
Associations between Overweight and Obesity and Common Mental Disorders and Eating Behaviors of Adult Women

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Nutritional Status and Food Consumption
2.3. Mental Health and Eating Behavior Assessments
2.4. Statistical Analysis
3. Results
3.1. Lean Participants Presented Better Dietary Habits
3.2. Overweight and Obese Group Had Higher Scores for Risk of Mental Disorders, Emotional Eating, and Bingeing Behaviors
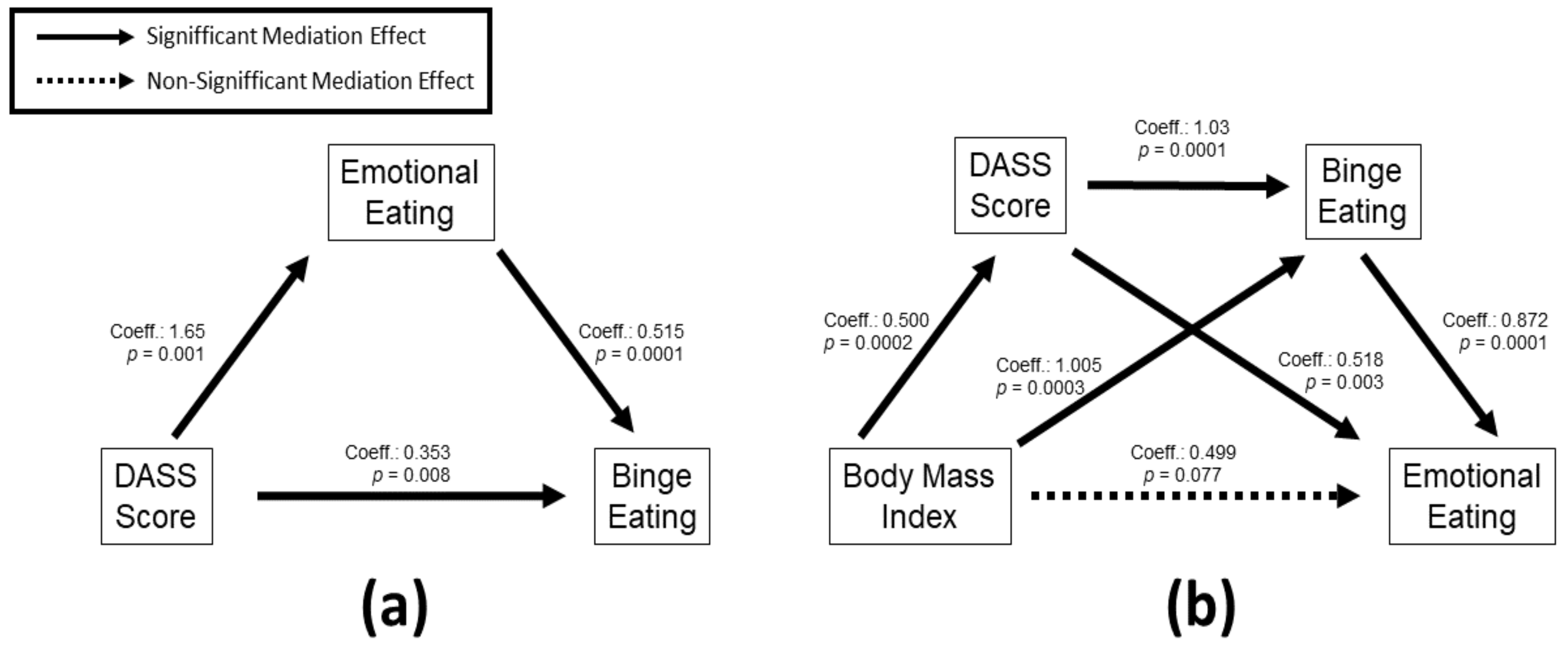
3.3. Body Mass Index, Mental Health and Eating Behavior Scores Present Several Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boutari, C.; Mantzoros, C.S. A 2022 update on the epidemiology of obesity and a call to action: As its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef] [PubMed]
- ABESO—Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica. Diretrizes Brasileiras de Obesidade 2016, 4th ed.; ABESO—Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica: São Paulo, Brazil, 2016. [Google Scholar]
- Nittari, G.; Scuri, S.; Petrelli, F.; Pirillo, I.; di Luca, N.M.; Grappasonni, I. Fighting obesity in children from European World Health Organization member states. Epidemiological data, medical-social aspects, and prevention programs. Clin. Ter. 2019, 170, e223–e230. [Google Scholar] [CrossRef] [PubMed]
- Lash, M.M.; Armstrong, A. Impact of obesity on women’s health. Fertil. Steril. 2009, 91, 1712–1716. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, A.J. Weight stigma is stressful. A review of evidence for the Cyclic Obesity/Weight-Based Stigma model. Appetite 2014, 82, 8–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuijpers, P.; Auerbach, R.P.; Benjet, C.; Bruffaerts, R.; Ebert, D.; Karyotaki, E.; Kessler, R.C. The World Health Organization World Mental Health International College Student initiative: An overview. Int. J. Methods Psychiatr. Res. 2019, 28, e1761. [Google Scholar] [CrossRef]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Noble, R.E. Depression in women. Metabolism 2005, 54, 49–52. [Google Scholar] [CrossRef]
