
Platelet Concentration and Platelet/Lymphocyte Ratio as Prognostic Indicators in Luminal Breast Cancer

 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of the Patients
3.2. Establishment of Cutoff—ROC Curves
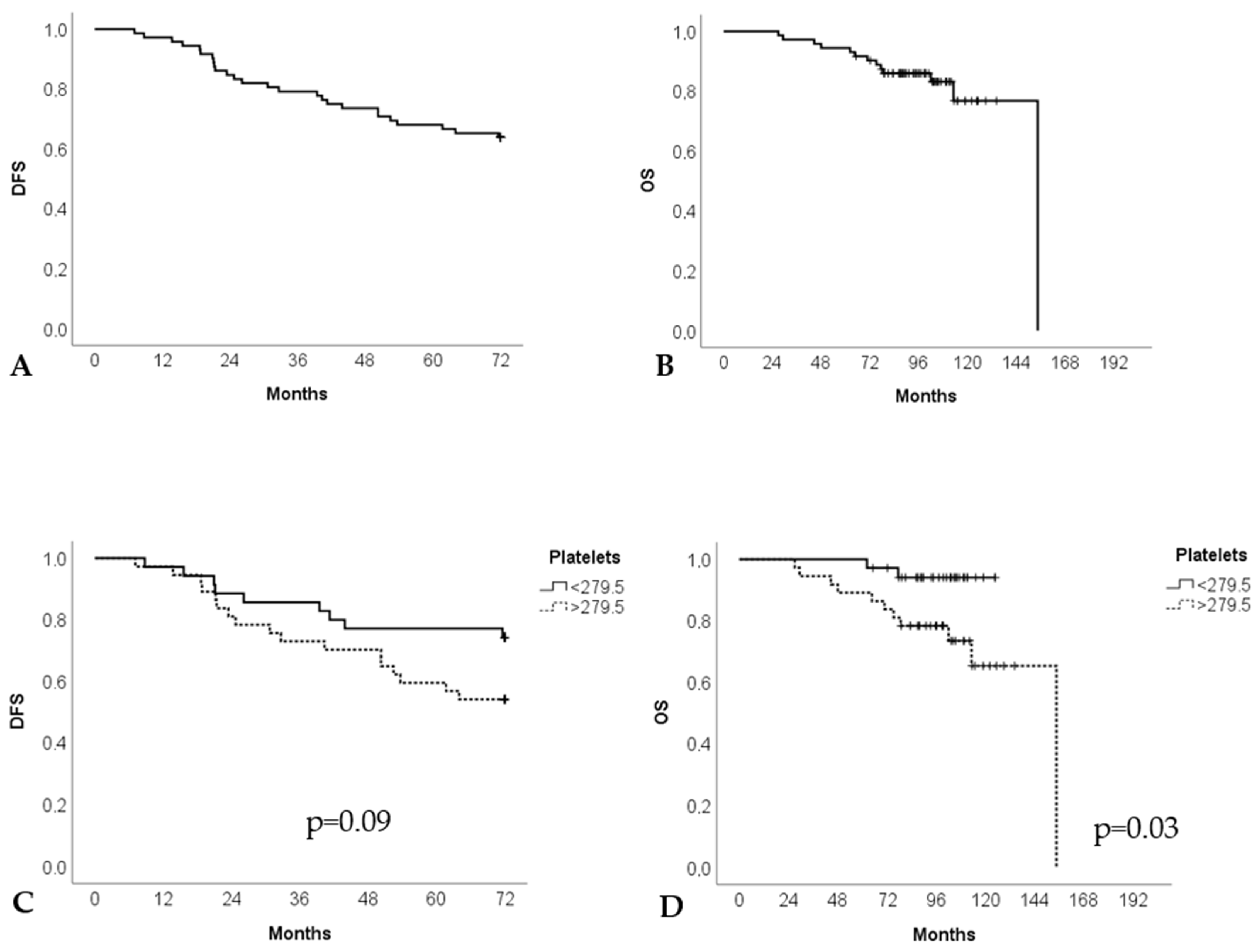
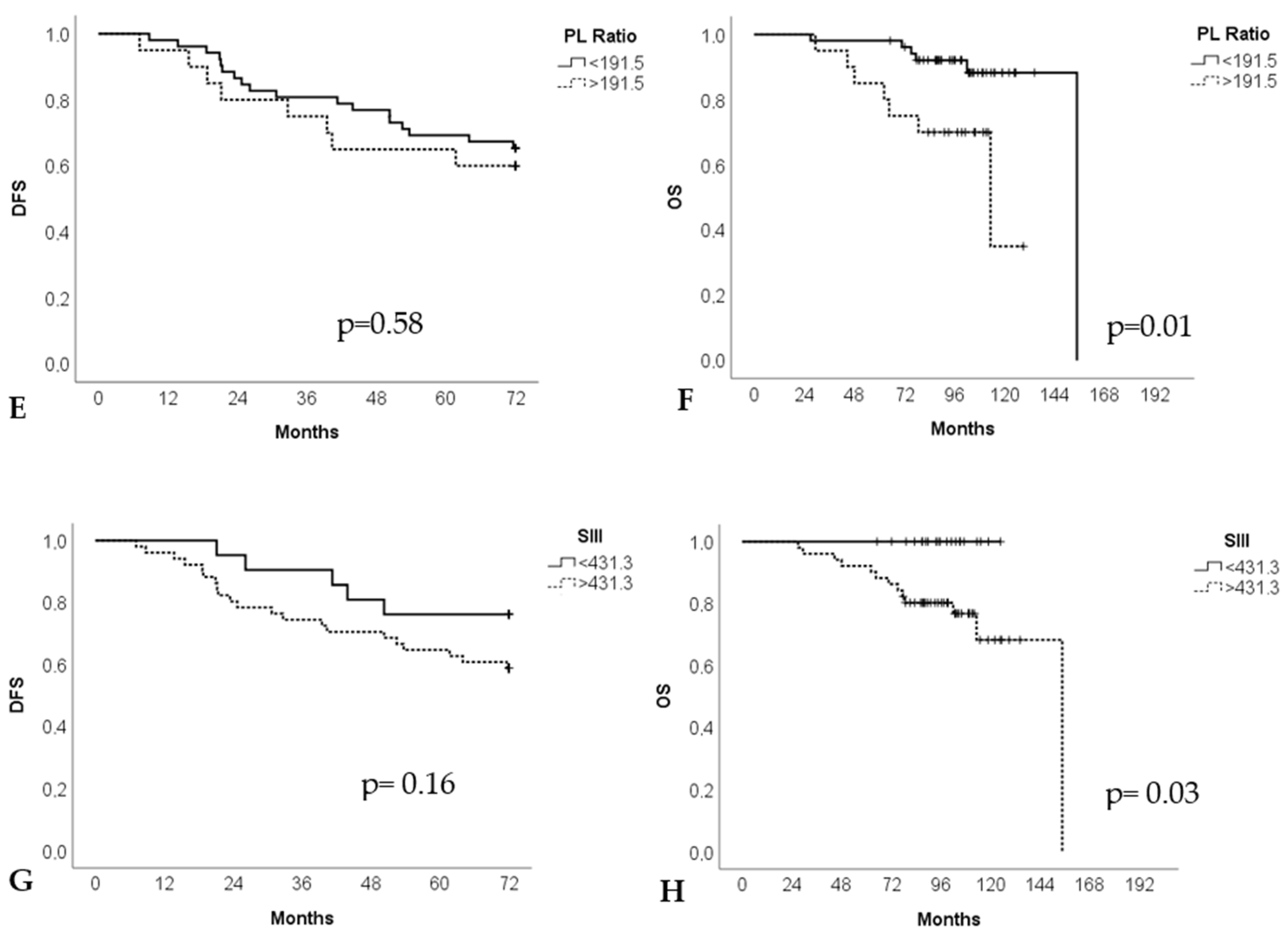
3.3. Prognostic Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferroni, P.; Santilli, F.; Cavaliere, F.; Simeone, P.; Costarelli, L.; Liani, R.; Tripaldi, R.; Riondino, S.; Roselli, M.; Davi, G.; et al. Oxidant stress as a major determinant of platelet activation in invasive breast cancer. Int. J. Cancer 2017, 140, 696–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, A.C.; Panis, C.; Victorino, V.J.; Campos, F.C.; Colado-Simão, A.N.; Cecchini, A.L.; Cecchini, R. Molecular subtype is determinant on inflammatory status and immunological profile from invasive breast cancer patients. Cancer Immunol. Immunother. 2012, 61, 2193–2201. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, X.; Qiu, J.; Pang, T.; Huang, L.; Zeng, Q. Comparisons of p53, KI67 and BRCA1 expressions in patients with different molecular subtypes of breast cancer and their relationships with pathology and prognosis. J. BUON 2019, 24, 2361–2368. [Google Scholar] [PubMed]
- Becht, E.; Giraldo, N.A.; Germain, C.; de Reyniès, A.; Laurent-Puig, P.; Zucman-Rossi, J.; Dieu-Nosjean, M.C.; Sautès-Fridman, C.; Fridman, W.H. Immune Contexture, Immunoscore, and Malignant Cell Molecular Subgroups for Prognostic and Theranostic Classifications of Cancers. Adv. Immunol. 2016, 130, 95–190. [Google Scholar]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Borniger, J.C. Central regulation of breast cancer growth and metastasis. J. Cancer Metastasis Treat. 2019, 5, 23. [Google Scholar] [CrossRef]
- Masood, S. Prognostic/predictive factors in breast cancer. Clin. Lab. Med. 2005, 25, 809–825. [Google Scholar] [CrossRef]
- Galdiero, M.R.; Bonavita, E.; Barajon, I.; Garlanda, C.; Mantovani, A.; Jaillon, S. Tumor associated macrophages and neutrophils in cancer. Immunobiology 2013, 218, 1402–1410. [Google Scholar] [CrossRef]
