
Liraglutide and Exercise: A Possible Treatment for Obesity?
by
 ,
,
Ana Paula Azevêdo Macêdo
1, 
Renan Fudoli Lins Vieira
1,
Guilherme Domingos Brisque
1,
Gabriela Ferreira Abud
2 and
José Rodrigo Pauli
1,3,* 1
Laboratory of Molecular Biology of Exercise (LaBMEx), University of Campinas (UNICAMP), Limeira 13484-350, SP, Brazil
2
Department of Health Sciences, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto 14049-900, SP, Brazil
3
Laboratory of Cell Signaling, Obesity and Comorbidities Research Center (OCRC), University of Campinas, Campinas 13083-864, SP, Brazil
*
Author to whom correspondence should be addressed.
Obesities 2022, 2(3), 285-291; https://doi.org/10.3390/obesities2030023
Submission received: 21 July 2022
/
Revised: 6 August 2022
/
Accepted: 13 August 2022
/
Published: 17 August 2022
(This article belongs to the Topic Metabolism and Health)
{kind=link}
Abstract
:(1) Background: Obesity has become an important public health problem worldwide, and its characterization as a chronic disease reflects the impact of a complex and multifactorial condition. The treatment for obesity is based on lifestyle interventions that induce a negative energy balance. However, adherence to a lifestyle intervention is a challenge for many overweight and obese people. Thus, pharmacotherapy in the management of obesity is used to increase patient adherence to lifestyle changes and overcome the biological adaptations that occur with weight loss. Among these drugs, liraglutide stands out. Liraglutide is an analog of human glucagon-like peptide-1 (GLP-1), a hormone that regulates glucose-dependent insulin secretion, and glucagon release. (2) Results: Liraglutide appears to be effective in weight reduction and glycemic control in diabetic and obese patients, and combination of liraglutide and exercise can also bring benefits in weight loss. Furthermore, the combination of liraglutide and physical exercise can prevent adverse effects observed in the administration of liraglutide. (3) Conclusions: liraglutide seems to contribute to cardiometabolic improvement in obese individuals with or without diabetes, and the combination of liraglutide and physical exercise can prevent adverse effects observed in the administration of liraglutide.
1. Introduction
Obesity has become an important public health problem worldwide, and its characterization as a chronic disease reflects the impact of a complex and multifactorial condition, with genetic, physiological, behavioral, and socio-cultural contributions [1]. The clinical complications of obesity encompass a range of disorders, including metabolic (diabetes, hypertension, and nonalcoholic steatohepatitis), mechanical (obstructive sleep apnea and orthopedic problems), and mental health (anxiety and depression) disorders, as well as others, such as cardiovascular diseases and certain types of cancer [2].
The treatment for obesity is based on lifestyle interventions that induce a negative energy balance. When decreasing energy intake and increasing physical activity, accompanied by behavior change techniques, a daily energy deficit of approximately 500 kcal is recommended for weight loss [3]. This energy deficit can produce moderate weight loss over a year. Energy balance changes with weight loss, making it necessary to adjust energy intake and expenditure during weight control. However, adherence to a lifestyle intervention is a challenge for many overweight and obese people [1].
Thus, pharmacotherapy in the management of obesity is used to increase patient adherence to lifestyle changes and overcome the biological adaptations that occur with weight loss. There are several agents for the pharmacological therapy of obesity, leading to decreased appetite, gastric emptying, nutrient absorption, or increased satiety. Growing evidence shows that behavior-based interventions with an anti-obesity drug can result in greater weight loss than usual care conditions alone [1].
Among these drugs, liraglutide stands out. Liraglutide is an analog of human glucagon-like peptide-1 (GLP-1), a hormone that regulates glucose-dependent insulin secretion, and glucagon release, and also modulates appetite, satiety, and energy intake [4]. Liraglutide was originally approved for the treatment of type 2 diabetes at a subcutaneous dose of 1.2 mg or 1.8 mg daily and subsequently approved in many countries for weight management at a higher dose of 3.0 mg per day, in combination with diet and exercise interventions [2]. Thus, this mini-review aims to provide scientific evidence on the effects of liraglutide in the treatment and prevention of obesity in combination with physical exercise.