- Sattler, K.M.; Deane, F.P.; Tapsell, L.; Kelly, P.J. Gender differences in the relationship of weight-based stigmatisation with motivation to exercise and physical activity in overweight individuals. Health Psychol. Open 2018, 5, 2055102918759691. [Google Scholar] [CrossRef] [Green Version]
- Puhl, R.; Suh, Y. Health Consequences of Weight Stigma: Implications for Obesity Prevention and Treatment. Curr. Obes. Rep. 2015, 4, 182–190. [Google Scholar] [CrossRef]
- Tomiyama, A.J. Stress and Obesity. Annu. Rev. Psychol. 2019, 70, 703–718. [Google Scholar] [CrossRef]
- Walker-Clarke, A.; Walasek, L.; Meyer, C. Psychosocial factors influencing the eating behaviours of older adults: A systematic review. Ageing Res. Rev. 2022, 77, 101597. [Google Scholar] [CrossRef]
- Lee, P.C.; Dixon, J.B. Food for Thought: Reward Mechanisms and Hedonic Overeating in Obesity. Curr. Obes. Rep. 2017, 6, 353–361. [Google Scholar] [CrossRef]
- Finlayson, G. Food addiction and obesity: Unnecessary medicalization of hedonic overeating. Nat. Rev. Endocrinol. 2017, 13, 493–498. [Google Scholar] [CrossRef] [Green Version]
- Faith, M.S.; Butryn, M.; Wadden, T.A.; Fabricatore, A.; Nguyen, A.M.; Heymsfield, S.B. Evidence for prospective associations among depression and obesity in population-based studies. Obes. Rev. 2011, 12, e438–e453. [Google Scholar] [CrossRef]
- De Wit, L.; Luppino, F.; van Straten, A.; Penninx, B.; Zitman, F.; Cuijpers, P. Depression and obesity: A meta-analysis of community-based studies. Psychiatry Res. 2010, 178, 230–235. [Google Scholar] [CrossRef]
- IBGE. Projeções da População do Brasil e Unidades da Federação por Sexo e Idade: 2010–2060. 2018. Available online: https://www.ibge.gov.br/estatisticas/sociais/populacao/9109-projecao-da-populacao.html (accessed on 1 March 2021).
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, J.E.L. International Standards for Anthropometric Assessment; North-West University: Potchefstroom, South Africa, 2006. [Google Scholar]
- Ministério da Saúde. Guia Alimentar para a População Brasileira, 2nd ed.; Básica, D.d.A., Ed.; Ministério da Saúde: Brasília, Brazil, 2014; p. 156.
