
The Role of Cisternostomy in the Management of Severe Traumatic Brain Injury: A Triple-Center Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Selection
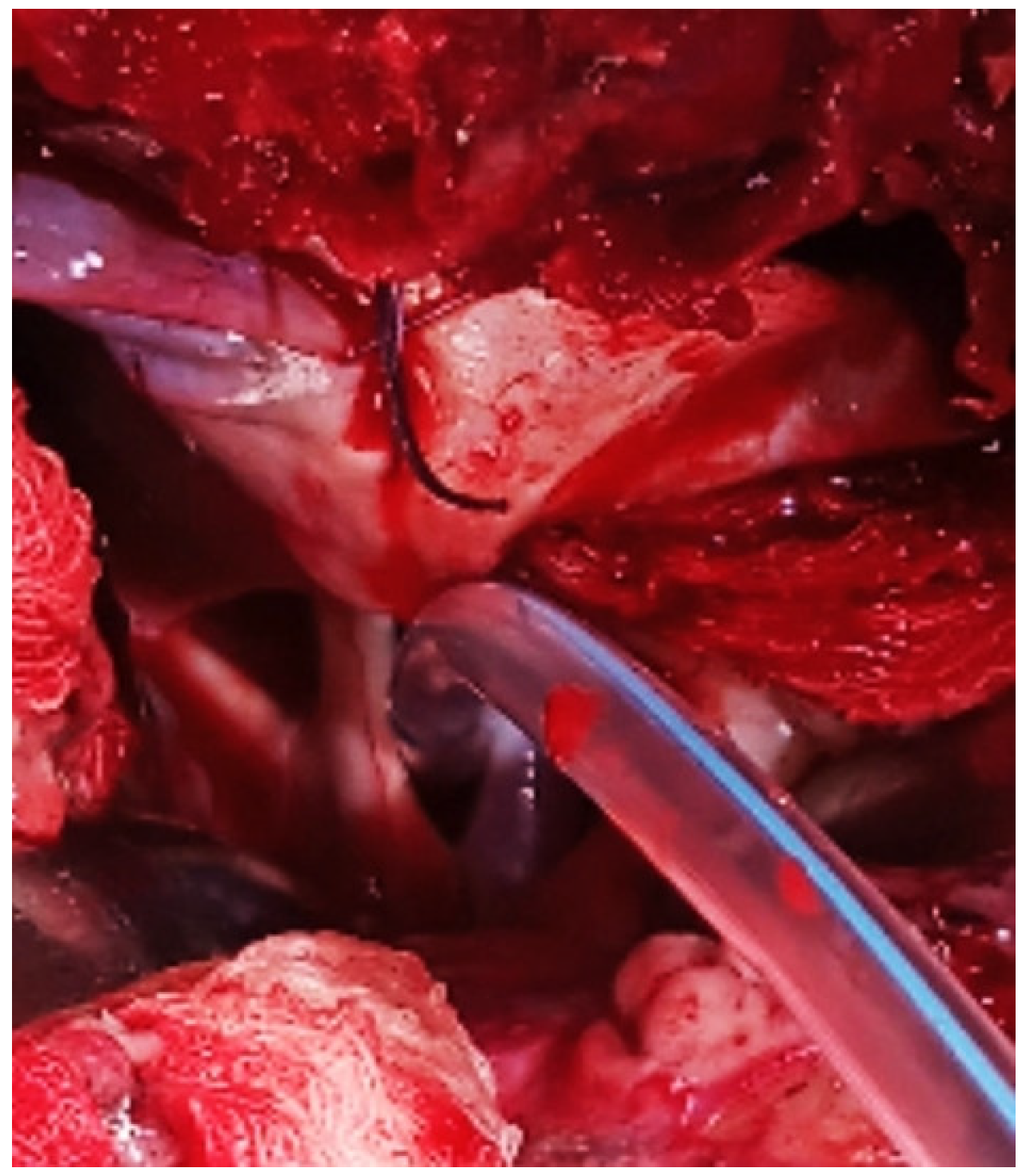
2.2. Surgical Procedure
2.3. Data Collection
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montemurro, N.; Santoro, G.; Marani, W.; Petrella, G. Posttraumatic synchronous double acute epidural hematomas: Two craniotomies, single skin incision. Surg. Neurol. Int. 2020, 11, 435. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.J.; Rosenfeld, J.V.; Murray, L.; Arabi, Y.M.; Davies, A.R.; D’Urso, P.; Kossmann, T.; Ponsford, J.; Seppelt, I.; Reilly, P.; et al. Decompressive craniectomy in diffuse traumatic brain injury. N. Engl. J. Med. 2011, 364, 1493–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, J.H. Craniectomy for traumatic brain injury: Results from the DECRA trial. Neurosurgery 2011, 68, N19–N20. [Google Scholar]
- Honeybul, S.; Ho, K.M.; Lind, C.R. What can be learned from the DECRA study. World Neurosurg. 2013, 79, 159–161. [Google Scholar]
- Kolias, A.G.; Adams, H.; Timofeev, I.S.; Corteen, E.A.; Hossain, I.; Czosnyka, M.; Timothy, J.; Anderson, I.; Bulters, D.O.; Belli, A.; et al. Evaluation of Outcomes Among Patients with Traumatic Intracranial Hypertension Treated with Decompressive Craniectomy vs Standard Medical Care at 24 Months: A Secondary Analysis of the RESCUEicp Randomized Clinical Trial. JAMA Neurol. 2022, 79, 664–671. [Google Scholar] [CrossRef]
- Kumar, P.; Goyal, N.; Chaturvedi, J.; Arora, R.K.; Singh, P.R.; Shakya, J.; Rekapalli, R.; Sadhasivam, S.; Sihag, R.; Bahurupi, Y. Basal Cisternostomy in Head Injury: More Questions than Answers. Neurol. India 2022, 70, 1384–1390. [Google Scholar]
- Hoz, S.S.; Alramadan, A.H.; Hadi, A.Q.; Moscote Salazar, L.R. Cisternostomy in Neurosurgery: A New Proposed General Classification Based on Mechanism and Indications of the Cisternostomy Proper. J. Neurosci. Rural. Pract. 2018, 9, 650–652. [Google Scholar]
- Espaillat, A.; Encarnacion Ramirez, M.D.J.; Barrientos, R.; Nurmukhametov, R.; Peralta, I.; Coats, C.; Marmol, F.; Jimenez, O.; Fermin, R.; Valenzuela, S.; et al. Prevalece and Topography Anatomy of Dilated Virchow-Robin Spaces. World J. Med. Case Rep. 2022, 3, 11–20. [Google Scholar]
- Cherian, I.; Grasso, G.; Bernardo, A.; Munakomi, S. Anatomy and physiology of cisternostomy. Chin. J. Traumatol. 2016, 19, 7–10. [Google Scholar] [CrossRef]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef] [Green Version]
