
Two Cases of Herlyn-Werner-Wunderlich Syndrome with Severe Dysmenorrhea, One Misdiagnosis and One Missed Diagnosis
Departments of Obstetrics and Gynecology, Soonchunhyang University Gumi Hospital, Gumi 39371, Republic of Korea
*
Author to whom correspondence should be addressed.
Surgeries 2023, 4(1), 10-16; https://doi.org/10.3390/surgeries4010002
Submission received: 22 October 2022
/
Revised: 17 December 2022
/
Accepted: 19 December 2022
/
Published: 29 December 2022
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Herlyn-Werner-Wunderlich (HWW) syndrome is a rare variant of mullerian duct anomalies characterized by the triad of uterine didelphys, obstructed hemivagina and ipsilateral renal agenesis. We report two cases of HWW syndrome in young women with abdominal pain. This diagnosis can easily be missed if a clinician is not aware of the syndrome. In one case, the computed tomography image of obstructed hemivagina with hematocolpos was initially mistaken for a cystic tumor of adnexa by the radiologist; in the other case, correct diagnosis was missed for years despite numerous visits to different hospitals due to lack of awareness of the syndrome.
1. Introduction
Herlyn-Werner-Wunderlich (HWW) syndrome is a rare congenital anomaly characterized by uterus didelphys, obstructed hemivagina and ipsilateral renal agenesis [1,2]. Following the first description of the syndrome in 1922, prevalence has not been reported exactly but is assumed to be between 0.1% and 3.8% [3,4]. Gradually increasing dysmenorrhea or pelvic pain unrelated to menstruation in diseased young women is usually the chief complaint, and pelvic or vaginal mass can also be present. Pelvic magnetic resonance imaging (MRI) is considered the best diagnostic modality. Treatment involves surgical resection of the obstructed wall of the hemi-vagina.
We report two cases of HWW syndrome; in one case, the computed tomography (CT) image of obstructed hemi-vagina with hematocolpos was initially mistaken for a cystic tumor of adnexa by the radiologist, hence the patient was referred to the Gynecology department for emergency diagnostic laparoscopy. In the other case, even though the patient underwent all the necessary evaluations from different hospitals for years, correct diagnosis was delayed.
2. Case Presentation
Case 1
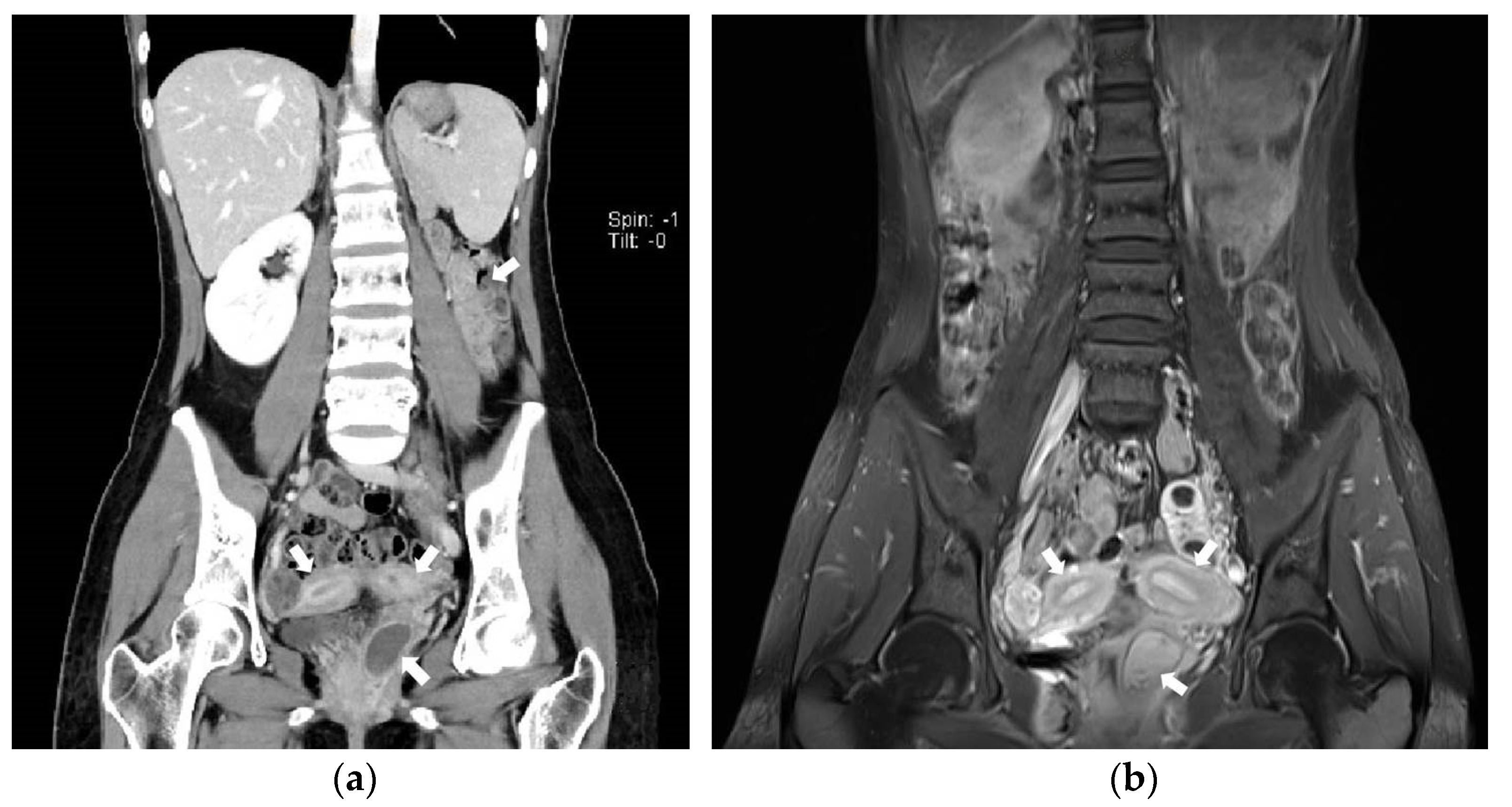
A 23-year-old unmarried woman with no history of coitus came to the Gastroenterology department presenting with acute-onset cramping pain of the left lower abdomen. The patient was referred to the Gynecology department after undergoing an abdominopelvic CT scan, during which one of our radiologists reported “uterus didelphys or bicornuate uterus with left par-ovarian or ovarian cyst” (Figure 1a).