2. Liraglutide Mechanism of Action
Liraglutide is an approved GLP-1 receptor agonist at a daily dose of 3.0 mg for chronic weight management in eligible patients with and without diabetes [5]. GLP-1 is a polypeptide incretin hormone that induces glucose-dependent insulin secretion, reduces plasma glucagon concentrations, delays gastric emptying, and suppresses appetite. GLP-1 is derived from post-translational processing of the pre-proglucagon gene and subsequently cleaved into its biologically active forms, GLP-1 amide, which comprises approximately 80% of circulating GLP-1 [5,6]. GLP-1 is secreted by the alpha (α) cells of the islets of Langerhans in the distal intestinal mucosa, mainly in response to the presence of nutrients in the intestinal lumen. Once in circulation, the half-life of GLP-1 is less than 2 min due to rapid degradation by the enzyme dipeptidyl peptidase-IV (DPP-IV) [6].
GLP-1 is classified as an incretin hormone because it stimulates decreases in blood glucose levels by increasing the amount of insulin released by pancreatic beta cells after eating before blood glucose levels rise. GLP-1 is also effective in controlling blood glucose because it suppresses glucagon secretion and delays gastric emptying [6].
Another analog of GLP-1, semaglutide in oral administration has similar liraglutide via the subcutaneous route, not resulting in glycemic control. Treatment with semaglutide in patients with type 2 diabetes for 52 weeks results in a reduction in HbA1c levels similar to subcutaneous liraglutide. However, there was a significant reduction in body weight compared to the administration of subcutaneous liraglutide [7]. Among overweight or obese adults without diabetes, once weekly subcutaneous semaglutide compared to once daily subcutaneous liraglutide resulted in significantly greater weight loss at 68 weeks [8].
In addition, liraglutide modifies the distribution of body fat, probably through a combination of mechanisms that reduce plasma glucagon, delay gastric emptying, and suppress appetite via neuronal pathways [5]. However, little is known about the biochemical and molecular mechanisms involved in this process.
3. Liraglutide and Obesity Treatment
The majority of individuals with type 2 diabetes are obese, and weight control has also been investigated in these individuals. In this context, Garvey et al. (2020) researched a 56-week, randomized, double-blind, placebo-controlled, multinational, multicenter study in subjects with overweight or obesity and type 2 diabetes treated with basal insulin and oral antidiabetic drugs. Subjects were randomized to liraglutide (3.0 mg) combined with intensive behavioral therapy or placebo. Liraglutide as an adjunct to intensive behavioral therapy was superior to placebo in weight loss and improved glycemic control in obese diabetics [9]. Similarly, for overweight and obese participants with type 2 diabetes, the use of subcutaneous liraglutide (3.0 mg) daily, compared with placebo, resulted in weight loss over 56 weeks [10].
Furthermore, liraglutide appears to be effective even in the absence of diabetes. In a randomized, double-blind, placebo, and active-controlled, multicenter, dose-ranging study in adults with a body mass index (BMI) of 30 kg/m2, liraglutide (3.0 mg; started at 0.6 mg per day and increased by 0.6 mg per week) promoted significant dose-related weight loss in combination with dietary and exercise interventions [2]. Corroborating these data, a randomized, double-blind, placebo-controlled trial evaluated adults with a BMI of at least 30 kg/m2 or a BMI of at least 27 kg/m2 with metabolic syndrome but no diabetes, submitted to treatment with subcutaneous liraglutide (3.0 mg) or placebo once daily, and a 500-kcal reduced-calorie diet and guideline-recommended physical activity advice. In overweight or obese adults at a high risk of cardiovascular disease, 3.0 mg of liraglutide once daily plus a lifestyle intervention significantly reduced visceral adipose tissue over 40 weeks of treatment [5].