- Wira Wiguna, I.G.W.; Indrani Remitha, N.P.S.; Sadvika, I.G.A.S.; Wiranata, S.; Putra, I.W.A.S.; Adiputra, P.A.T.; Supadmanaba, I.G.P.; Wihandani, D.M. Pretreatment Leukocyte Count Ratios as Metastatic Predictive Factors in Luminal Type Breast Cancer. Asian Pac. J. Cancer Prev. 2022, 23, 1595–1601. [Google Scholar] [CrossRef]
- De Giorgi, U.; Mego, M.; Scarpi, E.; Giordano, A.; Giuliano, M.; Valero, V.; Alvarez, R.H.; Ueno, N.T.; Cristofanilli, M.; Reuben, J.M. Association between circ ulating tumor cells and peripheral blood monocytes in metastatic breast cancer. Ther. Adv. Med. Oncol. 2019, 11, 1758835919866065. [Google Scholar] [CrossRef] [Green Version]
- Panni, R.Z.; Lopez, A.G.; Liu, J.; Poultsides, G.A.; Rocha, F.G.; Hawkins, W.G.; Strasberg, S.M.; Trikalinos, N.A.; Maithel, S.; Fields, R.C. and other members of US-NETSG. Association of preoperative monocyte-to-lymphocyte and neutrophil-to-lymphocyte ratio with recurrence-free and overall survival after resection of pancreatic neuroendocrine tumors (US-NETSG). J. Surg. Oncol. 2019, 120, 632–638. [Google Scholar]
- Rao, J.S.; Hanumappa, H.K.; Joseph, E.P.; Chowdappa, R.G.; Ramesh, R. Elevated Neutrophil–Lymphocyte Ratio in Luminal-Type Locally Advanced Breast Cancer to Circumvent Neo-Adjuvant Chemotherapy. Indian J. Surg. Oncol. 2019, 10, 454–459. [Google Scholar]
- Valpione, S.; Martinoli, C.; Fava, P.; Mocellin, S.; Campana, L.G.; Quaglino, P.; Ferrucci, P.F.; Pigozzo, J.; Astrua, C.; Testori, A.; et al. Personalised medicine: Development and external validation of a prognostic model for metastatic melanoma patients treated with ipilimumab. Eur. J. Cancer 2015, 51, 2086–2094. [Google Scholar] [CrossRef]
- Leblanc, R.; Peyruchaud, O. Metastasis: New functional implications of platelets and megakaryocytes. Blood 2016, 128, 24–31. [Google Scholar] [CrossRef]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Früh, M. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer 2017, 111, 176–181. [Google Scholar] [CrossRef]
- Guthrie, G.J.; Charles, K.A.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil-lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef]
- Ogihara, K.; Kikuchi, E.; Yuge, K.; Yanai, Y.; Matsumoto, K.; Miyajima, A.; Asakura, H.; Oya, M. The preoperative neutrophil-to-lymphocyte ratio is a novel biomarker for predicting worse clinical outcomes in non-muscle invasive bladder cancer patients with a previous history of smoking. Ann. Surg. Oncol. 2016, 23, 1039–1047. [Google Scholar] [CrossRef]