After her menarche at the age of thirteen, the patient experienced menstruations with irregular cycles of approximately sixty days. The menstrual amount was small and she complained of menstrual pain which required a pain killer. Because the patient had not previously had sexual intercourse, we did not perform vaginal speculum exam or transvaginal ultrasonogram (USG).
Having been informed that the patient had one kidney, we noticed the patient had HWW syndrome, so we performed a pelvic MRI (Figure 1b)
Pre-operative laboratory finding revealed no remarkable results. We informed the patient preoperatively about the possibility of hymen tear during the planned surgery.
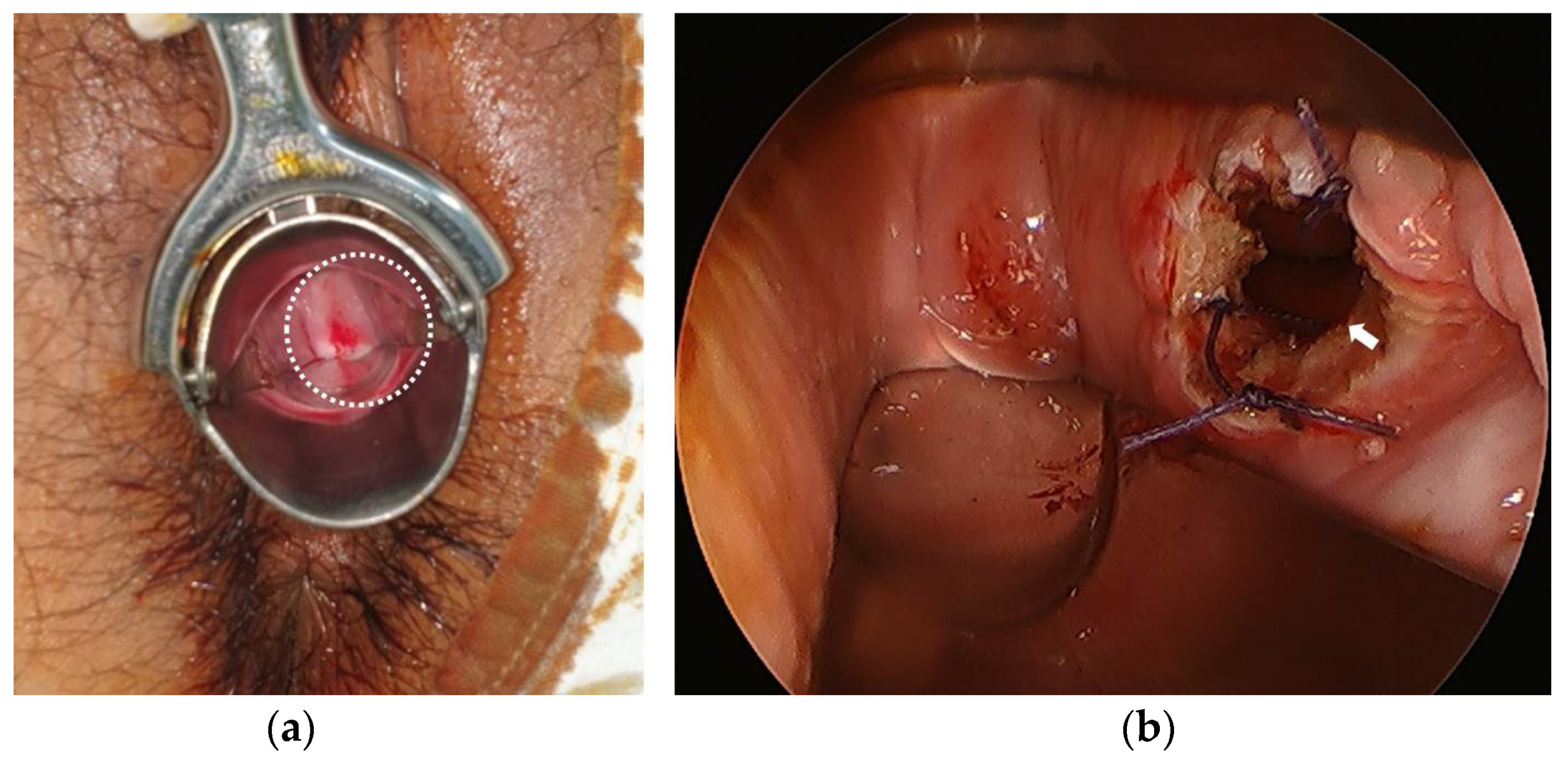
During surgery, bulging left vaginal wall was noticed (Figure 2a). We made a circular incision of 2 cm diameter on the bulged wall. After suctioning the hematoma, we were able to identify the normal-looking left vaginal cavity using a laparoscope with a light source. We then performed marsupialization with vicryl on the resected circular margin of the vaginal wall (Figure 2b) and repaired the torn hymen.
