Doran, E.; Vannella, K.M.; et al. T H2 and Th17 Inflammatory Pathways Are Reciprocally Regulated in Asthma. Sci. Transl. Med. 2015, 7. [Google Scholar] [CrossRef]
- Yang, Y.-W.; Keller, J.J.; Lin, H.-C. Medical Comorbidity Associated with Psoriasis in Adults: A Population-Based Study. Br. J. Dermatol. 2011, 165, 1037–1043. [Google Scholar] [CrossRef]
- Hajdarbegovic, E.; Nijsten, T.; Westgeest, A.; Habraken, F.; Hollestein, L.; Thio, B. Decreased Prevalence of Atopic Features in Patients with Psoriatic Arthritis, but Not in Psoriasis Vulgaris. J. Am. Acad. Dermatol. 2013, 68, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Radtke, M.A.; Glaeske, G.; Reich, K.; Christophers, E.; Schaefer, I.; Jacobi, A. Epidemiology and Comorbidity in Children with Psoriasis and Atopic Eczema. Dermatology 2015, 231, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.-Y.; Liao, W.-C.; Lin, C.-L.; Chen, C.-H.; Kao, C.-H. Association between Psoriasis and Asthma: A Population-Based Retrospective Cohort Analysis. Br. J. Dermatol. 2015, 172, 1066–1071. [Google Scholar] [CrossRef]
- Lønnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Meteran, H.; Backer, V.; Thomsen, S.F. Asthma in Patients with Psoriasis. Br. J. Dermatol. 2015, 172, 1660–1661. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Y.M.F.; Egeberg, A.; Gislason, G.H.; Skov, L.; Thyssen, J.P. Burden of Respiratory Comorbidities in Patients with Atopic Dermatitis and Psoriasis. Br. J. Dermatol. 2017, 177, e145–e146. [Google Scholar] [CrossRef] [PubMed]
- Galili, E.; Barzilai, A.; Twig, G.; Caspi, T.; Daniely, D.; Shreberk-Hassidim, R.; Astman, N. Allergic Rhinitis and Asthma Among Adolescents with Psoriasis: A Population-Based Cross-Sectional Study. Acta Derm. Venereol. 2020, 100. [Google Scholar] [CrossRef] [PubMed]
- Joel, M.Z.; Fan, R.; Damsky, W.; Cohen, J.M. Psoriasis Associated with Asthma and Allergic Rhinitis: A US-Based Cross-Sectional Study Using the All of US Research Program. Arch. Derm. Res. 2023. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Khalid, U.; Gislason, G.H.; Mallbris, L.; Skov, L.; Hansen, P.R. Risk of Psoriasis in Patients with Childhood Asthma: A Danish Nationwide Cohort Study. Br. J. Dermatol. 2015, 173, 159–164. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Increased Risk of Psoriasis in Children and Elderly Patients with Asthma: A Longitudinal Follow-up Study Using a National Sample Cohort. Int. Forum Allergy Rhinol. 2019, 9, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Bang, C.H.; Han, K.; Ryu, J.Y.; Lee, J.Y.; Park, Y.M.; Lee, J.H. The Risk of Psoriasis in Patients with Allergic Diseases: A Nationwide Population-Based Cohort Study. Allergy Asthma Immunol. Res. 2021, 13, 638. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.W. Asthma and Psoriasis: What Do They Have in Common? IL-17A! J. Allergy Clin. Immunol. 2019, 144, 1169–1171. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, H.; Hirose, K. Role of IL-23 and Th17 Cells in Airway Inflammation in Asthma. Immune Netw. 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.Y.; Peebles, R.S. The Emerging Role of IL-23 in Asthma and Its Clinical Implications. Expert. Rev. Clin. Immunol. 2023, 19, 1–5. [Google Scholar] [CrossRef]
