
Single Center Experience of Oral Vancomycin Therapy in Young Patients with Primary Sclerosing Cholangitis: A Case Series

 , ,
, , 
Abstract
:1. Introduction
1.1. Background
1.2. Objectives
2. Materials and Methods
2.1. Sample and Setting
2.2. Baseline Data
2.3. Data Collection and Analysis
3. Results
3.1. Demographics
3.2. Baseline Characteristics
3.2.1. Baseline Clinical Features
3.2.2. Baseline Biochemical Laboratory Values
3.2.3. Baseline Imaging and Histopathology Findings
3.3. Oral Vancomycin Regimen
3.4. Post-OV Therapy Characteristics
3.4.1. Post-OV Clinical Features
3.4.2. Post-OV Biochemical Laboratory Trends
3.4.3. Post-OV Imaging Findings
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deneau, M.R.; El-Matary, W.; Valentino, P.L.; Abdou, R.; Alqoaer, K.; Amin, M.; Amir, A.Z.; Auth, M.; Bazerbachi, F.; Broderick, A.; et al. The natural history of primary sclerosing cholangitis in 781 children: A multicenter, international collaboration. Hepatology 2017, 66, 518–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deneau, M.; Perito, E.; Ricciuto, A.; Gupta, N.; Kamath, B.M.; Palle, S.; Vitola, B.; Smolka, V.; Ferrari, F.; Amir, A.Z.; et al. Ursodeoxycholic Acid Therapy in Pediatric Primary Sclerosing Cholangitis: Predictors of Gamma Glutamyltransferase Normalization and Favorable Clinical Course. J. Pediatr. 2019, 209, 92–96.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mertz, A.; Nguyen, N.A.; Katsanos, K.H.; Kwok, R.M. Primary sclerosing cholangitis and inflammatory bowel disease comorbidity: An update of the evidence. Ann. Gastroenterol. 2019, 32, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Davies, Y.K.; Tsay, C.J.; Caccamo, D.V.; Cox, K.M.; Castillo, R.O.; Cox, K.L. Successful treatment of recurrent primary sclerosing cholangitis after orthotopic liver transplantation with oral vancomycin. Case Rep. Transplant. 2013, 2013, 314292. [Google Scholar] [CrossRef] [Green Version]