- Landskron, G.; De la Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic inflammation and cytokines in the tumor microenvironment. J. Immunol. Res. 2014, 2014, 149185. [Google Scholar] [CrossRef] [Green Version]
- Ravelli, A.; Roviello, G.; Cretella, D.; Cavazzoni, A.; Biondi, A.; Cappelletti, M.R.; Zanotti, L.; Ferrero, G.; Ungari, M.; Zanconati, F.; et al. Tumor-infiltrating lymphocytes and breast cancer: Beyond the prognostic and predictive utility. Tumor Biol. 2017, 39, 1010428317695023. [Google Scholar] [CrossRef] [Green Version]
- Jia, W.; Wu, J.; Jia, H.; Yang, Y.; Zhang, X.; Chen, K.; Su, F. The Peripheral Blood Neutrophil-To-Lymphocyte Ratio Is Superior to the Lymphocyte-To-Monocyte Ratio for Predicting the Long-Term Survival of Triple Negative Breast Cancer Patients. PLoS ONE 2015, 10, e0143061. [Google Scholar] [CrossRef]
- Noh, H.; Eomm, M.; Han, A. Usefulness of pretreatment neutrophil to lymphocyte ratio in predicting disease-specific survival in breast cancer patients. J. Breast Cancer 2013, 16, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Buyukkaya, E.; Karakas, M.F.; Karakas, E.; Akçay, A.B.; Tanboga, I.H.; Kurt, M.; Sen, N. Correlation of neutrophil to lymphocyte ratio with the presence and severity of metabolic syndrome. Clin. Appl. Thromb. Hemost. 2014, 20, 159–163. [Google Scholar] [CrossRef] [Green Version]
- Lal, I.; Dittus, K.; Holmes, C.E. Platelets, coagulation, and fibrinolysis in breast cancer progression. Breast Cancer Res. 2013, 15, 207. [Google Scholar] [CrossRef] [PubMed]
- Krenn-Pilko, S.; Langsenlehner, U.; Thurner, E.M.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S.; Langsenlehner, T. The elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis in breast cancer patients. Brit. J. Cancer 2014, 110, 2524–2530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Ma, Y.; Sun, L.; Shi, Y.; Jiang, S.; Yu, K.; Zhou, S. Prognostic Significance of Pretreatment Neutrophil/Lymphocyte Ratio and Platelet/Lymphocyte Ratio in Patients with Diffuse Large B-Cell Lymphoma. Biomed Res. Int. 2018, 2018, 