- Taherian, M.; Razavi, A.R.; Izad, M.; Boghozian, R.; Namdari, H.; Ghayedi, M.; Rahimzadeh, P.; Bidad, K.; Salehi, E. The Role of Interleukin-23 in Stability of in Vitro T Helper-17 Cells. Iran. J. Allergy Asthma Immunol. 2014, 13, 131–137. [Google Scholar]
- Al-Ramli, W.; Préfontaine, D.; Chouiali, F.; Martin, J.G.; Olivenstein, R.; Lemière, C.; Hamid, Q. TH17-Associated Cytokines (IL-17A and IL-17F) in Severe Asthma. J. Allergy Clin. Immunol. 2009, 123, 1185–1187. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Wills-Karp, M. The Potential Role of Interleukin-17 in Severe Asthma. Curr. Allergy Asthma Rep. 2011, 11, 388–394. [Google Scholar] [CrossRef]
- Peng, J.; Yang, X.O.; Chang, S.H.; Yang, J.; Dong, C. IL-23 Signaling Enhances Th2 Polarization and Regulates Allergic Airway Inflammation. Cell. Res. 2010, 20, 62–71. [Google Scholar] [CrossRef]
- Frieder, J.; Kivelevitch, D.; Haugh, I.; Watson, I.; Menter, A. Anti-IL-23 and Anti-IL-17 Biologic Agents for the Treatment of Immune-Mediated Inflammatory Conditions. Clin. Pharmacol. Ther. 2018, 103, 88–101. [Google Scholar] [CrossRef]
- Langley, R.G.; Lebwohl, M.; Krueger, G.G.; Szapary, P.O.; Wasfi, Y.; Chan, D.; Hsu, M.C.; You, Y.; Poulin, Y.; Korman, N.; et al. Long-term Efficacy and Safety of Ustekinumab, with and without Dosing Adjustment, in Patients with Moderate-to-severe Psoriasis: Results from the PHOENIX 2 Study through 5 Years of Follow-up. Br. J. Dermatol. 2015, 172, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, A.; Kato, T.; Kato, M.; Song, M.; Nakagawa, H.; The Japanese Ustekinumab Study Group. Efficacy and Safety of Ustekinumab in Japanese Patients with Moderate-to-Severe Plaque-Type Psoriasis: Long-Term Results from a Phase 2/3 Clinical Trial: Ustekinumab in Japanese Psoriasis Patients. J. Dermatol. 2012, 39, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.-F.; Ho, J.-C.; Song, M.; Szapary, P.; Guzzo, C.; Shen, Y.-K.; Li, S.; Kim, K.-J.; Kim, T.-Y.; Choi, J.-H.; et al. Efficacy and Safety of Ustekinumab for the Treatment of Moderate-to-Severe Psoriasis: A Phase III, Randomized, Placebo-Controlled Trial in Taiwanese and Korean Patients (PEARL). J. Dermatol. Sci. 2011, 63, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zheng, M.; Song, M.; Shen, Y.-K.; Chan, D.; Szapary, P.O.; Wang, B. LOTUS Investigators Efficacy and Safety of Ustekinumab in Chinese Patients with Moderate to Severe Plaque-Type Psoriasis: Results from a Phase 3 Clinical Trial (LOTUS). J. Drugs Dermatol. 2013, 12, 166–174. [Google Scholar] [PubMed]
- Albanesi, C.; Madonna, S.; Gisondi, P.; Girolomoni, G. The Interplay Between Keratinocytes and Immune Cells in the Pathogenesis of Psoriasis. Front. Immunol. 2018, 9, 1549. [Google Scholar] [CrossRef]
