


Vaccine Hesitancy in Women of Childbearing Age and Occupational Physicians: Results from a Cross-Sectional Study (Italy, 2022)



Abstract
:1. Introduction
2. Results
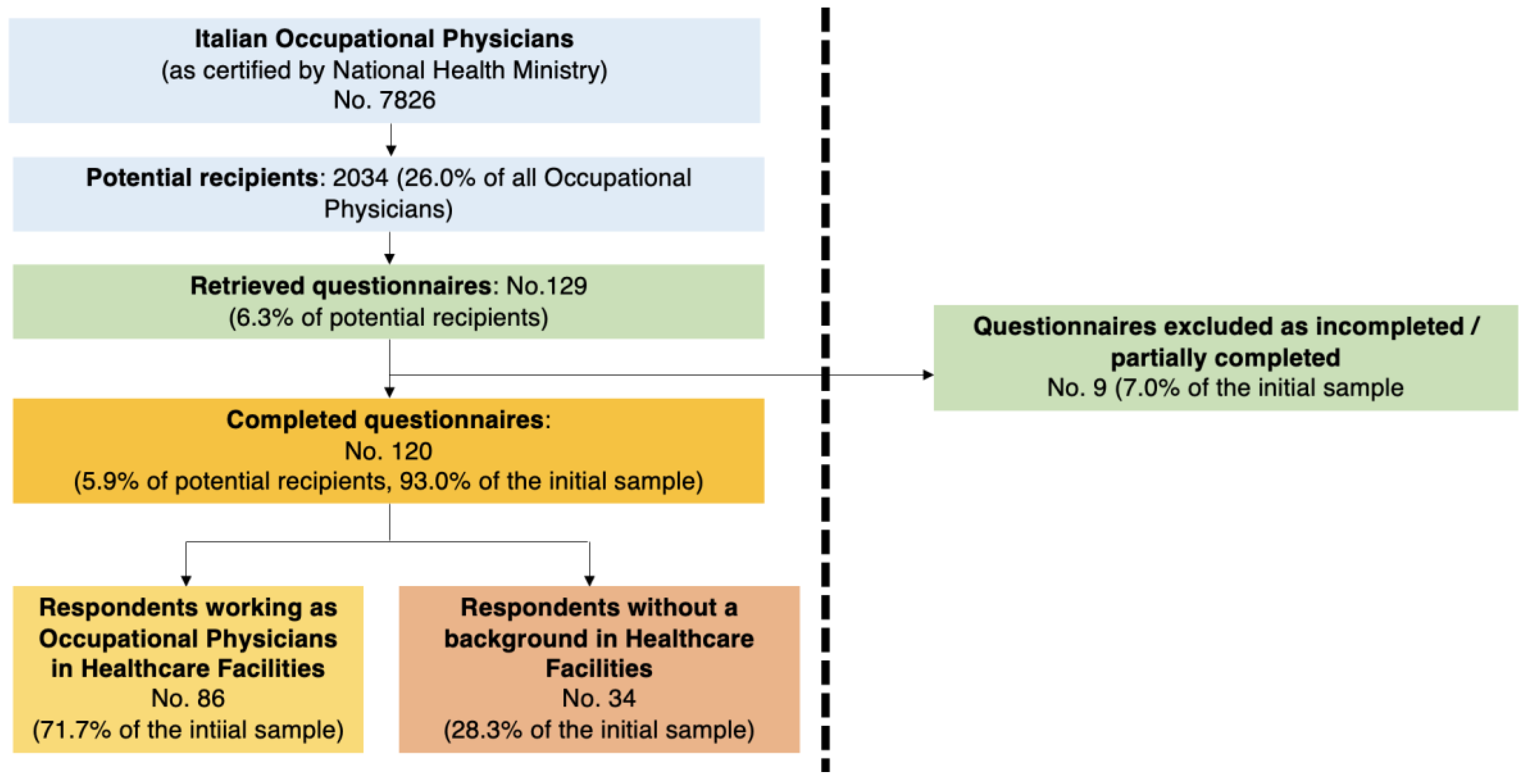
2.1. Descriptive Analysis
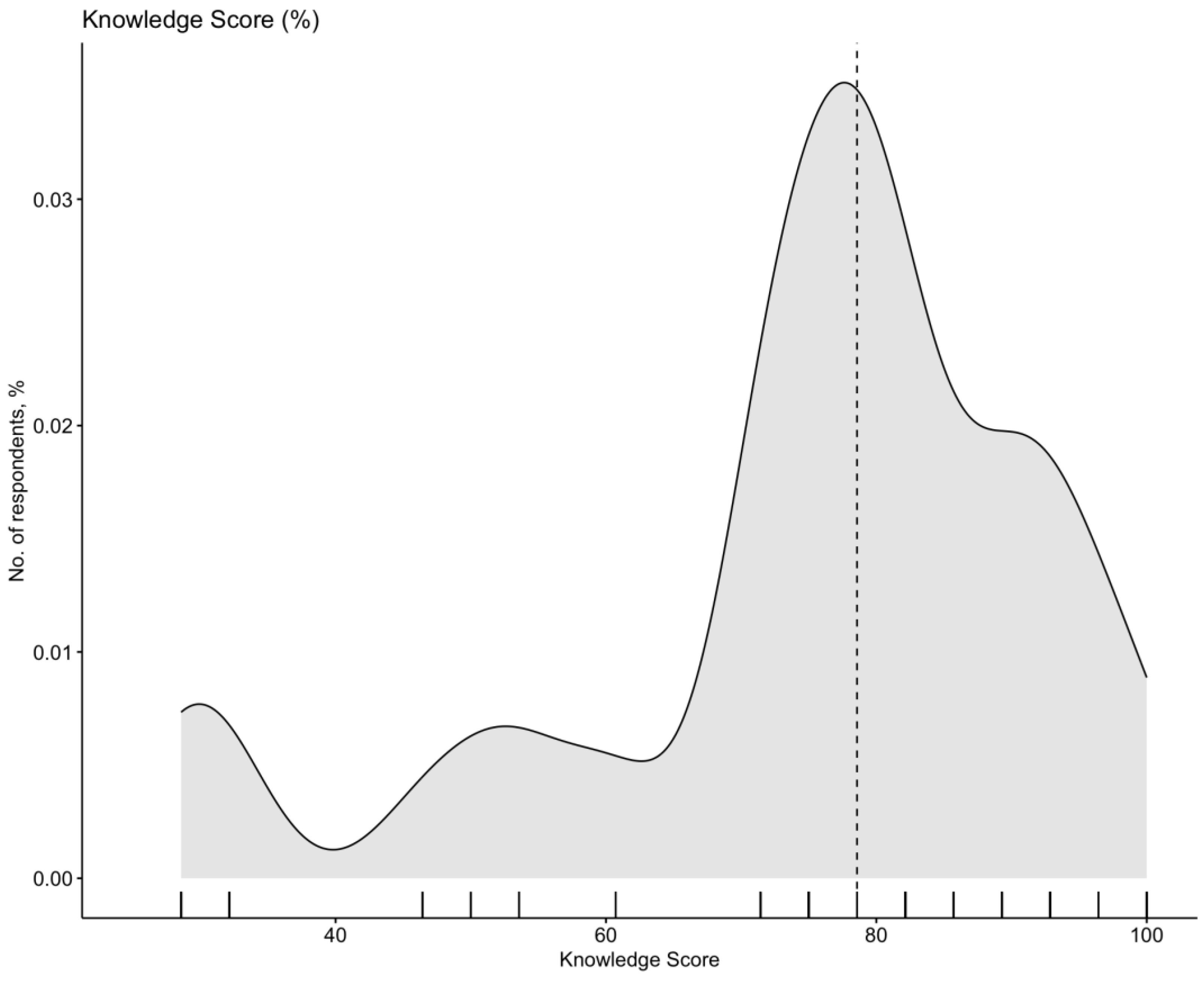
2.2. Assessment of Knowledge Status
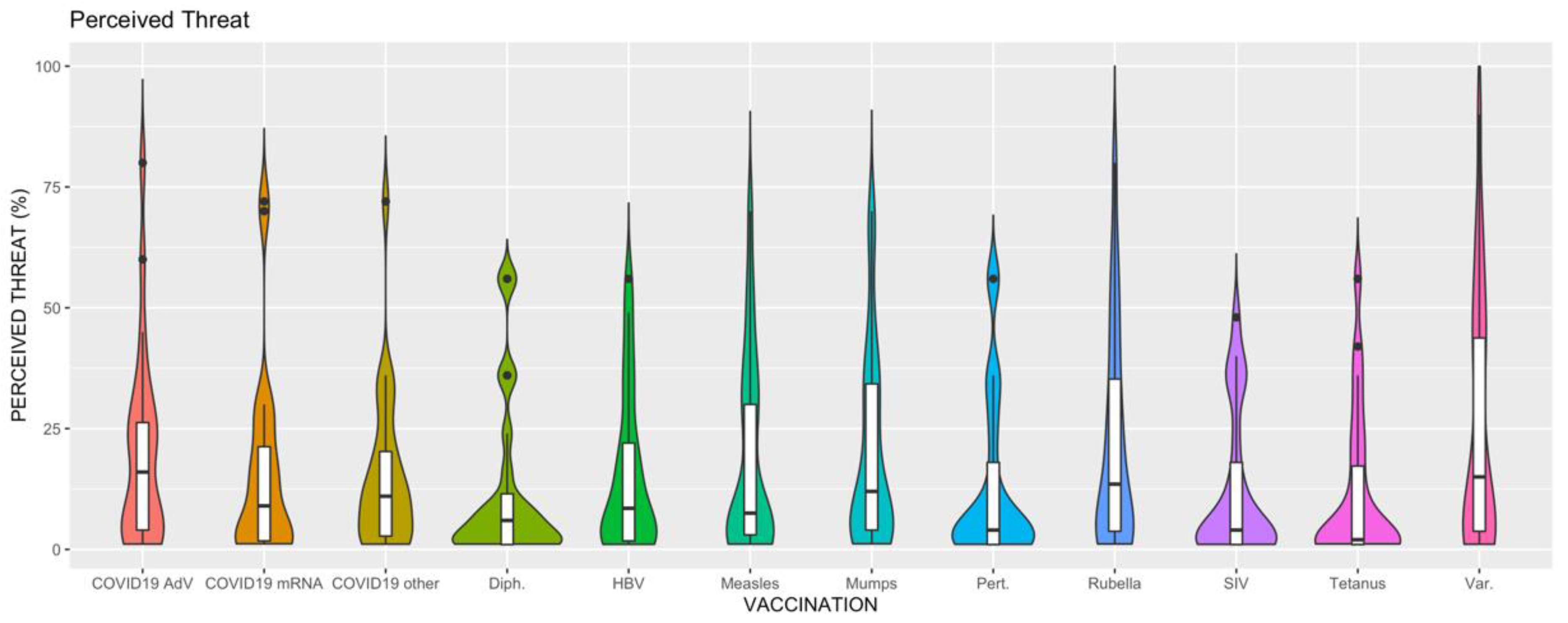
2.3. Risk Perception
2.4. Attitudes towards Vaccination
2.5. Univariate Analysis
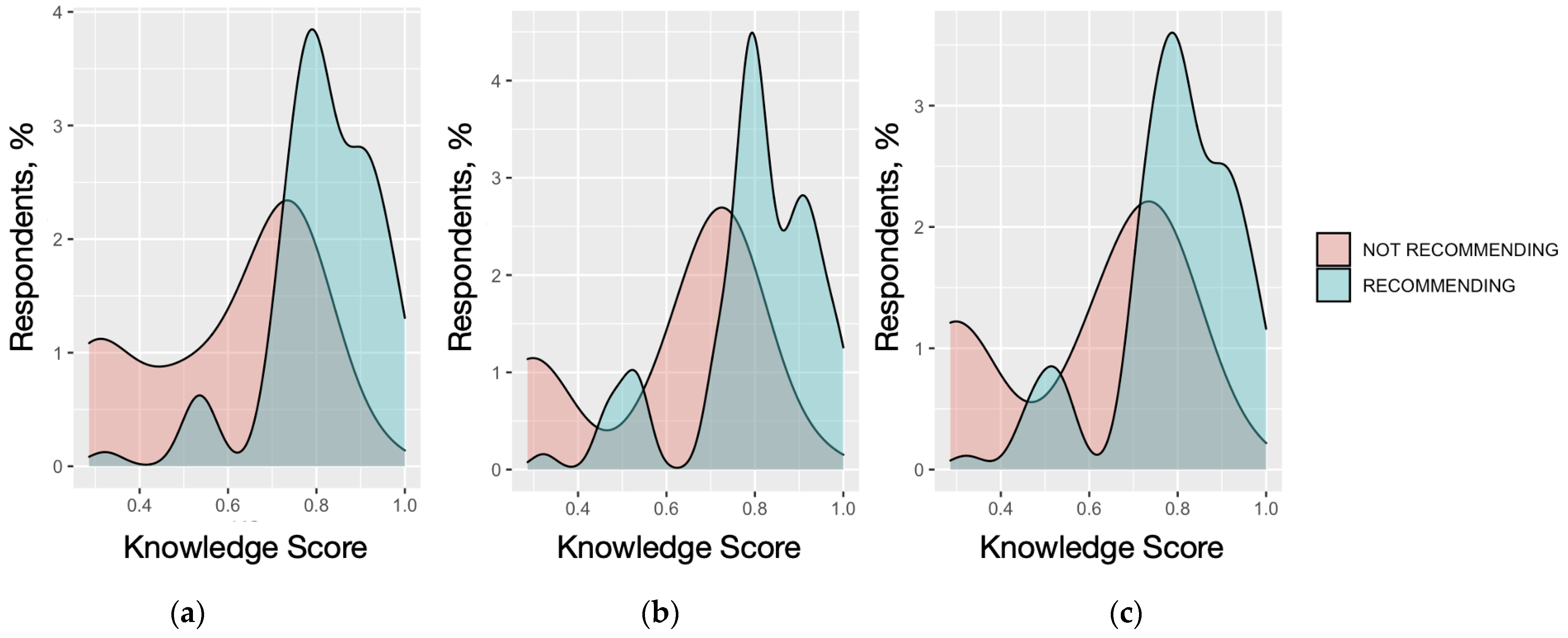
2.6. Multivariable Analysis
- (a)
- Model 1: GKS > median value; having been working as OP in healthcare facilities; having been vaccinated against seasonal influenza; RPS towards SIV and seasonal influenza > median values.
- (b)
- Model 2: being of male gender; GKS > median value; RPS on diphtheria and pertussis > median values; reporting RPS on the vaccine for tetanus > median value.
- (c)
- Model 3: being older than 50 years at the time of the survey; reporting a GKS > median value, having been vaccinated against SARS-CoV-2, reporting RPS values for SARS-CoV-2 vaccines based on mRNA formulates and adenoviral vectors > median.
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Questionnaire and Availability of Data and Material
- Individual characteristics: age, seniority as OPs, gender, and whether they (a) had any professional experience as an occupational physician with any healthcare provider (yes vs. no) and (b) had any child.
- Knowledge test: participants received a 31-item questionnaire on vaccination in pregnancy [29] that was based on previous KAP studies in occupational settings [137,138]. Briefly, the questionnaire included a series of true/false items based on the current understanding and guidelines on vaccinations in pregnancy, specifically focusing on (a) general issues about vaccinations and (b) official recommendations on SARS-CoV-2, SIV, and Tdap. GKS was calculated as the sum of correctly and incorrectly marked recommendations: for all correct answers, +1 was added to a sum score, while a missing/“don’t know” answer or a wrong indication added 0 to the cumulative score.
