
Glycemia and New-Onset Diabetes among COVID-19 Patients with Prediabetes: A Follow-Study of Case Series in India


Abstract
:1. Introduction
2. Materials and Methods
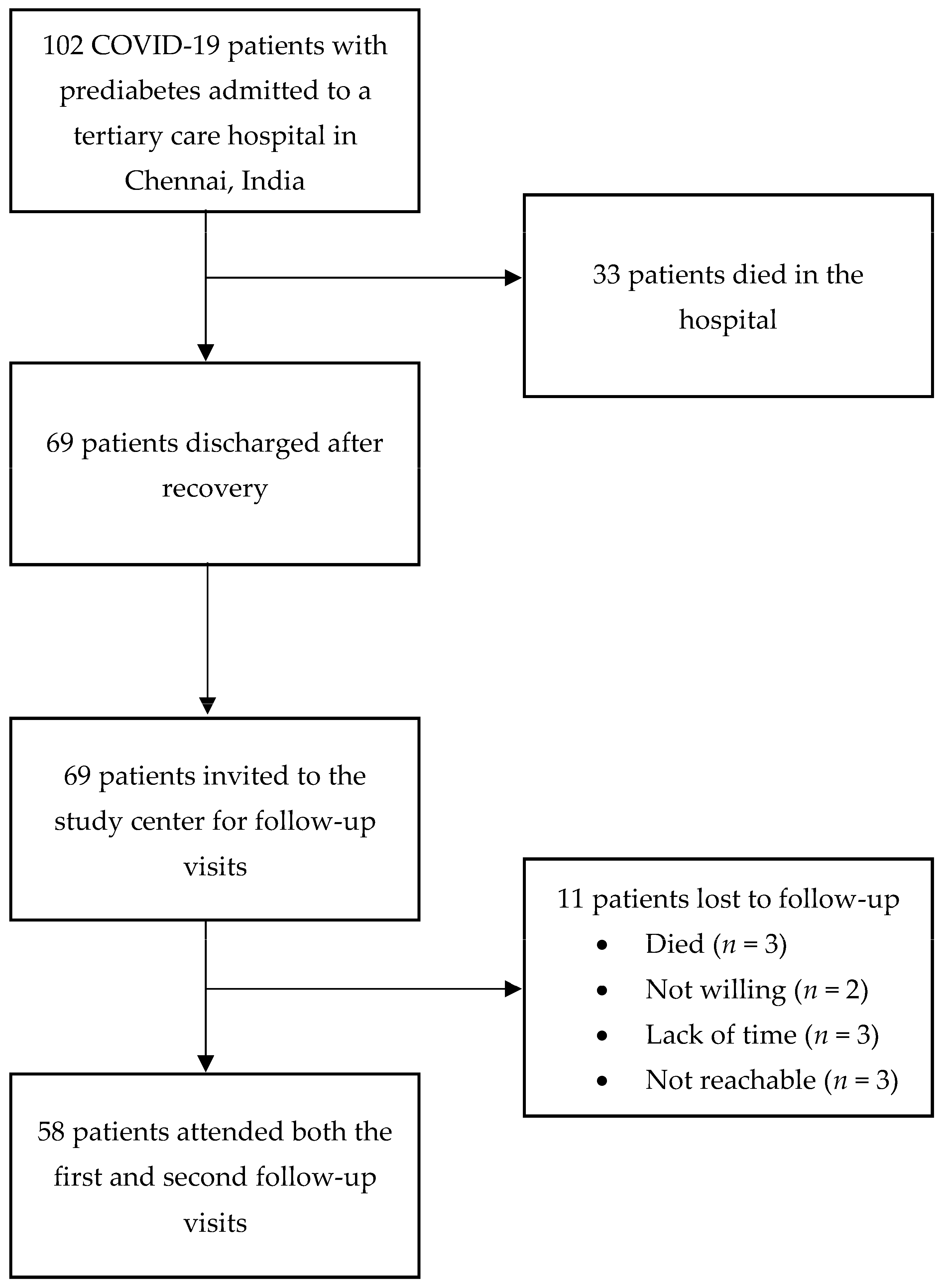
2.1. Study Design, Setting, and Selection of Participants
2.2. Data Collection on Hospital Admission
2.3. Follow-Up Visits
2.4. Plasma Glucose and HbA1c Analysis