- Zaba, L.C.; Suárez-Fariñas, M.; Fuentes-Duculan, J.; Nograles, K.E.; Guttman-Yassky, E.; Cardinale, I.; Lowes, M.A.; Krueger, J.G. Effective Treatment of Psoriasis with Etanercept Is Linked to Suppression of IL-17 Signaling, Not Immediate Response TNF Genes. J. Allergy Clin. Immunol. 2009, 124, 1022–1030.e395. [Google Scholar] [CrossRef]
- Zaba, L.C.; Fuentes-Duculan, J.; Eungdamrong, N.J.; Johnson-Huang, L.M.; Nograles, K.E.; White, T.R.; Pierson, K.C.; Lentini, T.; Suárez-Fariñas, M.; Lowes, M.A.; et al. Identification of TNF-Related Apoptosis-Inducing Ligand and Other Molecules That Distinguish Inflammatory from Resident Dendritic Cells in Patients with Psoriasis. J. Allergy Clin. Immunol. 2010, 125, 1261–1268.e9. [Google Scholar] [CrossRef]
- Fuentes-Duculan, J.; Suárez-Fariñas, M.; Zaba, L.C.; Nograles, K.E.; Pierson, K.C.; Mitsui, H.; Pensabene, C.A.; Kzhyshkowska, J.; Krueger, J.G.; Lowes, M.A. A Subpopulation of CD163-Positive Macrophages Is Classically Activated in Psoriasis. J. Investig. Dermatol. 2010, 130, 2412–2422. [Google Scholar] [CrossRef]
- Lee, H.S.; Park, D.-E.; Lee, J.-W.; Chang, Y.; Kim, H.Y.; Song, W.-J.; Kang, H.-R.; Park, H.-W.; Chang, Y.-S.; Cho, S.-H. IL-23 Secreted by Bronchial Epithelial Cells Contributes to Allergic Sensitization in Asthma Model: Role of IL-23 Secreted by Bronchial Epithelial Cells. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2017, 312, L13–L21. [Google Scholar] [CrossRef]
- Li, H.; Yao, Q.; Mariscal, A.G.; Wu, X.; Hülse, J.; Pedersen, E.; Helin, K.; Waisman, A.; Vinkel, C.; Thomsen, S.F.; et al. Epigenetic Control of IL-23 Expression in Keratinocytes Is Important for Chronic Skin Inflammation. Nat. Commun. 2018, 9, 1420. [Google Scholar] [CrossRef]
- Halwani, R.; Sultana, A.; Vazquez-Tello, A.; Jamhawi, A.; Al-Masri, A.A.; Al-Muhsen, S. Th-17 Regulatory Cytokines IL-21, IL-23, and IL-6 Enhance Neutrophil Production of IL-17 Cytokines during Asthma. J. Asthma 2017, 54, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberatî, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Thatiparthi, A.; Liu, J.; Ge, S.; Egeberg, A.; Wu, J.J. Association between Psoriasis and Asthma among United States Adults in the 2009-2014 National Health and Nutrition Examination Survey. J. Am. Acad. Dermatol. 2022, 86, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Mleczko, M.; Gerkowicz, A.; Krasowska, D. Chronic Inflammation as the Underlying Mechanism of the Development of Lung Diseases in Psoriasis: A Systematic Review. IJMS 2022, 23, 1767. [Google Scholar] [CrossRef] [PubMed]
- Richer, V.; Roubille, C.; Fleming, P.; Starnino, T.; McCourt, C.; McFarlane, A.; Siu, S.; Kraft, J.; Lynde, C.; Pope, J.E.; et al. Psoriasis and Smoking: A Systematic Literature Review and Meta-Analysis with Qualitative Analysis of Effect of Smoking on Psoriasis Severity. J. Cutan. Med. Surg. 2016, 20, 221–227. [Google Scholar] [CrossRef]
