1. Introduction
Climate action failure is the second top global risk in 2021 (followed by extreme weather) [
1]. Currently, commitments made by nations to address climate change (nationally determined contributions) fall short of commitments needed to limit global warming to well below 2 degrees Celsius [
2]. Countries around the world are implementing and legislating policies and laws to effect the goals of achieving net zero emissions by 2050 [
3]. These commitments will require the phasing out of fossil fuels and more renewables, including wind, solar, and geothermal. The International Energy Agency, the leading energy organization covering all fuels and technologies, in a 2019 report, concluded achieving the Paris Agreement cannot be made without an increase in nuclear power [
4]. The mix of power production sources that jurisdictions will adopt in this transition is complicated and contextual [
5]. In Canada, the provinces of Saskatchewan, Ontario, New Brunswick, and Alberta have recently signed a memorandum of understanding to coordinate in exploring small modular nuclear reactors (SMRs), and demonstration projects are advancing with potential availability in 2026 [
6]. In the past, nuclear deployment has been limited due to public perceptions of risk, many concerning exposure to high doses of radiation due to accidents [
7], but also including radiation risks from normal plant operation (even though these are no different than natural or medical sources [
8,
9]).
Nuclear experts (In this paper, we use the term “Nuclear Expert” for people who answered positively to the question “Do you have personal experience working in a job that involves the use of radioactivity (e.g., nuclear power plant, industry or hospital using radioactive sources, natural radioactivity in ores and other materials)?”) perceive risks to radiation in respect of LDR and nuclear power generation very differently than non-experts or the general public [
10]. Previous studies have concluded that public perceptions of risk in relation to nuclear power plants are not likely shared by nuclear experts [
11]. However, nuclear experts mostly express risk surrounding nuclear medicine radiation exposure, while non-experts do not [
10]. Experts and the general public regard risk very differently. For experts, risk and uncertainty in science are accepted, but for the general public, it means anxiety [
12]. Social science documents how uncertainty, fear or dread, and distant long-term risks impact people’s perceptions of risk [
13]. But while experts have more accurate perceptions of risk, it is not the experts that determine the vision for society’s future [
14]. How people think about the risk and benefits of climate change and clean energy technology is important in relation to the acceptance of clean energy technology [
15,
16]. It is clear that how to mitigate and adapt to climate change is a messy problem where people, policy, and social choices play an active role in the success of decarbonized energy technologies [
17,
18].
A report presented by the National Council on Radiation Protection and Measurements in 2009 in the United States concluded that although the largest LDR exposure of people is to naturally occurring radiation in our environment (37% radon and 13% other), people are exposed to cosmic radiation (with people living at higher altitudes receiving more), terrestrial radiation (from soils enriched with uranium such as in Yellowknife, Canada which measures the highest), and through inhalation (through radon gas emitted from the ground and inhaled with residents in Manitoba and Saskatchewan receiving the most) and ingestion (through food and water) [
19]), medical imaging (such as CT Scans and Chest X-rays) (48%), airplane travel 2%, and nuclear power plants (0%) account for the remainder [
20]. These concerns have not contributed to the reduction of LDR exposure in medical imaging or people’s rejection of these medical procedures, as people’s exposure to LDR is increasing. According to Dr. Evans from the University of Vermont College of Medicine, “Only one-third of individuals who received a medical imaging test in the past year were educated by their healthcare professional about the risks of these tests” [
21,
22,
23].
Many studies document: (1) peoples’ concerns and misperceptions surrounding sources and risks of low dose radiation (LDR) (defined as below 100 mSv of ionizing radiation) [
11,
12,
21,
22,
24,
25]; (2) peoples’ concerns post-accident to LDR after accidents such as Fukushima or Chernobyl [
26]; (3) peoples’ concerns surrounding nuclear energy in relation to accidents and potential exposure to high dose radiation [
7]. While there are studies of people’s perceptions of risks of nuclear energy in relation to climate change [
27,
28,
29], exploring differences in expert and the general public’s risk perceptions in relation to nuclear energy [
30,
31] and LDR [
10,
25], the authors found it very difficult to get studies linking people and experts’ risk perceptions surrounding LDR and nuclear energy together. There is one study that asked about risk perceptions in Vermont to LDR, including those from a nuclear power plant, but not in relation to the acceptability of nuclear power production [
21]. Another study run in Europe in 2017 among participants that had a professional connection to radiation protection or the use of radiation in medicine or industry found that people with a high level of scientific/technical knowledge trust the radiation protection industry, and they also expressed satisfaction with the information available on radiation risk [
32]. This research answers three questions for the Canadian provinces of Ontario and Saskatchewan:
- (a)
What are the differences in knowledge and perceptions about radiation between radiation workers, those with deep expert knowledge, and the general population?
- (b)
Do radiation workers and the general population express the risks and benefits associated with radiation differently?
- (c)
Do radiation workers and people with deep expertise in radiation have a higher degree of acceptance of nuclear power and small modular reactors (SMRs)?
2. Knowledge, Risk, and Uncertainty Surrounding Radiation
A rich literature has been amassed over the last decades surrounding people’s perceptions of LDR, radiation, and nuclear energy [
27,
30,
33]. Research shows that people do not assess the risks of climate change, nuclear power, and LDR exposure in the same way [
27]. Very often, people will answer questions about LDR, radiation, and nuclear issues using various heuristics that are based on what they know and what they do not know or a form of guessing [
30]. Emotions, or affect, are part of this response based on fast, intuitive, automatic responses which are not accessible to conscious awareness [
33]. Fear, anxiety, pain, discomfort, diverse moods, and emotions are affective states, and these are real, rapid, and automatically experienced [
22]. Affective responses interact with cognitive (thinking) responses and influence all decision-making and attitudes toward LDR and nuclear power [
22,
34].
This behavioral science informs the communication framing and messaging around LDR and radiation. In prospect theory, or loss aversion theory, even with an equal probability of an equal outcome, people prefer avoiding loss rather than securing gains [
12]. Underpinned in prospect theory, Takebayashi et al. [
13] explored the impact of people’s perceptions of risk in relation to LDR and radiation. This study established that fear or dread, uncertainty, and time frame (immediate versus long term) of the consequences of radiation exposure are important factors in people’s decision-making. People’s risk acceptance increases as the degree of benefit associated with the exposure increases. For people with a medical issue, the benefit of radiation treatment or X-rays is accepted in relation to the harm that might be suffered without such a medical procedure. In respect of non-medical radiation, such as the irradiation of food, different framing is required; a framing of positive gain through the process of irradiation is preferred [
12].
Framing of science issues, and LDR and radiation specifically, is an important component of the information communication surrounding radiation and LDR. Studies confirm that the media plays a key role in forming people’s attitudes [
35,
36], often increasing negative perceptions and perhaps heightening fear based on the way messages are framed [
35,
37]. By amplifying negative imagery, the media has been shown to reduce trust [
38,
39]. Hendee [
40] concluded that the news media and entertainment industry have contributed to the public’s concern and abhorrence of radiation, radioactivity, and nuclear energy. The lack of scientific education results in an increase in the media’s influence [
41]. However, the longer people pay attention to media coverage, the higher their satisfaction with information and the lower their perception of risk in relation to nuclear science [
42]. Thus, the length of time of engagement is a factor in forming risk perceptions.
The unidirectional provision of scientific information by scientists to the public in an attempt to fill their deficit of knowledge has been proven ineffective [
43,
44]. Instead, new approaches consider behavioral science and affect and group identity [
45,
46]. Further, the methods of dissemination and goals of dissemination are key considerations [
46,
47]. Goals of increasing substantive scientific knowledge and scientific methods, or expanding the participants’ consideration of how science informs and advances society, are key components and considerations [
46,
47]. Studies have found that consideration of nuclear power in the context of climate change has improved people’s attitude to nuclear power as they consider the benefits of climate change mitigation [
48]. However, there has been documented confusion that nuclear is a carbon-free source of energy [
49].