2.5. Definition of New-Onset Diabetes
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Patients on Admission
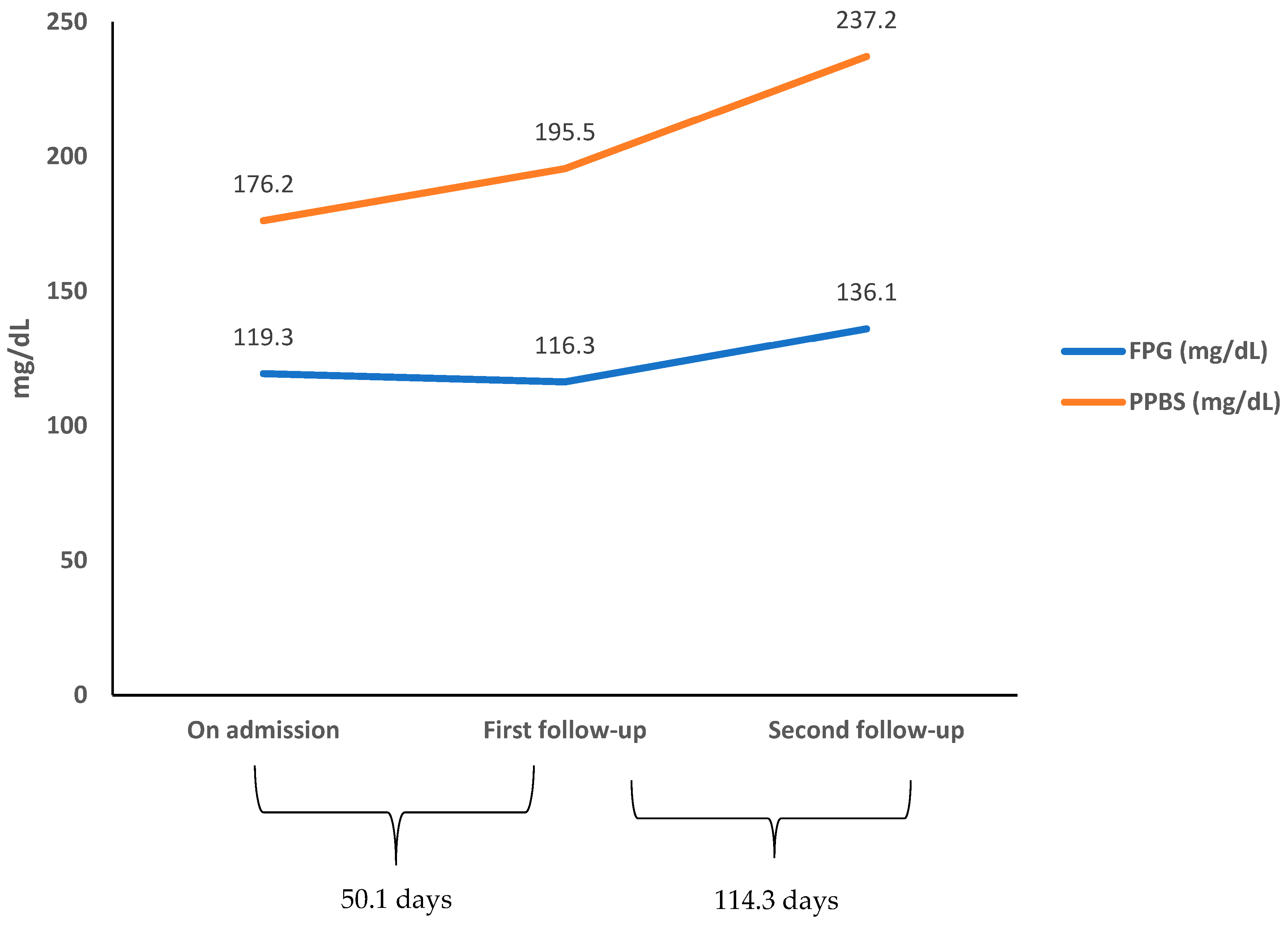
3.2. Longitudinal Changes in Glycemic Parameters
3.3. Glucose-Lowering Medications and New-Onset Diabetes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 17 November 2022).