- Timofeev, I.; Dahyot-Fizelier, C.; Keong, N.; Nortje, J.; Al-Rawi, P.G.; Czosnyka, M.; Menon, D.K.; Kirkpatrick, P.J.; Gupta, A.K.; Hutchinson, P.J. Ventriculostomy for control of raised ICP in acute traumatic brain injury. Acta Neurochir. Suppl. 2008, 102, 99–104. [Google Scholar]
- Giammattei, L.; Messerer, M.; Oddo, M.; Borsotti, F.; Levivier, M.; Daniel, R.T. Cisternostomy for Refractory Posttraumatic Intracranial Hypertension. World Neurosurg. 2018, 109, 460–463. [Google Scholar] [CrossRef]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef]
- Grasso, G.; Cherian, I. Cisternostomy for Traumatic Brain Injury: A New Era Begins. Bull. Emerg. Trauma 2016, 4, 119–120. [Google Scholar]
- Badke, G.L.; Araujo, J.L.V.; Miura, F.K.; Guirado, V.; Saade, N.; Paiva, A.L.C.; Avelar, T.M.; Pedrozo, C.A.G.; Veiga, J.C.E. Analysis of direct costs of decompressive craniectomy in victims of traumatic brain injury. Arq. Neuropsiquiatr. 2018, 76, 257–264. [Google Scholar] [CrossRef]
- Valle, D.; Villarreal, X.P.; Lunny, C.; Chalamgari, A.; Wajid, M.; Mahmood, A.; Buthani, S.; Lucke-Wold, B. Surgical Management of Neurotrauma: When to Intervene. J. Clin. Trials Regul. 2022, 4, 41–55. [Google Scholar]
- Iliff, J.J.; Chen, M.J.; Plog, B.A.; Zeppenfeld, D.M.; Soltero, M.; Yang, L.; Singh, I.; Deane, R.; Nedergaard, M. Impairment of glymphatic pathway function promotes tau pathology after traumatic brain injury. J. Neurosci. 2014, 34, 16180–16193. [Google Scholar] [CrossRef] [Green Version]
- Encarnacion Ramirez, M.; Barrientos Castillo, R.E.; Musa, G.; Nurmukhametov, R.; Igorevich, B.O. ‘Brain Tissue Out’ in a Train Struck Victim: A Case Report. Neurol. Neurobiol. 2022, 1, 2613–7828. [Google Scholar]
- Prasad, G.L.; Gupta, D.K.; Mahapatra, A.K.; Sharma, B.S. Surgical results of decompressive craniectomy in very young children: A level one trauma centre experience from India. Brain Inj. 2015, 29, 1717–1724. [Google Scholar] [CrossRef]
- Eraky, A.M.; Treffy, R.; Hedayat, H.S. Cisternostomy as a Surgical Treatment for Traumatic Brain Injury-Related Prolonged and Delayed Intracranial Pressure Elevation: A Case Report. Cureus 2023, 15, e37508. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Benet, A.; Lawton, M.T. Julius Caesar’s Epilepsy: Was It Caused by A Brain Arteriovenous Malformation? World Neurosurg. 2015, 84, 1985–1987. [Google Scholar] [CrossRef] [PubMed]
- Eraky, A.M.; Treffy, R.; Hedayat, H.S. Cisternotomy and Liliequist’s Membrane Fenestration as a Surgical Treatment for Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): A Case Report. Cureus 2022, 14, e31363. [Google Scholar] [CrossRef] [PubMed]