9651254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliwell, B. Oxidative stress and cancer: Have we moved forward? Biochem. J. 2007, 401, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Bekele, R.T.; Venkatraman, G.; Liu, R.Z.; Tang, X.; Mi, S.; Benesch, M.G.; Mackey, J.R.; Godbout, R.; Curtis, J.M.; McMullen, T.P.; et al. Oxidative stress contributes to the tamoxifen-induced killing of breast cancer cells: Implications for tamoxifen therapy and resistance. Sci. Rep. 2016, 6, 21164. [Google Scholar] [CrossRef] [Green Version]
- Azab, B.; Shah, N.; Radbel, J.; Tan, P.; Bhatt, V.; Vonfrolio, S.; Habeshy, A.; Picon, A.; Bloom, S. Pretreatment neutrophil/lymphocyte ratio is superior to platelet/lymphocyte ratio as a predictor of long-term mortality in breast cancer patients. Med. Oncol. 2013, 30, 432. [Google Scholar] [CrossRef]
- Tao, Z.; Shi, A.; Lu, C.; Song, T.; Zhang, Z.; Zhao, J. Breast Cancer: Epidemiology and Etiology. Cell Biochem. Biophys. 2015, 272, 333–338. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Blohmer, J.U.; Costa, S.D.; Denkert, C.; Eidtmann, H.; Eiermann, W.; Gerber, B.; Hanusch, C.; Hilfrich, J.; Huober, J.; et al. Response-Guided Neoadjuvant Chemotherapy for Breast Cancer. J. Clin. Oncol. 2013, 31, 3623–3630. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Relapse | Death | |||||
|---|---|---|---|---|---|---|
| Characteristic | N (%) | Without 46 (63.9) | With 26 (36.1) | Without 59 (81.9) | With 13 (18.1) | Total 72 (100) |
| Age at diagnosis (72) | 47.0 ± 12.2 | 46.1 ± 12.6 | 47.3 ± 12.8 | 44.2 ± 9.88 | ||
| ≤40 year | 32 (44) | 19 (41.3) | 13 (50.0) | 25 (42.4) | 7 (53.8) | 32 (44.4) |
| 40 to 60 years | 30 (42) | 20 (43.5) | 10 (38.5) | 25 (43.5) | 5 (38.5) | 30 (41.7) |
| ≥60 years | 10 (14) | 7 (15.2) | 3 (11.5) | 9 (15.3) | 1 (7.7) | 10 (13.9) |
| Tumoral grade (72) | ||||||
| I | 12 (16.7) | 11 (23.9) | 1 (3.8) * | 12 (20.3) | 0 (0.0) | 12 (16.7) |
| II | 35 (48.6) | 24 (52.2) | 11 (42.3) * | 29 (49.2) | 6 (46.2) | 35 (48.6) |
| III Clinical staging (71) | 25 (34.7) | 11 (23.9) | 14 (53.8) * | 18 (30.5) | 7 (53.8) | 25 (34.7) |
| T1 | 27 (37.5) | 23 (50.0) | 4 (15.4) ** | 26 (44.8) | 1 (7.7) * | 27 (38.0) |