Because obese people have difficulty maintaining lifestyle-change protocols, a retrospective, observational cohort study compared the clinical outcomes of treatment with 120 mg of orlistat and liraglutide (up to 3 mg daily) in obese adults with at least one weight-related comorbidity who had not lost at least 5% of their weight after 6 months of lifestyle modification. Treatment with both drugs significantly reduced weight, fasting blood glucose, systolic blood pressure, and low-density lipoprotein-cholesterol. In addition, with liraglutide, weight loss was significantly greater than that observed with orlistat [11]. Weight loss and persistence outcomes with 3.0 mg liraglutide were assessed across obesity classes, in an observational, retrospective study of 3.0 mg liraglutide for weight management (as adjunct to diet and exercise). The treatment with 3.0 mg liraglutide, regardless of obesity class, is associated with similar clinically significant weight loss, time to maintenance dose, and medication persistence [12].
However, it is important to mention the most common adverse events with the use of liraglutide, such as gastrointestinal symptoms, mainly nausea, which are also reported for other GLP-receptor agonists. To complement the information on side effects, we recommend reading the study by Lundgren et al. [13], which shows the adverse effects presented by the participants after using the drug.
Based on these data, liraglutide appears to be effective in weight reduction and glycemic control in diabetic and obese patients, but the safety and toxicity of the drug need to be investigated at different doses.
4. Physical Exercise and Obesity Treatment
Physical exercise is another strategy adopted for the prevention and treatment of obesity [14]. The various beneficial effects of physical exercise on health as a whole are already well established [14,15]. In obesity, exercise promotes a negative energy balance, mainly due to the increase in energy expenditure [14,15,16]. In this way, physical exercise reduces body mass and contributes to the reduction and prevention of obesity. It is worth mentioning that physical exercise will often bring benefits and promote health improvement even without loss of body mass.
However, it is necessary to point out that adherence to a long-term exercise program is often difficult, especially for overweight and obese people [17,18]. In addition, exercise promotes adaptation, and for weight loss to remain constant, it is necessary to make adjustments to the training program (intensity, volume, frequency); otherwise, there will be a stagnation in the results [17,18,19]. Therefore, it is ultimately more comfortable and easier to use medication to solve the problem [20,21,22].