Previous studies document how people working with radiation and medical professionals can have confusion and misunderstanding surrounding LDR and the health risks of radiation [
10,
25]. These medical/nuclear experts also think and express LDR and radiation risks differently from laypeople [
12]. Physicians focus on medical benefits and risks in terms of medical results, while physicists focus on radiation delivery and keeping doses as low as reasonably achievable. Epidemiologists express risk in terms of effects on a population [
22]. Thus, while there is a clear basis in the literature for the importance of medical and radiation experts in communicating to the public about radiation and LDR, there is a cause for further investigation. This research explores the questions of how radiation workers and those with deep knowledge express the risk and benefits of radiation and think about nuclear power and SMRs.
3. Methods
This article reports part of the findings of two representative surveys conducted in Saskatchewan and Ontario surrounding perceptions (including risk perceptions) of LDR and nuclear energy, specifically SMRs. After the surveys, thirteen focus groups were conducted to explore the survey findings in more depth. Respondents were asked if they had experience working with radioactivity. Specifically, “Do you have personal experience working in a job that involves the use of radioactivity (e.g., nuclear power plant, industry or hospital using radioactive sources, natural radioactivity in ores and other materials)?” People with this experience are referred to as ‘radiation workers’. Approximately 22% of Saskatchewan Respondents and 18% of Ontario respondents answered in the affirmative. This research compares the results of those who identified as radiation workers with those who did not or the general public.
The provinces chosen were Saskatchewan (western Canada), a uranium mining province, and Ontario (central Canada), a nuclear power-dependent province. The survey was conducted by telephone and included 1004 respondents from Saskatchewan and 1008 from Ontario during the months of November 2019 to July 2020. There were slightly more female respondents than males, reflecting the gender distribution of Canada. Indigeneity was also reflected (151 Indigenous or 7%). The survey was slightly skewed to older people, with those aged 65–75 being more numerous.
Respondents reflected the population in respect of gender and geography. In total, there were 1017 female respondents, 995 male respondents, and 6 non-binary/third gender/other respondents. There were slightly more female than male respondents from Saskatchewan compared to Ontario. In total, there were 151 Indigenous respondents and 1863 non-Indigenous respondents. There were more Indigenous respondents from Saskatchewan (101) than from Ontario (50). Older respondents were the most numerous (65–75), followed by (55–64); younger respondents were less represented.
At the end of the survey, participants were asked if they wished to participate in a focus group. In total, 17 focus groups were conducted through 2020 and 2021 with a representative sample by gender and age. Thirteen of these focus groups were held with the general public, and four focus groups with people who had experience in the nuclear and radiation field, as indicated in
Table 1. Of the general population, six occurred in Saskatchewan and seven in Ontario. There were two focus groups with radiation workers in Saskatchewan and two in Ontario. Of these four focus groups with radiation workers, one focus group in Ontario, one in Saskatchewan contained experts only, and one focus group in Ontario and one in Saskatchewan contained a mix of experts and non-experts in relation to their level of understanding of radiation. This composition was not pre-planned but was determined after analyzing the focus groups based on the participants rating their own knowledge and answering questions surrounding LDR and radiation correctly.
Participants were screened for age and gender representation. The first four focus groups in Saskatchewan were held face to face, but after March 2020, focus groups had to be conducted online via Zoom due to COVID-19.
The focus groups were taped and transcribed and then analyzed using both NVivo qualitative data analysis software and SPSS (Statistical Package for the Social Sciences software). Coding was both thematic (utilizing the focus group guide) but also inductive, whereby multiple variables that included new themes were created, and then each focus group was compared for similarities and differences as well as different knowledge levels surrounding radiation and perceptions of risks.
4. Results and Analysis
This section analyses and highlights significant differences between the general population and radiation workers, first in their understanding of radiation and LDR, and second, their concerns about and perceptions of the benefits of LDR and radiation.
4.1. Understanding of Radiation and LDR
Radiation workers who participated in the focus groups had a higher degree of knowledge surrounding radiation than those who identified as radiation workers in the survey. In the surveys, those who identified as radiation workers had a slightly higher understanding of LDR (65% of radiations workers, or 14% more than the general population, correctly answered that it was ‘true’ that there are two kinds of radiation—ionizing and nonionizing). However, radiation workers in the focus groups had a much greater understanding of the two types of radiation (ionizing and nonionizing), with only two out of 25 radiation worker focus group participants incorrectly answering this question. Radiation worker focus groups also identified that nonionizing radiation could include electric and magnetic fields, radio waves, microwaves, or ultraviolet waves and does not have enough energy to ionize atoms or molecules [
50]. Radiation workers’ focus groups were also more accurate in identifying where LDR occurs naturally in soils, rocks, airplanes (sky), potassium in your own body, radon in your basement, everywhere, sources at work, helping crops survive, helping people with illnesses, and sterilizing [
51].
Conversely, people who did not identify as radiation workers in the survey (termed the ‘general population’) fared much better at answering questions about radiation than in the focus groups (due to the statistical probability of answering a question with only two answers correctly). Overall, 52% of the general population in the survey answered the question about two types of radiation correctly, but in the focus groups, only three participants (out of 101) admitted having heard about ionizing and nonionizing radiation previously. Only one of these provided the correct definition of ionizing radiation.
Comparisons of the answers to medical treatments that expose patients to ionizing radiation, including X-rays, CT Scans, MRIs, and ultrasounds in focus groups and surveys, also confirmed this finding. When asked to identify medical treatments that were a source of ionizing radiation, there was no significant difference between radiation workers and the general population in the survey. Overall, 75% of respondents identified dental X-rays and chest X-rays as sources of ionizing radiation, but only 66% correctly identified a CT scan and just under 60% a mammogram. Meanwhile, 55% incorrectly identified an MRI, and 35% incorrectly identified an ultrasound. Radiation workers answered these questions differently by a few percentage points. Again, focus groups for the general population demonstrated greater incorrect answers to these questions. A few people in the general population just could not believe cell phones and microwaves did not generate LDR.
A few radiation workers also experienced similar confusion. However, most radiation workers in focus groups did correctly identify the medical treatment sources of ionizing radiation. From the radiation worker focus group discussions, the initial explanations of ionizing appear to influence the group into deferring to the early identified experts for answers. This provides an explanation for why the radiation worker focus group discussions were more accurate than the radiation worker survey results. Radiation workers were more accurate in identifying where LDR occurs naturally in soils, rocks, airplanes (sky), potassium in your own body, radon in your basement, sources at work, helping crops survive, helping people with illnesses, and sterilizing [
51].
4.2. Perceptions of Radiation Risks and Benefits
4.2.1. Perceptions of Risk of Exposure to Radiation in General
Significant differences emerged from the focus groups and the survey surrounding perceptions of risk and LDR in relation to LDR harming health and causing cancer. When surveyed, 73% of respondents answered that it was true that exposure to radiation, even at extremely low doses (several microsieverts), might harm their health, and there was no significant difference between the general public and radiation workers (74% general population and 70% radiation workers). Overall, 24% believed this to be false (23% general population and 28% radiation workers), and the rest did not know or did not answer. Similar results were found when asked if they believed LDR could influence cancer. In total, 53% of survey respondents answered in the affirmative (52% general population and 57% radiation workers), and 36.7% in the negative (36% general population and 37% radiation workers). The remainder answered that they did not know or refused to answer.
Very different positions were taken on this issue in the focus groups. The survey question was not directly asked in the focus groups, but there was a question surrounding ‘concern’ regarding LDR. In the general population focus groups, only a small minority of people expressed concern over exposure to LDR, and in the radiation workers, only two individuals (described more comprehensively in
Section 4.3) did so. Several in the general population groups asked questions about when low levels become harmful and whether there was a cumulative effect resulting in a potential for cancer.
There was very little concern about LDR expressed in the radiation worker focus groups. Many acknowledged LDR risk was not necessarily zero but tolerable. One said, “I thought about it, realized the very low risk and put it out of my mind.” Another, “I don’t know the exposure limits by regulation but even the maximum dose allowed by law is a magnitude lower than the amount needed to cause health issues.” One participant said, “and once you learn more about radiation and doses, etc., you really stop being concerned.” Later they said, “If you work around higher-level stuff, the low dose stuff doesn’t make you bat an eye.” In the Saskatchewan focus group full of knowledgeable radiation workers, a similar experience occurred. For example, one person stated, “I’m ok with it all. I’ve waded through radioactive tailings when I was a teenager. Pretty immune to radiation now-a-days. Have four healthy kids.” Generally, most felt LDR risk was negligible compared to life’s other health and safety risks.