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Del Prato, S. COVID-19 in people with diabetes: Understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Cao, Y.; Kapoor, N. Newly diagnosed diabetes in COVID-19 patients. Prim. Care Diabetes 2021, 15, 194. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Anton, M.C. Newly diagnosed diabetes in patients with mild to moderate COVID-19. Diabetes Metab. Syndr. 2021, 15, 569–571. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Kapoor, N.; Cao, Y.; Tapp, R.J.; Zimmet, P. Proportion of newly diagnosed diabetes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Obes. Metab. 2021, 23, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Anton, M.C.; Sivakumar, T. New-onset diabetes in “long COVID”. J. Diabetes 2021, 13, 693–694. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, M.; Pal, R.; Dutta, S. Risk of incident diabetes post-COVID-19: A systematic review and meta-analysis. Prim. Care Diabetes 2022, 16, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Ssentongo, P.; Zhang, Y.; Witmer, L.; Chinchilli, V.M.; Ba, D.M. Association of COVID-19 with diabetes: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 20191. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Mei, Q.; Zhang, Z.; Walline, J.H.; Liw, Y.; Zhu, H.; Zhang, S. Risk of newly diagnosed diabetes after COVID-19: A systematic review and meta-analysis. BMC Med. 2022, 20, 444. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Tapp, R.J.; Cooper, M.E.; Zimmet, P. Potential metabolic and inflammatory pathways between COVID-19 and new-onset diabetes. Diabetes Metab. 2021, 47, 101204. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Cao, Y.; Kapoor, N. Preexisting prediabetes and the severity of COVID-19. Prim. Care Diabetes 2021, 15, 28–29. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, N.D.; Velure Raja Rao, M.R.; Sathish, T. Clinical characteristics and outcomes of COVID-19 patients with prediabetes. Diabetes Metab. Syndr. 2021, 15, 102192. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S17–S38. [Google Scholar] [CrossRef] [PubMed]
- NABL INDIA. National Accreditation Board for Testing and Calibration Laboratories. Available online: https://nabl-india.org (accessed on 17 November 2022).
- Brown, H.; Prescott, R. Applied Mixed Models in Medicine, 3rd ed.; Wiley: Hoboken, NJ, USA, 2015. [Google Scholar]
- World Health Organization. COVID-19: Symptoms and Severity. Available online: https://www.who.int/westernpacific/emergencies/covid-19/information/asymptomatic-covid-19 (accessed on 17 November 2022).