- Tabibian, J.H.; Ali, A.H.; Lindor, K.D. Primary Sclerosing Cholangitis, Part 1: Epidemiology, Etiopathogenesis, Clinical Features, and Treatment. Gastroenterol. Hepatol. 2018, 14, 293. [Google Scholar]
- Ricciuto, A.; Kamath, B.M.; Griffiths, A.M. The IBD and PSC Phenotypes of PSC-IBD. Curr. Gastroenterol. Rep. 2018, 20, 16. [Google Scholar] [CrossRef]
- Cotter, J.M.; Mack, C.L. Primary sclerosing cholangitis: Unique aspects of disease in children. Clin. Liver Dis. (Hoboken) 2017, 10, 120–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilscher, M.; Enders, F.B.; Carey, E.J.; Lindor, K.D.; Tabibian, J.H. Alkaline phosphatase normalization is a biomarker of improved survival in primary sclerosing cholangitis. Ann. Hepatol. 2016, 15, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, A.E.; Perrault, J.; El-Youssif, M.; Lindor, K.D.; Freese, D.K.; Angulo, P. Primary sclerosing cholangitis in children: A long-term follow-up study. Hepatology 2003, 38, 210–217. [Google Scholar] [CrossRef]
- Berhane, B.; van Rheenen, P.F.; Verkade, H.J. Gamma-glutamyl transferase and disease course in pediatric-onset primary sclerosing cholangitis: A single-center cohort study. Health Sci. Rep. 2023, 6, e1086. [Google Scholar] [CrossRef]
- Santiago, P.; Scheinberg, A.R.; Levy, C. Cholestatic liver diseases: New targets, new therapies. Therap. Adv. Gastroenterol. 2018, 11, 1756284818787400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vesterhus, M.; Karlsen, T.H. Emerging therapies in primary sclerosing cholangitis: Pathophysiological basis and clinical opportunities. J. Gastroenterol. 