Immediately after surgery, her abdominal pain subsided and she was discharged.
The patient has made follow-up visits for two years so far, and she has not experienced mestrual pain or other abdominal pain since the surgery. The transvaginal USG findings are not remarkable.
Case 2
A 20-year-old sexually active unmarried woman visited the emergency room (ER) with severe dysmenorrhea. She complained of symptoms such as fever, chilling, nausea, severe lower abdominal or whole abdominal pain on almost every menstrual period for two years, for which doctors had been unable to determine the cause. The patient was aware that she has uterus didelphys with vagina and only one kidney. She was informed about her uterus didelphys when she was 17 after visiting a Gynecologist to obtain a prescription for oral pills. When she went to another gynecologist for a papanicolaou smear, she was told that she had a vagina and one uterine cervix. When she visited another ER last year for dysmenorrhea, she was informed that she had only one kidney after taking abdominopelvic CT.
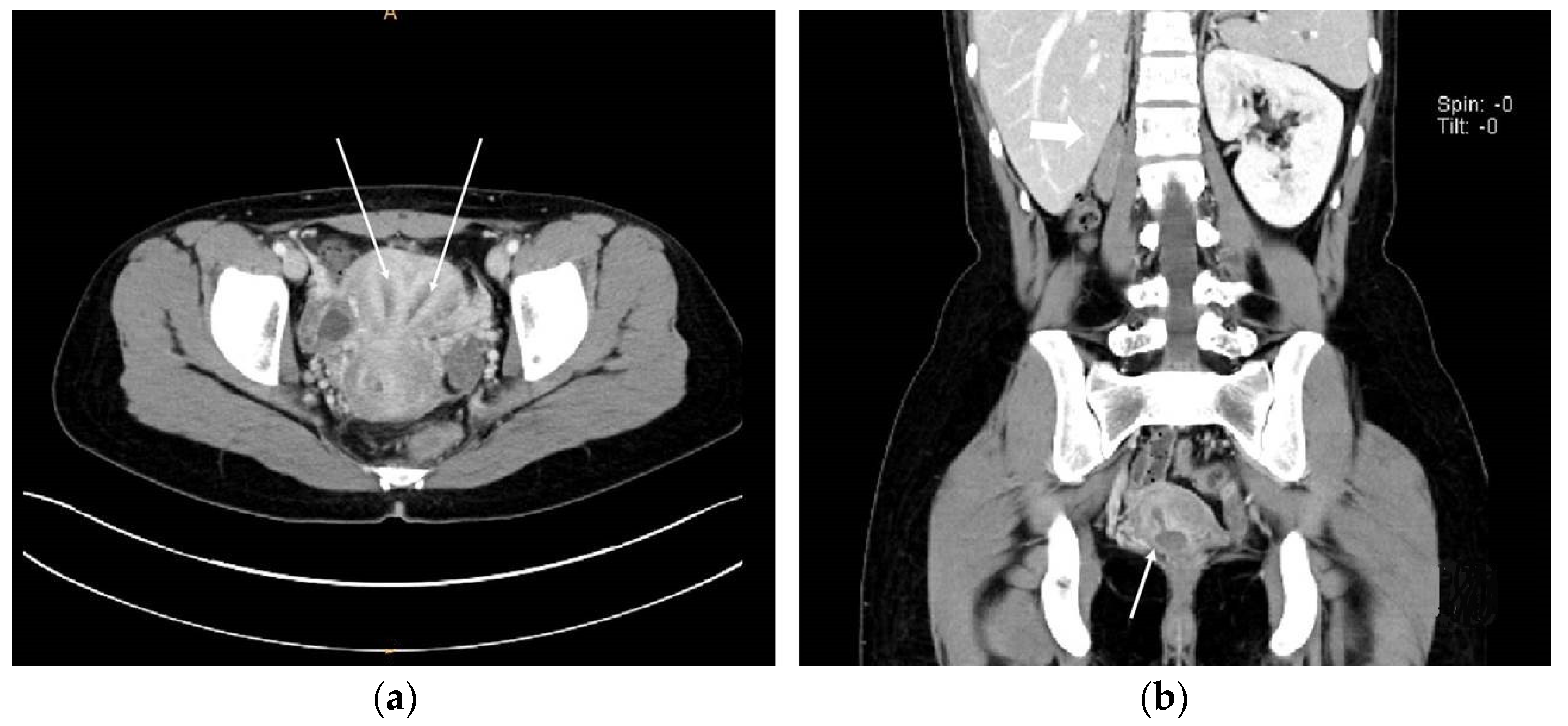
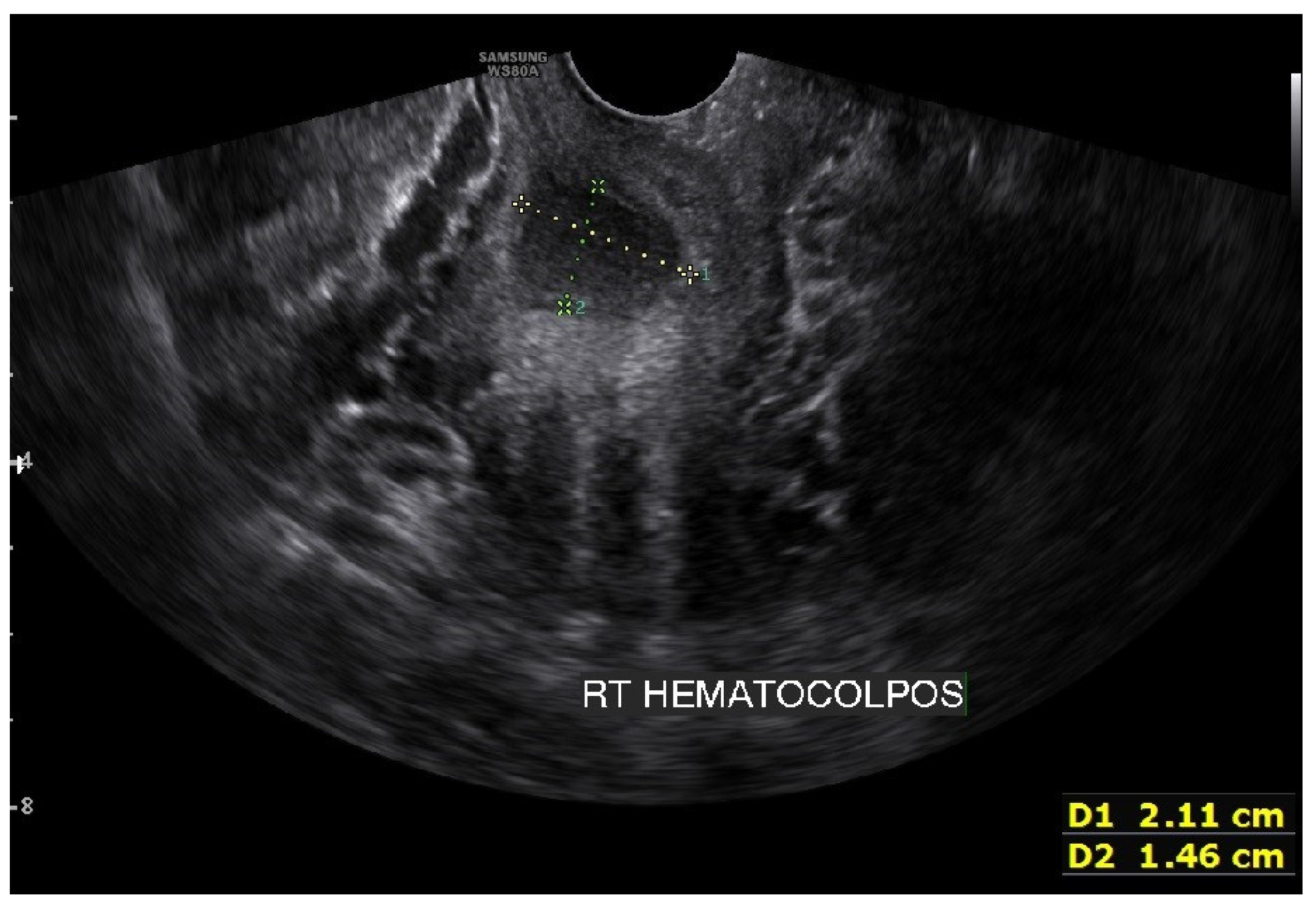
On the abdominopelvic CT image taken at the ER, we noticed she had HWW syndrome (right side hemi-vagina and right kidney agenesis) with acute pyelonephritis (APN) of the left kkidne (Figure 3a,b). After admission, transvaginal USG (Figure 4) and pelvic MRI (Figure 5a–c) were performed. We planned to perform the vaginal wall resection surgery on the next menstrual period as she needed antibiotics treatment for the APN, and the amount of hematocolpos was not so extensive that we could not clearly identify the bulging vaginal wall.
One month later, three days before the planned operation, the patient again visited ER due to severe lower pelvic pain. This time we were able to identify the bulging vaginal wall using a vaginal speculum exam and transvaginal USG (Figure 6a,b).
During surgery, we made a circular incision of 3 cm diameter on the bulging wall (Figure 7a) and removed the hematoma. Marsupialization was perfomed with vicryl (Figure 7b). The patient reported immediate relief from pain after recovery from the general anesthesia.
The patient has experienced regular menstruation without any pain after the surgery for two months so far.