- Risk perception: participants were initially asked to rate by means of a fully labeled 5-point Likert scale (range: 1, “of no significant concern in daily practice”, to 5, “of very high concern in daily practice”) the perceived severity (C) and the perceived frequency (I) of a series of vaccine-preventable disorders in pregnant women: seasonal influenza, tetanus, diphtheria, pertussis, measles, parotitis, rubella, varicella, hepatitis B, SARS-CoV-2. Similarly, participants were then asked to rate how they perceived a series of vaccinations (i.e., against seasonal flu, tetanus, diphtheria, pertussis, measles, parotitis, rubella, varicella, hepatitis B virus, SARS-CoV-2 delivered as mRNA formulate, adenoviral vector-based formulates, and subunit vaccine) when delivered to pregnant women in terms of the perceived severity (C) and frequency (I) of their side effects.
- 4.
- Attitudes and practices: we initially inquired of participants whether they had previously received any of the following vaccinations: seasonal influenza virus, Tdap or dT, MPR, varicella (either as a single formulate or within an MPR-V vaccine), hepatitis B virus, SARS-CoV-2 (any). Similarly, participants were asked whether, during the last 12 months, they had recommended any of the aforementioned vaccines in women of childbearing age. Finally, we reported a series of potential barriers towards vaccinations in women of childbearing age (i.e., fear of side effects; costs of vaccinations; not being perceived as a priority by other medical professionals; inappropriate risk perception by pregnant women; vaccination services are scarcely available; inappropriate understanding of official recommendations by pregnant women; inappropriate understanding of official recommendations by medical professionals), and participants were asked to rate their perceived significance through a 5-point Likert scale ranging from 1 (not agreeing at all) to 5 (totally agreeing).