2020, 55, 588–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.J.; Gou, H.Z.; Zhang, Y.L.; Song, X.J.; Zhang, L. Role of intestinal flora in primary sclerosing cholangitis and its potential therapeutic value. World J. Gastroenterol. 2022, 28, 6213–6229. [Google Scholar] [CrossRef] [PubMed]
- Black, D.D.; Mack, C.; Kerkar, N.; Miloh, T.; Sundaram, S.S.; Anand, R.; Gupta, A.; Alonso, E.; Arnon, R.; Bulut, P.; et al. A Prospective Trial of Withdrawal and Reinstitution of Ursodeoxycholic Acid in Pediatric Primary Sclerosing Cholangitis. Hepatol. Commun. 2019, 3, 1482–1495. [Google Scholar] [CrossRef] [Green Version]
- Nerandzic, M.M.; Mullane, K.; Miller, M.A.; Babakhani, F.; Donskey, C.J. Reduced acquisition and overgrowth of vancomycin-resistant enterococci and Candida species in patients treated with fidaxomicin versus vancomycin for Clostridium difficile infection. Clin. Infect. Dis. 2012, 55 (Suppl. S2), S121–S126. [Google Scholar] [CrossRef] [PubMed]
- Damman, J.L.; Rodriguez, E.A.; Ali, A.H.; Buness, C.W.; Cox, K.L.; Carey, E.J.; Lindor, K.D. Review article: The evidence that vancomycin is a therapeutic option for primary sclerosing cholangitis. Aliment. Pharmacol. Ther. 2018, 47, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Abarbanel, D.N.; Seki, S.M.; Davies, Y.; Marlen, N.; Benavides, J.A.; Cox, K.; Nadeau, K.C.; Cox, K.L. Immunomodulatory effect of vancomycin on Treg in pediatric inflammatory bowel disease and primary sclerosing cholangitis. J. Clin. Immunol. 2013, 33, 397–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, Y.K.; Cox, K.M.; Abdullah, B.A.; Safta, A.; Terry, A.B.; Cox, K.L. Long-term treatment of primary sclerosing cholangitis in children with oral vancomycin: An immunomodulating antibiotic. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Laborda, T.J.; Jensen, M.K.; Kavan, M.; Deneau, M. Treatment of primary sclerosing cholangitis in children. World J. Hepatol. 2019, 11, 19–36. [Google Scholar] [CrossRef]