These observations and statements did not mean these participants were nonchalant about radiation. They still were careful and cautious when working with it on a daily basis but stated, “you’d be hard pressed to reach that high dose limit without a medical intervention or accidental exposure.” A few identified that industrial radiography equipment could have a high source of radiation, but it is shielded, so per se, not a high-dose source. Radiation workers did speak to their protective practices, including the use of dosimeters, using the principle of ‘ALARA,’ or ‘as low as reasonably achievable,’ and time, distance, and shielding NORM guidelines, working in a lead box (so their exposure is even less than the general public). Employees who used dosimeters stated they were always below their yearly exposure limits. Reference to safety and practice courses at work, monitoring and correcting equipment, recordkeeping, RAD testing, CNSC audits, and yearly reviews were also made. Participants in the expert radiation workers’ focus groups felt well-informed about radiation, with nothing missing.
General population focus groups were concerned about high-dose radiation, but there was no discussion of this in the radiation worker focus groups. Participants in general public focus groups identified high radiation dose exposure as coming from uranium mining and nuclear power plants—with a few stating “nuclear plant accidents.” People in Hamilton were concerned about people living in Darlington being exposed to high-dose radiation. These statements illustrate that it is not only affect and heuristics but also group identity or cultural theory and people that are egalitarians (concerned about other minorities and vulnerable groups) that express concern about nuclear [
30].
4.2.2. Perceptions of Risk of Exposure to Radiation from Medical X-rays, Power Facilities, and Occupational Exposure
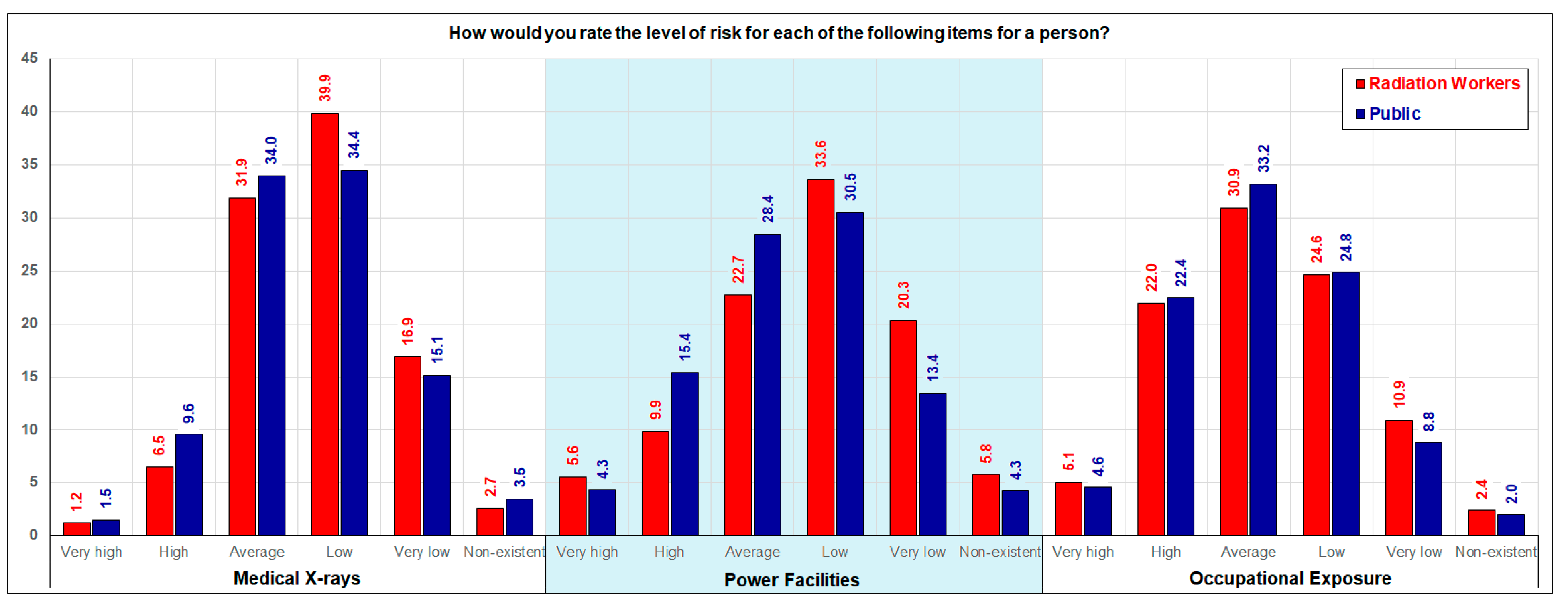
In the survey, respondents were very similar in ranking the risk of radiation exposure in relation to medical X-rays, power production facilities, and occupational exposure. Radiation workers rank risk marginally lower in relation to medical X-rays and power production facilities, but in relation to occupational exposure, there is more commonality, as depicted in
Figure 1. More survey respondents ranked the risk of occupational exposure to radiation as average, high, and very high than they did medical X-rays and power facilities. There was little discussion of occupational exposure to radiation in the general population focus groups, but as described in
Section 4.2.1, there was much discussion in the radiation worker focus groups. However, the concern expressed in the focus groups was generally low (which is not consistent with the radiation workers’ answers to the survey). However, the expert radiation worker focus group discussion was very focused on protective measures that made the risk of exposure to radiation very small. The wording of the survey question does not qualify for precautionary measures as the question was, “How would you rate the level of risk of radiation from occupational exposure?”
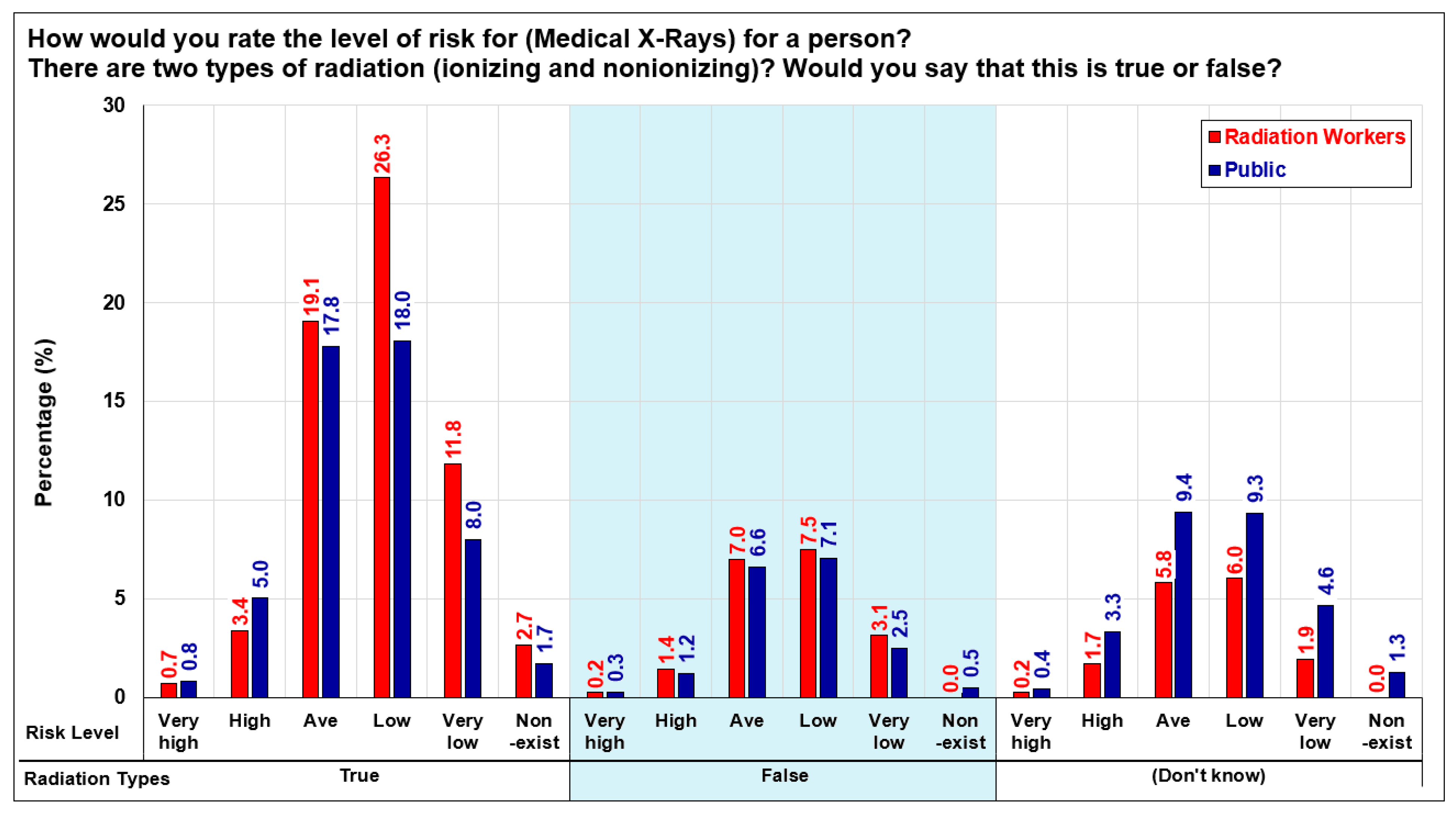
Figure 1 shows medical X-rays receiving the highest number of respondents ranking risk as low or very low, followed by power facilities. Survey results adjusted for the correct answer of ‘true’ to two types of radiation (ionizing and nonionizing) and ranking of risk for medical X-rays are illustrated in
Figure 2. More survey respondents correctly answered this question and ranked risk from medical X-rays as average to non-existent. More radiation workers than the public ranked the risk as low, very low, and non-existent. Similar findings in relation to the risk of power facilities are illustrated in
Figure 3. Only a small percentage of those who did not know the answer surrounding ionizing and nonionizing radiation also ranked the risk of X-rays as high or very high.