- Cerveri, I.; Cazzoletti, L.; Corsico, A.G.; Marcon, A.; Niniano, R.; Grosso, A.; Ronzoni, V.; Accordini, S.; Janson, C.; Pin, I.; et al. The Impact of Cigarette Smoking on Asthma: A Population-Based International Cohort Study. Int. Arch. Allergy Immunol. 2012, 158, 175–183. [Google Scholar] [CrossRef]
- Fleming, P.; Kraft, J.; Gulliver, W.P.; Lynde, C. The Relationship of Obesity with the Severity of Psoriasis: A Systematic Review. J. Cutan. Med. Surg. 2015, 19, 450–456. [Google Scholar] [CrossRef]
- Jacobi, A.; Langenbruch, A.; Purwins, S.; Augustin, M.; Radtke, M.A. Prevalence of Obesity in Patients with Psoriasis: Results of the National Study PsoHealth3. Dermatology 2015, 231, 231–238. [Google Scholar] [CrossRef]
- Peters, S. The Impact of Comorbid Atopic Disease on Asthma: Clinical Expression and Treatment. J. Asthma 2007, 44, 149–161. [Google Scholar] [CrossRef]
- Huang, Y.J. The Respiratory Microbiome and Innate Immunity in Asthma. Curr. Opin. Pulm. Med. 2015, 21, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M.; Agnew, K.; Anagnostou, N.; Andrews, M.; Armour, K.; Baker, C.; Foley, P.; Gebauer, K.; Gupta, M.; Marshman, G.; et al. Psoriasis and Infection. A Clinical Practice Narrative. Australas. J. Derm. 2019, 60, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Kirenga, B.J.; Mugenyi, L.; De Jong, C.; Lucian Davis, J.; Katagira, W.; Van Der Molen, T.; Kamya, M.R.; Boezen, M. The Impact of HIV on the Prevalence of Asthma in Uganda: A General Population Survey. Respir. Res. 2018, 19, 184. [Google Scholar] [CrossRef]
- Alpalhão, M.; Borges-Costa, J.; Filipe, P. Psoriasis in HIV Infection: An Update. Int. J. STD AIDS 2019, 30, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Weryńska-Kalemba, M.; Filipowska-Grońska, A.; Kalemba, M.; Krajewska, A.; Grzanka, A.; Bożek, A.; Jarząb, J. Analysis of Selected Allergic Reactions among Psoriatic Patients. PDIA 2016, 1, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Baxi, S.N.; Phipatanakul, W. The Role of Allergen Exposure and Avoidance in Asthma. Adolesc. Med. State Art. Rev. 2010, 21, 57–71. [Google Scholar] [PubMed]
- Kapoor, B.; Gulati, M.; Rani, P.; Gupta, R. Psoriasis: Interplay between Dysbiosis and Host Immune System. Autoimmun. Rev. 2022, 21, 103169. [Google Scholar] [CrossRef] [PubMed]
- Hufnagl, K.; Pali-Schöll, I.; Roth-Walter, F.; Jensen-Jarolim, E. Dysbiosis of the Gut and Lung Microbiome Has a Role in Asthma. Semin. Immunopathol. 2020, 42, 75–93. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The Association between Psoriasis and Hypertension: A Systematic Review and Meta-Analysis of Observational Studies. J. Hypertens. 2013, 31, 433–443. [Google Scholar] [CrossRef]
- Coto-Segura, P.; Eiris-Salvado, N.; González-Lara, L.; Queiro-Silva, R.; Martinez-Camblor, P.; Maldonado-Seral, C.; García-García, B.; Palacios-García, L.; Gomez-Bernal, S.; Santos-Juanes, J.; et al. Psoriasis, Psoriatic Arthritis and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Br. J. Dermatol. 2013, 169, 783–793. [Google Scholar] [CrossRef]