- Ali, A.H.; Damman, J.; Shah, S.B.; Davies, Y.; Hurwitz, M.; Stephen, M.; Lemos, L.M.; Carey, E.J.; Lindor, K.D.; Buness, C.W.; et al. Open-label prospective therapeutic clinical trials: Oral vancomycin in children and adults with primary sclerosing cholangitis. Scand. J. Gastroenterol. 2020, 55, 941–950. [Google Scholar] [CrossRef]
- Deneau, M.R.; Mack, C.; Abdou, R.; Amin, M.; Amir, A.; Auth, M.; Bazerbachi, F.; Marie Broderick, A.; Chan, A.; DiGuglielmo, M.; et al. Gamma Glutamyltransferase Reduction Is Associated with Favorable Outcomes in Pediatric Primary Sclerosing Cholangitis. Hepatol. Commun. 2018, 2, 1369–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, K.L.; Cox, K.M. Oral vancomycin: Treatment of primary sclerosing cholangitis in children with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 1998, 27, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Rahimpour, S.; Nasiri-Toosi, M.; Khalili, H.; Ebrahimi-Daryani, N.; Nouri-Taromlou, M.K.; Azizi, Z. A Triple Blinded, Randomized, Placebo-Controlled Clinical Trial to Evaluate the Efficacy and Safety of Oral Vancomycin in Primary Sclerosing Cholangitis: A Pilot Study. J. Gastrointest. Liver Dis. 2016, 25, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Deneau, M.R.; Mack, C.; Mogul, D.; Perito, E.R.; Valentino, P.L.; Amir, A.Z.; DiGuglielmo, M.; Draijer, L.G.; El-Matary, W.; Furuya, K.N.; et al. Oral Vancomycin, Ursodeoxycholic Acid, or No Therapy for Pediatric Primary Sclerosing Cholangitis: A Matched Analysis. Hepatology 2021, 73, 1061–1073. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age at Diagnosis (Year) | Gender | Associated Diagnosis- CD/UC | Time from Diagnosis to OV | Albumin (g/dL) | Total Bilirubin (mg/dL) | GGT (U/L) | ALT (U/L) | AST (U/L) | ALP (U/L) | ESR (mm/Hour) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient 1 | 5 | Male | UC | 4 years 8 months | 3.6 | 1.2 | 122 | 85 | 72 | 467 | 17 |
| Patient 2 | 9 | Male | - | 5 months | 4.3 | 0.6 | 171 | 160 | 56 | 422 | - |
| Patient 3 | 11 | Male | CD | 2 years 4 months | 3.3 | 1.0 | 251 | 67 | 94 | 980 | 109 |
| Patient 4 | 13 | Male | - | 1 year 9 months | 4.1 | 1.6 | 38 | 33 | 35 | 444 | 24 |
| Patient 5 | 13 | Male | CD | 3 years 9 months | 4.2 | 0.5 | 512 | 146 | 96 | 500 | 19 |
| Patient 6 | 16 | Female | UC | 1 month | 4.3 | 0.2 | 155 | 38 | 44 | 200 | 37 |
| Patient 7 | 16 | Male | CD | 10 days | 4.7 | 0.8 | 720 | 275 | 140 | 274 | 9 |
| Patient 8 | 16 | Male | CD | 13 days | 2.8 | 1.7 | 198 | 106 | 100 | 661 | 87 |
| Patient 9 | 17 | Male | UC | 6 days | 4.4 | 0.3 | 120 | 30 | 17 | 128 | 35 |
| Patient 10 | 18 | Male | UC | 7 days | 4.1 | 0.6 | 381 | 252 | 124 | 383 | 10 |
| Patient 11 | 13 | Male | UC | 5 years | 3.8 | 0.5 | 275 | 84 | 65 | 677 | 19 |
| Patient 12 | 18 | Male | UC | 8 months | 4.2 | 0.2 | 21 | 12 | 22 | 160 | 14 |
| Patient 13 | 18 | Male | UC | 1 year 10 months | 4.4 | 0.6 | 215 | 31 | 33 | 143 | 31 |
| Patient 14 | 20 | Male | UC | 4 years 7 months | 3.9 | 1.8 | 443 | 72 | 108 | 294 | 24 |
| Patient 15 | 22 | Female | UC | 9 years | 4.0 | 0.4 | 221 | 53 | 45 | 248 | 25 |
| Patient 16 | 22 | Female | UC | 7 months | 2.4 | 1.5 | 627 | 31 | 93 | 845 | 100 |
| Patient 17 | 16 | Male | UC | 2 years 10 months | 4.4 | 0.5 | 139 | 97 | 99 | 124 | 1 |