- Gabe, K.T.; Jaime, P.C. Development and testing of a scale to evaluate diet according to the recommendations of the Dietary Guidelines for the Brazilian Population. Public Health Nutr. 2019, 22, 785–796. [Google Scholar] [CrossRef]
- Gonçalves, D.M.; Stein, A.T.; Kapczinski, F. Avaliação de desempenho do Self-Reporting Questionnaire como instrumento de rastreamento psiquiátrico: Um estudo comparativo com o Structured Clinical Interview for DSM-IV-TR. Cad. Saúde Pública 2008, 24, 380–390. [Google Scholar] [CrossRef] [Green Version]
- Vignola, R.C.; Tucci, A.M. Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J. Affect. Disord. 2014, 155, 104–109. [Google Scholar] [CrossRef]
- Natacci, L.C.; Ferreira Júnior, M. The three factor eating questionnaire—R21: Tradução para o português e aplicação em mulheres brasileiras. Rev. Nutr. 2011, 24, 383–394. [Google Scholar] [CrossRef]
- Valeri, L.; Vanderweele, T.J. Mediation analysis allowing for exposure-mediator interactions and causal interpretation: Theoretical assumptions and implementation with SAS and SPSS macros. Psychol. Methods 2013, 18, 137–150. [Google Scholar] [CrossRef]
- Santos, M.M.D.; Nascimento, F.F.D.; Cabral, S.D.M.R.; Oliveira, E.S.D.; Santos, R.M.D.; Carvalho, L.D.S. Relação bilateral entre excesso de peso e transtornos mentais. Rev. Bras. Promoção Saúde 2018, 31, 1–7. [Google Scholar] [CrossRef]
- Bielemann, R.M.; Motta, J.V.; Minten, G.C.; Horta, B.L.; Gigante, D.P. Consumption of ultra-processed foods and their impact on the diet of young adults. Rev. Saude Publica 2015, 49, 28. [Google Scholar] [CrossRef]
- Marti, A. Ultra-Processed Foods Are Not “Real Food” but Really Affect Your Health. Nutrients 2019, 11, 1902. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2017, 21, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Lima, L.F.; Ghetti, F.F.; Lacerda, K.C.; Elias, M.A.R.; Silva, A.A.; Luquetti, S.C.P.D. Relação entre medidas antropométricas, escolaridade, renda e índice de qualidade da dieta de mulheres climatéricas. HU Rev. 2017, 42, 297–305. [Google Scholar]
- Guo, X.; Warden, B.A.; Paeratakul, S.; Bray, G.A. Healthy Eating Index and obesity. Eur. J. Clin. Nutr. 2004, 58, 1580–1586. [Google Scholar] [CrossRef] [Green Version]
- Costa, D.D.; Reis, B.Z.; Vieira, D.A.D.S.; Costa, J.O.; Teixeira, P.D.S.; Raposo, O.F.F.; Lima, F.E.L.D.; Mendes-Netto, R.S. Índice de qualidade da dieta de mulheres usuárias de um programa de atividade física regular “Academia da Cidade”, Aracajú, SE. Rev. Nutr. 2012, 25, 731–741. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.-Y.; Huang, C.-K.; Tai, C.-M.; Lin, H.-Y.; Kao, Y.-H.; Tsai, C.-C.; Hsuan, C.-F.; Lee, S.-L.; Chi, S.-C.; Yen, Y.