An important point when we talk about exercise is the fact that it is a natural and non-pharmacological strategy for obesity. This is an important factor to analyze because of the side effects of the use of drugs, such as liraglutide, which have shown some adverse effects, mainly gastrointestinal events [13,15,22]. Given all this information, it remains for us to analyze the combined effects of physical activity and the use of liraglutide, to see if this combination can bring more robust or additional effects in the treatment of obesity.
5. Liraglutide and Physical Exercise
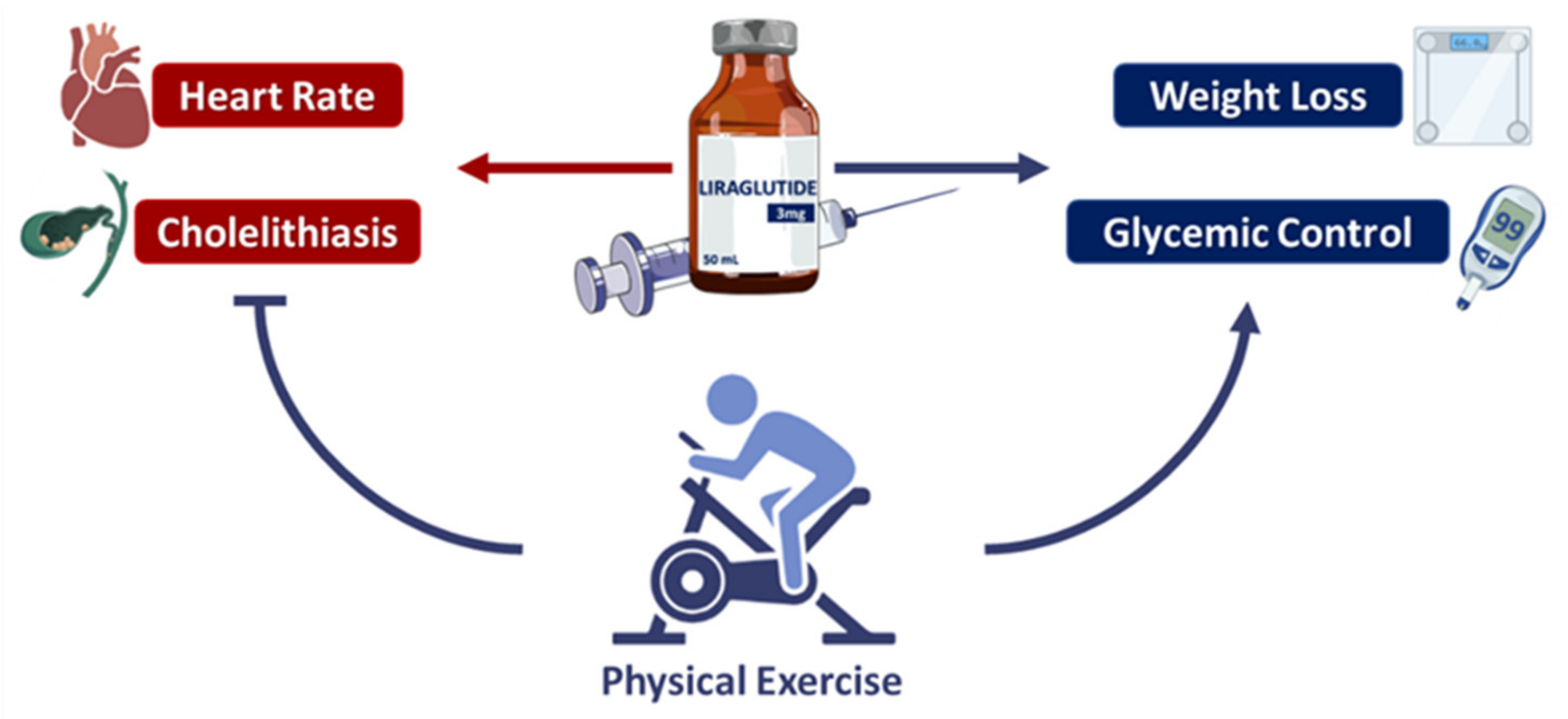
The practice of physical exercise alone or in combination with medications or dietary interventions, such as time-restricted feeding, has been shown to be effective for health and to present relevant effects on organs and tissues [13,23,24,25]. Exercise training improves body weight and body composition in overweight or obese adults [26]. Although the effect on weight and fat loss is often of relatively small magnitude, the reduction in visceral fat already improves the cardiometabolic health of the patients [27]. In addition to the difficulties of weight loss in the treatment of obesity, subsequent weight regain after weight loss is another important factor. In a randomized, direct, placebo-controlled study of obese adults without diabetes by Lundgren et al. [13], participants underwent an 8-week intervention with a low-calorie diet, which promoted a reduction in body weight and fat percentage. After 8 weeks, participants were randomly assigned for 1 year to placebo, exercise (150 min per week of moderate-intensity aerobic physical activity, or 75 min per week of vigorous-intensity aerobic physical activity), liraglutide (3.0 mg daily), and liraglutide-plus-exercise groups. After 1 year, all active treatment strategies led to greater weight loss than placebo, showing the effectiveness of exercise and liraglutide alone and in combination in controlling weight loss. However, the combined strategies had more robust results in weight loss and fat percentage, in addition to improving cardiorespiratory fitness, insulin sensitivity, and glycated hemoglobin levels. Another important point of the study was the increase in heart rate and cholelithiasis observed in the liraglutide group. These adverse effects of liraglutide administration were not observed in the combined group.