| T2 | 29 (40.3) | 19 (41.3) | 10 (38.5) ** | 24 (41.4) | 5 (38.5) * | 29 (40.8) |
| T3/T4 | 15 (20.8) | 4 (8.7) | 11 (42.3) ** | 8 (13.8) | 7 (53.8) * | 15 (21.2) |
| N0 | 36 (50.0) | 32 (69.6) | 4 (15.4) ** | 33 (56.9) | 3 (23.1) * | 36 (50.7) |
| N1 | 20 (27.8) | 12 (26.1) | 8 (30.8) ** | 16 (27.6) | 4 (30.8) * | 20 (28.2) |
| N2/N3 | 15 (20.8) | 2 (4,4) | 13 (50.0) ** | 9 (15.5) | 6 (46.1) * | 15 (21.1) |
| Treatment | ||||||
| Radiotherapy | 62/69 (86.1) | 39 (62.9) | 23 (37.1) | 49 (87.5) | 13 (100) | 62/69 (89.8) |
| Chemotherapy | 16/61 (22.2) | 27 (44.3) | 18 (29.5) ** | 36 (69.2) | 9 (100) | 45/61 (73.8) |
| Histology (72) | ||||||
| Ductal | 63 (87.5) | 41 (65.1) | 22(34.9) | 52 (82.5) | 11 (17.4) | 63 (87.5) |
| Lobular | 9 (12.5) | 5 (55.5) | 4 (44.4) | 7 (77.8) | 2 (22.2) | 9 (12.5) |
| Immunohistochemistry (72) | ||||||
| Ki 67 < 14 | 45/72 (62.5) | 33 (73.3) | 12 (26.7) | 39 (66.1) | 6 (46.2) | 45 (62.5) |
| Ki 67 > 14 | 27/72 (37.5) | 14 (51.8) | 13 (48.2) | 20 (33.9) | 7 (53.8) | 27 (37.5) |
| Variable | N | Platelet (×103/mm3) | p | |
|---|---|---|---|---|
| <297 | >297 | |||
| Age at diagnosis | 72 | 43 (100) | 29 (100) | 0.35 |
| ≤40 years | 32 | 21 (48.8) | 11 (37.9) | |
| 40 to 60 years | 30 | 18 (41.9) | 12 (41.1) | |
| ≥60 years | 10 | 4 (9.3) | 6 (20.7) | |
| Median ± std deviation | 45.2 ± 11.7 | 49.1 ± 13.0 | 0.19 | |
| Tumoral grade | 72 | 43 (100) | 29 (100) | 0.08 |
| I | 12 | 10 (23.3) | 2 (6.9) | |
| II | 35 | 22 (51.2) | 13 (44.8) | |
| III | 25 | 11 (25.6) | 14 (48.3) | |
| Clinical staging | 71 | 42 (100) | 29 (100) | |
| T1 | 27 | 21 (50.0) | 6 (20.7) | 0.01 |
| T2 | 29 | 16 (38.1) | 13 (44.8) | |
| T3 | 7 | 4 (9.5) | 3 (10.3) | |
| T4 | 8 | 1 (2.4) | 7 (24.1) | |
| N0 | 71 | 24 (57.1) | 12 (41.4) | 0.01 |
| N1 | 20 | 15 (35.7) | 5 (17.2) | |
| N2 | 8 | 3 (7.1) | 5 (17.2) | |
| N3 | 7 | 0 (0.0) | 7 (24.1) | |
| Relapse | 72 | 43 (100) | 29 (100) | 0.04 |
| No | 46 | 32 (69.6) | 14 (30.4) | |
| Yes | 26 | 11 (42.3) | 15 (57.7) | |
| Death | 72 | 43 (100) | 29 (100) | 0.04 |
| No | 59 | 39 (66.1) | 20 (33.9) | |
| Yes | 13 | 4 (30.8) | 9 (69.2) | |
| Radiotherapy | 69 | 40 (100) | 29 (100) | 0.69 |
| No | 7 | 5 (12.5) | 2 (6.9) | |
| Yes | 62 | 35 (87.5) | 27 (93.1) | |
| Chemotherapy | 61 | 39 (100) | 22 (100) | 0.44 |