3. Discussion
After Purslow first reported uterus didelphys with obstructed hemivagina in a case of unilateral hematocolpos, hematometra, and mematosalpinx in 1922, Herlyn and Werner named the obstructed hemi-vagina ipsilateral renal agenesis Herlyn-Werner syndrome in 1971. Wunderlich identified the relationship between the two syndromes and named it HWW syndrome in 1976. It is also called OHVIRA syndrome: obstructive hemi-vagina and ipsilateral renal anomaly syndrome [1,2].
Patients with HWW syndrome often experience dysmenorrhea and/or pelvic pain after menarche, with possible vaginal or pelvic mass as a result of hematometrocolpos. In 2006, Gholoum et al. reported 12 cases of HWW syndrome between 1982 and 2004, and 10 out of 12 patients exhibited classic symptoms of abdominal pain with pelvic mass [5].
We assumed that the abdominal pain of our two cases resulted from hematocolpos, similar to the pain of patients with an imperforate hymen. However, unlike imperforate hymen cases, the diagnosis of hematocolpos can be delayed because patients present with menstruations beforehand.
Pelvic USG and abdominopelvic CT are useful diagnostic tools. Pelvic MRI is strongly recommended as it provides thorough information on the shape of the uterus, vaginal cavity and vaginal septum [6]. In case 1, the obstructed hemi-vagina was more easily identified on MRI than CT images.
In South Korea, unmarried women with no previous history of coitus are reluctant to visit a Gynecology clinic. This is thought to be one of the reasons why the diagnosis was made at a relatively older age in case 1. Another reason is that she had oligomenorrhea, so the amount of blood forming hematocolpos was small, and the menstruation was irregular, so the patient did not think the pain was ‘periodic’. As stated above, pelvic mass is easily found in HWW syndrome patients [5], but if physicians or radiologists are unaware of the syndrome, they may make incorrect diagnosis such as hemorrhagic corpus luteal cyst or endometrioma and plan for an inappropriate procedure such as diagnostic laparoscopy.
The patient in case 2 had met numerous doctors, but each doctor was provided with only a segment of information. The doctor who took the abdominopelvic CT one year ago was clearly not aware of HWW syndrome, so the integrated diagnosis was delayed. This is why clinicians should be aware of the disease so that patients suffer for a shorter period of their lives.
The patient in case 2 had previously experienced multiple episodes of APN and pelvic inflammatory disease (PID). The consequent regurgitation of menstrual blood might be related to higher prevalence of a genitourinary tract infection [7]. More supporting evidence needs to be collected.
The patient in case 2 was younger in age and had severer symptoms than the patient in case 1. We believe that what made the difference was that the patient in case 2 was sexually active and had a heavier amount of menstrual bleeding.
During the operation, we noticed menstrual bleeding with a significant foul odor which was considered to be the result of blood retained in the pelvic cavity, endometrial cavity and obstructed hi-vagina for a long period of time.
Delayed diagnosis of the HWW syndrome can cause PID, tubo-ovarian abscess, endometriosis, or even infertility, so it is essential to make the diagnosis at as early an age as possible and apply surgical treatment involving vaginal septum removal and marsupialization [3,4].
We recommend that physicians offer HWW syndrome as a differential diagnosis when they see a young woman with abdominal pain with uterus didelphys, and perform abdominopelvic CT to determine whether the patient has obstructed hemivagina with ipsilateral kidney agenesis.
Author Contributions
Conceptualization, D.J. and J.-A.H.; methodology, D.J. and J.-A.H.; software, H.S.H.; validation, D.J., H.S.H. and J.-A.H.; formal analysis, D.J.; investigation, D.J. and J.-A.H.; resources, H.S.H. and J.-A.H.; data curation, D.J. and J.-A.H.; writing—original draft preparation, D.J. and J.-A.H.; writing—review and editing, D.J., H.S.H. and J.-A.H.; visualization, J.-A.H.; supervision, H.S.H.; project administration, D.J.; funding acquisition, D.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of of Soonchunhyang University Gumi Hospital (IRB No, 2022-20, 28 December 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Orazi, C.; Lucchetti, M.C.; Schingo, P.M.; Marchetti, P.; Ferro, F. Herlyn-Werner-Wunderlich syndrome: Uterus didelphys, blind hemivagina and ipsilateral renal agenesis. Sonographic and MR findings in 11 cases. Pediatr. Radiol. 2007, 37, 657–665. [Google Scholar] [CrossRef]
- Karaca, L.; Pirimoglu, B.; Bayraktutan, U.; Ogul, H.; Oral, A.; Kantarci, M. Herlyn-Werner-Wunderlich syndrome: A very rare urogenital anomaly in a teenage girl. J. Emerg. Med. 2015, 48, e73–e75. [Google Scholar] [CrossRef]
- Smith, N.A.; Laufer, M.R. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: Management and follow-up. Fertil. Steril. 2007, 87, 918–922. [Google Scholar] [CrossRef]
- Zurawin, R.K.; Dietrich, J.E.; Heard, M.J.; Edwards, C.L. Didelphic uterus and obstructed hemivagina with renal agenesis: Case report and review of the literature. J. Pediatr. Adolesc. Gynecol. 2004, 17, 137–141. [Google Scholar] [CrossRef]
- Gholoum, S.; Puligandla, P.S.; Hui, T.; Su, W.; Quiros, E.; Laberge, J.M. Management and outcome of patients with combined vaginal septum, bifid uterus, and ipsilateral renal agenesis (Herlyn-Werner-Wunderlich syndrome). J. Pediatr. Surg. 2006, 41, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Carrington, B.M.; Hricak, H.; Nuruddin, R.N.; Secaf, E.; Laros, R.K., Jr.; Hill, E.C. Mullerian duct anomalies: MR imaging evaluation. Radiology 1990, 176, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Carlson, R.L.; Garmel, G.M. Didelphic uterus and unilaterally imperforate double vagina as an unusual presentation of right lower-quadrant abdominal pain. Ann. Emerg. Med. 1992, 21, 1006–1008. [Google Scholar] [CrossRef]
Figure 1.