4.3. Ethical Approval
4.4. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acronyms | Meaning |
|---|---|
| 95%CI | 95% Confidence Interval |
| aOR | Adjusted Odds Ratio |
| BMI | Body Mass Index |
| COVID-19 | Coronavirus Disease 2019 |
| GKS | General Knowledge Score |
| HAV | Hepatitis A Virus |
| HBV | Hepatitis B Virus |
| HPV | Human Papillomavirus |
| ICOH | International Commission on Occupational Health |
| ISS | Italian National Institute of Health (in Italian, Istituto Superiore di Sanità) |
| KAP | Knowledge, Attitudes, Practices |
| MPR | Measles-Parotitis-Rubella vaccine |
| NHS | National Health Service |
| NIP | (Italian) National Immunization Plan |
| OPs | Occupational Physicians |
| PPE | Personal Protective Equipment |
| RPS | Risk Perception Score |
| RSV | Respiratory Syncytial Virus |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SIV | Seasonal Influenza Virus |
| STROBE | STrengthening the Reporting of Observational studies in Epidemiology |
| Tdap | trivalent formulation tetanus-diphtheria-acellular pertussis |
| VPDs | Vaccine-Preventable Disease |
| Statement | Correct Answer | No./120, % |
|---|---|---|
| Q01. Addictive used in vaccines are not dangerous for human health | TRUE | 80, 66.7% |
| Q02. Multiple sclerosis may be elicited by HBV recombinant vaccine | FALSE | 105, 87.5% |
| Q03. Subacute sclerosing panencephalitis can be elicited by the measles vaccine | FALSE | 81, 67.5% |
| Q04. Encephalitis lethargica can be elicited by vaccines against influenza (in particular, against pandemic influenza) | FALSE | 80, 66.7% |
| Q05. Some vaccinations increase the risk of developing diabetes | FALSE | 100, 83.3% |
| Q06. Some vaccinations increase the risk of developing autoimmune disorders including Hashimoto’s thyroiditis | FALSE | 76, 63.3% |
| Q07. Some vaccinations increase the risk of developing autism (e.g., vaccine against measles) | FALSE | 110, 91.7% |
| Q08. Some vaccinations increase the risk of developing allergies | FALSE | 85, 70.8% |
| Q09. Vaccines are of limited value in controlling infectious diseases as etiological drugs are extensively available | FALSE | 110, 91.7% |
| Q10. Without vaccination programs, smallpox would still exist | TRUE | 115, 95.8% |
| Q11. The efficacy of vaccines has been extensively proven | TRUE | 115, 95.8% |
| Q12. Children would exhibit greater resistance to infectious diseases if they received a more limited number of vaccines | FALSE | 100, 93.3% |
| Q13. A substantial share of vaccines is delivered too early to properly activate the immune system | FALSE | 105, 87.5% |
| Q14. The proper development of the immune system could be impaired by the delivery of a large number of vaccines | FALSE | 85, 70.8% |
| Q15. According to the current National Vaccination Plan, shots with combined vaccine Diphtheria-Tetanus-Pertussis (Tdap) to all pregnant women | TRUE | 65, 54.2% |
| Q16. According to the current National Vaccination Plan, vaccines should be avoided during pregnancy, in general | FALSE | 110, 91.7% |
| Q17. According to the current National Vaccination Plan, live-attenuated vaccines should be avoided during pregnancy | TRUE | 65, 54.2% |
| Q18. According to the current National Vaccination Plan, tetanus vaccination shots should be delivered to all adults every 10 years | TRUE | 110, 91.7% |
| Q19. A vaccine preventing Respiratory Syncytial Virus (RSV) is currently recommended for pregnant women | FALSE | 45, 37.5% |
| Q20. According to the current National Vaccination Plan, seasonal influenza vaccine should be avoided in pregnant women during the third trimester | FALSE | 97, 80.8% |
| Q21. Vaccines against measles, parotitis, and rubella (with and without varicella) can elicit secondary cases with epidemic potential | FALSE | 81, 67.5% |
| Q22. According to our current understanding, mRNA vaccines against SARS-CoV-2 can elicit impairment of fertility | FALSE | 95, 79.2% |
| Q23. According to our current understanding, mRNA vaccines against SARS-CoV-2 should be avoided in women with a previous history of deep vein thrombosis | FALSE | 57, 47.5% |
| Q24. According to the current guidelines, combined delivery of SARS-CoV-2 and Seasonal Influenza vaccines in pregnant women is a potential option. | TRUE | 100, 83.3% |
| Q25. Pregnant women should avoid all occupational settings with a well-defined biological risk. | TRUE | 104, 86.7% |
| Pathogen | RPS (95%CI) | Mean Difference (95%CI) | p Value (ANOVA, Dunnet’s Post Hoc Test) |
|---|---|---|---|
| Seasonal influenza Virus | 45.29 (39.59 to 50.99) | REFERENCE | REFERENCE |
| Tetanus | 26.58 (23.37 to 31.80) | 18.71 (9.31 to 28.11) | <0.001 |
| Diphtheria | 27.58 (23.37 to 31.80) | 17.71 (8.31 to 27.11) | <0.001 |
| Pertussis | 37.79 (32.69 to 42.89) | 7.50 (−1.90 to 16.90) | 0.185 |
| Measles | 41.00 (36.25 to 45.75) | 4.29 (−5.11 to 13.69) | 0.774 |
| Parotitis | 40.75 (35.78 to 45.72) | 4.54 (−4.86 to 13.94) | 0.722 |
| Rubella | 50.33 (45.50 to 55.16) | −5.04 (−14.44 to 4.36) | 0.614 |
| Varicella | 49.42 (44.42 to 54.41) | −4.13 (−13.52 to 5.27) | 0.806 |
| Hepatitis B | 35.08 (31.11 to 39.06) | 10.21 (0.81 to 19.61) | 0.026 |
| SARS-CoV-2 | 52.71 (46.76 to 58.65) | −7.42 (−16.81 to 1.98) | 0.195 |
| Pathogen | RPS (95%CI) | Mean Difference (95%CI) | p Value (ANOVA, Dunnet’s Post Hoc Test) |
|---|---|---|---|
| Seasonal Influenza Vaccine | 12.13 (9.42 to 14.83) | REFERENCE | REFERENCE |
| Tetanus | 11.38 (8.61 to 14.14) | 0.75 (−5.94 to 7.44) | 0.999 |
| Diphtheria | 12.13 (9.12 to 15.13) | 0.00 (−6.69 to 6.69) | 1.000 |
| Pertussis | 12.96 (9.88 to 16.03) | −0.83 (−7.53 to 5.86) | 0.999 |
| Measles | 18.44 (14.85 to 22.04) | −6.32 (−13.01 to 0.38) | 0.075 |
| Parotitis | 19.52 (15.89 to 23.14) | −7.39 (−14.09 to −0.70) | 0.022 |
| Rubella | 21.79 (17.75 to 25.83) | −9.67 (−16.36 to 2.97) | 0.001 |
| Varicella | 25.46 (20.81 to 30.11) | −13.33 (−20.03 to −6.64) | <0.001 |
| Hepatitis B | 15.29 (12.35 to 18.23) | −3.17 (−9.86 to 3.53) | 0.775 |
| SARS-CoV-2 | |||
| mRNA | 15.67 (12.16 to 19.18) | −3.54 (−10.24 to 3.15) | 0.660 |
| Adenoviral carrier | 19.92 (16.34 to 23.50) | −7.79 (−14.49 to −1.10) | 0.013 |
| Subunit vaccine | 15.17 (12.25 to 18.08) | −3.04 (−9.74 to 3.65) | 0.811 |
| RPS (Disease) vs. GKS | RPS (Vaccination) vs. RPS (Disease) | RPS (Vaccination) vs. GKS | |
|---|---|---|---|
| Seasonal Influenza Virus | r = 0.341 p < 0.001 | r = −0.157 p = 0.088 | r = −0.352 p < 0.001 |
| Diphtheria | r = 0.072 p = 0.473 | r = 0.008 p = 0.931 | r = −0.450 p < 0.001 |
| Tetanus | r = 0.041 p = 0.655 | r = −0.136 p = 0.139 | r = −0.367 p < 0.001 |
| Pertussis | r = 0.200 p = 0.028 | r = 0.152 p = 0.097 | r = −0.379 p < 0.001 |
| Measles | r = 0.356 p < 0.001 | r = 0.121 p = 0.186 | r = −0.061 p = 0.509 |
| Parotitis | r = 0.237 p = 0.009 | r = 0.146 p = 0.111 | r = −0.079 p = 0.391 |
| Rubella | r = 0.177 p = 0.053 | r = 0.208 p = 0.022 | r = −0.056 p = 0.541 |
| Varicella | r = 0.196 p = 0.032 | r = 0.135 p = 0.141 | r = −0.010 p = 0.918 |
| Hepatitis B Virus | r = 0.406 p < 0.001 | r = 0.164 p = 0.074 | r = −0.191 p = 0.037 |
| SARS-CoV-2 | r = 0.428 p < 0.001 | - | - |
| mRNA vaccine | - | r = −0.054 p = 0.558 | r = −0.354 p < 0.001 |
| Adenoviral-based vaccines | - | r = 0.239 p = 0.009 | r = −0.294 p = 0.001 |
| Subunit | - | r = 0.155 p = 0.091 | r = −0.314 p < 0.001 |
| Model I | Model 2 | Model 3 | |
|---|---|---|---|
| Male Gender | Not included | Included | Not included |
| Age ≥ 50 years | Not included | Not included | Included |
| Any Child in the household | Not included | Not Included | Not included |
| Higher Knowledge status | Included | Included | Included |
| Working as Occupational Physician for Healthcare facilities | Included | Not included | Not included |
| Vaccinated (SIV) | Included | - | - |
| Vaccinated (Tdap) | - | Not included | - |
| Vaccinated (SARS-CoV-2) | - | - | Included |
| Higher RPS vs. seasonal influenza | Included | - | - |
| Higher RPS vs. diphtheria | - | Included | - |
| Higher RPS vs. tetanus | - | Not included | - |
| Higher RPS vs. pertussis | - | Included | - |
| Higher RPS vs. SARS-CoV-2 | - | - | Not included |
| Higher RPS vs. SIV | Included | - | - |
| Higher RPS vs. diphtheria vaccine | - | Not included | - |
| Higher RPS vs. tetanus vaccine | - | Included | - |
| Higher RPS vs. pertussis vaccine | - | Not included | - |
| Higher RPS vs. SARS-CoV-2 vaccine (mRNA) | - | - | Included |
| Higher RPS vs. SARS-CoV-2 vaccine (adenoviral carrier) | - | - | Included |
| Higher RPS vs. SARS-CoV-2 vaccine (subunit) | - | - | Not Included |
References
- Betsch, C.; Wicker, S. Personal Attitudes and Misconceptions, Not Official Recommendations Guide Occupational Physicians’ Vaccination Decisions. Vaccine 2014, 32, 4478–4484. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes, Beliefs and Practices of Occupational Physicians towards Vaccinations of Health Care Workers: A Cross Sectional Pilot Study in North-Eastern Italy. Int. J. Occup. Med. Environ. Health 2017, 30, 775–790. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Beck, F.; Legleye, S.; L’Haridon, O.; Ward, J. A Future Vaccination Campaign against COVID-19 at Risk of Vaccine Hesitancy and Politicisation. Lancet 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Verger, P.; Dubé, E. Restoring Confidence in Vaccines in the COVID-19 Era. Expert Rev. Vaccines 2020, 19, 991–993. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of Healthcare Workers towards COVID-19 Vaccination: A Survey in France and French-Speaking Parts of Belgium and Canada, 2020. Euro Surveill. 2021, 26, 2002047. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Gualerzi, G.; Ranzieri, S.; Ferraro, P.; Bragazzi, N.L. Knowledge, Attitudes, Practices (KAP) of Italian Occupational Physicians towards Tick Borne Encephalitis. Trop. Med. Infect. Dis. 2020, 5, 117. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Mandate or Not Mandate: Knowledge, Attitudes, and Practices of Italian Occupational Physicians towards SARS-CoV-2 Immunization at the Beginning of Vaccination Campaign. Vaccines 2021, 9, 889. [Google Scholar] [CrossRef]
