
The Scrotal Excision of Paratesticular Mesothelioma of the Tunica Vaginalis: A Case Report
 ,
,
Abstract
:1. Introduction
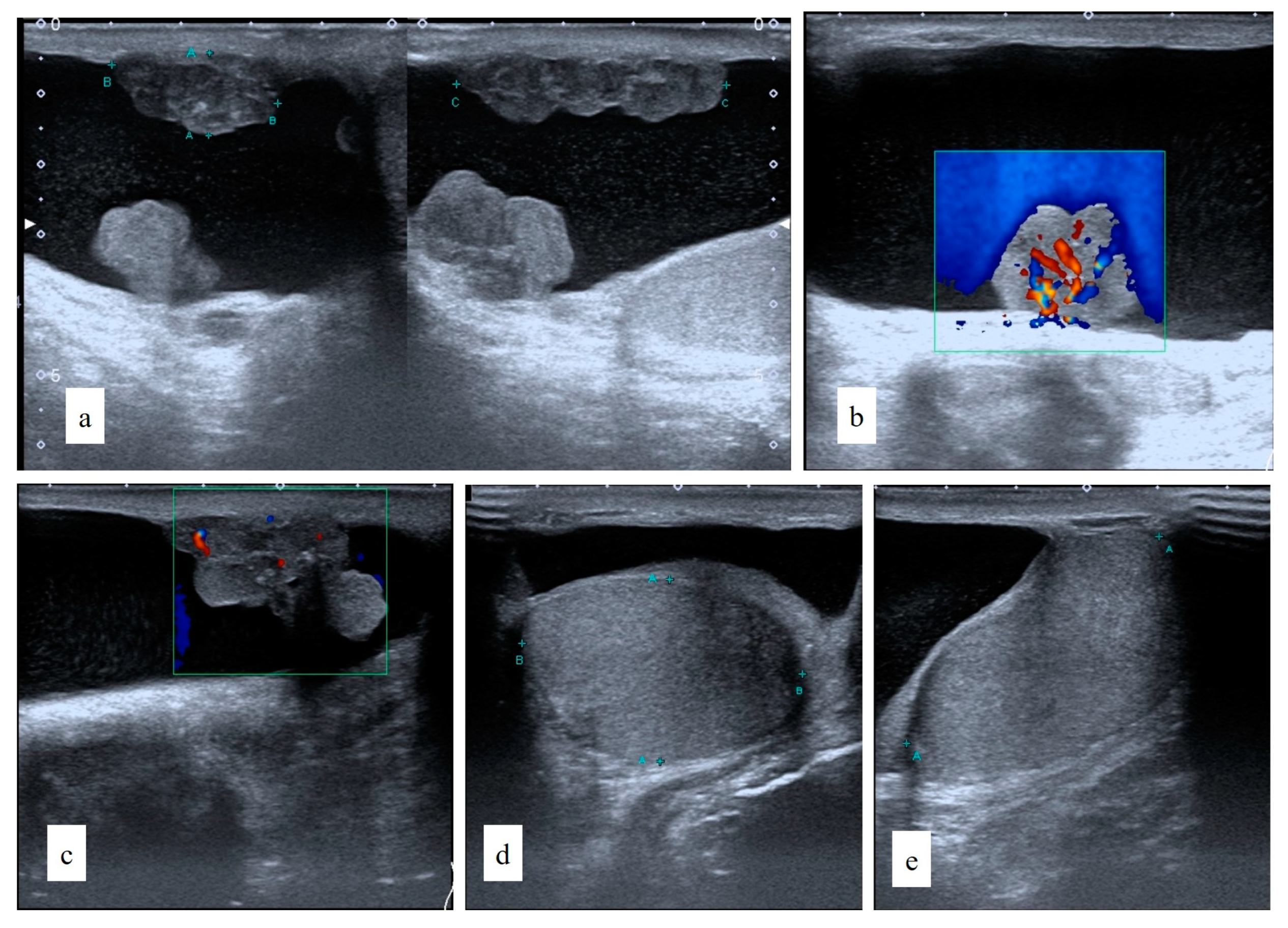
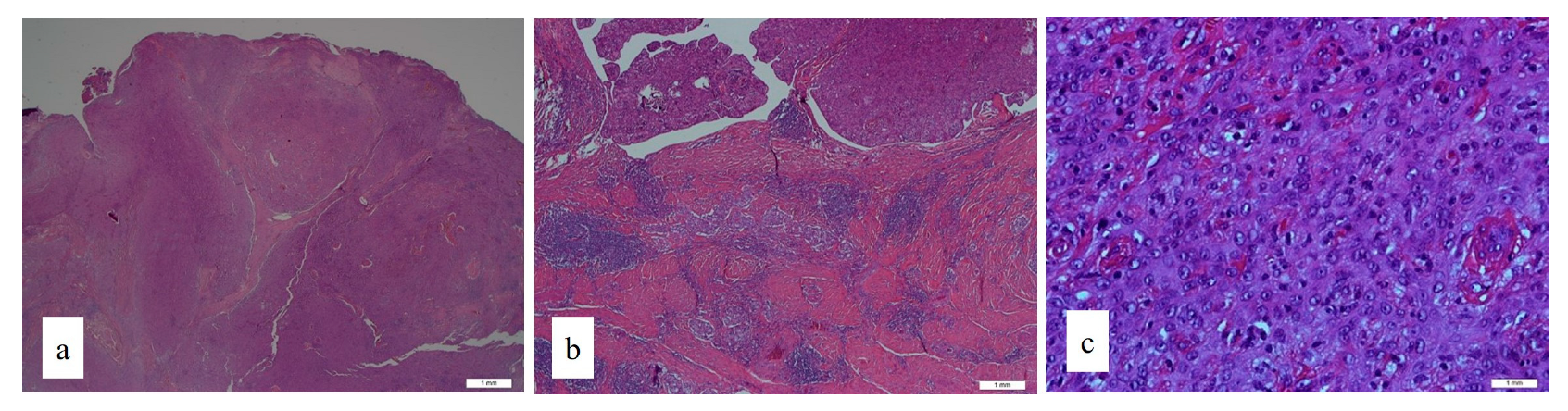
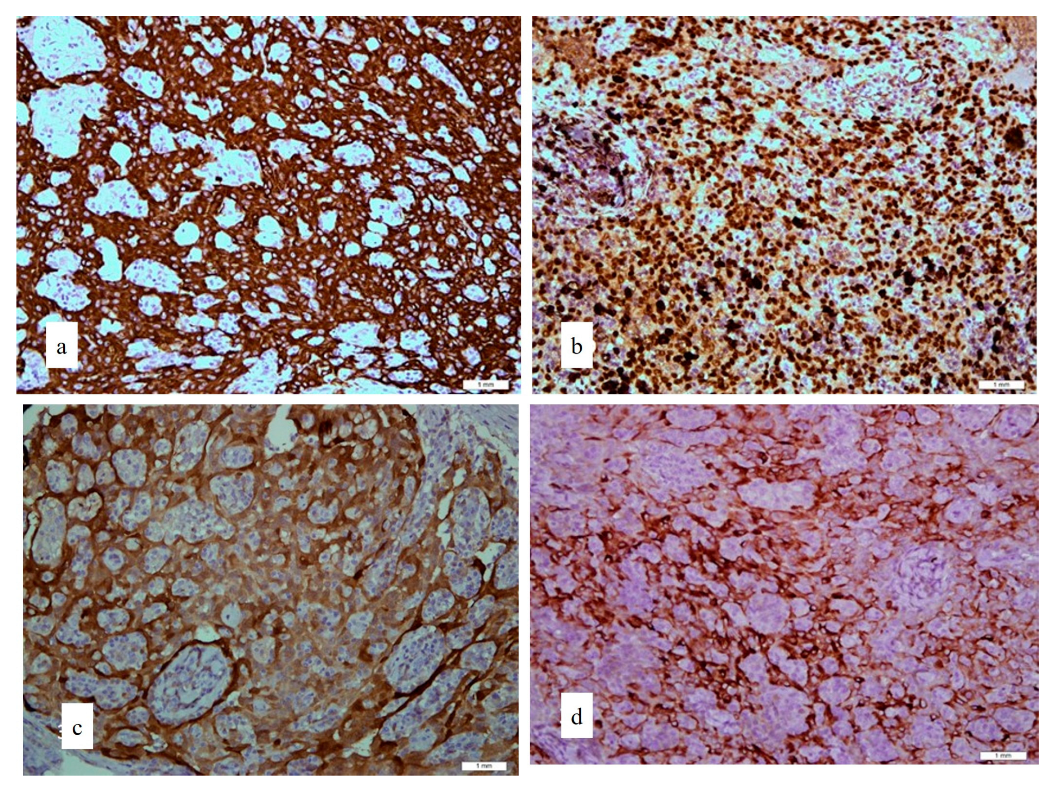
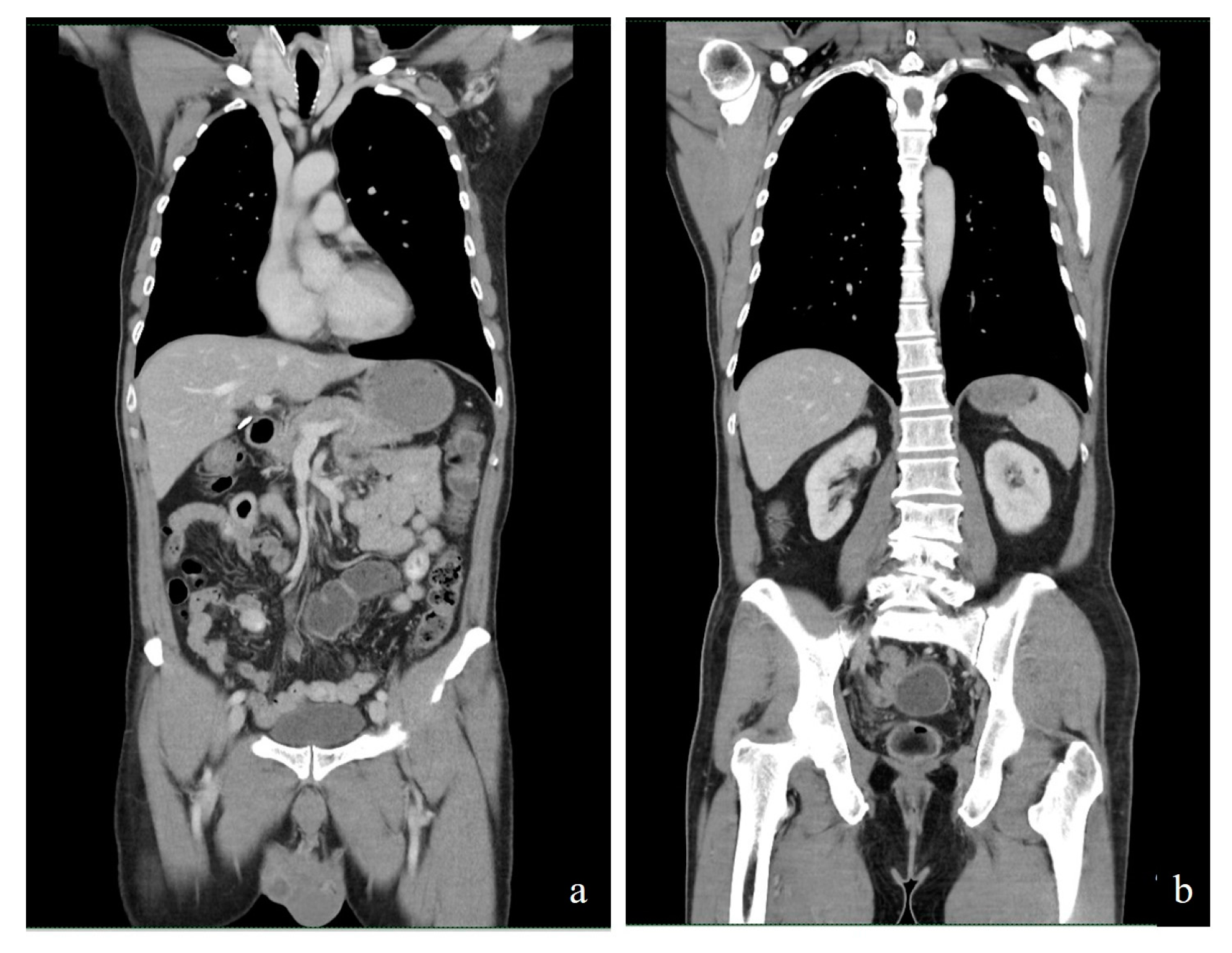
2. Case Report
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Reports | Clinical Features | |||
|---|---|---|---|---|
| Age of Male | Physical Examination | Ultrasound Examination | Blood Investigations | |
| Gurdal & Erol [8] | 67 | Positive transillumination, right scrotal swelling, and normal left testis and scrotum were detected. | Examination confirmed hydrocele without any suspicion of malignancy. | αFP and β-HCG levels were within normal limits. |
| Goel et al. [13] | 65 | A hard palpable mass was detected in the left iliac fossa and a testicular enlargement was noted on the left side. | Left testis