A randomized, double-blind study with obese adolescents, consisting of a 56-week treatment period and a 26-week follow-up period, evaluated the effect of liraglutide administration and lifestyle changes. The results showed a reduction in body weight compared to the placebo group [28], indicating that this combination of liraglutide and exercise can also benefit younger individuals.
A recent study investigated the effects of liraglutide and voluntary running on glycemic homeostasis, brown adipose tissue fatty acid composition, and white adipose tissue browning in an animal model of diabetes (db/db) [29]. The animals were randomly divided into voluntary running, liraglutide, voluntary running-plus-liraglutide, and control groups. Voluntary running or treatment with liraglutide significantly reduced blood glucose and increased insulin levels, with the combined group demonstrating a better effect than liraglutide alone. Thus, the combined treatment led to an increased hypoglycemic effect. In addition, the combined group of liraglutide and exercise also showed a reduction in body weight compared to the control group, and higher activation of brown adipose tissue and white adipose tissue browning. This is an important point given the role of brown adipose tissue in relation to thermogenesis, energy expenditure, and glucose consumption. The effects of liraglutide and physical exercise are summarized in Figure 1.
6. Liraglutide and Pediatric Studies
In pediatric clinical trials, liraglutide also appears to promote promising effects on glycemic control and weight loss. A randomized, placebo-controlled trial with type 2 diabetic children and adolescents treated with oral antidiabetics investigated the effects of administering liraglutide (1.8 mg daily) associated with diet and exercise counseling for a 26-week double-blind trial, followed by a 26-week open-label extension period. The results demonstrated the superiority of liraglutide over placebo, reducing plasma glucose levels at 26 weeks and 52 weeks. In addition, the liraglutide group showed lower glycated hemoglobin levels compared to the placebo group at 26 weeks and was also at 52 weeks [30]. Another randomized, double-blind, placebo-controlled study was conducted in obese children without diabetes for a short period, at least 7 weeks, with the potential, based on being granted permission, for up to 6 weeks of optional treatment with liraglutide starting at 0.3 mg with weekly dose escalations up to 3.0 mg or maximum tolerated dose. In liraglutide-treated participants, a significant reduction was observed in BMI Z score and weight loss compared to the control group, although this was not a significant difference [31].
Another important point of the study is that safety and tolerability were evaluated throughout the trial, the results of which showed adverse events with the use of liraglutide, such as gastrointestinal disturbances, nausea, vomiting, and episodes of hypoglycemia. Although there is evidence from pediatric clinical trials on the subject, more studies are needed to better elucidate the effects of the drug, especially the use of liraglutide associated with physical exercise in this specific population. In the study by Tamborlane et al. (2019) [30], counseling was only provided to participants on diet and exercise. Therefore, future studies investigating the effects of the combination of liraglutide and physical exercise in children and adolescents are needed.
7. Conclusions
Based on this review, liraglutide seems to contribute to cardiometabolic improvement in obese individuals with or without diabetes. Although this benefit appears to be independent of glycemic changes, there are still many mechanisms to be investigated, mainly molecular mechanisms. In addition, the combination of liraglutide and exercise can enhance the benefits of both treatments, and the results may be more robust. Finally, the combination of liraglutide and physical exercise can prevent adverse effects observed in the administration of liraglutide (increased resting heart rate, cholelithiasis, and gastrointestinal events, including nausea, vomiting, and diarrhea). Studies evaluating the effects of liraglutide associated or not with exercise are still recent, and more studies are needed to evaluate these two therapies for obesity together.