(a) Coronal view of abdominopelvic CT image suggesting Herlyn-Werner-Wunderlich syndrome. Uterine didelphys, hematocolpos of obstructed hemi-vagina, and ipsilateral renal agenesis are noted with white arrows.; (b) Coronal view of pelvic MRI T1-weighted image suggesting Herlyn-Werner-Wunderlich syndrome. Uterine didelphys and hematocolpos are noted with white arrows.
Figure 1.
(a) Coronal view of abdominopelvic CT image suggesting Herlyn-Werner-Wunderlich syndrome. Uterine didelphys, hematocolpos of obstructed hemi-vagina, and ipsilateral renal agenesis are noted with white arrows.; (b) Coronal view of pelvic MRI T1-weighted image suggesting Herlyn-Werner-Wunderlich syndrome. Uterine didelphys and hematocolpos are noted with white arrows.

Figure 2.
(a) Intraoperative image of bulging vaginal septum of left side (in the white circle); (b) Intraoperative hysteroscopic image after removal of vaginal septum and marsupialization (left vaginal cavity is noted with arrow).
Figure 2.
(a) Intraoperative image of bulging vaginal septum of left side (in the white circle); (b) Intraoperative hysteroscopic image after removal of vaginal septum and marsupialization (left vaginal cavity is noted with arrow).

Figure 3.
Abdominopelvic CT images. (a) Axial view showing the two uterine corpuses (indicated with white arrows); (b) Coronal view suggesting Herlyn-Werner-Wunderlich syndrome. White thick arrow; agenesis of right kidney. White thin arrow; hematocolpos of obstructed hemi-vagina connected with right endometrial cavity.
Figure 3.
Abdominopelvic CT images. (a) Axial view showing the two uterine corpuses (indicated with white arrows); (b) Coronal view suggesting Herlyn-Werner-Wunderlich syndrome. White thick arrow; agenesis of right kidney. White thin arrow; hematocolpos of obstructed hemi-vagina connected with right endometrial cavity.

Figure 4.
Transvaginal ultrasonogram image showing approximately 21 mm × 15 mm of fluid collection in the right side obstructed hemivagina. This suggested hematocolpos on the right side was too small and made it difficult to operate on the first visit.
Figure 4.
Transvaginal ultrasonogram image showing approximately 21 mm × 15 mm of fluid collection in the right side obstructed hemivagina. This suggested hematocolpos on the right side was too small and made it difficult to operate on the first visit.

Figure 5.
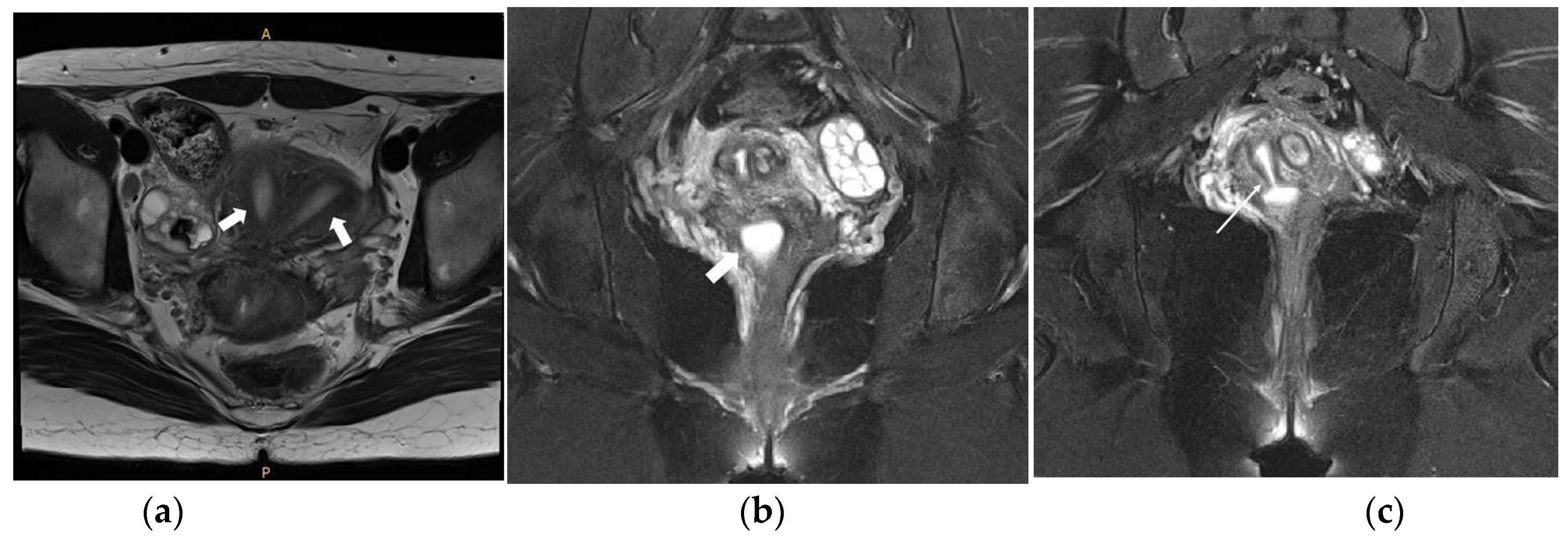
Pelvic MRI images. (a) Axial view T2-weighted image showing the two uterine corpuses (indicated with two white arrows); (b) Coronal view T2-weighted image showing the small cystic mass filled with fluid suggesting hematocolpos on the right side (indicated with a white arrow); (c) Coronal view T2-weighted image showing the hematocolpos connected with the right endometrial cavity (indicated with a white arrow).