was enlarged 3.9 cm × 3 cm × 3.2 cm, showing diffusely heterogenous echo-texture and irregular nodular surface with irregular hypoechoic thickening of the scrotal wall with left-sided hydrocele. | |
| Park et al. [3] | 65 | A palpable mass was detected in the left inguinal area. The mass was hard, globular, smooth, and nontender, and the lower margins were not palpable below the inguinal ligament. A hard spermatic cord was palpated. The scrotum was normal except for a slightly enlarged nontender left testis. | Ultrasound examination of the abdomen and scrotum showed a 3.0 cm × 3.3 cm × 1.8 cm nodal mass in the left inguinal area. The right testis was 3.0 cm × 2.2 cm × 4.9 cm in size, whereas the left testis was enlarged to 3.3 cm × 2.7 cm × 4.9 cm, contained a little hydrocele, and had normal echogenicity and vascularity. | |
| Akin et al. [4] | 49 | A hard and painless mass was evident in the left scrotum and was suggestive of a hydrocele on palpation. No left inguinal hernia was evident. The right testis was normal, as was the scrotal skin. No palpable lymph node was detected in the pelvic or inguinal areas. | Ultrasonography revealed an increase in the size of the left scrotum, with many multiloculated cysts of different sizes. The parenchyma and size of the left testis were normal. | The levels of αFP, β-HCG, and LDH were not elevated. |
| Kazaz et al. [12] | 75 | A fluid-filled palpable mass (approximately 10 cm in size) filled the left hemiscrotum and extended to the inguinal canal. | Nil | Nil |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mezei, G.; Chang, E.T.; Mowat, F.S.; Moolgavkar, S.H. Epidemiology of mesothelioma of the pericardium and tunica vaginalis testis. Ann. Epidemiol. 2017, 27, 348–359.e11. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ordonez, B.; Srigley, J. Mesothelial lesions of the paratesticular region. Semin. Diagn. Pathol. 2000, 17, 294–306. Available online: https://pubmed.ncbi.nlm.nih.gov/11202546/ (accessed on 19 September 2022). [PubMed]
- Park, Y.J.; Kong, H.J.; Jang, H.C.; Shin, H.S.; Oh, H.K.; Park, J.S. Malignant mesothelioma of the spermatic cord. Korean J. Urol. 2011, 52, 225–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akin, Y.; Bassorgun, I.; Basara, I.; Yucel, S. Malignant mesothelioma of tunica vaginalis: An extremely rare case presenting without risk factors. Singap. Med. Assoc. 2015, 56, e53. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4371211/ (accessed on 19 September 2022). [CrossRef] [PubMed] [Green Version]
- National Cancer Institute. Tumor Markers. Available online: https://training.seer.cancer.gov/testicular/abstract-code-stage/extent/markers.html (accessed on 14 November 2022).