Author Contributions
A.P.A.M.—writing—original draft preparation. R.F.L.V.—writing—review and editing. G.D.B.—writing—review and editing. G.F.A.—writing—review and editing. J.R.P.—conceptualization, writing—review and editing, supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wiechert, M.; Holzapfel, C. Nutrition Concepts for the Treatment of Obesity in Adults. Nutrients 2022, 14, 169. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, P.M.; Birkenfeld, A.L.; McGowan, B.; Mosenzon, O.; Pedersen, S.D.; Wharton, S.; Carson, C.G.; Jepsen, C.H.; Kabisch, M.; Wilding, J.P.H. Efficacy and Safety of Semaglutide Compared with Liraglutide and Placebo for Weight Loss in Patients with Obesity: A Randomised, Double-Blind, Placebo and Active Controlled, Dose-Ranging, Phase 2 Trial. Lancet 2018, 392, 637–649. [Google Scholar] [CrossRef]
- Lemstra, M.; Bird, Y.; Nwankwo, C.; Rogers, M.; Moraros, J. Weight Loss Intervention Adherence and Factors Promoting Adherence: A Meta-Analysis. Patient Prefer. Adherence 2016, 10, 1547–1559. [Google Scholar] [CrossRef] [PubMed]
- Dailey, M.J.; Moran, T.H. Glucagon-like Peptide 1 and Appetite. Trends Endocrinol. Metab. 2013, 24, 85–91. [Google Scholar] [CrossRef]
- Neeland, I.J.; Marso, S.P.; Ayers, C.R.; Lewis, B.; Oslica, R.; Francis, W.; Rodder, S.; Pandey, A.; Joshi, P.H. Effects of Liraglutide on Visceral and Ectopic Fat in Adults with Overweight and Obesity at High Cardiovascular Risk: A Randomised, Double-Blind, Placebo-Controlled, Clinical Trial. Lancet Diabetes Endocrinol. 2021, 9, 595–605. [Google Scholar] [CrossRef]
- Ladenheim, E.E. Liraglutide and Obesity: A Review of the Data so Far. Drug Des. Dev. Therapy. 2015, 2015, 1867–1875. [Google Scholar] [CrossRef]
- Pratley, R.; Amod, A.; Hoff, S.T.; Kadowaki, T.; Lingvay, I.; Nauck, M.; Pedersen, K.B.; Saugstrup, T.; Meier, J.J. Oral Semaglutide versus Subcutaneous Liraglutide and Placebo in Type 2 Diabetes (PIONEER 4): A Randomised, Double-Blind, Phase 3a Trial. Lancet 2019, 394, 39–50. [Google Scholar] [CrossRef]
- Rubino, D.M.; Greenway, F.L.; Khalid, U.; O’Neil, P.M.; Rosenstock, J.; Sørrig, R.; Wadden, T.A.; Wizert, A.; Garvey, W.T. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults with Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA—J. Am. Med. Assoc. 2022, 327, 138–150. [Google Scholar] [CrossRef]
- Garvey, W.T.; Birkenfeld, A.L.; Dicker, D.; Mingrone, G.; Pedersen, S.D.; Satylganova, A.; Skovgaard, D.; Sugimoto, D.; Jensen, C.; Mosenzon, O. Efficacy and Safety of Liraglutide 3.0 Mg in Individuals with Overweight or Obesity and Type 2 Diabetes Treated with Basal Insulin: The SCALE Insulin Randomized Controlled Trial. Diabetes Care 2020, 43, 1085–1093. [Google Scholar] [CrossRef]
- Davies, M.J.; Bergenstal, R.; Bode, B.; Kushner, R.F.; Lewin, A.; Skjøth, T.V.; Andreasen, A.H.; Jensen, C.B.; DeFronzo, R.A.; Valensi, P.; et al. Efficacy of Liraglutide for Weight Loss among Patients with Type 2 Diabetes: The SCALE Diabetes Randomized Clinical Trial. JAMA—J. Am. Med. Assoc. 2015, 314, 687–699. [Google Scholar] [CrossRef]