- Salihbegovic, E.; Hadzigrahic, N.; Suljagic, E.; Kurtalic, N.; Hadzic, J.; Zejcirovic, A.; Bijedic, M.; Handanagic, A. Psoriasis and Dyslipidemia. Mater. Sociomed. 2015, 27, 15. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, S.F.; Quesenberry, C.P.; Van Den Eeden, S.K.; Shan, J.; Ferrara, A. Patients Diagnosed with Diabetes Are at Increased Risk for Asthma, Chronic Obstructive Pulmonary Disease, Pulmonary Fibrosis, and Pneumonia but Not Lung Cancer. Diabetes Care 2010, 33(1), 55–60. [Google Scholar] [CrossRef] [PubMed]
- Song, W.-J.; Niimi, A. Angiotensin-Converting Enzyme Inhibitors, Asthma, and Cough: Relighting the Torch. J. Allergy Clin. Immunol. Pract. 2021, 9, 3440–3441. [Google Scholar] [CrossRef] [PubMed]
- Balak, D.; Hajdarbegovic, E. Drug-Induced Psoriasis: Clinical Perspectives. PTT 2017, 7, 87–94. [Google Scholar] [CrossRef]
- Rongioletti, F.; Fiorucci, C.; Parodi, A. Psoriasis Induced or Aggravated by Drugs. J. Rheumatol. Suppl. 2009, 83, 59–61. [Google Scholar] [CrossRef]
- Ohyama, K.; Arai, H.; Sugiura, M.; Hori, Y. Psoriasis Associated with ACE Inhibitors: An Analysis of the FAERS Database. Pharmazie 2020, 75, 524–526. [Google Scholar]
- Wu, S.; Han, J.; Qureshi, A. Use of Aspirin, Non-Steroidal Anti-Inflammatory Drugs, and Aceta minophen (Paracetamol), and Risk of Psoriasis and Psoriatic Arthritis: A Cohort Study. Acta Derm. Venerol. 2015, 95, 217–222. [Google Scholar] [CrossRef]
- Reich, K. The Concept of Psoriasis as a Systemic Inflammation: Implications for Disease Management: Systemic Disease and Therapy for Psoriasis. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 3–11. [Google Scholar] [CrossRef]
- Chang, H.S.; Lee, T.-H.; Jun, J.A.; Baek, A.R.; Park, J.-S.; Koo, S.-M.; Kim, Y.-K.; Lee, H.S.; Park, C.-S. Neutrophilic Inflammation in Asthma: Mechanisms and Therapeutic Considerations. Expert. Rev. Respir. Med. 2017, 11, 29–40. [Google Scholar] [CrossRef]
- Lowes, M.A.; Russell, C.B.; Martin, D.A.; Towne, J.E.; Krueger, J.G. The IL-23/T17 Pathogenic Axis in Psoriasis Is Amplified by Keratinocyte Responses. Trends Immunol. 2013, 34, 174–181. [Google Scholar] [CrossRef]
- Singh, T.P.; Schön, M.P.; Wallbrecht, K.; Gruber-Wackernagel, A.; Wang, X.-J.; Wolf, P. Involvement of IL-9 in Th17-Associated Inflammation and Angiogenesis of Psoriasis. PLoS ONE 2013, 8, e51752. [Google Scholar] [CrossRef] [PubMed]
- Bullens, D.M.; Truyen, E.; Coteur, L.; Dilissen, E.; Hellings, P.W.; Dupont, L.J.; Ceuppens, J.L. IL-17 MRNA in Sputum of Asthmatic Patients: Linking T Cell Driven Inflammation and Granulocytic Influx? Respir. Res. 2006, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Elder, J.T. Genome-Wide Association Scan Yields New Insights into the Immunopathogenesis of Psoriasis. Genes. Immun. 2009, 10, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Weidinger, S.; Willis-Owen, S.; Kamatani, Y.; Baurecht, H.; Morar, N.; Liang, L.; Edser, P.; Street, T.; Rodriguez, E.; O’Regan, G.M.; et al. A Genome-Wide Association Study of Atopic Dermatitis Identifies Loci with Overlapping Effects on Asthma and Psoriasis. Hum. Mol. Genet. 2013, 22, 4841–4856. [Google Scholar] [CrossRef] [PubMed]