In the survey, 7.7% of radiation workers, compared to 11% of non-radiation workers, rated the level of risk from X-rays as high or very high. These concerns were generally congruent with the literature where people are concerned that X-rays might be harmful (carcinogenic) and radiation might accumulate in the body [
24]. While the discussions surrounding X-rays in the focus groups generally revolved around the benefits of X-rays outweighing the risks, there was often acknowledgment of keeping LDR exposure to a minimum through infrequent X-rays.
In the survey, only 14% of the general population and 18% of radiation workers reported a time when they ‘declined’ to undergo an X-ray examination. In the general population focus groups, the benefits of X-rays were discussed, and no participants described a time when they had refused an X-ray. A few mentioned a time when a doctor advised an X-ray was not necessary.
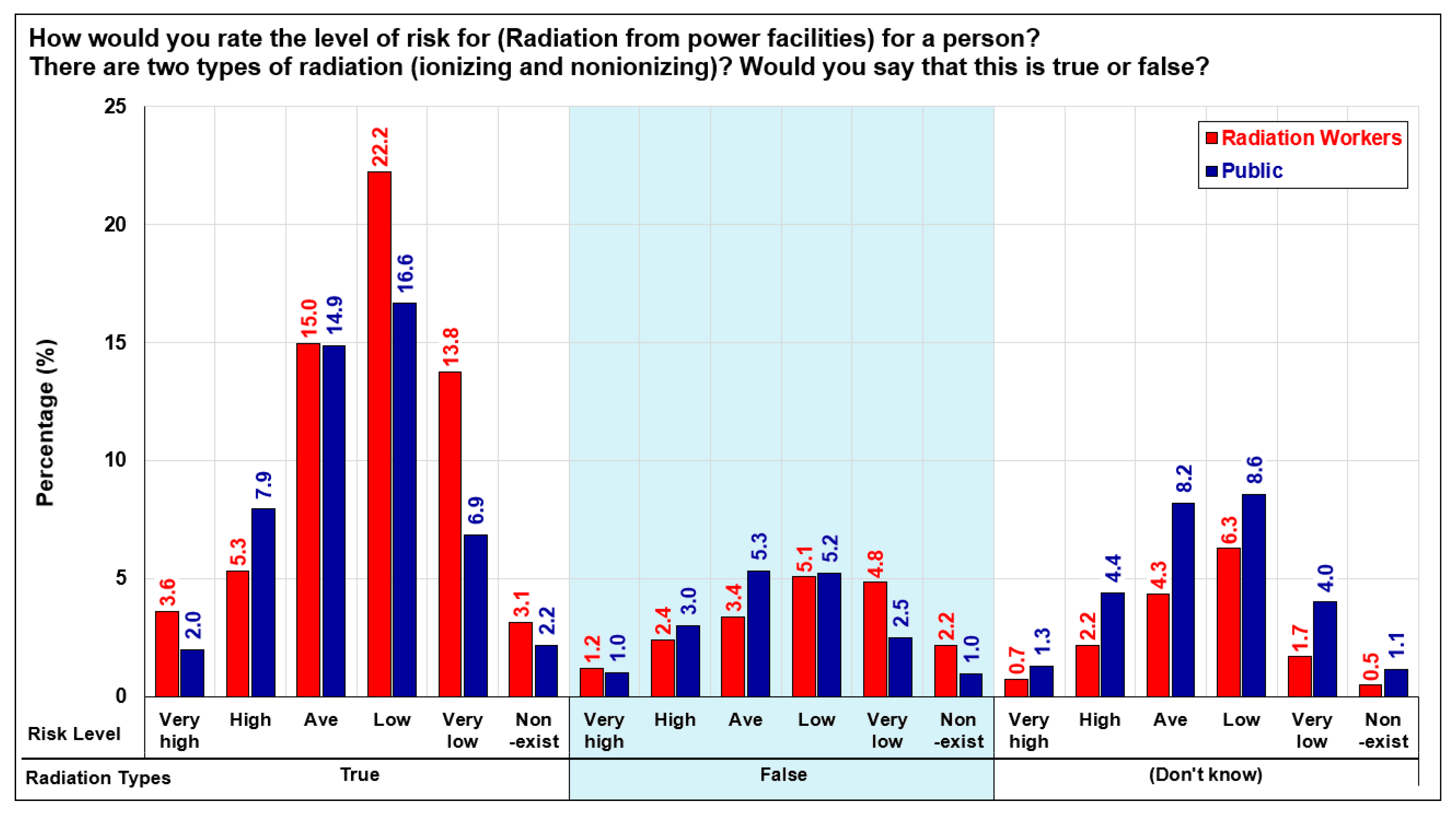
Survey results adjusted for the correct answer of ‘true’ to two types of radiation (ionizing and nonionizing) and ranking of risk from power facilities, as illustrated in
Figure 3. More survey respondents correctly answered this question and ranked risk from power facilities as average to non-existent. More radiation workers than the public ranked the risk as low, very low, and non-existent. Similar findings in relation to the risk of power facilities are illustrated in
Figure 3. Again only a small percentage of respondents who did not know the answer to the ionizing and nonionizing radiation question ranked the risk of radiation from power facilities as high to very high; the majority ranked the risk from average to non-existent.
Statements of the general population demonstrated cultural concern for people living near nuclear plants (whom they believed were exposed to radiation). In contrast, radiation workers expressed a different form of egalitarian thinking. For radiation workers, nuclear power was a solution to the problem of climate change. Based on the data collected in this study, it was not possible to conclude if other ‘group identities,’ such as hierarchists (who see the world in structured, centralized terms) and those generally agreeable to nuclear power [
30], dominated in focus groups.
Both
Figure 2 and
Figure 3 show that respondents that answered the ionizing and nonionizing questions correctly had a greater number of respondents who ranked risk as average, low, and very low. Stated another way, the respondents who answered the ionizing and nonionizing questions incorrectly had a much flatter curve in relation to the risk ranking of both X-rays and radiation from power facilities. This group is more diverse in perspective in relation to ranking risk from high to low, while respondents answering correctly are more in agreement by centering their risk ratings in the average to very low categories. However, the focus groups did not reflect these results in relation to knowledge (as described in
Section 4.3) and the discussion surrounding the risks and benefits of radiation.