- Cherian, I.; Yi, G.; Munakomi, S. Cisternostomy: Replacing the age old decompressive hemicraniectomy? Asian J. Neurosurg. 2013, 8, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Masoudi, M.S.; Rezaee, E.; Hakiminejad, H.; Tavakoli, M.; Sadeghpoor, T. Cisternostomy for Management of Intracranial Hypertension in Severe Traumatic Brain Injury; Case Report and Literature Review. Bull. Emerg. Trauma 2016, 4, 161–164. [Google Scholar]
- Cherian, I.; Bernardo, A.; Grasso, G. Cisternostomy for traumatic brain injury: Pathophysiological mechanisms and surgical technical notes. World Neurosurg. 2016, 89, 51–57. [Google Scholar] [CrossRef]
- Hutchinson, P.J.; Kolias, A.G.; Timofeev, I.S.; Corteen, E.A.; Czosnyka, M.; Timothy, J.; Anderson, I.; Bulters, D.O.; Belli, A.; Eynon, C.A.; et al. RESCUEicp Trial Collaborators. Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension. N. Engl. J. Med. 2016, 375, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Jessen, N.A.; Munk, A.S.F.; Lundgaard, I.; Nedergaard, M. The glymphatic system: A beginner’s guide. Neurochem. Res. 2015, 40, 2583–2599. [Google Scholar] [CrossRef] [Green Version]
- Johnston, M.; Zakharov, A.; Papaiconomou, C.; Salmasi, G.; Armstrong, D. Evidence of connections between cerebrospinal fluid and nasal lymphatic vessels in humans, non-human primates and other mammalian species. Cereb. Fluid Res. 2004, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Encarnacion Ramirez, M.D.J.; Barrientos Castillo, R.E.; Vorobiev, A.; Kiselev, N.; Aquino, A.A.; Efe, I.E. Basal cisternostomy for traumatic brain injury: A case report of unexpected good recovery. Chin. J. Traumatol. 2022, 25, 302–305. [Google Scholar] [CrossRef]
- Grasso, G. Surgical treatment for traumatic brain injury: Is it time for reappraisal? World Neurosurg. 2015, 84, 594. [Google Scholar] [CrossRef]
- Volovici, V.; Haitsma, I.K. Cisternostomy in Traumatic Brain Injury: Time for the World to Listen-Cerebrospinal Fluid Release: Possibly the Missing Link in Traumatic Brain Injury. World Neurosurg. 2022, 162, 3–5. [Google Scholar] [CrossRef]
- Chandra, V.V.R.; Mowliswara Prasad, B.C.; Banavath, H.N.; Chandrasekhar Reddy, K. Cisternostomy versus Decompressive Craniectomy for the Management of Traumatic Brain Injury: A Randomized Controlled Trial. World Neurosurg. 2022, 162, e58–e64. [Google Scholar] [CrossRef]
- Goyal, N.; Kumar, P. Putting ‘CSF-Shift Edema’ Hypothesis to Test: Comparing Cisternal and Parenchymal Pressures After Basal Cisternostomy for Head Injury. World Neurosurg. 2021, 148, e252–e263. [Google Scholar] [CrossRef]