- Accurti, V.; Gambitta, B.; Iodice, S.; Manenti, A.; Boito, S.; Dapporto, F.; Leonardi, M.; Molesti, E.; Fabietti, I.; Montomoli, E.; et al. SARS-CoV-2 Seroconversion and Pregnancy Outcomes in a Population of Pregnant Women Recruited in Milan, Italy, between April 2020 and October 2020. Int. J. Environ. Res. Public Health 2022, 19, 16720. [Google Scholar] [CrossRef]
- Gabutti, G.; Cetin, I.; Conversano, M.; Costantino, C.; Durando, P.; Giuffrida, S. Experts’ Opinion for Improving Pertussis Vaccination Rates in Adolescents and Adults: A Call to Action. Int. J. Environ. Res. Public Health 2022, 19, 4412. [Google Scholar] [CrossRef]
- van Beukering, M.D.M.; Schuster, H.J.; Peelen, M.J.C.S.; Schonewille, M.E.A.; Hajenius, P.J.; Duijnhoven, R.G.; Brand, T.; Painter, R.C.; Kok, M. Working Conditions in Low Risk Nulliparous Women in The Netherlands: Are Legislation and Guidelines a Guarantee for a Healthy Working Environment? A Cohort Study. Int. Arch. Occup. Environ. Health 2022, 95, 1305–1315. [Google Scholar] [CrossRef]
- Esté, J.; Cabrera-rodrí, R. Zika Virus Pathogenesis: A Battle for Immune Evasion. Vaccines 2021, 9, 294. [Google Scholar]
- Loconsole, D.; Metallo, A.; De Robertis, A.L.; Morea, A.; Quarto, M.; Chironna, M. Seroprevalence of Dengue Virus, West Nile Virus, Chikungunya Virus, and Zika Virus in International Travelers Attending a Travel and Migration Center in 2015–2017, Southern Italy. Vector Borne Zoonotic Dis. 2018, 18, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.M.; Santos, N.C.; Martins, I.C. Dengue and Zika Viruses: Epidemiological History, Potential Therapies, and Promising Vaccines. Trop. Med. Infect. Dis. 2020, 5, 150. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, L.; Antinolfi, F.; Malacarne, F.; Cocconi, R.; Brusaferro, S. A Wide Range of Strategies to Cope with Healthcare Workers’ Vaccine Hesitancy in A North-Eastern Italian Region: Are They Enough? Healthcare 2020, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Maggiore, U.L.R.; Scala, C.; Toletone, A.; Debarbieri, N.; Perria, M.; D’Amico, B.; Montecucco, A.; Martini, M.; Dini, G.; Durando, P. Susceptibility to Vaccine-Preventable Diseases and Vaccination Adherence among Healthcare Workers in Italy: A Cross-Sectional Survey at a Regional Acute-Care University Hospital and a Systematic Review. Hum. Vaccin. Immunother. 2017, 13, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M. Covid-19 Vaccine Acceptance, Hesitancy, and Refusal among Canadian Healthcare Workers: A Multicenter Survey. Am. J. Infect. Control. 2021; in press. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Ledda, C.; Rapisarda, V.; Theodoridou, M. Vaccination of Healthcare Workers: Is Mandatory Vaccination Needed? Expert Rev. Vaccines 2019, 18, 5–13. [Google Scholar] [CrossRef]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza Vaccination in Healthcare Workers: A Comprehensive Critical Appraisal of the Literature. Hum. Vaccin. Immunother. 2018, 14, 772–789. [Google Scholar] [CrossRef]
- Chodick, G.; Ashkenazi, S.; Livni, G.; Lerman, Y. Cost-Effectiveness of Varicella Vaccination of Healthcare Workers. Vaccine 2005, 23, 5064–5072. [Google Scholar] [CrossRef]
- Loulergue, P.; Moulin, F.; Vidal-Trecan, G.; Absi, Z.; Demontpion, C.; Menager, C.; Gorodetsky, M.; Gendrel, D.; Guillevin, L.; Launay, O. Knowledge, Attitudes and Vaccination Coverage of Healthcare Workers Regarding Occupational Vaccinations. Vaccine 2009, 27, 4240–4243. [Google Scholar] [CrossRef]
- Marshall, H.; McMillan, M.; Andrews, R.M.; Macartney, K.; Edwards, K. Vaccines in Pregnancy: The Dual Benefit for Pregnant Women and Infants. Hum. Vaccin. Immunother. 2016, 12, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, B.M. Recommended Vaccines Underused During Pregnancy. J. Am. Med. Assoc. 2019, 320, 1949. [Google Scholar] [CrossRef] [PubMed]
- Fortner, K.B.; Nieuwoudt, C.; Reeder, C.F.; Swamy, G.K. Infections in Pregnancy and the Role of Vaccines. Obstet. Gynecol. Clin. N. Am. 2018, 45, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Gall, S.A. Vaccines for Pertussis and Influenza: Recommendations for Use in Pregnancy. Clin. Obstet. Gynecol. 2008, 51, 486–497. [Google Scholar] [CrossRef]
- Bonville, C.A.; Cibula, D.A.; Domachowske, J.B.; Suryadevara, M. Vaccine Attitudes and Practices among Obstetric Providers in New York State Following the Recommendation for Pertussis Vaccination during Pregnancy. Hum. Vaccin. Immunother. 2015, 11, 713–718. [Google Scholar] [CrossRef]
- Naleway, A.L.; Smith, W.J.; Mullooly, J.P. Delivering Influenza Vaccine to Pregnant Women. Epidemiol. Rev. 2006, 28, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, E.O.; Vazquez-Benitez, G.; Lipkind, H.S.; Klein, N.P.; Cheetham, T.C.; Naleway, A.L.; Lee, G.M.; Hambidge, S.; Jackson, M.L.; Omer, S.B.; et al. Maternal Tdap Vaccination: Coverage and Acute Safety Outcomes in the Vaccine Safety Datalink, 2007–2013. Vaccine 2016, 34, 968–973. [Google Scholar] [CrossRef]
- DeSilva, M.; Vazquez-Benitez, G.; Nordin, J.D.; Lipkind, H.S.; Klein, N.P.; Cheetham, T.C.; Naleway, A.L.; Hambidge, S.J.; Lee, G.M.; Jackson, M.L.; et al. Maternal Tdap Vaccination and Risk of Infant Morbidity. Vaccine 2017, 35, 3655–3660. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Balzarini, F.; Capozzi, V.A.; Volpi, L. Knowledge, Attitudes, Beliefs and Practices of Obstetrics-Gynecologists on Seasonal Influenza and Pertussis Immunizations in Pregnant Women: Preliminary Results from North-Western Italy. Minerva Ginecol. 2019, 71, 288–297. [Google Scholar] [CrossRef]
- Bonanni, P.; Ferrero, A.; Guerra, R.; Iannazzo, S.; Odone, A.; Pompa, M.; Rizzuto, E.; Signorelli, C. Vaccine Coverage in Italy and Assessment of the 2012–2014 National Immunization Prevention Plan. Epidemiol. Prev. 2015, 39, 146–158. [Google Scholar] [CrossRef]
- Signorelli, C.; Guerra, R.; Siliquini, R.; Ricciardi, W. Italy’s Response to Vaccine Hesitancy: An Innovative and Cost Effective National Immunization Plan Based on Scientific Evidence. Vaccine 2017, 35, 4057–4059. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, F.; Napolitano, P.; Angelillo, I.F. Seasonal Influenza Vaccination in Pregnant Women: Knowledge, Attitudes, and Behaviors in Italy. BMC Infect. Dis. 2017, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, A.; Napolitano, F.; D’Ambrosio, A.; Angelillo, I.F. Vaccination Knowledge and Acceptability among Pregnant Women in Italy. Hum. Vaccin. Immunother. 2018, 14, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Principi, N. Prevention of Pertussis: An Unresolved Problem. Hum. Vaccin. Immunother. 2018, 14, 2452–2459. [Google Scholar] [CrossRef]
- Meregaglia, M.; Ferrara, L.; Melegaro, A.; Demicheli, V. Parent “Cocoon” Immunization to Prevent Pertussis-Related Hospitalization in Infants: The Case of Piemonte in Italy. Vaccine 2013, 31, 1135–1137. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Bragazzi, N.L.; Balzarini, F. Pertussis Immunization in Healthcare Workers Working in Pediatric Settings: Knowledge, Attitudes and Practices (KAP) of Occupational Physicians. Prelim. Results A Web-Based Surv. 2020, 61, E66–E75. [Google Scholar]
- Durando, P.; Dini, G.; Massa, E.; La Torre, G. Tackling Biological Risk in the Workplace: Updates and Prospects Regarding Vaccinations for Subjects at Risk of Occupational Exposure in Italy. Vaccines 2019, 7, 141. [Google Scholar] [CrossRef]
- Esposito, S.; Durando, P.; Bosis, S.; Ansaldi, F.; Tagliabue, C.; Icardi, G. Vaccine-Preventable Diseases: From Paediatric to Adult Targets. Eur. J. Intern. Med. 2014, 25, 203–212. [Google Scholar] [CrossRef]
- Manzoli, L.; Sotgiu, G.; Magnavita, N.; Durando, P.; Barchitta, M.; Carducci, A.; Conversano, M.; De Pasquale, G.; Dini, G.; Firenze, A.; et al. Evidence-Based Approach for Continuous Improvement of Occupational Health. Epidemiol. Prev. 2015, 39, 81–85. [Google Scholar]
- Ding, H.; Black, C.L.; Ball, S.; Fink, R.V.; Williams, W.W.; Fiebelkorn, A.P.; Lu, P.-J.; Kahn, K.E.; D’Angelo, D.V.; Devlin, R.; et al. Influenza Vaccination Coverage Among Pregnant Women—United States, 2016–2017 Influenza Season. Morb. Mortal. Wkly. Rep. 2017, 66, 1016–1022. [Google Scholar] [CrossRef]
- Sukumaran, L.; McCarthy, N.L.; Kharbanda, E.O.; Weintraub, E.S.; Vazquez-Benitez, G.; McNeil, M.M.; Li, R.; Klein, N.P.; Hambidge, S.J.; Naleway, A.L.; et al. Safety of Tetanus, Diphtheria, and Acellular Pertussis and Influenza Vaccinations in Pregnancy. Obstet. Gynecol. 2016, 48, 923–930. [Google Scholar] [CrossRef]
- Regan, A.K.; Tracey, L.E.; Blyth, C.C.; Richmond, P.C.; Effler, P.V. A Prospective Cohort Study Assessing the Reactogenicity of Pertussis and Influenza Vaccines Administered during Pregnancy. Vaccine 2016, 34, 2299–2304. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G.; Grinceviciene, S.; Haldre, K.; Lonnee-Hoffmann, R.; Donders, F.; Tsiakalos, A.; Adriaanse, A.; de Oliveira, J.M.; Ault, K.; Mendling, W. Isidog Consensus Guidelines on Covid-19 Vaccination for Women before, during and after Pregnancy. J. Clin. Med. 2021, 10, 2902. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Safety and Effectiveness of COVID-19 Vaccination during Pregnancy. 2022, CDC, Atlanta, USA. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/pregnancy.html (accessed on 3 May 2023).