4.2.3. Identification of Benefits of Radiation
Focus group discussions also covered participants’ views of the benefits of radiation. People working with radiation were supportive of the technologies that result from nuclear science, and some (including people in the general population) recognized the benefits of exposure to LDR. Many radiation workers also cited the benefits of nuclear power and addressing climate change. Both the general population and radiation workers identified the benefit of radiation in relation to cancer. In a few general population focus groups, the irony was pointed out that radiation is portrayed in fictional books and movies as ‘evil,’ but it actually is beneficial in treating cancer. Radiation workers also made this observation:
“I work in a profession that treats cancer patients daily with radiation. Most people don’t understand what radiation therapy is. They often think we are Radiologists, most people associate cancer with chemotherapy and are very unfamiliar with the benefits of radiation. It typically has a negative association from my experience.”
In the survey and the focus groups, radiation workers were twice as likely to ‘strongly agree’ with the statement that the benefits of radiation outweigh the risks than non-radiation workers. People without experience working with radiation (the general population) were twice as likely to be undecided when asked if the benefits of radiation outweighed the risk.
Most focus group participants listed the benefits of radiation, including power, cooking, modern lives and living in the modern world, and living longer with medical therapies. All focus group participants, especially the expert groups, felt the benefits of LDR outweighed the risks. One expert stated, “I think nuclear energy and almost all aspects of nuclear science are absolutely amazing and they have helped revolutionize our world.” Radiation worker focus groups provided examples related to the benefits of technology and medical procedures that are possible because of nuclear science. One in the Saskatchewan expert radiation worker group pointed out radiation is more of a tool than harmful. One expert in the Ontario mixed focus group pointed out that everyone was discussing the benefits of the technology (medical diagnoses, medical cancer treatments) and not of the radiation itself. The group then started talking about the benefits of sunlight, synthesis, and vitamin D. They also listed benefits, including the increased immune system and which results in fewer health issues and provides treatment for alleviating arthritis. The very knowledgeable worker in the mixed Ontario focus group stated that there is some evidence LDR may be healthy, “kind of like salt in your diet—a little bit is good, too much is bad and protect yourself, focus on sunlight first.” The Saskatchewan expert focus group also listed the ability of small exposures to activate certain DNA repair mechanisms in the body. One cited studies that showed that LDR could reduce cancer. Radiation workers felt the benefits outweigh the risks, pointing to higher life expectancy because of the X-ray tests and medical advances. In the radiation workers’ focus group, several expressed the sentiment that there were many other things people should be concerned about that likely need more attention.
4.2.4. Level of Support for Small Modular Nuclear Reactors (SMRs)
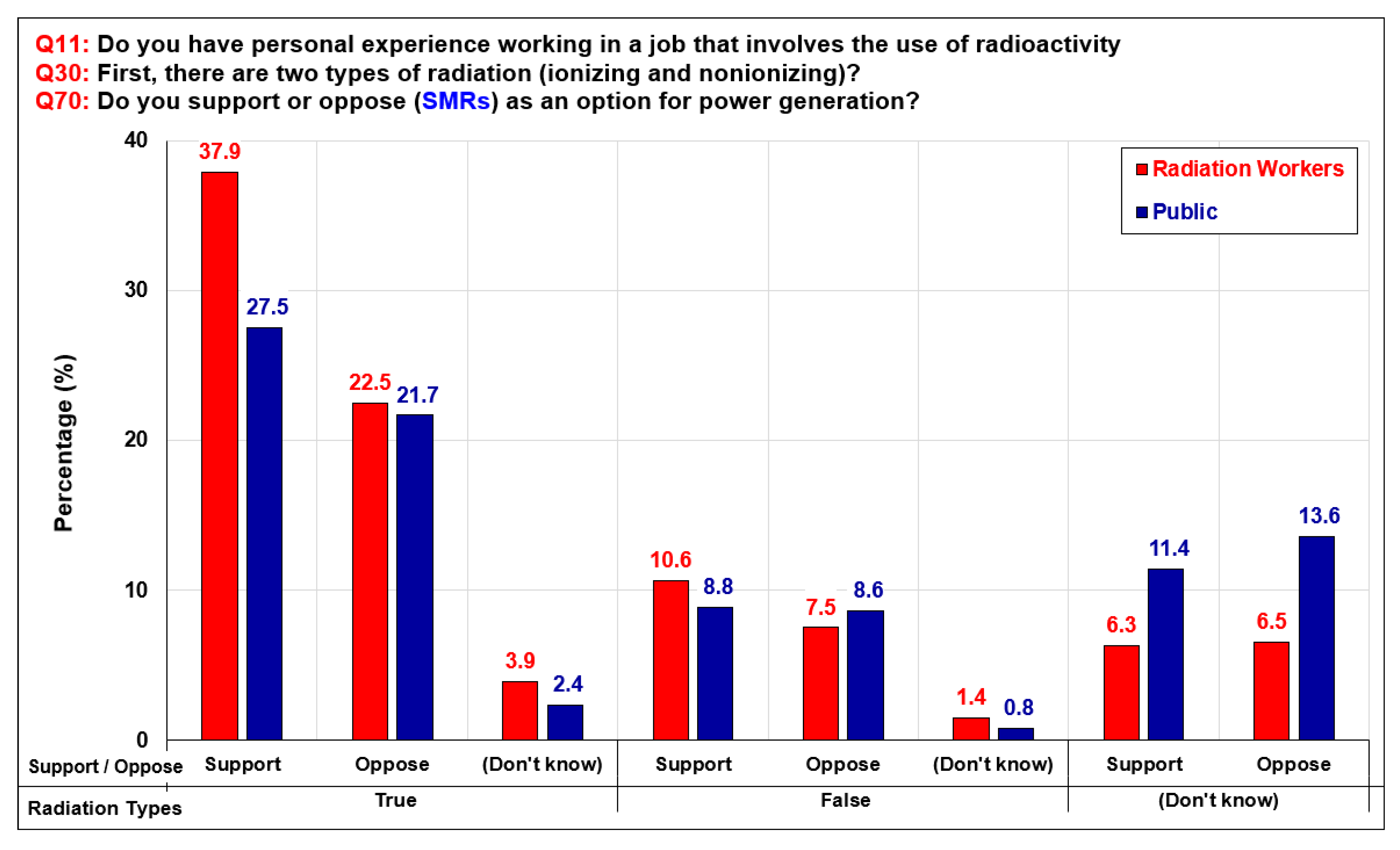
When asked if respondents would support or oppose SMRs as an option for power generation, the level of support was highest amongst radiation workers and radiation workers who correctly answered the question about ionizing and nonionizing radiation. This is also the case with the general public, as shown in
Figure 4. Of those that answered the question about ionizing radiation correctly, 37.9% of radiation workers and 27.5% of the general public support SMRs as a new power source. For respondents that did not answer the ionizing and nonionizing radiation questions correctly, respondents were evenly split in support of and opposition to SMRs. This was the case for both the radiation workers and the general public.
4.3. Emotions and Concerns about LDR and Radiation
In the survey, more radiation workers were positive (18%) or neutral (37%) when hearing the word ‘radiation’ than the general population (7% positive and 29% neutral). More people that were not radiation workers reacted negatively to the word ‘radiation’ (28%) than radiation workers (16%). This survey finding was also replicated in the focus groups.
In the focus groups, radiation workers were more likely to acknowledge that LDR was unavoidable, existed everywhere in a variety of doses, and was impossible to avoid. As a group, they talked about their own history of being tested, and a few identified that they were healthy into their 70s or later, so it was not likely harmful. In the radiation worker focus groups, people with an emotional response to radiation had less understanding of radiation and LDR than their colleagues. Radiation workers who had high knowledge and correctly answered questions surrounding LDR and radiation used fewer emotive words to describe radiation.