| Patients | GGT (U/L) | GGT 6 Months | GGT 1 Year | ALT (U/L) | ALT 6 Months | ALT 1 Year |
|---|---|---|---|---|---|---|
| Patient 1 | 122 | 60 | 17 | 85 | 65 | 55 |
| Patient 2 | 171 | 21 | - | 160 | 30 | 33 |
| Patient 3 | 251 | 254 | 312 | 67 | 56 | 62 |
| Patient 4 | 38 | 41 | 32 | 33 | 35 | 34 |
| Patient 5 | 512 | 73 | 57 | 146 | 34 | 30 |
| Patient 6 | 155 | 25 | 34 | 38 | 11 | 16 |
| Patient 7 | 720 | 33 | - | 275 | 32 | - |
| Patient 8 | 198 | - | - | 106 | 89 | 85 |
| Patient 9 | 120 | 85 | 305 | 30 | 40 | 125 |
| Patient 10 | 381 | 283 | 118 | 252 | 176 | 82 |
| Patient 11 | 275 | 328 | 204 | 84 | 327 | 167 |
| Patient 12 | 21 | 10 | 40 | 12 | 29 | 30 |
| Patient 13 | 215 | 37 | - | 31 | 12 | 8 |
| Patient 14 | 443 | 122 | - | 72 | 55 | 66 |
| Patient 15 | 221 | - | - | 53 | 32 | 70 |
| Patient 16 | 627 | - | - | 31 | 70 | - |
| Patient 17 | 139 | - | - | 97 | 18 | - |
| Median | 215 | 60 | 57 | 72 | 35 | 58.5 |
| N= | 17 | 13 | 9 | 17 | 17 | 14 |
| Range | 21–720 | 10–328 | 17–312 | 12–275 | 11–327 | 8–167 |
| Baseline | 6 Months | 1 Year | ||||
|---|---|---|---|---|---|---|
| Factor | N | Median (min, max) | N | Median (min, max) | N | Median (min, max) |
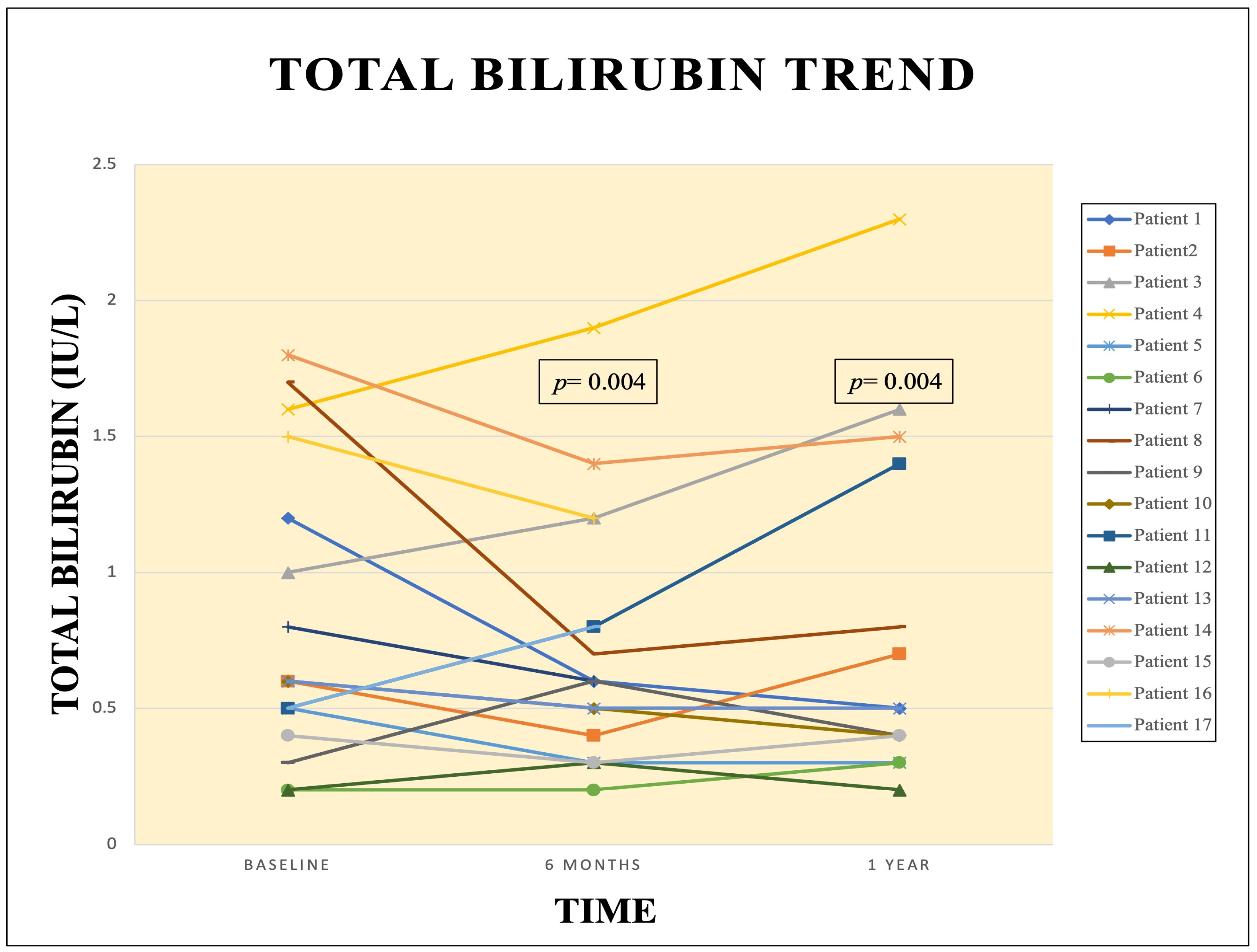
| Total Bilirubin | 17 | 0.60 (0.20, 1.8) | 17 | 0.60 (0.20, 1.9) | 14 | 0.50 (0.20, 2.3) |
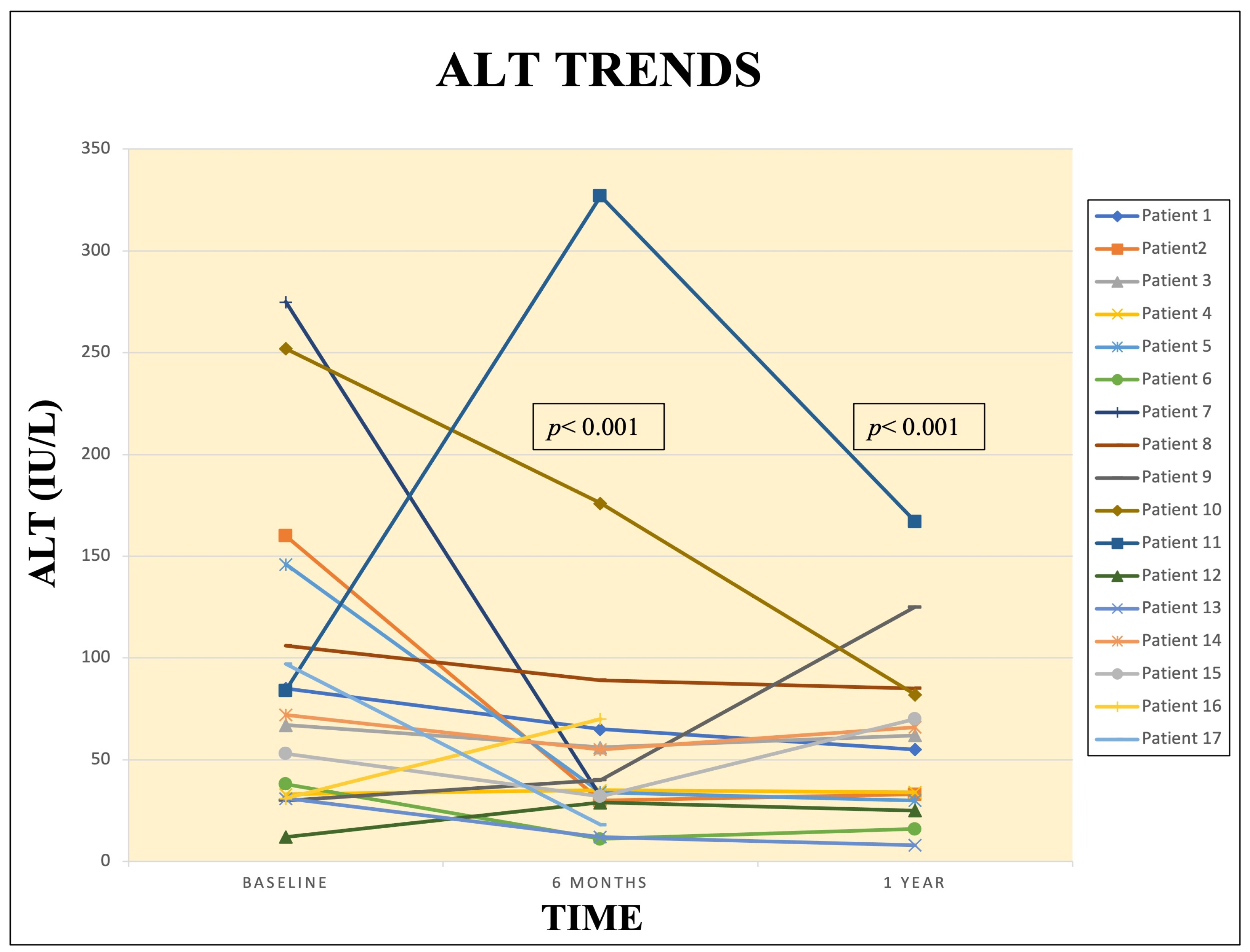
| ALT | 17 | 72 (12, 275) | 17 | 35 (11, 327) | 14 | 59 (8.0, 167) |
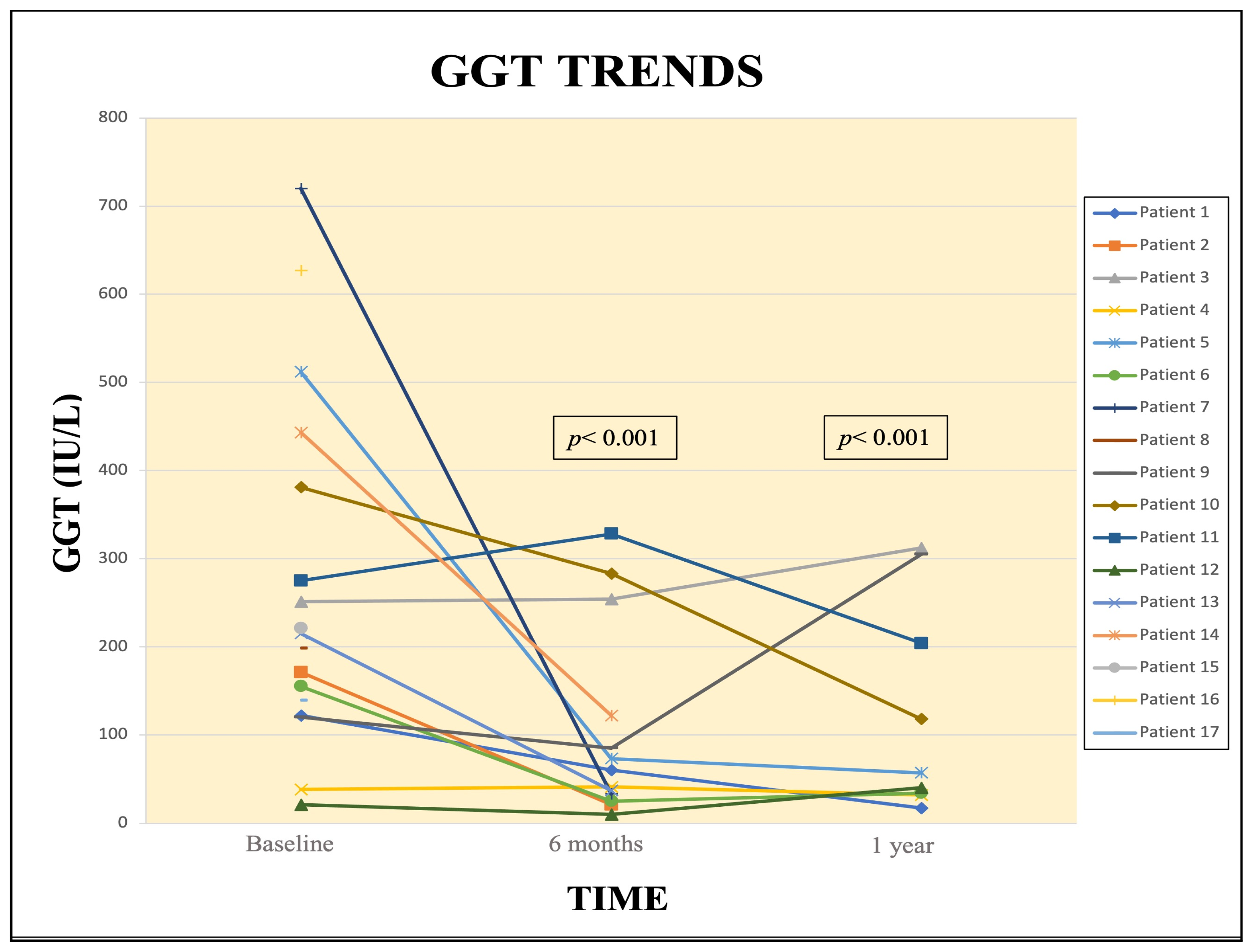
| GGT | 17 | 215 (21, 720) | 13 | 60 (10, 328) | 9 | 57 (17, 312) |
| ESR/WSR | 16 | 24 (1.0, 109) | 9 | 15 (2.0, 66) | 9 | 15 (2.0, 140) |
| ALP | 17 | 383 (124, 980) | 17 | 180 (64, 1079) | 14 | 206.5 (69, 918) |
| Changes From Baseline to 6 Months and 1 Year Post OV | |||