- Giusti, A.; Zambri, F.; Marchetti, F.; Corsi, E.; Preziosi, J.; Sampaolo, L. Interim Guidance on Pregnancy, Childbirth, Breastfeeding and Care of Infants (0–2 Years) in Response to the COVID-19 Emergency. 2021 Italian National Health Institute (ISS), Rome. Available online: https://www.iss.it/documents/5430402/0/Rapporto+ISS+COVID-19+2_2021_EN.pdf/421a0bc6-1933-aa77-6b39-a7860d866a16?t=1615472502820 (accessed on 3 May 2023).
- Falato, R.; Ricciardi, S.; Franco, G. Influenza Risk Perception and Vaccination Attitude in Medical and Nursing Students during the Vaccination Campaigns of 2007/2008 (Seasonal Influenza) and 2009/2010 (H1N1 Influenza). Med. Lav. 2011, 102, 208–215. [Google Scholar] [PubMed]
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare 2017, 5, 13. [Google Scholar] [CrossRef]
- Graves, M.C.; Harris, J.R.; Kohn, M.; Hannon, P.A.; Lichiello, P.A.; Martin, D.P. Employers’ Views on Influenza and Tetanus-Diphtheria-Pertussis Vaccination in the Workplace. J. Occup. Environ. Med. 2016, 58, e157–e158. [Google Scholar] [CrossRef]
- Dubé, E.; MacDonald, N.E. How Can a Global Pandemic Affect Vaccine Hesitancy? Expert Rev. Vaccines 2020, 19, 899–901. [Google Scholar] [CrossRef]
- Bloom, B.R.; Marcuse, E.; Mnookin, S. Addressing Vaccine Hesitancy. Science 2014, 344, 339. [Google Scholar] [CrossRef]
- Goldstein, S.; MacDonald, N.E.; Guirguis, S.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Larson, H.; Manzo, M.L.; et al. Health Communication and Vaccine Hesitancy. Vaccine 2015, 33, 4212–4214. [Google Scholar] [CrossRef]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to Vaccination: A Critical Review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes, Beliefs and Practices of Occupational Physicians towards Seasonal Influenza Vaccination: A Cross-Sectional Study from North-Eastern Italy. J. Prev. Med. Hyg. 2017, 58, E141–E154. [Google Scholar] [PubMed]
- Dorribo, V.; Lazor-Blanchet, C.; Hugli, O.; Zanetti, G. Health Care Workers’ Influenza Vaccination: Motivations and Mandatory Mask Policy. Occup. Med. (Chic. Ill.) 2015, 65, 739–745. [Google Scholar] [CrossRef]
- Riphagen-Dalhuisen, J.; Gefenaite, G.; Hak, E. Predictors of Seasonal Influenza Vaccination among Healthcare Workers in Hospitals: A Descriptive Meta-Analysis. Occup. Environ. Med. 2012, 69, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Gargalianos, P.; Nikolaidis, P.; Katerelos, P.; Tedoma, N.; Maltezos, E.; Lazanas, M. Attitudes towards Mandatory Vaccination and Vaccination Coverage against Vaccine-Preventable Diseases among Health-Care Workers in Tertiary-Care Hospitals. J. Infect. 2012, 64, 319–324. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Wicker, S.; Borg, M.; Heininger, U.; Puro, V.; Theodoridou, M.; Poland, G.A. Vaccination Policies for Health-Care Workers in Acute Health-Care Facilities in Europe. Vaccine 2011, 29, 9557–9562. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Botelho-Nevers, E.; Brantsæter, A.B.; Carlsson, R.M.; Heininger, U.; Hübschen, J.M.; Josefsdottir, K.S.; Kassianos, G.; Kyncl, J.; Ledda, C.; et al. Vaccination of Healthcare Personnel in Europe: Update to Current Policies. Vaccine 2019, 37, 7576–7584. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop. Med. Infect. Dis. 2022, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Morrone, T.; Napolitano, F.; Albano, L.; Di, G. Meningococcal Serogroup B Vaccine: Knowledge and Acceptability among Parents in Italy Meningococcal Serogroup B Vaccine: Knowledge and Acceptability among Parents in Italy. Hum. Vaccines Immunother. 2017, 3, 1921–1927. [Google Scholar] [CrossRef]
- Eppes, C.; Wu, A.; Cameron, K.A.; Garcia, P.; Grobman, W. Does Obstetrician Knowledge Regarding Influenza Increase HINI Vaccine Acceptance among Their Pregnant Patients? Vaccine 2012, 30, 5782–5784. [Google Scholar] [CrossRef]
- Bert, F.; Olivero, E.; Rossello, P.; Gualano, M.R.; Castaldi, S.; Damiani, G.; D’Errico, M.M.; di Giovanni, P.; Fantini, M.P.; Fabiani, L.; et al. Knowledge and Beliefs on Vaccines among a Sample of Italian Pregnant Women: Results from the NAVIDAD Study. Eur. J. Public Health 2019, 30, 286–292. [Google Scholar] [CrossRef]
- Loubet, P.; Kernéis, S.; Groh, M.; Loulergue, P.; Blanche, P.; Verger, P.; Launay, O. Attitude, Knowledge and Factors Associated with Influenza and Pneumococcal Vaccine Uptake in a Large Cohort of Patients with Secondary Immune Deficiency. Vaccine 2015, 33, 3703–3708. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Olivero, E.; Voglino, G.; Corezzi, M.; Rossello, P.; Vicentini, C.; Bert, F.; Siliquini, R. Knowledge, Attitudes and Beliefs towards Compulsory Vaccination: A Systematic Review. Hum. Vaccin. Immunother. 2019, 15, 918–931. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; While, A.E.; Norman, I.J. Knowledge and Attitudes Regarding Influenza Vaccination among Nurses: A Research Review. Vaccine 2010, 28, 7207–7214. [Google Scholar] [CrossRef]
- Smith, S.; Sim, J.; Halcomb, E. Nurses’ knowledge, attitudes and practices regarding influenza vaccination: An integrative review. J. Clin. Nurs. 2016, 25, 2730–2744. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Alicandro, G.; Negri, E.; Scarpino, V.; Coggiola, M.; Spatari, G. Attitudes towards COVID-19 Vaccination and Containment Measures in Italy and the Role of Occupational Physicians. Med. Del Lav. 2022, 113, e2022018. [Google Scholar] [CrossRef]
- Bagnasco, A.; Zanini, M.; Catania, G.; Watson, R.; Hayter, M.; Dasso, N.; Dini, G.; Agodi, A.; Pasquarella, C.; Zotti, C.M.; et al. Predicting Needlestick and Sharps Injuries in Nursing Students: Development of the SNNIP Scale. Nurs. Open 2020, 7, 1578–1587. [Google Scholar] [CrossRef] [PubMed]
- Kirupakaran, J.; Meloche, C.; Upfal, M. Practices and Attitudes of Michigan-Based Occupational Physicians Regarding Adult Immunization. J. Occup. Environ. Med. 2018, 60, 1034–1041. [Google Scholar] [CrossRef]
- La Torre, G.; Semyonov, L.; Mannocci, A.; Boccia, A. Knowledge, Attitude, and Behaviour of Public Health Doctors towards Pandemic Influenza Compared to the General Population in Italy. Scand. J. Soc. Med. 2012, 40, 69–75. [Google Scholar] [CrossRef]
- Albano, L.; Matuozzo, A.; Marinelli, P.; di Giuseppe, G. Knowledge, Attitudes and Behaviour of Hospital Health-Care Workers Regarding Influenza A/H1N1: A Cross Sectional Survey. BMC Infect. Dis. 2014, 14, 208. [Google Scholar] [CrossRef]
- Levi, M.; Bonanni, P.; Biffino, M.; Conversano, M.; Corongiu, M.; Morato, P.; Maio, T. Influenza Vaccination 2014–2015: Results of a Survey Conducted among General Practitioners in Italy. Hum. Vaccin. Immunother. 2018, 14, 1342–1350. [Google Scholar] [CrossRef]
- Levi, M.; Sinisgalli, E.; Lorini, C.; Santomauro, F.; Chellini, M.; Bonanni, P. The “Fluad Case” in Italy: Could It Have Been Dealt Differently? Hum. Vaccin. Immunother. 2017, 13, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Bonanni, P.; Boccalini, S.; Zanobini, P.; Dakka, N.; Lorini, C.; Santomauro, F.; Bechini, A. The Appropriateness of the Use of Influenza Vaccines: Recommendations from the Latest Seasons in Italy. Hum. Vaccin. Immunother. 2018, 14, 699–705. [Google Scholar] [CrossRef] [PubMed]
- van Lier, A.; Ferreira, J.A.; Mollema, L.; Sanders, E.A.M.; de Melker, H.E. Intention to Vaccinate Universally against Varicella, Rotavirus Gastroenteritis, Meningococcal B Disease and Seasonal Influenza among Parents in the Netherlands: An Internet Survey. BMC Res. Notes 2017, 10, 672. [Google Scholar] [CrossRef]