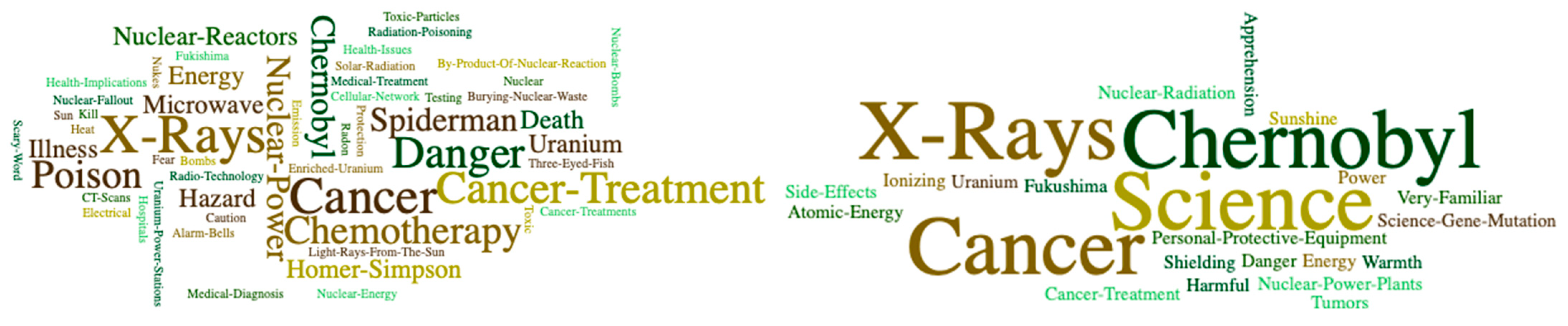
Radiation workers’ initial emotions and responses to the word ‘radiation’ in the focus groups were different from the general public. When focus group participants were asked what they associated with the word ‘radiation’ and what comes to mind when they hear the word ‘radiation,’ the public focus groups generated a very different world cloud than the radiation workers (
Figure 5). The responses to these questions were recorded and divided into two groups: all responses for the general population focus groups and all responses for the radiation worker focus groups. A word cloud was generated for each. More participants were in the general population focus group, so a larger word cloud was generated. Words in small print only appeared once, and larger words were used by more participants.
Emotive responses based on fast, intuitive automatic responses often first come to mind [
33]. While the word clouds are not statistically significant, they shed light on people’s affective first impressions or first emotional responses in relation to ‘radiation’ [
52]. Emotive words used in the radiation worker focus groups included, ‘Chernobyl, Fukushima, and apprehension.’ The people who used these words were the people in these focus groups that demonstrated the least knowledge of LDR and radiation. The person who identified ‘Chernobyl’ twice was a nurse who ranked their level of knowledge of radiation as ‘somewhat familiar’ as they had just finished nursing school as an RN. They described this knowledge as:
“Don’t have tons of knowledge on like radiation and what it is, but it is something that I am exposed to in the workplace as well. So I’ve had had training on like kind of how to protect myself and patients.”
However, this person did not know millisieverts was the measurement of radiation before the focus group (and could not name any other measurement), nor did they state they had heard the phrase LDR before. This person guessed a microwave was exposure to LDR and ‘definitely’ cell phones. Another nurse in another focus group also identified microwaves as having LDR, as well as computer screens. At the end of the focus group, this person stated, “I feel for the most part that I’m barely prepared and confident enough to care for those patients who are undergoing radiation. For example, how to handle bodily fluids that may be emitting radiation.” The radiation worker who identified ‘Fukushima’ and ‘apprehension’ lived in Japan 150 km away at the time of the incident and likewise ranked their knowledge as ‘substantial of LDR.’ But again, this radiation worker could not identify the measure or definition of LDR. This person also thought cell phones, ultrasounds, and MRIs were sources of LDR.
The fact emotive responses were expressed by two focus group participants with the least knowledge of radiation and LDR is consistent with the findings of Goodfellow et al. [
30]. Goodfellow et al. concluded that people often respond in an emotive way surrounding nuclear issues based on what they do not know or a form of guessing.
While the focus group findings are interesting, they are not statistically significant, given they concern only two people in relation to four focus groups and a total of 25 people. As a result, we tested through ordered logistical regression analysis to confirm if radiation workers were more positive and less emotive in relation to radiation and if this correlated with correctly answering the background knowledge surrounding radiation questions. We also wanted to understand these variables in relation to the acceptance of nuclear power and SMRs.
4.4. Understanding Radiation, Emotions, and Acceptance of Nuclear Power and SMRs—Ordered Logistic Regression Analyses
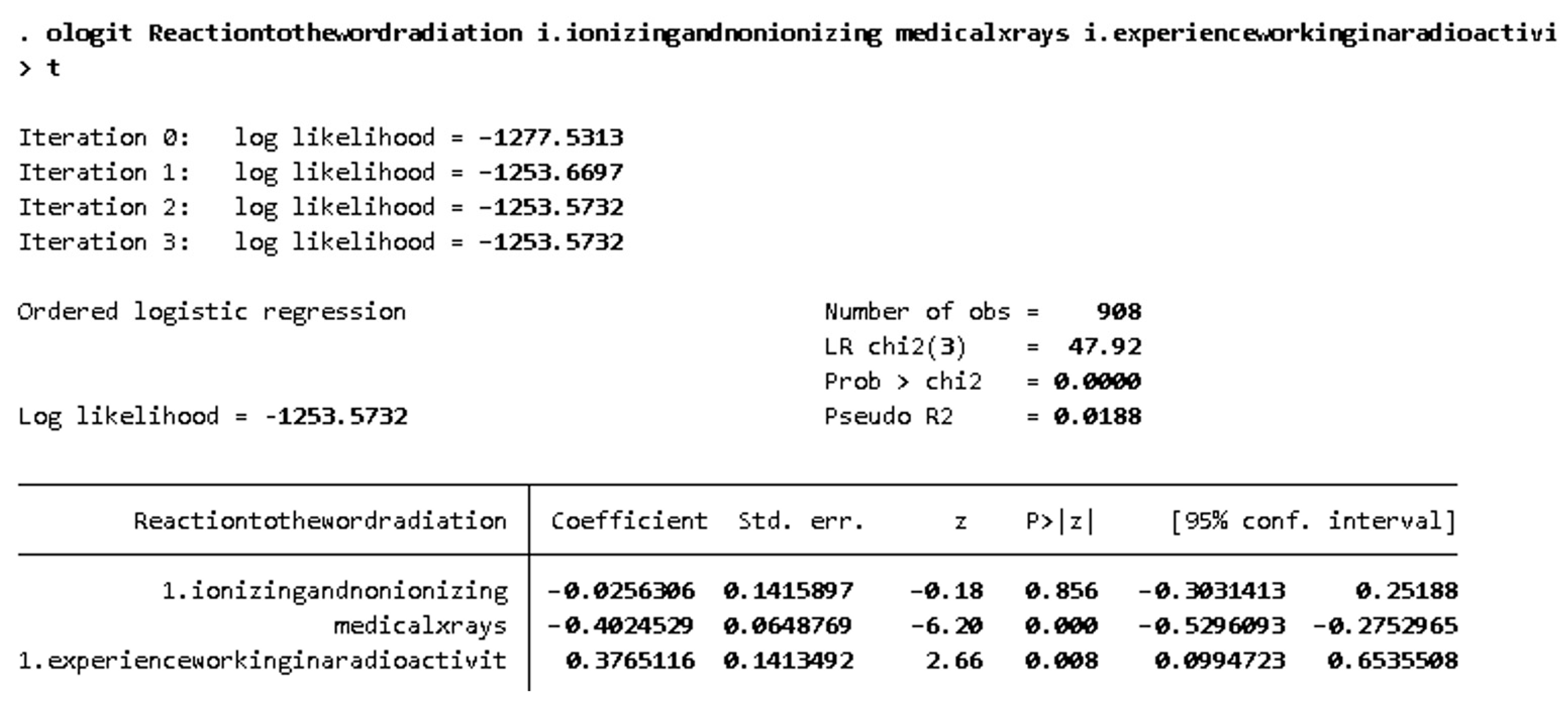
Our study's focus group and survey results varied significantly and as a result, we asked more questions surrounding knowledge of and emotion surrounding radiation within our survey analysis. To deepen our analysis of the survey results, two ordered logistic regression models were built to investigate two research questions of this paper. Statistical analyses were carried out using STATA 17.0. Ordered logistic regression was used because of the ranked categorical data of the dependent variables under investigation. For research question 2: Do radiation workers, people with deep expertise in radiation, and the general population express risks and benefits associated with radiation differently? The dependent variable was the survey question, “Overall, when you hear the word “radiation”, would you say that your first reaction is…” Ranked answers to this question were coded as 1 “Entirely negative” 2 “Mainly negative” 3 “A mix of positive and negative” 4 “Neutral” 5 “Mainly positive” 6 “Entirely positive.” Independent variables included (1) whether or not respondents correctly answered that there are two different types of radiation (ionizing and nonionizing), which is a categorical binary variable where 0 = false (or incorrect) and 1 = true (or correct); (2) the level of risk assigned by respondents to radiation from medical X-rays (coded 1 “non-existent” 2 “very low” 3 “low” 4 “average” 5 “high” 6 “very high”); and (3) whether or not respondents said they had personal experience working in a job that involves the use of radioactivity (e.g., nuclear power plant, industry or hospital using radioactive sources, natural radioactivity in ores and other materials)—a binary categorical variable where 0 = no and 1 = yes. After removing missing data (those who answered either “Don’t know” or “Refused” within the set of survey questions under investigation), 908 observations remained.