|---|---|---|---|
| Label | N | Median (Min, Max) | p Value * |
| Change in ALT, baseline to 6 months post-OV | 17 | −70.6 (−274.4, −11.7) | <0.001 |
| Change in GGT, baseline to 6 months post OV | 17 | −144.0 (−688.0, 52.0) | <0.001 |
| Change in ESR/WSR, baseline to 6 months post OV | 12 | 46.5 (−12.0, 309.0) | 0.003 |
| Change in Total Bilirubin, baseline to 6 months post OV | 9 | 14.4 (1.2, 64.3) | 0.004 |
| Change in ALT, baseline to 1 year post OV | 14 | −68.0 (−251.6, −11.8) | <0.001 |
| Change in GGT, baseline to 1 year post OV | 14 | −138.5 (−482.0, 5.0) | <0.001 |
| Change in ESR/WSR, baseline to 1 year post OV | 9 | 38.0 (−3.0, 270.0) | 0.016 |
| Change in Total Bilirubin, baseline to 1 year post OV | 9 | 14.8 (1.4, 139.0) | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alenchery, A.J.; Patel, S.; Mahajan, L.; Kurowski, J.A.; Worley, S.; Hupertz, V.; Radhakrishnan, K.; Kabbany, M.N. Single Center Experience of Oral Vancomycin Therapy in Young Patients with Primary Sclerosing Cholangitis: A Case Series. Livers 2023, 3, 93-104. https://doi.org/10.3390/livers3010009
Alenchery AJ, Patel S, Mahajan L, Kurowski JA, Worley S, Hupertz V, Radhakrishnan K, Kabbany MN. Single Center Experience of Oral Vancomycin Therapy in Young Patients with Primary Sclerosing Cholangitis: A Case Series. Livers. 2023; 3(1):93-104. https://doi.org/10.3390/livers3010009
Chicago/Turabian StyleAlenchery, Amala J., Sophia Patel, Lori Mahajan, Jacob A. Kurowski, Sarah Worley, Vera Hupertz, Kaddakal Radhakrishnan, and Mohammad Nasser Kabbany. 2023. "Single Center Experience of Oral Vancomycin Therapy in Young Patients with Primary Sclerosing Cholangitis: A Case Series" Livers 3, no. 1: 93-104. https://doi.org/10.3390/livers3010009