- Parthiban, J.K.B.C.; Sundaramahalingam, S.; Rao, J.B.; Nannaware, V.P.; Rathwa, V.N.; Nasre, V.Y.; Prahlad, S.T. Basal Cisternostomy—A Microsurgical Cerebro Spinal Fluid Let Out Procedure and Treatment Option in the Management of Traumatic Brain Injury. Analysis of 40 Consecutive Head Injury Patients Operated with and without Bone Flap Replacement Following Cisternostomy in a Tertiary Care Centre in India. Neurol. India 2021, 69, 328–333. [Google Scholar]
- Abdulla, E.; Ravindra, J.; Rahman, S.; Rahman, M.M. Letter to the Editor Regarding “Cisternostomy in Traumatic Brain Injury: Time for the World to Listen. Cerebrospinal Fluid Release: Possibly the Missing Link in TBI”. World Neurosurg. 2022, 162, 203–204. [Google Scholar] [CrossRef]
- Marani, W.; Mannará, F.; Noda, K.; Kondo, T.; Ota, N.; Perrini, P.; Montemurro, N.; Kinoshita, Y.; Tsuji, S.; Kamiyama, H.; et al. Management of an Uncommon Complication: Anterior Choroidal Artery Occlusion by Posterior Clinoid Process Detected Through Intraoperative Monitoring After Clipping of Paraclinoid Aneurysm: 2-Dimensional Operative Video. Oper. Neurosurg. 2021, 21, E124–E125. [Google Scholar] [CrossRef]
- Horiuchi, T.; Yamamoto, Y.; Kuroiwa, M.; Rahmah, N.N.; Hongo, K. Pontine infarction caused by medial branch injury of the basilar artery as a rare complication of cisternal drain placement. J. Clin. Neurosci. 2012, 19, 592–593. [Google Scholar] [CrossRef] [Green Version]
- Montemurro, N.; Scerrati, A.; Ricciardi, L.; Trevisi, G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. J. Clin. Med. 2021, 11, 223. [Google Scholar] [CrossRef]
- Lizana, J.; Montemurro, N.; Aliaga, N.; Marani, W.; Tanikawa, R. From textbook to patient: A practical guide to train the end-to-side microvascular anastomosis. Br. J. Neurosurg. 2023, 37, 116–120. [Google Scholar] [CrossRef]
- Rush, B.; Rousseau, J.; Sekhon, M.S.; Griesdale, D.E. Craniotomy Versus Craniectomy for Acute Traumatic Subdural Hematoma in the United States: A National Retrospective Cohort Analysis. World Neurosurg. 2016, 88, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Encarnacion Ramirez, M.; Ramirez Pena, I.; Barrientos Castillo, R.E.; Sufianov, A.; Goncharov, E.; Soriano Sanchez, J.A.; Colome-Hidalgo, M.; Nurmukhametov, R.; Cerda Céspedes, J.R.; Montemurro, N. Development of a 3D Printed Brain Model with Vasculature for Neurosurgical Procedure Visualisation and Training. Biomedicines 2023, 11, 330. [Google Scholar] [CrossRef] [PubMed]