According to this model, the reaction to the word radiation is more positive among respondents who have experience working with radiation, while the reaction to the word radiation is more negative as the level of risk of medical X-rays increases. Correctly answering the survey question on ionizing vs. nonionizing radiation was not statistically significant according to this model. The likelihood ratio chi-square of 47.92 with a
p-value of 0.0000 indicates that the model as a whole is statistically significant, as compared to the null model with no predictors. See
Appendix A for STATA calculations.
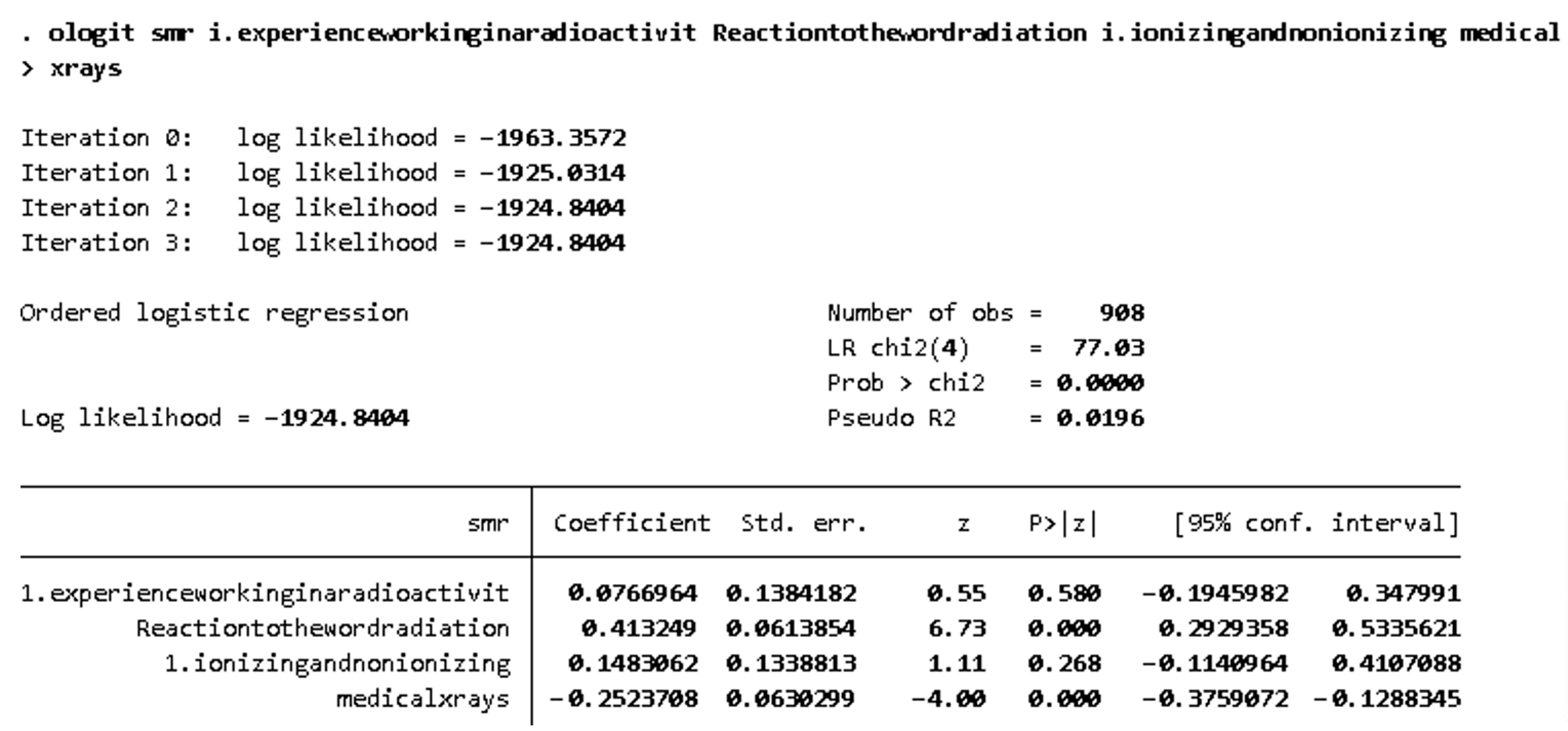
For research question 3, Do radiation workers and people with a deep expertise in radiation have a higher degree of acceptance of nuclear power and small modular reactors (SMRs)?; support for SMRs served as the dependent variable of the ordered logistic regression model. SMRs were chosen alone to avoid multi-collinearity of nuclear power and SMRs, and because survey respondents from both Ontario and Saskatchewan were asked to rank their support for SMRs while only respondents from Ontario assessed nuclear power generated from the Pickering and Darlington power stations in that province. Answers were coded from 1 to 10, where 1 = “Don’t support at all” and 10 = “Completely support.” Independent variables in this model to predict support for SMRs included survey respondents’ reaction to the word radiation, whether or not they had experience working with radiation, whether or not respondents correctly answered that there are two types of radiation (ionizing and nonionizing), and the level of risk assigned to radiation from medical x-rays. According to this model, support for SMRs decreases as the level of risk assigned to radiation from medical X-rays increases, while support for SMRs increases as the reaction to the word radiation becomes more positive. Experience working with radiation and correctly answering that there are two types of radiation (ionizing and nonionizing) are not statistically significant in predicting support for SMRs according to this model. The likelihood ratio chi-square of 77.03 with a p-value of 0.0000 indicates that the model as a whole is statistically significant, as compared to the null model with no predictors. These findings indicate that experience working with radiation and knowing the difference between ionizing and nonionizing radiation do not predict support for SMRs as much as emotional reactions to the word radiation and the level of risk survey respondents assigned to radiation from medical x-rays. As noted in this paper, survey analysis in this area differed from what emerged through the focus group discussions.
Overall, ordered logistic regression analyses of the survey results indicate that radiation workers are more likely to react positively to the word radiation than the general public, and how respondents reacted to the word radiation has a bigger impact on support for SMRs than whether or not they have experience working with radiation. Furthermore, correctly answering that there are two types of radiation (ionizing and nonionizing) is not a statistically evident predictor of either emotional reaction to the word radiation or support for SMRs when other variables are considered.
5. Discussion
This research supports previous literature’s finding that radiation workers and the general public have misperceptions about LDR and nuclear power radiation [
9,
22]. Consistent with the findings of other studies [
12,
21], people have misperceptions and misunderstandings surrounding LDR and radiation. Although radiation workers have more accurate information, they still do not all answer questions accurately. Of radiation worker focus group participants, workers who trained others in radiation and described themselves as highly knowledgeable about radiation exhibited high degrees of understanding about radiation; only two radiation workers (a nurse and someone who lived in proximity of Fukushima) did not have a good understanding of radiation.
Qualitative research methods of focus groups can uncover the significance of the lack of knowledge that survey questions do not because of the ability to ‘guess’ a true and false question correctly. In the same way, focus groups with expert radiation workers can augment the level of knowledge in the discussion as the group quickly defers to the experts in relation to technical questions. This research should not be taken as supporting the resurrection of the ‘deficit model’ or the idea that simply providing more nuclear science information, especially in a unidirectional manner, will address people’s misunderstandings and concerns. Consistent with previous studies [
10,
25], the focus group participants felt that confusion and misunderstanding surrounding LDR and its risks and benefits would benefit from prolonged engagement surrounding nuclear science, uncertainty, and risk.
Rational decision-making requires a complex interplay between both emotion and reason. Affect or ‘faint whispers of emotion’ are important in dual process theories of thinking in respect of issues of LDR and radiation [
33]. This impact of affect or emotion was illustrated through people’s initial responses and thoughts surrounding LDR and radiation. These initial responses were used to generate word clouds by focus group participants [
21,
22,
25]. Radiation workers were more likely neutral or positive when hearing the word ‘radiation’ and generated fewer emotive words in their first reactions.