| No | 16 | 12 (30.8) | 4 (18.2) | |
| Yes | 45 | 27 (69.2) | 18 (81.8) | |
| Histology | 72 | 43 (100) | 29 (100) | 0.73 |
| Ductal | 63 | 37 (86.0) | 26 (89.7) | |
| Lobular | 9 | 6 (14.0) | 3 (10.3) | |
| Leukocyte | 72 | 6124 ± 2057 | 7355 ± 1986 | 0.01 |
| Neutrophil | 72 | 3647 ± 1419 | 4605 ± 1635 | 0.01 |
| Lymphocyte | 72 | 1788 ± 743 | 1969 ± 650 | 0.29 |
| Monocyte | 72 | 483 ± 176 | 576 ± 154 | 0.02 |
| 6 years DFS (95% CI) | 72 | 60.9 (54.7–67.2) | 54.0 (46.3–61.6) | 0.04 |
| 6 years OS (95% CI) | 72 | 119.1 (113.6–124.6) | 127.4 (110.1 ± 144.7) | 0.08 |
| Variable | N | PLR | p | Platelet (×103/mm3) | p | SII | p | |||
|---|---|---|---|---|---|---|---|---|---|---|
| <191.5 | >191.5 | <279 | >279 | <431.3 | >431.3 | |||||
| Age at diagnosis | 72 | 46 (100) | 26 (100) | 0.36 | 35 (100) | 37 (100) | 0.74 | 21 (100) | 51 (100) | 0.78 |
| ≤40 years | 25 (48.1) | 7 (35.0) | 17 (48.6) | 15 (40.5) | 10 (47.6) | 22 (43.1) | ||||
| 40 to 60 years | 19 (36.5) | 11 (55.0) | 14 (40.0) | 16 (43.2) | 9 (42.9) | 21 (41.2) | ||||
| ≥60 years | 8 (15.4) | 2 (10.0) | 4 (11.4) | 6 (16.2) | 2 (9.5) | 8 (15.7) | ||||
| Tumoral grade | 72 | 52 (100) | 20 (100) | 0.61 | 35 (100) | 37 (100) | 0.12 | 21 (100) | 51 (100) | 0.82 |
| I | 10 (19.2) | 2 (10.0) | 7 (20.0) | 5 (13.5) | 4 (19.0) | 8 (15.7) | ||||
| II | 24 (46.2) | 11 (55.0) | 20 (57.1) | 15 (40.5) | 9 (42.9) | 26 (51.0) | ||||
| III | 18 (34.6) | 7 (35.0) | 8 (22.9) | 17 (45.9) | 8 (38.1) | 17 (33.3) | ||||
| Clinical staging | 71 | 51 (100) | 20 (100) | 34 (100) | 37 (100) | 20 (100) | 51 (100) | |||
| T1 | 20 (39.2) | 7 (35.0) | 0.09 | 17 (50.0) | 10 (27.0) | 0.02 | 7 (35.0) | 20 (39.2) | 0.38 | |
| T2 | 24 (47.1) | 5 (25.0) | 14 (41.2) | 15 (40.5) | 11 (55.0) | 18 (35.3) | ||||
| T3 | 3 (5.9) | 4 (20.0) | 3 (8.8) | 4 (10.8) | 1 (5.0) | 6 (11.8) | ||||
| T4 | 4 (7.8) | 4 (20.0) | 0 (0.0) | 8 (21.6) | 1 (5.0) | 7 (13.7) | ||||
| N0 | 71 | 24 (47.1) | 12 (60.0) | 0.54 | 24 (61.8) | 15 (40.5) | 0.04 | 11 (55.0) | 25 (49.0) | 0.34 |
| N1 | 14 (27.5) | 6 (30.0) | 10 (29.4) | 10 (27.0) | 7 (35) | 13 (25.5) | ||||
| N2 | 7 (13.7) | 1 (5.0) | 3 (8.8) | 5 (13.5) | 2 (10.0) | 6 (11.8) | ||||
| N3 | 6 (11.8) | 1 (5.0) | 0 (0.0) | 7 (18.9) | 0 (0.0) | 7 (13.7) | ||||