Figure 5.
Pelvic MRI images. (a) Axial view T2-weighted image showing the two uterine corpuses (indicated with two white arrows); (b) Coronal view T2-weighted image showing the small cystic mass filled with fluid suggesting hematocolpos on the right side (indicated with a white arrow); (c) Coronal view T2-weighted image showing the hematocolpos connected with the right endometrial cavity (indicated with a white arrow).

Figure 6.
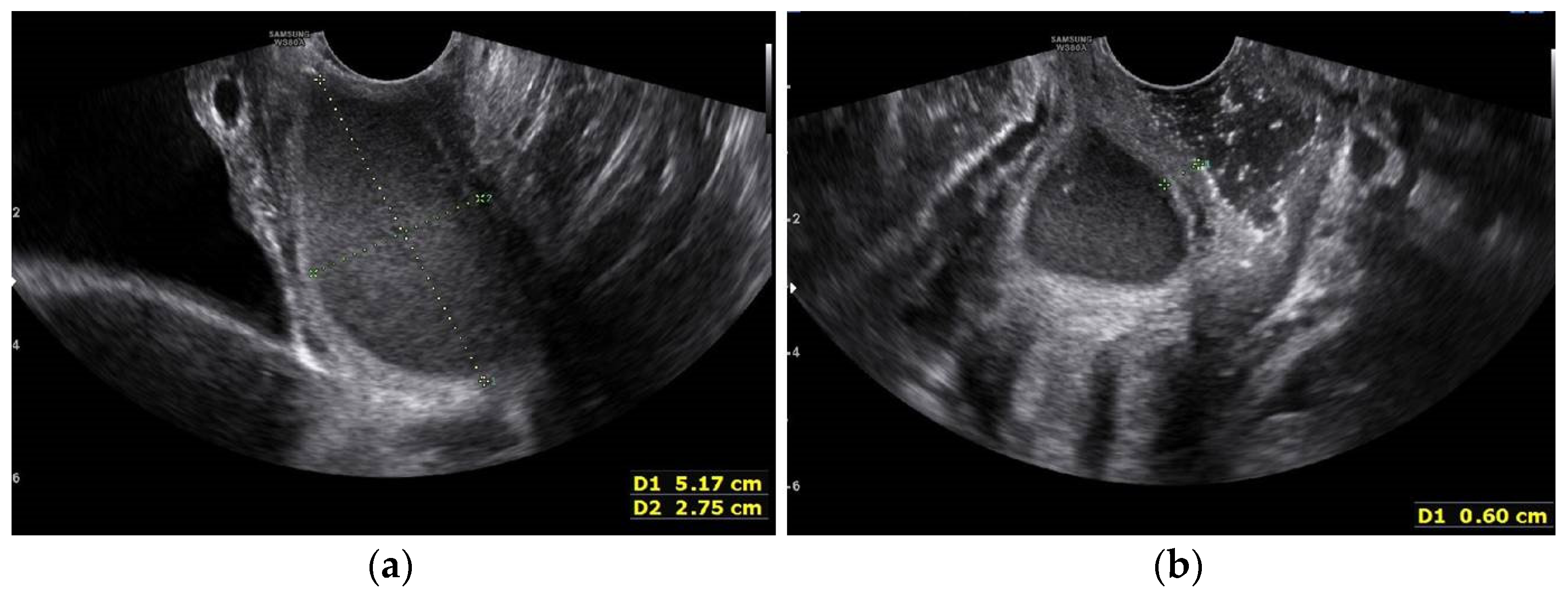
Transvaginal USG image one month after the initial visit. (a) More substantial fluid collection in the right side obstructed hemi-vagina; (b) Transvaginal ultrasonogram image showing the thickness of the vaginal septum to be approximately 6 mmn (measured with +calipers).
Figure 6.
Transvaginal USG image one month after the initial visit. (a) More substantial fluid collection in the right side obstructed hemi-vagina; (b) Transvaginal ultrasonogram image showing the thickness of the vaginal septum to be approximately 6 mmn (measured with +calipers).