-C. Psychiatric disorders of patients seeking obesity treatment. BMC Psychiatry 2013, 13, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Löffler, A.; Luck, T.; Then, F.S.; Sikorski, C.; Kovacs, P.; Böttcher, Y.; Breitfeld, J.; Tönjes, A.; Horstmann, A.; Löffler, M.; et al. Eating Behaviour in the General Population: An Analysis of the Factor Structure of the German Version of the Three-Factor-Eating-Questionnaire (TFEQ) and Its Association with the Body Mass Index. PLoS ONE 2015, 10, e0133977. [Google Scholar] [CrossRef] [PubMed]
- Braden, A.; Flatt, S.W.; Boutelle, K.N.; Strong, D.; Sherwood, N.E.; Rock, C.L. Emotional eating is associated with weight loss success among adults enrolled in a weight loss program. J. Behav. Med. 2016, 39, 727–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvo, V.; Sanudo, A.; Kristeller, J.; Schveitzer, M.C.; Martins, P.; Favarato, M.L.; Demarzo, M. Mindful eating for overweight and obese women in Brazil: An exploratory mixed-methods pilot study. Nutr. Health 2021. [Google Scholar] [CrossRef]
- Zervos, K.; Koletsi, M.; Mantzios, M.; Skopeliti, N.; Tsitsas, G.; Naska, A. An Eight-Week Mindful Eating Program Applied in a Mediterranean Population with Overweight or Obesity: The EATT Intervention Study. Psychol. Rep. 2022, 125, 1011–1040. [Google Scholar] [CrossRef]
- Grilo, C.M.; Masheb, R.M.; Wilson, G.T.; Gueorguieva, R.; White, M.A. Cognitive-behavioral therapy, behavioral weight loss, and sequential treatment for obese patients with binge-eating disorder: A randomized controlled trial. J. Consult. Clin. Psychol. 2011, 79, 675–685. [Google Scholar] [CrossRef] [Green Version]
- Spinelli, S.; Monteleone, E. Food Preferences and Obesity. Endocrinol. Metab. 2021, 36, 209–219. [Google Scholar] [CrossRef]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e63. [Google Scholar] [CrossRef]


{kind=link}
| Lean (n = 105) | Overweight and Obese (n = 64) | p Value | |
|---|---|---|---|
| Age (years) | 29.88 ± 5.2 | 30.35 ± 5.4 | 0.575 |
| Body Mass Index (kg/m2) | 22.20 ± 1.8 | 31.57 ± 4.6 | 0.001 * |
| Diet Quality Score | 46.79 ± 9.1 | 37.37 ± 9.5 | 0.001 * |
| Classification of the Nutritional Status ( n (%)) | |||
| Eutrophic | 105 (100%) | 0 (0%) | - |
| Overweight | 0 (0%) | 25 (39.1%) | - |
| Obese grade I | 0 (0%) | 28 (43.8%) | - |
| Obese grade II | 0 (0%) | 11 (17.2%) | - |
| Lean (n = 105) | Overweight and Obese (n = 64) | p value | Cohen’s d | Effect-Size r | |
|---|---|---|---|---|---|
| SRQ-20 Score | 4.92 ± 3.3 | 7.32 ± 4.4 | 0.001 ** | −0.72 | 0.34 |
| DASS Score | 10.36 ± 7.8 | 16.09 ± 11.23 | 0.001 ** | −0.71 | 0.33 |
| Depression Scale Score | 2.62 ± 2.7 | 4.73 ± 4.55 | 0.001 ** | −0.69 | 0.32 |
| Anxiety Scale Score | 2.73 ± 3.1 | 4.71 ± 3.8 | 0.001 ** | −0.65 | 0.31 |
| Stress Scale Score | 5.15 ± 3.15 | 6.64 ± 3.8 | 0.007 ** | −0.48 | 0.23 |
| Binge Eating Score | 34.33 ± 20.4 | 48.61 ± 22.9 | 0.001 ** | −0.74 | 0.34 |