- Gorgojo-Martínez, J.J.; Basagoiti-Carreño, B.; Sanz-Velasco, A.; Serrano-Moreno, C.; Almodóvar-Ruiz, F. Effectiveness and Tolerability of Orlistat and Liraglutide in Patients with Obesity in a Real-World Setting: The XENSOR Study. Int. J. Clin. Pract. 2019, 73, e13399. [Google Scholar] [CrossRef]
- Wharton, S.; Haase, C.L.; Kamran, E.; Liu, A.; Mancini, J.; Neish, D.; Pakseresht, A.; Power, G.S.; Christensen, R.A.G. Weight Loss and Persistence with Liraglutide 3.0 Mg by Obesity Class in the Real-World Effectiveness Study in Canada. Obes. Sci. Pract. 2020, 6, 439–444. [Google Scholar] [CrossRef]
- Lundgren, J.R.; Janus, C.; Jensen, S.B.K.; Juhl, C.R.; Olsen, L.M.; Christensen, R.M.; Svane, M.S.; Bandholm, T.; Bojsen-Møller, K.N.; Blond, M.B.; et al. Healthy Weight Loss Maintenance with Exercise, Liraglutide, or Both Combined. N. Engl. J. Med. 2021, 384, 1719–1730. [Google Scholar] [CrossRef]
- Petridou, A.; Siopi, A.; Mougios, V. Exercise in the Management of Obesity. Metab. Clin. Exp. 2019, 92, 163–169. [Google Scholar] [CrossRef]
- Bray, G.A.; Frühbeck, G.; Ryan Donna, H.; Wilding Jhon, P.H. Management of Obesity. Lancet 2016, 397, 1947–1956. [Google Scholar] [CrossRef]
- Hsu, K.J.; de Liao, C.; Tsai, M.W.; Chen, C.N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef]
- Fothergill, E.; Guo, J.; Howard, L.; Kerns, J.C.; Knuth, N.D.; Brychta, R.; Chen, K.Y.; Skarulis, M.C.; Walter, M.; Walter, P.J.; et al. Persistent Metabolic Adaptation 6 Years after “The Biggest Loser” Competition. Obesity 2016, 24, 1612–1619. [Google Scholar] [CrossRef] [PubMed]
- Hunter, G.R.; Brock, D.W.; Byrne, N.M.; Chandler-Laney, P.C.; del Corral, P.; Gower, B.A. Exercise Training Prevents Regain of Visceral Fat for 1 Year Following Weight Loss. Obesity 2010, 18, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Rogers, R.J.; Davis, K.K.; Collins, K.A. Role of Physical Activity and Exercise in Treating Patients with Overweight and Obesity. Clin. Chem. 2018, 64, 99–107. [Google Scholar] [CrossRef]
- Aaseth, J.; Ellefsen, S.; Alehagen, U.; Sundfør, T.M.; Alexander, J. Diets and Drugs for Weight Loss and Health in Obesity—An Update. Biomed. Pharmacother. 2021, 140, 111789. [Google Scholar] [CrossRef]
- Srivastava, G.; Apovian, C. Future Pharmacotherapy for Obesity: New Anti-Obesity Drugs on the Horizon. Curr. Obes. Rep. 2018, 7, 147–161. [Google Scholar] [CrossRef] [PubMed]
- Johansson, K.; Neovius, M.; Hemmingsson, E. Effects of Anti-Obesity Drugs, Diet, and Exercise on Weight-Loss Maintenance after a Very-Low-Calorie Diet or Low-Calorie Diet: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2014, 99, 14–23. [Google Scholar] [CrossRef]
- Vieira, R.F.L.; Muñoz, V.R.; Junqueira, R.L.; de Oliveira, F.; Gaspar, R.C.; Nakandakari, S.C.B.R.; de Oliveira Costa, S.; Torsoni, M.A.; da Silva, A.S.R.; Cintra, D.E.; et al. Time-Restricted Feeding Combined with Aerobic Exercise Training Can Prevent Weight Gain and Improve Metabolic Disorders in Mice Fed a High-Fat Diet. J. Physiol. 2021, 600, 797–813. [Google Scholar] [CrossRef]