Figure 7.
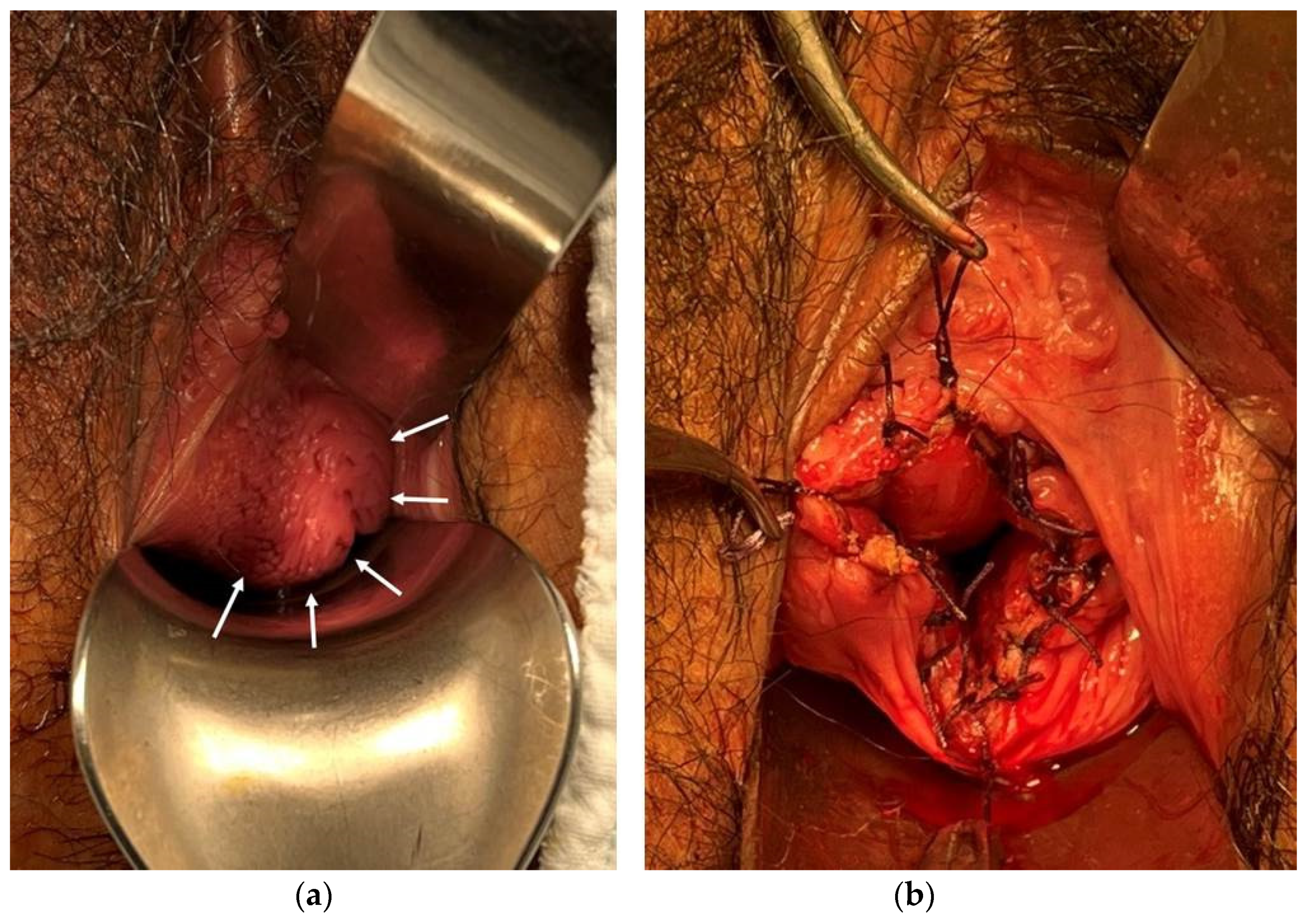
Intraoperative image. (a) Bulging vaginal septum of right side (indicated with white arrows); (b) After removal of vaginal septum and marsupialization.
Figure 7.
Intraoperative image. (a) Bulging vaginal septum of right side (indicated with white arrows); (b) After removal of vaginal septum and marsupialization.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Jeon, D.; Han, H.S.; Hong, J.-A. Two Cases of Herlyn-Werner-Wunderlich Syndrome with Severe Dysmenorrhea, One Misdiagnosis and One Missed Diagnosis. Surgeries 2023, 4, 10-16. https://doi.org/10.3390/surgeries4010002
AMA Style
Jeon D, Han HS, Hong J-A. Two Cases of Herlyn-Werner-Wunderlich Syndrome with Severe Dysmenorrhea, One Misdiagnosis and One Missed Diagnosis. Surgeries. 2023; 4(1):10-16. https://doi.org/10.3390/surgeries4010002
Chicago/Turabian StyleJeon, Dongsoo, Hyo Sang Han, and Jeong-A Hong. 2023. "Two Cases of Herlyn-Werner-Wunderlich Syndrome with Severe Dysmenorrhea, One Misdiagnosis and One Missed Diagnosis" Surgeries 4, no. 1: 10-16. https://doi.org/10.3390/surgeries4010002