Radiation workers participating in focus groups were less concerned about radiation than the general population. Radiation workers were also more likely to rank their knowledge greater than the general population and to be neutral or positive when hearing the word radiation. Because radiation workers were more knowledgeable about LDR and radiation, in their focus groups, they expressed little concern, if not acceptance of LDR, and many discussed the benefits. Radiation workers also assessed the risk level from power facilities, dental X-rays, and radioactive waste as significantly lower than the survey respondents who were not radiation workers. Radiation workers felt there were many other things that people should be concerned about before radiation. Several radiation workers provided testimonials of their advanced years, healthy offspring, and exposure to LDR from uranium mining tailings and natural sources. This is not to say radiation workers were nonchalant about radiation. Extensive measures to ensure their safety was recounted.
Focus groups identified the benefits of medical diagnostics and treatments, and no participant indicated they had ever refused an LDR or radiation medical procedure. These findings confirm benefit-risk calculation for exposure to LDR in regard to medical procedures, and avoided risks continue to be an important communication technique [
22]. Consistent with prospect theory, research participants accessed medical treatments with benefits with very little concern or questioning. Participants in focus groups concluded the benefits of radiation outweighed the negatives, but radiation workers were far more verbose and thoughtful in their explanations.
Although there has been criticism of using cultural theory or group paradigms to explain people’s risk perception [
53], this research was not designed to test group identity (elitist, individual, hierarchical, and egalitarian) through inductive coding of focus groups; two group characterizations were determined. In the general population focus groups, there were sentiments expressed of concern for people living next to nuclear power plants and their exposure to LDR and radiation. In the general population, voluntary risks associated with nuclear power generation and living in proximity were not as accepted as medical exposure to radiation. By contrast, radiation workers were concerned about climate change and its impacts on people (identifying with the climate change altruistic group [
37]) and regarded nuclear as a viable solution, where concern was expressed over the public not understanding this. These comments confirm it is not just emotion or affect that impacts perceptions surrounding LDR and radiation but also group identity [
30].
Framing of survey questions, such as “Do you believe that low dose radiation can induce cancer?” with a yes or no response/ and “Exposure to radiation even at extremely low doses (several microsieverts) might harm your health” with a true/false response may implicitly lead to a biased result due to framing. Focus group results based on the discussion of radiation and LDR did not reflect the significance of the concern found in the survey. However, the survey is both statistically significant and representative and confirmed differing concerns surrounding occupation exposure to radiation, X-rays, and power facilities. The general population’s focus groups also reflected concerns related to the last two, X-rays and power facilities.
The two participants (out of 25) in the radiation worker focus groups who used emotive words had the least understanding of radiation. This is consistent with literature that has demonstrated that people with an increased understanding of science have an increased understanding of uncertainty and are better with or more accepting of risk [
12]. Science literacy has been shown to reduce people’s risk perception surrounding LDR and radiation and increases their acceptance of nuclear power [
34]. Although focus groups demonstrated a correlation between two members of the radiation workers' expert focus group, emotional responses to the word radiation, and the lack of knowledge surrounding radiation, this was not proven within the survey. A greater divergence or polarization of support for nuclear facilities and SMRs occurred in relation to people not answering the question about two types of radiation (ionizing and nonionizing) correctly versus those that did. A standard deviation curve represented those answering the question correctly in relation to concerns surrounding radiation and power facilities and X-rays.
Using an ordered logistic regression analyses, it was determined that reaction to the word ‘radiation’ is more positive among respondents who have experience working with radiation, while reaction to the word ‘radiation’ is more negative as the level of the perceived risk of medical X-rays increased. Correctly answering the survey question on ionizing vs. nonionizing radiation was not statistically significant according to this model in relation to the emotional response to the word radiation. This result is surprising and interesting in relation to the pervasiveness of medical X-rays and the possibility that this procedure might provide for both exploring and understanding emotions and understanding and exposure to LDR.
Findings also indicate that experience working with radiation and knowing the difference between ionizing and nonionizing radiation do not predict support for SMRs as much as emotional reactions to the word ‘radiation’ and the level of risk survey respondents assigned to radiation from medical X-rays. Again, this is an interesting finding concerning the link between medical exposure to LDR through X-rays and emotions and nuclear power generation and SMRs. However, no previous studies linking the perceptions of risks and benefits, knowledge, affect, LDR, nuclear power, and SMRs could be identified. In analyzing health communication studies, Kim [
12] concludes the benefit of radiation treatment or X-rays is accepted in relation to the harm that might be suffered without such medical procedure; conversely, in non-medical radiation, a different frame of positive gain is required [
12]. Affective responses interact with cognitive (thinking) responses and influence all decision making and attitudes towards LDR [
22] and nuclear power [
34]. More research in how affective responses of attitudes to LDR in other contexts and decision making realms, nuclear power, and climate change are needed.
The most often identified need for radiation workers was for information correcting the inaccuracies being disseminated in films surrounding Chernobyl and media surrounding Fukushima. Radiation workers also strongly supported the idea of more information surrounding the benefits of LDR and nuclear power, including its very important role in addressing climate change. Literature has demonstrated that in the context of climate change, more positive attitudes to nuclear energy and acceptance of risk can occur [
48]. The general public was interested in more information surrounding LDR and basic questions about its definition, if it cumulates within the body, how it impacts people, and what level is safe.
6. Conclusions
As the risks and impact of climate change increase, governments such as Canada are increasing their laws and policies for reducing GHG emissions, including phasing out fossil fuels and replacing them with renewables and potentially nuclear power [
4,
6]. Nuclear deployment has been constrained by public perceptions of risk due to accidents [
7] and radiation from normal plant operations [
8,
9]. How people perceive the risks of climate change, nuclear power, and LDR is important in the acceptance of nuclear generations and SMR technology [
15,
16]. Nuclear science experts and the public, both in the health field of LDR and the nuclear power field, have different perceptions and expressions of nuclear risk [
10,
11]. This study is unique as it combines quantitative survey data in two provinces of Canada with qualitative focus group data of radiation workers and the general public’s risk perceptions and affective response to radiation (both LDR and radiation) and acceptance of nuclear power production and SMRs.
Radiation workers answered questions surrounding radiation more accurately than the public. In the focus groups, expert radiation workers were very accepting of radiation, ranking the risk surrounding it (including LDR) as very low. They expressed and endorsed the benefits of nuclear science and technology. Due to the statistical probability of answering survey questions correctly and perhaps the self-selection bias of people identifying as radiation experts and being willing to participate in focus groups, the radiation worker focus groups demonstrated greater radiation knowledge than the surveys.
In the radiation worker focus groups, positive affect was expressed in relation to nuclear science, nuclear power, and nuclear medical procedures. Only two participants of the radiation worker focus groups had an emotive response to the word radiation, and these were the least knowledgeable about radiation. However, the deficit model of science understanding was not found in relation to the survey analysis described below. Many of the benefits of the technologies resulting from nuclear science and the benefits of LDR were identified in these focus groups. The general public focus groups also determined that the benefits of radiation outweighed the risk.
Radiation workers ranked the level of risk from medical X-rays and power facilities as less than the public. Respondents that correctly answered the question about two types of radiation (ionizing and nonionizing) were represented in a standard deviation curve between low and high, whereas those that inaccurately answered this question had greater kurtosis, a flatter curve, and more polarization in the ranking of risk. However, an ordered logistic regression analysis confirmed these results were not statistically significant. There was more negative affect in response to the word ‘radiation’ as the level of risk of medical X-rays increased. Support for SMRs was impacted more by people’s affective reaction to the word radiation than their experience working with radiation.
In addition to findings in relation to the affect and perceptions of risk and acceptance of nuclear power production, the focus groups did demonstrate some group paradigms. The general public was concerned about people working and living near nuclear power plants; radiation workers were concerned about climate change. The general public did not understand radiation, risk, and nuclear technology. A limitation of our research is we did not explore cultural group affinities.
Study participants identified a need and desire for more information and understanding of LDR and radiation. While the general population supported this, the radiation workers were very passionate and provided many suggestions for mechanisms and specific content. More research into the impact of their suggested content and methods is required.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}