- Taddei, C.; Ceccherini, V.; Niccolai, G.; Porchia, B.R.; Boccalini, S.; Levi, M.; Tiscione, E.; Santini, M.G.; Baretti, S.; Bonanni, P.; et al. Attitude toward Immunization and Risk Perception of Measles, Rubella, Mumps, Varicella, and Pertussis in Health Care Workers Working in 6 Hospitals of Florence, Italy 2011. Hum. Vaccin. Immunother. 2014, 10, 2612–2622. [Google Scholar] [CrossRef] [PubMed]
- Fedeli, U.; Zanetti, C.; Saia, B. Susceptibility of Healthcare Workers to Measles, Mumps Rubella and Varicella. J. Hosp. Infect. 2002, 51, 133–135. [Google Scholar] [CrossRef]
- Lambert, N.; Strebel, P.; Orenstein, W.; Icenogle, J.; Poland, G.A. Rubella. Lancet 2015, 385, 2297–2307. [Google Scholar] [CrossRef]
- Schenk, J.; Abrams, S.; Theeten, H.; van Damme, P.; Beutels, P.; Hens, N. Immunogenicity and Persistence of Trivalent Measles, Mumps, and Rubella Vaccines: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2021, 21, 286–295. [Google Scholar] [CrossRef]
- Asma, S.; Akan, H.; Uysal, Y.; Poçan, A.G.; Sucaklı, M.H.; Yengil, E.; Gereklioğlu, Ç.; Korur, A.; Başhan, İ.; Erdogan, A.F.; et al. Factors Effecting Influenza Vaccination Uptake among Health Care Workers: A Multi-Center Cross-Sectional Study. BMC Infect. Dis. 2016, 16, 192. [Google Scholar] [CrossRef]
- Hayward, A.C.; Harling, R.; Wetten, S.; Johnson, A.M.; Munro, S.; Smedley, J.; Murad, S.; Watson, J.M. Effectiveness of an Influenza Vaccine Programme for Care Home Staff to Prevent Death, Morbidity, and Health Service Use among Residents: Cluster Randomised Controlled Trial. BMJ 2006, 333, 1241. [Google Scholar] [CrossRef]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Quantifying the Efficacy of Influenza Vaccines: Authors’ Reply. Lancet Infect. Dis. 2012, 12, 660–661. [Google Scholar] [CrossRef]
- Zhai, Y.; Santibanez, T.A.; Kahn, K.E.; Black, C.L.; de Perio, M.A. Paid Sick Leave Benefits, Influenza Vaccination, and Taking Sick Days Due to Influenza-like Illness among U.S. Workers. Vaccine 2018, 36, 7316–7323. [Google Scholar] [CrossRef] [PubMed]
- Gianino, M.M.; Politano, G.; Scarmozzino, A.; Charrier, L.; Testa, M.; Giacomelli, S.; Benso, A.; Zotti, C.M. Estimation of Sickness Absenteeism among Italian Healthcare Workers during Seasonal Influenza Epidemics. PLoS ONE 2017, 12, e0182510. [Google Scholar] [CrossRef] [PubMed]
- Buchy, P.; Badur, S.; Kassianos, G.; Preiss, S.; Tam, J.S. Vaccinating Pregnant Women against Influenza Needs to Be a Priority for All Countries: An Expert Commentary. Int. J. Infect. Dis. 2020, 92, 1–12. [Google Scholar] [CrossRef]
- Dubé, E.; Gagnon, D.; Kaminsky, K.; Green, C.R.; Ouakki, M.; Bettinger, J.A.; Brousseau, N.; Castillo, E.; Crowcroft, N.S.; Driedger, S.M.; et al. Vaccination Against Influenza in Pregnancy: A Survey of Canadian Maternity Care Providers. J. Obstet. Gynaecol. Can. 2019, 41, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Bert, F.; Voglino, G.; Buttinelli, E.; D’Errico, M.M.; de Waure, C.; di Giovanni, P.; Fantini, M.P.; Giuliani, A.R.; Marranzano, M.; et al. Attitudes towards Compulsory Vaccination in Italy: Results from the NAVIDAD Multicentre Study. Vaccine 2018, 36, 3368–3374. [Google Scholar] [CrossRef]
- Eppes, C.; Wu, A.; You, W.; Cameron, K.A.; Garcia, P.; Grobman, W. Barriers to Influenza Vaccination among Pregnant Women. Vaccine 2013, 31, 2874–2878. [Google Scholar] [CrossRef]
- O’Leary, S.T.; Riley, L.E.; Lindley, M.C.; Allison, M.A.; Crane, L.A.; Hurley, L.P.; Beaty, B.L.; Brtnikova, M.; Collins, M.; Albert, A.P.; et al. Immunization Practices of U.S. Obstetrician/Gynecologists for Pregnant Patients. Am. J. Prev. Med. 2018, 54, 205–213. [Google Scholar] [CrossRef]
- Stark, L.M.; Power, M.L.; Turrentine, M.; Samelson, R.; Siddiqui, M.M.; Paglia, M.J.; Strassberg, E.R.; Kelly, E.; Murtough, K.L.; Schulkin, J. Influenza Vaccination among Pregnant Women: Patient Beliefs and Medical Provider Practices. Infect. Dis. Obstet. Gynecol. 2016, 2016, 3281975. [Google Scholar] [CrossRef]
- Vilca, M.L.; Esposito, S. The Crucial Role of Maternal Care Providers as Vaccinators for Pregnant Women. Vaccine 2017, 36, 5379–5384. [Google Scholar] [CrossRef]
- Willame, C.; Dodd, C.; Durán, C.; Elbers, R.; Gini, R.; Bartolini, C.; Paoletti, O.; Wang, L.; Ehrenstein, V.; Kahlert, J.; et al. Background Rates of 41 Adverse Events of Special Interest for COVID-19 Vaccines in 10 European Healthcare Databases—An ACCESS Cohort Study. Vaccine 2023, 41, 251–262. [Google Scholar] [CrossRef]
- Lee, M.T.; Choi, W.; You, S.H.; Park, S.; Kim, J.Y.; Nam, D.R.; Lee, J.W.; Jung, S.Y. Safety Profiles of MRNA COVID-19 Vaccines Using World Health Organization Global Scale Database (VigiBase): A Latent Class Analysis. Infect. Dis. Ther. 2022, 12, 443–458. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Palamenghi, L.; Graffigna, G. Public Reaction towards the Potential Side Effects of a COVID-19 Vaccine: An Italian Cross-Sectional Study. Vaccines 2022, 10, 429. [Google Scholar] [CrossRef] [PubMed]
- Serrao, A.; Agrippino, R.; Brescini, M.; Mormile, R.; Chistolini, A. Thromboembolic Events Following MRNA Vaccines for COVID 19: A Case Series. J. Thromb. Thrombolysis 2022, 53, 971–973. [Google Scholar] [CrossRef] [PubMed]
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep Vein Thrombosis (DVT) Occurring Shortly after the Second Dose of MRNA SARS-CoV-2 Vaccine. Intern. Emerg. Med. 2021, 16, 803–804. [Google Scholar] [CrossRef]
- Durand, J.; Dogné, J.; Cohet, C.; Browne, K.; Gordillo Maranon, M.; Piccolo, L.; Zaccaria, C.; Genov, G. Safety Monitoring of COVID-19 Vaccines: Perspective from the European Medicines Agency. Clin. Pharmacol. Ther. 2022; Epub Ahead of print. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, Acceptance and Hesitancy among the General Population Worldwide to Receive the COVID-19 Vaccines and Their Contributing Factors: A Systematic Review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef]
- Killian, M.; Detoc, M.; Berthelot, P.; Charles, R.; Gagneux-Brunon, A.; Lucht, F.; Pulcini, C.; Barbois, S.; Botelho-Nevers, E. Vaccine Hesitancy among General Practitioners: Evaluation and Comparison of Their Immunisation Practice for Themselves, Their Patients and Their Children. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1837–1843. [Google Scholar] [CrossRef]
- Mesch, G.S.; Schwirian, K.P. Social and Political Determinants of Vaccine Hesitancy: Lessons Learned from the H1N1 Pandemic of 2009–2010. Am. J. Infect. Control. 2015, 43, 1161–1165. [Google Scholar] [CrossRef]
- Moore, P.J.A.; Millar, B.C.; Moore, J.E. Meningococcal ACWY Vaccine Uptake and Awareness among Student Freshers Enrolled at Northern Ireland Universities. Int. J. Adolesc. Med. Health 2017, 32, 20160087. [Google Scholar] [CrossRef]
- Richmond, P.; Hatchuel, L.; Dong, M.; Ma, B.; Hu, B.; Smolenov, I.; Li, P.; Liang, P.; Han, H.H.; Liang, J.; et al. Safety and Immunogenicity of S-Trimer (SCB-2019), a Protein Subunit Vaccine Candidate for COVID-19 in Healthy Adults: A Phase 1, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2021, 397, 682–694. [Google Scholar] [CrossRef]
- AIFA (Italian Medicine Agency) Rapporto Sulla Sorveglianza Dei Vaccini Anti-COVID-19, N.13; AIFA, Rome. 2022. Available online: https://www.aifa.gov.it/web/guest/rapporti-su-sorveglianza-dei-vaccini-covid-19?p_p_id=it_gov_aifa_portlet_GestioneCookies&p_p_lifecycle=1&p_p_state=normal&p_p_mode=view&_it_gov_aifa_portlet_GestioneCookies_javax.portlet.action=saveCookieAIFA (accessed on 1 March 2023).