| Relapse | 72 | 52 (100) | 20 (100) | 0.88 | 35 (100) | 37 (100) | 0.12 | 21 (100) | 51 (100) | 0.26 |
| No | 34 (65.4) | 12 (60.0) | 26 (74.3) | 20 (54.1) | 16 (76.2) | 30 (58.8) | ||||
| Yes | 18 (34.6) | 8 (40.0) | 9 (25.7) | 17 (45.9) | 5 (23.8) | 21 (41.2) | ||||
| Death | 72 | 52 (100) | 20 (100) | 0.04 | 35 (100) | 37 (100) | 0.02 | 21 (100) | 51 (100) | 0.01 |
| No | 46 (88.5) | 13 (65.0) | 33 (94.3) | 26 (70.3) | 21 (100) | 38 (74.5) | ||||
| Yes | 6 (11.5) | 7 (35.0) | 2 (5.7) | 11 (29.7) | 0 (0.0) | 13(25.5) | ||||
| Histology | 72 | 52 (100) | 20 (100) | 0.70 | 35 (100) | 37 (100) | 1.00 | 21 (100) | 51 (100) | 0.71 |
| Ductal | 46 (88.5) | 17 (85.0) | 31 (88.6) | 32 (86.5) | 18 (85.7) | 45 (88.2) | ||||
| Lobular | 6 (11.5) | 3 (15.0) | 4 (11.4) | 5 (13.5) | 3 (14.3) | 6 (11.8) | ||||
| Leukocyte | 72 | 7048 ± 2060 | 5508 ± 1829 | 0.00 | 6426 ± 2050 | 6804 ± 2166 | 0.45 | 5839 ± 2405 | 6942 ± 1900 | 0.04 |
| Neutrophil | 72 | 4210 ± 1541 | 3574 ± 1595 | 0.12 | 3941 ± 1314 | 4121 ± 1795 | 0.63 | 2973 ± 1408 | 4470 ± 1430 | 0.00 |
| Lymphocyte | 72 | 2095 ± 679 | 1252 ± 308 | 0.00 | 1779 ± 789 | 1937 ± 623 | 0.35 | 2137 ± 900 | 1746 ± 584 | 0.03 |
| Monocyte | 72 | 531 ± 175 | 496 ± 170 | 0.44 | 495 ± 185 | 545 ± 159 | 0.22 | 508 ± 210 | 526 ± 157 | 0.68 |
| Platelet (×103/mm3) | 72 | 266 ± 63 | 321 ± 81 | 0.00 | 222 ± 32 | 337 ± 52 | 0.00 | 242 ± 49 | 297 ± 74 | 0.03 |
| DFS | OS | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | |||||
| p | HR Ratio (95% CI) | p | HR Ratio (95% CI) | p | HR Ratio (95% CI) | p | HR Ratio (95% CI) | |
| Age | 0.79 | 0.996 (0.64–0.30) | ---- | ---- | 0.15 | 0.961 (0.91–4.02) | ---- | ---- |
| Grade 3 (vs. Grade 1–2) | 0.01 | 2.754 (1.27–5.98) | 0.53 | 1.346 (0.53–3.42) | 0.23 | 1.992 (0.64–6.18) | ---- | ---- |
| T2 (vs. T1) | 0.12 | 2.520 (0.79–8.04) | 0.53 | 1.497 (0.43–5.20) | 0.17 | 4.516 (0.53–38.74) | 0.18 | 4.761 (0.50–45.64) |
| T3 (vs. T1) | 0.01 | 8.118 (2.16–30.48) | 0.13 | 3.221 (0.72–14.40) | 0.02 | 14.337(1.48–148.32) | 0.37 | 2.984 (0.27–32.97) |
| T4 (vs. T1) | 0.00 | 8.622 (2.41–30.80) | 0.19 | 2.713 (0.61–12.18) | 0.03 | 11.686 (1.21–113.03) | 0.54 | 2.206 (0.18–27.16) |