- Grossmann, V.; Schmitt, V.H.; Zeller, T.; Panova-Noeva, M.; Schulz, A.; Laubert-Reh, D.; Juenger, C.; Schnabel, R.B.; Abt, T.G.J.; Laskowski, R.; et al. Profile of the Immune and Inflammatory Response in Individuals With Prediabetes and Type 2 Diabetes. Diabetes Care 2015, 38, 1356–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonas, E.; Alwi, I.; Pranata, R.; Huang, I.; Lim, M.A.; Yamin, M.; Nasution, S.A.; Setiati, S.; Virani, S.S. Elevated interleukin levels are associated with higher severity and mortality in COVID 19—A systematic review, meta-analysis, and meta-regression. Diabetes Metab. Syndr. 2020, 14, 2219–2230. [Google Scholar] [CrossRef] [PubMed]
- Lodge, S.; Nitschke, P.; Kimhofer, T.; Coudert, J.D.; Begum, S.; Bong, S.-H.; Richards, T.; Edgar, D.; Raby, E.; Spraul, M.; et al. NMR Spectroscopic Windows on the Systemic Effects of SARS-CoV-2 Infection on Plasma Lipoproteins and Metabolites in Relation to Circulating Cytokines. J. Proteome Res. 2021, 20, 1382–1396. [Google Scholar] [CrossRef] [PubMed]
- Luethi, N.; Cioccari, L.; Tanaka, A.; Kar, P.; Giersch, E.; Deane, A.M.; Mårtensson, J.; Bellomo, R. Glycated Hemoglobin A1c Levels Are Not Affected by Critical Illness. Crit. Care Med. 2016, 44, 1692–1694. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Cao, Y. What is the role of admission HbA1c in managing COVID-19 patients? J. Diabetes 2021, 13, 273–275. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Symptoms, n (%) | Demographics, Mean (SD) or n (%) | ||
|---|---|---|---|
| Feve | 53 (76.8) | Age (years) | 44.9 (13.6) |
| Fatigue | 56 (81.2) | Male | 49 (71.0) |
| Cough | 42 (60.9) | Behavioral factors, n (%) | |
| Sputum | 31 (44.9) | Smoking | 35 (50.7) |
| Sore throat | 52 (75.4) | Alcohol use | 33 (47.8) |
| Running nose | 27 (39.1) | Comorbidities, n (%) | |
| Odynophagia | 22 (31.9) | Hypertension | 34 (49.3) |
| Headache | 39 (56.5) | Chronic kidney disease | 5 (7.3) |
| Dizziness | 31 (44.9) | Coronary heart disease | 4 (5.8) |
| Chest pain | 10 (14.5) | Chronic liver disease | 4 (5.8) |
| Chest tightness | 23 (33.3) | Cerebrovascular accident | 5 (7.4) |
| Dyspnea | 41 (59.4) | One or more comorbidities | 45 (65.2) |
| Nausea | 13 (18.8) | Clinical parameters, mean (SD) or n (%) | |
| Vomiting | 12 (17.4) | Positive RT-PCR | 62 (89.9) |
| Diarrhea | 11 (15.9) | Chest CT imaging—area of lung injury ≤50% >50% | 62 (89.9) 7 (10.1) |
| Abdominal discomfort | 15 (21.7) | Body mass index (kg/m2) | 26.9 (4.3) |
| Loss of smell | 32 (46.4) | Systolic blood pressure (mmHg) | 124.6 (16.0) |
| Loss of taste | 32 (46.4) | Diastolic blood pressure (mmHg) | 78.5 (10.8) |
| Loss of appetite | 34 (49.3) | Blood cells, mean (SD) or median (IQR) | |
| Sleep disturbances | 22 (31.9) | Total leucocyte count (cells per mm3) | 6600 (5200–10,000) |
| Palpitation | 24 (34.8) | Neutrophil count (cells per mm3) | 4092 (2880–7138) |
| Vital signs, mean (SD) | Lymphocyte count (cells per mm3) | 1504 (948–2226) | |
| Pulse rate (beats/min) | 86.9 (12.6) | Neutrophil-to-lymphocyte ratio | 2.6 (1.7–7.2) |