- Kere, J. Mapping Genes for Asthma and Psoriasis. Novartis Found. Symp. 2008, 360, 46–56. [Google Scholar] [CrossRef]
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. IJMS 2019, 20, 1475. [Google Scholar] [CrossRef]
- Sofen, H.; Smith, S.; Matheson, R.T.; Leonardi, C.L.; Calderon, C.; Brodmerkel, C.; Li, K.; Campbell, K.; Stanley, J.M., Jr.; Wasfi, Y.; et al. Guselkumab (an IL-23-Specific MAb) Demonstrates Clinical and Molecular Response in Patients with Moderate-to-Severe Psoriasis. J. Allergy Clin. Immunol. 2014, 133, 1032–1040. [Google Scholar] [CrossRef]
- Liu, T.; Li, S.; Ying, S.; Tang, S.; Ding, Y.; Li, Y.; Qiao, J.; Fang, H. The IL-23/IL-17 Pathway in Inflammatory Skin Diseases: From Bench to Bedside. Front. Immunol. 2020, 11, 594735. [Google Scholar] [CrossRef]
- Brightling, C.E.; Nair, P.; Cousins, D.J.; Louis, R.; Singh, D. Risankizumab in Severe Asthma—A Phase 2a, Placebo-Controlled Trial. N. Engl. J. Med. 2021, 385, 1669–1679. [Google Scholar] [CrossRef]
- Busse, W.W.; Holgate, S.; Kerwin, E.; Chon, Y.; Feng, J.; Lin, J.; Lin, S.-L. Randomized, Double-Blind, Placebo-Controlled Study of Brodalumab, a Human Anti–IL-17 Receptor Monoclonal Antibody, in Moderate to Severe Asthma. Am. J. Respir. Crit. Care Med. 2013, 188, 1294–1302. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Source and Site | Study Design | Region | Diagnosis Criteria Psoriasis/Asthma | Cases n/N | Control n/N | Included Age |
|---|---|---|---|---|---|---|---|
| Tsai, 2011 [9] | National Health Insurance Research Database (NHIRD) (1995–2008). Taiwan | Retrospective cohort | Asian | ICD-9-CM codes 696.0, 696.1/493.0, 493.1, 493.9 | 861/51,800 (1.66) | 2793/207,200 (1.35) | All ages |
| Yang, 2011 [23] | Longitudinal Health Insurance Database 2000 (LHID 2000) (2006–2007). Taiwan | Cross-sectional | Asian | ICD-9-CM code 696.1 or 696.0/ICD-9-CM NC | 102/1685 (6.05) | 227/5055 (4.49) | ≥18 |
| Hajdarbegovic, 2013 [24] | Department of Dermatology at Erasmus medical center (2009–2011). Netherlands | Cross-sectional | Europe | Certified dermatologist or rheumatologist/self-reported | 19/301 (6.31) | 14/147 (9.52) | All ages |
| Augustin, 2015 [25] | German statutory health insurance company (from 2009). Germany | Retrospective cohort | Europe | ICD-10 CODES L40/ICD-10 code NC | 160/1313 (12.19) | 27,319/291,868 (9.36) | <18 |
| Fang, 2015 [26] | Longitudinal Health Insurance Database (LHID) (1996–2010). Taiwan | Retrospective cohort | Asian | ICD-9-CM codes 696, 696.0, 696.1, 696.8/ICD-9-CM code 493 | 420/10,288 (4.08) | 1153/41,152 (2.80) | ≥20 |
| Lonnberg, 2015 [27] | Nationwide Danish Twin Registry. Denmark | Cross-sectional | Europe | Self-reported/Self-reported | 151/1385 (10.90) | 2714/31,993 (8.48) | 20–71 |