| N1 (vs. N0) | 0.02 | 4.390 (1.32–14.59) | 0.05 | 3.474 (1.00–12.21) | 0.22 | 2.533 (0.57–11.33) | 0.13 | 4.139 (0.65–26.52) |
| N2 (vs. N0) | 0.00 | 18.497 (5.29–64.64) | 0.00 | 11.255 (2.84–44.63) | 0.14 | 3.810 (0.63–22.88) | 0.03 | 21.012 (1.42–311.08) |
| N3 (vs. N0) | 0.00 | 11.838 (3.30–42.42) | 0.01 | 6.396 (1.45–28.18) | 0.02 | 6.561 (1.31–32.81) | 0.01 | 23.234 (2.08–259.71) |
| Platelets (×103/mm3) > 279 (vs. <279) | 0.04 | 2.241 (1.03–4.89) | 0.65 | 1.307 (0.42–4.07) | 0.04 | 4.788 (1.05–21.93) | 0.58 | 1.638 (0.28–9.52) |
| PLR > 191.5 (vs. <191.5) | 0.58 | 1.263 (0.549–2.905) | ---- | ----- | 0.01 | 4.402 (1.39–13.94) | 0.00 | 16.156 (2.83–109.25) |
| KI67 Pos (vs. Neg) | 0.16 | 1.728 (0.80–3.73) | ---- | ---- | 0.38 | 1.663 (0.53–5.19) | ---- | ---- |
| Histology Lobular (vs. Ductal) | 0.53 | 1.410 (0.49–4.09) | ---- | ---- | 0.64 | 1.440 (0.31–6.58) | ---- | ---- |
| Platelet (×103 mm3) | 0.27 | 1.003 (0.99–1.01) | ---- | ---- | 0.22 | 1.004 (1.00–1.01) | ---- | ---- |
| Leukocyte | 0.11 | 1.000 (1.00–1.00) | ---- | ---- | 0.29 | 1.000 (1.00–1.00) | ---- | ---- |
| Neutrophil | 0.25 | 1.000 (1.00–1.00) | ---- | ---- | 0.43 | 1.000 (1.00–1.00) | ---- | ---- |
| Lymphocyte | 0.14 | 1.000 (1.00–1.00) | ---- | ---- | 0.17 | 0.999 (1.00–1.00) | ---- | ---- |
| Monocyte | 0.17 | 1.002 (1.00–1.00) | ---- | ---- | 0.93 | 1.000 (1.00–1.01) | ---- | ---- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rönnau, A.D.R.O.; Berto, M.D.; Bica, C.G.; Alves, R.V.; Rotta, L.N. Platelet Concentration and Platelet/Lymphocyte Ratio as Prognostic Indicators in Luminal Breast Cancer. J. Mol. Pathol. 2023, 4, 15-27. https://doi.org/10.3390/jmp4010002
Rönnau ADRO, Berto MD, Bica CG, Alves RV, Rotta LN. Platelet Concentration and Platelet/Lymphocyte Ratio as Prognostic Indicators in Luminal Breast Cancer. Journal of Molecular Pathology. 2023; 4(1):15-27. https://doi.org/10.3390/jmp4010002
Chicago/Turabian StyleRönnau, Angela Della’Santa Rubio O., Maiquidieli Dal Berto, Claudia Giuliano Bica, Rafael Vargas Alves, and Liane Nanci Rotta. 2023. "Platelet Concentration and Platelet/Lymphocyte Ratio as Prognostic Indicators in Luminal Breast Cancer" Journal of Molecular Pathology 4, no. 1: 15-27. https://doi.org/10.3390/jmp4010002