- He, Q.; Wang, G.; He, J.; Wang, Y.; Zhang, J.; Luo, B.; Chen, P.; Luo, X.; Ren, J. Knowledge, Attitude and Practice Regarding Occupational Protection against COVID-19 among Midwives in China: A Nationwide Cross-Sectional Study. Int. J. Disaster Risk Reduct. 2022, 79, 103184. [Google Scholar] [CrossRef] [PubMed]
- Tasnim, H.; Amin, M.B.; Roy, N.; Aktarujjaman, M.; Rogers, B.T.; Rosby, R.; Hossain, E. Knowledge, Attitudes, and Practices towards COVID-19 among Pregnant Women in Northern Bangladesh: A Community-Based Cross-Sectional Study. Behav. Sci. 2022, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, F.; Navaro, M.; Vezzosi, L.; Santagati, G.; Angelillo, I.F. Primary Care Pediatricians’ Attitudes and Practice towards Hpv Vaccination: A Nationwide Survey in Italy. PLoS ONE 2018, 13, e0194920. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, G.; Pelullo, C.P.; della Polla, G.; Montemurro, M.V.; Napolitano, F.; Pavia, M.; Angelillo, I.F. Surveying Willingness towards SARS-CoV-2 Vaccination of Healthcare Workers in Italy. Expert Rev. Vaccines 2021, 20, 881–889. [Google Scholar] [CrossRef]
- Riccò, M.; Cerviere, M.P.; Marchesi, F.; Bottazzoli, M. Invasive Meningococcal Disease and Meningococcal Serogroup B Vaccination in Adults and Their Offspring: Knowledge, Attitudes, and Practices in Italy (2019). Vaccines 2023, 11, 508. [Google Scholar] [CrossRef]
- Heiervang, E.; Goodman, R. Advantages and Limitations of Web-Based Surveys: Evidence from a Child Mental Health Survey. Soc. Psychiat. Epidemiol. 2011, 46, 69–76. [Google Scholar] [CrossRef]
- Huang, Y.; Xu, S.; Lei, W.; Zhao, Y.; Liu, H.; Yao, D.; Xu, Y.; Lv, Q.; Hao, G.; Xu, Y.; et al. Knowledge, Attitudes, and Practices Regarding Zika: Paper and Internet Based Survey in Zhejiang, China. JMIR Public Health Surveill. 2017, 3, e81. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Hantaviruses in Agricultural and Forestry Workers: Knowledge, Attitudes and Practices in Italian Physicians. Trop. Med. Infect. Dis. 2021, 6, 169. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Camisa, V.; di Palma, P.; Minutolo, G.; Ranzieri, S.; Zaffina, S.; Baldassarre, A.; Restivo, V. Managing of Migraine in the Workplaces: Knowledge, Attitudes and Practices of Italian Occupational Physicians. Medicina (B Aires) 2022, 58, 686. [Google Scholar] [CrossRef]
- Maietti, E.; Reno, C.; Sanmarchi, F.; Montalti, M.; Fantini, M.P.; Gori, D. Are psychological status and trust in information related to vaccine hesitancy during COVID-19 pandemic? A latent class and mediation analyses in Italy. Hum. Vaccin. Immunother. 2022, 18, 2157622. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Balzarini, F. Challenges Faced by the Italian Medical Workforce. Lancet 2020, 395, e55–e56. [Google Scholar] [CrossRef] [PubMed]
- Vicarelli, G.; Pavolini, E. Health Workforce Governance in Italy. Health Policy 2015, 119, 1606–1612. [Google Scholar] [CrossRef] [PubMed]
- Hayat, A.M.; Tribble, D.R.; Sanders, J.W.; Faix, D.J.; Shiau, D.; Armstrong, A.W.; Riddle, M.S. Knowledge, Attitudes, and Practice of Travelers’ Diarrhea Management among Frontline Providers. J. Travel Med. 2011, 18, 310–317. [Google Scholar] [CrossRef]
- Çiftci, F.; Şen, E.; Demir, N.; Çiftci, O.; Erol, S.; Kayacan, O. Beliefs, Attitudes, and Activities of Healthcare Personnel about Influenza and Pneumococcal Vaccines. Hum. Vaccin. Immunother. 2018, 14, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Ranzieri, S. Respiratory Syncytial Virus: Knowledge, Attitudes and Beliefs of General Practitioners from North-Eastern Italy (2021). Pediatr. Rep. 2022, 14, 147–165. [Google Scholar] [CrossRef]
- Zingg, A.; Siegrist, M. Measuring People’s Knowledge about Vaccination: Developing a One-Dimensional Scale. Vaccine 2012, 30, 3771–3777. [Google Scholar] [CrossRef]
- Baraldi, E.; Checcucci Lisi, G.; Costantino, C.; Heinrichs, J.H.; Manzoni, P.; Riccò, M.; Roberts, M.; Vassilouthis, N. RSV Disease in Infants and Young Children: Can We See a Brighter Future? Hum. Vaccin. Immunother. 2022, 18, 2079322. [Google Scholar] [CrossRef]
- Cuadera, M.K.Q.; Mader, E.M.; Safi, A.G.; Harrington, L.C. Knowledge, attitudes, and practices for tick bite prevention and tick control among residents of Long Island, New York, USA. Ticks Tick Borne Dis. 2023, 14, 102124. [Google Scholar] [CrossRef]
- Coyer, L.; Sogan-Ekinci, A.; Greutélaers, B.; Kuhn, J.; Saller, F.S.; Hailer, J.; Böhm, S.; Brosch, R.; Wagner-Wiening, C.; Böhmer, M.M. Knowledge, Attitudes and Behaviors regarding Tick-Borne Encephalitis Vaccination and Prevention of Tick-Borne Diseases among Primary Care Physicians in Bavaria and Baden-Wuerttemberg, Germany, May-September 2022. Microorganisms 2023, 11, 961. [Google Scholar] [CrossRef]
- Bocquier, A.; Branchereau, M.; Gauchet, A.; Bonnay, S.; Simon, M.; Ecollan, M.; Chevreul, K.; Mueller, J.E.; Gagneux-Brunon, A.; Thilly, N. PrevHPV Study Group. Promoting HPV vaccination at school: A mixed methods study exploring knowledge, beliefs and attitudes of French school staff. BMC Public Health 2023, 23, 486. [Google Scholar] [CrossRef]
- Marano, C.; Moodley, M.; Melander, E.; de Moerlooze, L.; Nothdurft, H.D. Multinational Survey Shows Low Awareness of Tick-Borne Encephalitis and Rabies among Travellers to Endemic Regions. J. Travel Med. 2018, 26, S1–S2. [Google Scholar] [CrossRef]
- Olson, S.; Hall, A.; Riddle, M.S.; Porter, C.K. Travelers’ Diarrhea: Update on the Incidence, Etiology and Risk in Military and Similar Populations—1990–2005 versus 2005–2015, Does a Decade Make a Difference? Trop. Dis. Travel Med. Vaccines 2019, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.M.; St. Sauver, J.L.; Sia, I.G. Impact of Pre-Travel Consultation on Clinical Management and Outcomes of Travelers’ Diarrhea: A Retrospective Cohort Study. Trop. Dis. Travel Med. Vaccines 2018, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Zaniboni, A.; Satta, E.; Baldassarre, A.; Cerviere, M.P.; Marchesi, F.; Peruzzi, S. Management and Prevention of Traveler’s Diarrhea: A Cross-Sectional Study on Knowledge, Attitudes, and Practices in Italian Occupational Physicians (2019 and 2022). Trop. Med. Infect. Dis. 2022, 7, 370. [Google Scholar] [CrossRef]
- Cafiero-Fonseca, E.T.; Stawasz, A.; Johnson, S.T.; Sato, R.; Bloom, D.E. The Full Benefits of Adult Pneumococcal Vaccination: A Systematic Review. PLoS ONE 2017, 12, e0186903. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Santoro, P.E.; Borrelli, I.; Rossi, M.F.; Amantea, C.; Tumminello, A.; Daniele, A.; Beccia, F.; Moscato, U. Employee Participation in Workplace Vaccination Campaigns: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1898. [Google Scholar] [CrossRef]
- la Torre, G.; de Waure, C.; Chiaradia, G.; Mannocci, A.; Capri, S.; Bamfi, F.; Ricciardi, W. Guidance for Future HTA Applications to Vaccines: The HPV Lesson. Hum. Vaccin. 2011, 7, 900–904. [Google Scholar] [CrossRef]
- de Waure, C.; Quaranta, G.; Ianuale, C.; Panatto, D.; Amicizia, D.; Apprato, L.; Campanella, P.; Colotto, M.; de Meo, C.; di Nardo, F.; et al. Knowledge, Attitudes and Behaviors of the Italian Population towards Neisseria Meningitidis, Streptococcus Pneumoniae and HPV Diseases and Vaccinations: A Cross-Sectional Multicentre Study. Public Health 2016, 141, 136–142. [Google Scholar] [CrossRef]