- Ropelle, E.R.; Ramos Da Silva, A.S.; Cintra, D.E.; Pereira De Moura, L.; Teixeira, A.M.; Pauli, J.R. Physical Exercise: A Versatile Anti-Inflammatory Tool Involved in the Control of Hypothalamic Satiety Signaling. Exerc. Immunol. Rev. 2021, 27, 7–21. [Google Scholar]
- Gaspar, R.C.; Pauli, J.R.; Shulman, G.I.; Muñoz, V.R. An Update on Brown Adipose Tissue Biology: A Discussion of Recent Findings. Am. J. Physiol.-Endocrinol. Metab. 2021, 230, E488–E495. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Dias, S.; Strasser, B.; Hoffmann, G. Impact of Different Training Modalities on Anthropometric and Metabolic Characteristics in Overweight/Obese Subjects: A Systematic Review and Network Meta-Analysis. PLoS ONE 2013, 8, e82853. [Google Scholar] [CrossRef]
- Bellicha, A.; van Baak, M.A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraça, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; et al. Effect of Exercise Training on Weight Loss, Body Composition Changes, and Weight Maintenance in Adults with Overweight or Obesity: An Overview of 12 Systematic Reviews and 149 Studies. Obes. Rev. 2021, 22, e13256. [Google Scholar] [CrossRef]
- Kelly, A.S.; Auerbach, P.; Barrientos-Perez, M.; Gies, M.; Hale, P.M.; Marcus, C.; Mastrandrea, L.D.; Prabhu, N.; Arslanian, S. A Randomized, Controlled Trial of Liraglutide for Adolescents with Obesity. N. Engl. J. Med. 2022, 382, 2117–2128. [Google Scholar] [CrossRef]
- Yin, R.; Ma, Y.; Zhang, N.; Yang, L.; Zhao, D. Combined Effects of Voluntary Running and Liraglutide on Glucose Homeostasis, Fatty Acid Composition of Brown Adipose Tissue Phospholipids, and White Adipose Tissue Browning in Db/Db Mice. Chin. J. Physiol. 2022, 65, 117. [Google Scholar] [CrossRef]
- Tamborlane, W.V.; Barrientos-Pérez, M.; Fainberg, U.; Frimer-Larsen, H.; Hafez, M.; Hale, P.M.; Jalaludin, M.Y.; Kovarenko, M.; Libman, I.; Lynch, J.L.; et al. Liraglutide in Children and Adolescents with Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 637–646. [Google Scholar] [CrossRef]
- Mastrandrea, L.D.; Witten, L.; Petri Kristin, C.C.; Hale, P.M.; Hedman, H.K.; Riesenberg, R.A. Liraglutide Effects in a Pediatric (7–11 y) Population with Obesity: A Randomized, Double-Blind, Placebo-Controlled, Short-Term Trial to Assess Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics. Pediatr. Obes. 2019, 14, e12495. [Google Scholar] [CrossRef]
Figure 1.
Summary of the effects of liraglutide associated with exercise or not.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Macêdo, A.P.A.; Vieira, R.F.L.; Brisque, G.D.; Abud, G.F.; Pauli, J.R. Liraglutide and Exercise: A Possible Treatment for Obesity? Obesities 2022, 2, 285-291. https://doi.org/10.3390/obesities2030023
AMA Style
Macêdo APA, Vieira RFL, Brisque GD, Abud GF, Pauli JR. Liraglutide and Exercise: A Possible Treatment for Obesity? Obesities. 2022; 2(3):285-291. https://doi.org/10.3390/obesities2030023
Chicago/Turabian StyleMacêdo, Ana Paula Azevêdo, Renan Fudoli Lins Vieira, Guilherme Domingos Brisque, Gabriela Ferreira Abud, and José Rodrigo Pauli. 2022. "Liraglutide and Exercise: A Possible Treatment for Obesity?" Obesities 2, no. 3: 285-291. https://doi.org/10.3390/obesities2030023