- Van Wilpe, S.; Koornstra, R.; Den Brok, M.; De Groot, J.W.; Blank, C.; De Vries, J.; Gerritsen, W.; Mehra, N. Lactate dehydrogenase: A marker of diminished antitumor immunity. Oncoimmunology 2020, 9, 1731942. [Google Scholar] [CrossRef] [Green Version]
- Koschel, S.G.; Wong, L.M. Radical inguinal orchidectomy: The gold standard for initial management of testicular cancer. Transl. Androl. Urol. 2020, 9, 3094–3102. [Google Scholar] [CrossRef] [PubMed]
- Gürdal, M.; Erol, A. Malignant mesothelioma of tunica vaginalis testis associated with long-lasting hydrocele: Could hydrocele be an etiological factor? Int. Urol. Nephrol. 2001, 32, 687–689. [Google Scholar] [CrossRef]
- Molinari, L.; Stevenson, J. Mesothelioma Stages. Available online: https://www.mesothelioma.com/mesothelioma/stages/ (accessed on 14 November 2022).
- Blaivas, M.; Brannam, L. Testicular ultrasound. Emerg. Med. Clin. N. Am. 2004, 22, 723–748. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.J.; Parker, R.J.; Wiggins, J. Malignant mesothelioma. Orphanet J. Rare Dis. 2008, 3, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazaz, I.; Teoman, A.; Mungan, S. Mesothelioma of the tunica vaginalis testis: A case report. Indian J. Pathol. Microbiol. 2020, 63, 475–477. [Google Scholar] [CrossRef] [PubMed]
- Goel, A.; Agrawal, A.; Gupta, R.; Hari, S.; Dey, A.B. Malignant mesothelioma of the tunica vaginalis of the testis without exposure to asbestos. Cases J. 2008, 1, 310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butnor, K.J.; Pavlisko, E.N.; Sporn, T.A.; Roggli, V.L. Mesothelioma of the tunica vaginalis testis. Hum. Pathol. 2019, 92, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Ceresoli, G.L.; Zucali, P.A.; Favaretto, A.G.; Grossi, F.; Bidoli, P.; Del Conte, G.; Ceribelli, A.; Bearz, A.; Morenghi, E.; Cavina, R.; et al. Phase II study of pemetrexed plus carboplatin in malignant pleural mesothelioma. J. Clin. Oncol. 2006, 24, 1443–1448. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohd Hashim, M.H.; Fam, X.I.; Khoo, H.C.; Wan Ahmad Kammal, W.S.E.; Kamal, H. The Scrotal Excision of Paratesticular Mesothelioma of the Tunica Vaginalis: A Case Report. Uro 2022, 2, 277-283. https://doi.org/10.3390/uro2040031
Mohd Hashim MH, Fam XI, Khoo HC, Wan Ahmad Kammal WSE, Kamal H. The Scrotal Excision of Paratesticular Mesothelioma of the Tunica Vaginalis: A Case Report. Uro. 2022; 2(4):277-283. https://doi.org/10.3390/uro2040031
Chicago/Turabian StyleMohd Hashim, Mohammad Hifzi, Xeng Inn Fam, Hau Chun Khoo, Wan Syahira Ellani Wan Ahmad Kammal, and Haziq Kamal. 2022. "The Scrotal Excision of Paratesticular Mesothelioma of the Tunica Vaginalis: A Case Report" Uro 2, no. 4: 277-283. https://doi.org/10.3390/uro2040031