| Andersen, 2017 [28] | Danish Administrative Registries (1995–2012). Denmark | Cross-sectional | Europe | Self-reported/self-reported | 677/24,505 (2.76) | 1567/79,370 (1.97) | ≥18 |
| Andersen, 2019 [10] | Danish National patient registry (DNPR) (2007–2016). Denmark | Retrospective cohort | Europe | ICD-10 code L40/ICD-10 NC | 183/10,923 (1.68) | 1055/109,230 (0.97) | ≥18 |
| Galili, 2020 [29] | Database of the Israel Defense Force (IDF) (1999–2014). Israel | Cross-sectional | Europe | Clinically by dermatologist/pulmonologist | 345/3112 (11.09) | 70,636/884,653 (7.98) | 16–18 |
| Martin, 2022 [55] | National Health and Nutrition Examination Survey (2009–2014). USA | Cross-sectional | America | Self-reported/Self-reported | 118/501 (23.55) | 2414/17,017 (14.19) | ≥20 |
| Joel, 2023 [30] | All of US research program (2018–2022). USA | Cross-sectional | America | SNOMED codes 9014002/195967001 | 1348/5162 (26.11) | 29,737/230,386 (12.91) | ≥18 |
| Study | Source of Study. Study Site | Study Design | Region | Diagnosis Criteria Asthma/Psoriasis | Cases n/N | Control n/N | Included Age |
|---|---|---|---|---|---|---|---|
| Egeberg, 2015 [31] | The Danish National Patient Register. Denmark (1997–2011) | Retrospective cohort study | Europe | ICD-10 J45/ L40, M070-M073 | 87/21,725 (0.40) | 6499/1,456,385 (0.45) | 6–14 |
| Kim, 2019 [32] | Korean Health Insurance Review and Assessment Service-National Sample Cohort (HIRA-NSC) (2002–2013). Republic of Korea | Retrospective cohort | Asian | ICD-10 J45-46 code/B02 | 771/167,693 (0.46) | 589/167,693 (0.35) | All ages |
| Han, 2021 [33] | KNHIS database (2010–2017). Republic of Korea | Retrospective cohort | Asian | ICD-10 J45-46 code/L40 | 8340/279,451 (2.98) | ≥20 |
| Study, Year | Selection | Comparability | Outcome | Rating |
|---|---|---|---|---|
| Tsai, 2011 [9] | 4 | 2 | 3 | 9 |
| Yang, 2011 [23] | 4 | 2 | 1 | 7 |
| Hajdarbegovic, 2013 [24] | 3 | 2 | 0 | 5 |
| Augustin, 2015 [25] | 3 | 0 | 1 | 4 |
| Fang, 2015 [26] | 4 | 2 | 3 | 9 |
| Lǿnnberg, 2015 [27] | 2 | 2 | 0 | 4 |
| Egeberg, 2015 [31] | 4 | 2 | 3 | 9 |
| Andersen, 2017 [28] | 3 | 2 | 1 | 6 |
| Andersen, 2019 [10] | 4 | 2 | 3 | 9 |
| Kim, 2019 [32] | 4 | 2 | 3 | 9 |
| Galili, 2020 [29] | 4 | 2 | 3 | 9 |
| Han, 2021 [33] | 4 | 2 | 3 | 9 |
| Martin, 2022 [55] | 2 | 2 | 0 | 4 |
| Joel, 2023 [30] | 3 | 2 | 1 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, A.; Ramdass, P.V.A.K.; Ramos-Nino, M.E. Bidirectional Association between Psoriasis and Asthma: A Systematic Review and Meta-Analysis. J. Respir. 2023, 3, 60-74. https://doi.org/10.3390/jor3020007
Garcia A, Ramdass PVAK, Ramos-Nino ME. Bidirectional Association between Psoriasis and Asthma: A Systematic Review and Meta-Analysis. Journal of Respiration. 2023; 3(2):60-74. https://doi.org/10.3390/jor3020007
Chicago/Turabian StyleGarcia, Ashley, Prakash V. A. K. Ramdass, and Maria E. Ramos-Nino. 2023. "Bidirectional Association between Psoriasis and Asthma: A Systematic Review and Meta-Analysis" Journal of Respiration 3, no. 2: 60-74. https://doi.org/10.3390/jor3020007