| Cognitive Restraint Score | 50.16 ± 23.4 | 43.74 ± 19.6 | 0.069 | 0.31 | 0.15 |
| Emotional Eating Score | 37.66 ± 27.90 | 60.24 ± 28.55 | 0.001 ** | −0.87 | 0.40 |
| p Value | 95% C.I. for EXP(B) | Odds Ratio (%) | ||
|---|---|---|---|---|
| Mental Suffering | 0.001 | 1.05 | 1.187 | 11.6 |
| Depression | 0.001 | 1.054 | 1.245 | 14.5 |
| Anxiety | 0.001 | 1.058 | 1.204 | 12.9 |
| Stress | 0.009 | 0.941 | 1.257 | 8.8 |
| Binge Eating | 0.001 | 1.08 | 1.25 | 16.2 |
| Cognitive Restraint | 0.884 | 0.94 | 1.075 | 0.5 |
| Emotional Eating | 0.004 | 1.035 | 1.203 | 11.6 |
| BMI | SRQ20 | DASS | Depression | Anxiety | Stress | Binge Eating | Cognitive Restraint | Emotional Eating | |
|---|---|---|---|---|---|---|---|---|---|
| BMI | 1 | 0.247 * | 0.257 * | 0.218 ** | 0.253 * | 0.188 * | 0.385 * | −0.12 (NS) | 0.412 * |
| SRQ20 | 0.247 * | 1 | 0.698 * | 0.680 * | 0.572 * | 0.642 * | 0.498 * | −0.221 * | 0.569 * |
| DASS | 0.257 * | 0.698 * | 1 | 0.903 * | 0.896 * | 0.919 * | 0.539 * | −0.152 ** | 0.545 * |
| Depression | 0.218 ** | 0.680 * | 0.903 * | 1 | 0.741 * | 0.757 * | 0.506 * | −0.134 (NS) | 0.483 * |
| Anxiety | 0.253 * | 0.572 * | 0.896 * | 0.741 * | 1 | 0.756 * | 0.450 * | −0.224 ** | 0.434 * |
| Stress | 0.188 ** | 0.642 * | 0.919 * | 0.757 * | 0.756 * | 1 | 0.471 * | −0.087 (NS) | 0.514 * |
| Binge Eating | 0.385 * | 0.498 * | 0.539 * | 0.506 * | 0.450 * | 0.471 * | 1 | −0.022 (NS) | 0.772 * |
| Cognitive Restraint | −0.12 (NS) | −0.221 ** | −0.152 ** | −0.134 (NS) | −0.224 ** | −0.087 (NS) | −0.022 (NS) | 1 | 0.056 (NS) |
| Emotional Eating | 0.412* | 0.569 * | 0.545 * | 0.483 * | 0.434 * | 0.514 * | 0.772 * | 0.056 (NS) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valencio, A.C.J.; Antunes, A.B.; Fonseca, L.; Araujo, J.; Silva, M.C.G.; Costa, M.; Czermainski, J.G.e.S.; Rosa, C.B.; Coghetto, C.C.; Carteri, R.B. Associations between Overweight and Obesity and Common Mental Disorders and Eating Behaviors of Adult Women. Obesities 2022, 2, 350-360. https://doi.org/10.3390/obesities2040029
Valencio ACJ, Antunes AB, Fonseca L, Araujo J, Silva MCG, Costa M, Czermainski JGeS, Rosa CB, Coghetto CC, Carteri RB. Associations between Overweight and Obesity and Common Mental Disorders and Eating Behaviors of Adult Women. Obesities. 2022; 2(4):350-360. https://doi.org/10.3390/obesities2040029
Chicago/Turabian StyleValencio, Ana Clara Justino, Andressa Bueno Antunes, Lilian Fonseca, Julia Araujo, Maria Clara Goyer Silva, Marcia Costa, Juliana Gomes e Silva Czermainski, Carolina Böettge Rosa, Chaline Caren Coghetto, and Randhall Bruce Carteri. 2022. "Associations between Overweight and Obesity and Common Mental Disorders and Eating Behaviors of Adult Women" Obesities 2, no. 4: 350-360. https://doi.org/10.3390/obesities2040029