- Bogani, G.; Raspagliesi, F.; di Donato, V.; Brusadelli, C.; Guerrisi, R.; Pinelli, C.; Casarin, J.; Ghezzi, F.; del Fabro, A.; Ditto, A.; et al. Spotlight on the Role of Human Papillomavirus Vaccines. Gynecol. Oncol. 2021, 160, 346–350. [Google Scholar] [CrossRef]
- Monti, M.; D’aniello, D.; Scopelliti, A.; Tibaldi, V.; Santangelo, G.; Colagiovanni, V.; Giannini, A.; di Donato, V.; Palaia, I.; Perniola, G.; et al. Relationship between Cervical Excisional Treatment for Cervical Intraepithelial Neoplasiaand Obstetrical Outcome. Minerva Obstet. Gynecol. 2021, 73, 233–246. [Google Scholar] [CrossRef]
- Meites, E.; Szilagyi, P.G.; Chesson, H.W.; Unger, E.R.; Romero, J.R.; Markowitz, L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. Morb. Mortal. Wkly. Rev. 2019, 68, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N. Total Worker Health ®: An Emerging Innovation in Workplace Health and Well-Being. ACSM’s Health Fit. J. 2020, 24, 42–44. [Google Scholar] [CrossRef]
- di Prinzio, R.R.; Nigri, A.G.; Zaffina, S. Total Worker Heath Strategies in Italy: New Challenges and Opportunities for Occupational Health and Safety Practice. J. Health Soc. Sci. 2021, 6, 313–318. [Google Scholar]
- Riccò, M.; Vezzosi, L.; Cella, C.; Pecoraro, M.; Novembre, G.; Moreo, A.; Ognibeni, E.M.; Schellenberg, G.; Maranelli, G. Tetanus Vaccination Status in Construction Workers: Results from an Institutional Surveillance Campaign. Acta Biomed. 2019, 90, 269–278. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Balzarini, F.; Bragazzi, N.L. Inappropriate Risk Perception for SARS-CoV-2 Infection among Italian HCWs in the Eve of COVID-19 Pandemic. Acta Biomed. 2020, 91, 1–2. [Google Scholar] [CrossRef]
- Yates, F.J.; Stone, E.R. The Risk Construct. In Risk-Taking Behaviour; Yates, F.J., Ed.; John Wiley & Sons: Chichester, UK, 1992; pp. 1–25. ISBN 0471922501. [Google Scholar]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful Selection of Variables in Logistic Regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef]



| Variable | No./120 | Average ± SD |
|---|---|---|
| Gender | ||
| Male | 61, 50.8% | |
| Female | 59, 49.2% | |
| Age (years) | 48.2 ± 5.9 | |
| Age ≥ 50 years | 36, 30.0% | |
| Offspring | 104, 86.7% | |
| Seniority (years) | 16.3 ± 10.3 | |
| Seniority ≥ 10 years | 90, 75.0% | |
| Working as Occupational Physician for Healthcare Facilities | 86, 71.7% | |
| General Knowledge Score (%) | 74.5% ± 18.2 | |
| General Knowledge Score > median (78.6%) | 47, 39.2% |
| Perceived Barriers towards Vaccinations of Pregnant Women (Agree/Totally Agree) | No./120, % |
|---|---|
| Fear of side effects | 85, 70.8% |
| Costs of vaccinations | 15, 12.5% |
| Not perceived as a priority by other medical professionals | 55, 45.9% |
| Inappropriate risk perception by pregnant women | 100, 83.3% |
| Vaccination services are scarcely available | 45, 37.5% |
| Inappropriate understanding of official recommendations by pregnant women | 95, 79.2% |
| Inappropriate understanding of official recommendations by medical professionals | 75, 62.5% |
| Vaccines Actively Recommended on Women of Childbearing Age | No./120, % |
|---|---|
| Seasonal Influenza Virus | 80, 66.7% |
| Diphtheria/Tetanus/Pertussis | 85, 70.8% |
| Measles/Mumps/Rubella | 55, 45.8% |
| Varicella | 50, 41.7% |
| Hepatitis B Virus | 65, 54.2% |
| SARS-CoV-2 | 89, 74.2% |
| Previously Vaccinated against … | No./120, % |
|---|---|
| Seasonal Influenza Virus 1 | 79, 65.8% |
| Diphtheria/Tetanus/Pertussis 2 | 74, 61.7% |
| Measles/Parotitis/Rubella | 76, 63.3% |
| Varicella | 20, 16.7% |
| Hepatitis B Virus 3 | 86, 71.7% |
| SARS-CoV-2 | 110, 91.7% |
| SIV | |||
|---|---|---|---|
| Favorable (No./80, %) | Not Favorable (No./40, %) | p value | |
| Male Gender | 45, 56.3% | 16, 40.0% | 0.138 |
| Age ≥ 50 years | 24, 30.0% | 12, 30.0% | 1.000 |
| Any Offspring | 69, 86.3% | 35, 87.5% | 1.000 |
| Higher Knowledge status | 44, 55.0% | 3, 7.5% | <0.001 |
| Working as Occupational Physician for Healthcare facilities | 51, 63.7% | 35, 87.5% | 0.012 |
| Vaccinated against SIV | 66, 82.5% | 13, 32.5% | <0.001 |
| Higher RPS vs. SIV | 50, 62.5% | 10, 25.0% | <0.001 |
| Higher RPS vs. SIV vaccine | 20, 25.0% | 30, 75.0% | <0.001 |
| Tdap | |||
| Favorable (No./85, %) | Not Favorable (No./35, %) | p value | |
| Male Gender | 50, 58.8% | 11, 31.4% | 0.011 |
| Age ≥ 50 years | 24, 28.2% | 12, 34.3% | 0.661 |
| Any Offspring | 74, 87.1% | 30, 85.7% | 1.000 |
| Higher Knowledge status | 44, 51.8% | 3, 8.6% | <0.001 |
| Working as Occupational Physician for Healthcare facilities | 61, 71.8% | 25, 71.4% | 1.000 |
| Vaccinated with Tdap | 51, 60.0% | 23, 65.7% | 0.705 |
| Higher RPS vs. diphtheria | 45, 52.9% | 5, 14.3% | <0.001 |
| Higher RPS vs. diphtheria vaccine | 15, 17.6% | 10, 28.6% | 0.275 |
| Higher RPS vs. tetanus | 40, 47.1% | 10, 28.6% | 0.096 |
| Higher RPS vs. tetanus vaccine | 15, 17.6% | 15, 42.9% | 0.008 |
| Higher RPS vs. pertussis | 55, 64.7% | 5, 14.3% | <0.001 |
| Higher RPS vs. pertussis vaccine | 34, 40.0% | 20, 57.1% | 0.130 |
| SARS-CoV-2 | |||
| Favorable (No./89, %) | Not Favorable (No./31, %) | p value | |
| Male Gender | 43, 48.3% | 16, 51.6% | 0.914 |
| Age ≥ 50 years | 20, 22.5% | 16, 51.6% | 0.005 |
| Any Offspring | 77, 86.5% | 27, 87.1% | 1.000 |
| Higher Knowledge status | 45, 50.6% | 2, 6.5% | <0.001 |
| Working as Occupational Physician for Healthcare facilities | 65, 73.0% | 21, 67.7% | 0.740 |
| Vaccinated against SARS-CoV-2 | 88, 98.9% | 22, 71.0% | <0.001 |
| Higher RPS vs. SARS-CoV-2 | 48, 54.5% | 12, 37.5% | 0.148 |
| Higher RPS vs. SARS-CoV-2 vaccine (mRNA) | 34, 38.2% | 21, 67.7% | 0.008 |
| Higher RPS vs. SARS-CoV-2 vaccine (adenoviral carrier) | 39, 43.8% | 21, 67.7% | 0.037 |
| Higher RPS vs. SARS-CoV-2 vaccine (subunit) | 43, 48.3% | 17, 54.8% | 0.677 |
| SIV | Tdap | SARS-CoV-2 | |
|---|---|---|---|
| Adjusted Odds Ratio (95% Confidence Intervals) | |||
| Male Gender | - | 10.22 (2.60; 40.24) | - |
| Age ≥ 50 years | - | - | 0.62 (0.19; 1.99) |
| Higher Knowledge status | 102.24 (9.68; 1080.26) | 12.34 (2.62; 58.22) | 14.76 (2.74; 79.69) |
| Working as Occupational Physician for Healthcare facilities | 0.03 (0.01; 0.43) | - | - |
| Vaccinated against… | |||
| SIV | 4.90 (1.19; 20.14) | - | - |
| SARS-CoV-2 | - | - | 7.66 (0.72; 81.12) |
| Higher RPS vs. the pathogen | |||
| SIV | 1.04 (0.23; 4.71) | - | - |
| diphtheria | - | 2.38 (0.36; 15.84) | - |
| pertussis | - | 10.38 (1.47; 73.47) | - |
| Higher RPS vs. the vaccination | |||
| SIV | 0.04 (0.01; 0.35) | - | - |
| tetanus | - | 0.34 (0.10; 1.17) | - |
| SARS-CoV-2, mRNA | - | - | 0.14 (0.02; 1.17) |
| SARS-CoV-2, adenoviral vector | - | - | 2.59 (0.31; 21.45) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Baldassarre, A.; Cerviere, M.P.; Marchesi, F. Vaccine Hesitancy in Women of Childbearing Age and Occupational Physicians: Results from a Cross-Sectional Study (Italy, 2022). Women 2023, 3, 237-262. https://doi.org/10.3390/women3020019
Riccò M, Baldassarre A, Cerviere MP, Marchesi F. Vaccine Hesitancy in Women of Childbearing Age and Occupational Physicians: Results from a Cross-Sectional Study (Italy, 2022). Women. 2023; 3(2):237-262. https://doi.org/10.3390/women3020019
Chicago/Turabian StyleRiccò, Matteo, Antonio Baldassarre, Milena Pia Cerviere, and Federico Marchesi. 2023. "Vaccine Hesitancy in Women of Childbearing Age and Occupational Physicians: Results from a Cross-Sectional Study (Italy, 2022)" Women 3, no. 2: 237-262. https://doi.org/10.3390/women3020019