- Servadei, F.; Kolias, A.; Kirollos, R.; Khan, T.; Hutchinson, P. Cisternostomy for traumatic brain injury-rigorous evaluation is necessary. Acta Neurochir. 2020, 162, 481–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montemurro, N. Telemedicine: Could it represent a new problem for spine surgeons to solve? Glob. Spine J. 2022, 12, 1306–1307. [Google Scholar] [CrossRef]
- Suarilah, I.; Zulkarnain, H.; Saragih, I.D.; Lee, B.-O. Effectiveness of telehealth interventions among traumatic brain injury survivors: A systematic review and meta-analysis. J. Telemed. Telecare 2022, 3, 1357633X221102264. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Hospital Center | N° Patients (%) | Male/Female Ratio | GCS at Admission, Mean (Range) |
|---|---|---|---|
| RUDN University (Moscow, Russia) | 14 (46.7) | 13/1 | 5.9 (4–8) |
| General Hospital (Durango, Mexico) | 10 (33.3) | 6/4 | 6.2 (4–8) |
| Hospital Regional Universitario José María Cabral y Baez (Santiago, Dominican Republic) | 6 (20) | 2/4 | 5.3 (4–6) |
| Treatment Group | Mortality Rate | Surgical Morbidity | Favorable Outcome at Discharge | Favorable Recovery at 2 Weeks | Favorable Recovery at 3 Months | Favorable Recovery at 6 Months |
|---|---|---|---|---|---|---|
| DC + Cisternostomy (n = 24) | 12.5% | 20.8% | 29.2% | 54.5% | 87.5% | 91.7% |
| Cisternostomy Alone (n = 6) | 16.7% | 16.7% | 0% | 50% | 83.3% | 100% |
| p-value | 0.82 | 0.82 | 0.16 | 0.48 | 0.60 | 0.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Encarnación Ramirez, M.; Baez, I.P.; Marszal Mangbel’ Mikorska, H.; Mukengeshay, J.N.; Nurmukhametov, R.; Baldoncini, M.; Lafuente, J.; Ovalles, C.; López Santos, M.D.; Chmutin, G.E.; et al. The Role of Cisternostomy in the Management of Severe Traumatic Brain Injury: A Triple-Center Study. Surgeries 2023, 4, 283-292. https://doi.org/10.3390/surgeries4020029
Encarnación Ramirez M, Baez IP, Marszal Mangbel’ Mikorska H, Mukengeshay JN, Nurmukhametov R, Baldoncini M, Lafuente J, Ovalles C, López Santos MD, Chmutin GE, et al. The Role of Cisternostomy in the Management of Severe Traumatic Brain Injury: A Triple-Center Study. Surgeries. 2023; 4(2):283-292. https://doi.org/10.3390/surgeries4020029
Chicago/Turabian StyleEncarnación Ramirez, Manuel, Ismael Peralta Baez, Harmonie Marszal Mangbel’ Mikorska, Jeff Natalaja Mukengeshay, Renat Nurmukhametov, Matias Baldoncini, Jesus Lafuente, Carlos Ovalles, Michael David López Santos, Gennady E. Chmutin, and et al. 2023. "The Role of Cisternostomy in the Management of Severe Traumatic Brain Injury: A Triple-Center Study" Surgeries 4, no. 2: 283-292. https://doi.org/10.3390/surgeries4020029