| Respiratory rate (beats/min) | 22.0 (4.4) | Platelet count (cells per mm3) | 240,000 (190,000–284,000) |
| Sp02 (%) | 99.6 (3.0) | Urea (mg/dL) | 11 (8–14) |
| Inflammatory markets and coagulation indices, mean (SD) or median (IQR) | Creatinine (mg/dL) | 0.8 (0.7–1.0) | |
| D-dimer (ng/mL) | 222 (183–280) | eGFR (mL/min/1.73 m2) | 95.9 (32.2) |
| Ferritin (ng/mL) | 192 (104–305) | Total bilirubin (mg/dL) | 1.0 (0.9–1.2) |
| C-reactive protein (mg/L) | 40 (16.4–104) | Total protein (g/dL) | 6.7 (0.5) |
| Interleukin-6 (pg/mL) | 12 (6–22) | Albumin (g/dL) | 3.7 (0.5) |
| Prothrombin time (in seconds) | 14 (12–16) | Globulin (g/dL) | 3.0 (0.5) |
| aPTT (in seconds) | 28.5 (6.3) | Alanine aminotransferase (U/L) | 32 (22–45) |
| International normalized ratio | 1.13 (0.13) | Aspartate aminotransferase (U/L) | 40 (28–61) |
| Glucose parameters, mean (SD) | Lipids, mean (SD) | ||
| Fasting plasma glucose (mg/dL) | 119.3 (21.1) | Total cholesterol (mg/dL) | 236.0 (61.8) |
| 2 hr post-prandial glucose (mg/dL) | 176.2 (34.9) | Triglycerides (mg/dL) | 154.7 (43.5) |
| HbA1c (%) | 5.9 (0.2) | HDL cholesterol (mg/dL) | 39.0 (5.8) |
| In-Hospital Treatment, n (%) | |
| Favipiravir | 69 (100) |
| Remdesivir | 42 (60.9) |
| Dexamethasone | 69 (100) |
| Ceftriaxone | 16 (23.2) |
| Low molecular weight heparin | 69 (100) |
| Supplemental oxygen (non-invasive) | 33 (47.8) |
| Mechanical ventilation | 16 (23.2) |
| Complications, n (%) | |
| Acute respiratory distress syndrome | 28 (40.6) |
| Septic shock | 15 (21.7) |
| Thrombosis | 5 (7.3) |
| Acute kidney injury | 8 (11.6) |
| Intensive care unit admission | 16 (23.2) |
| Clinical outcomes, mean (SD) | |
| No. of hospital days | 9.0 (4.1) |
| N | First Follow-Up (Mean (SD)) | Mean Change from Baseline (95% CI) | p | N | Second Follow-Up (Mean (SD)) | Mean Change from Baseline (95% CI) | p | |
|---|---|---|---|---|---|---|---|---|
| FPG (mg/dL) | 58 | 116.3 (37.1) | −3.0 (−14.7 to 8.7) | 0.62 | 58 | 136.1 (46.4) | 16.8 (5.1 to 28.5) | 0.005 |
| PPBS (mg/dL) | 58 | 195.5 (61.6) | 19.3 (3.1 to 35.5) | 0.019 | 58 | 237.2 (61.0) | 61.0 (44.8 to 77.2) | <0.001 |
| HbA1c (%) | 58 | 6.4 (0.8) | 0.5 (0.4 to 0.7) | <0.001 | 58 | 6.5 (0.7) | 0.6 (0.4 to 0.7) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandrasekaran, N.D.; Sathish, T. Glycemia and New-Onset Diabetes among COVID-19 Patients with Prediabetes: A Follow-Study of Case Series in India. Diabetology 2023, 4, 19-27. https://doi.org/10.3390/diabetology4010003
Chandrasekaran ND, Sathish T. Glycemia and New-Onset Diabetes among COVID-19 Patients with Prediabetes: A Follow-Study of Case Series in India. Diabetology. 2023; 4(1):19-27. https://doi.org/10.3390/diabetology4010003
Chicago/Turabian StyleChandrasekaran, Nirmala Devi, and Thirunavukkarasu Sathish. 2023. "Glycemia and New-Onset Diabetes among COVID-19 Patients with Prediabetes: A Follow-Study of Case Series in India" Diabetology 4, no. 1: 19-27. https://doi.org/10.3390/diabetology4010003