
Surgical Lip Cancer Reconstruction in the COVID-19 Era: Are Free Flaps or Loco-Regional Flaps Better?
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Reconstructive Strategies
3.2. Surgical Length
3.3. Hospitalization Time
3.4. ICU Stay
3.5. Post Operative Complications
4. Discussion
4.1. Surgical Techniques for Malignant Tumors of the Lips
- Webster flap: allows the reconstruction of the lateral third of the lip but leads to lip regression with microstomia and modifications of the labial commissure [15].
- Nasogenian flap: this flap allows an extended repair towards the midline. It can be used to perform a complete reconstruction of the superior lip.
- Abbé flap: this flap is advantageous because it preserves the sphincter function of the mouth with aesthetically pleasing results.
- Estlander flap: it is similar to the Abbé flap but used to reconstruct lateral juxta commissural defects. For this reason, it is also referred to as Abbé-Estlander. The point of rotation of the flap will function as the new commissure, which will be subject to commissuroplasty in order to increase opening.
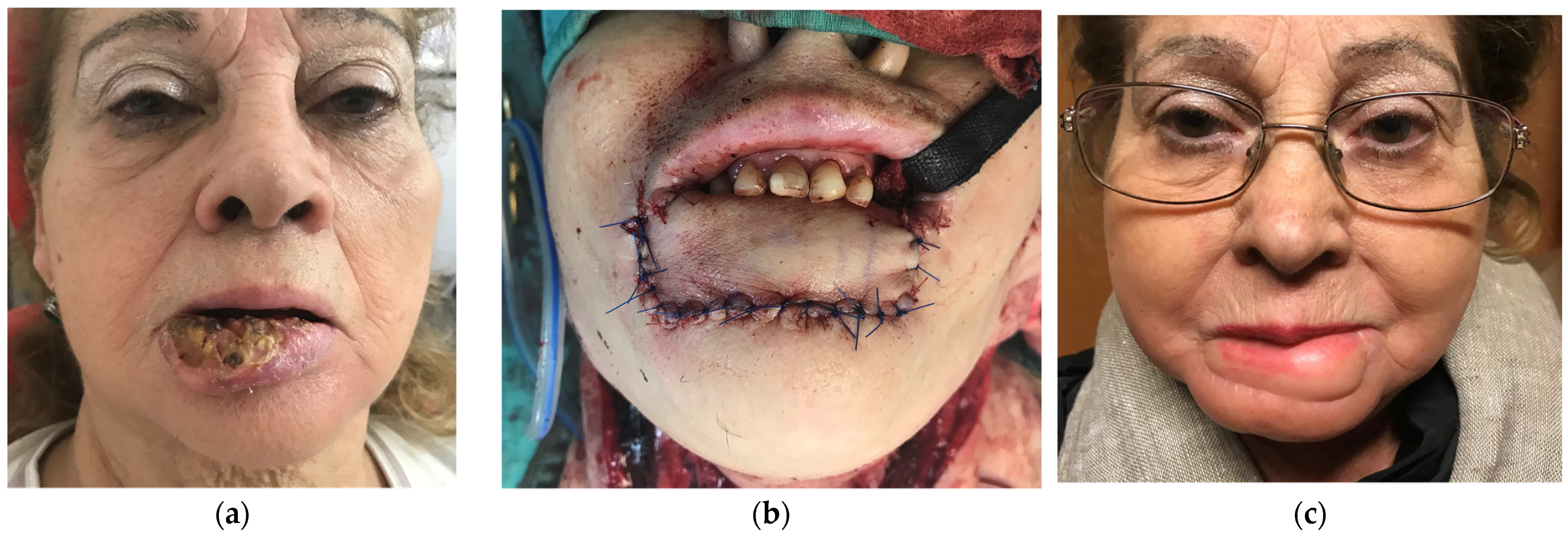
- Karapandzic flap: it is similar to the fan flap of Gillies, but in contrast to it, the mucosa is preserved, thus not being a full-thickness incision. This technique can be unilateral or bilateral.
- Gillies flap: it can be used for total upper lip reconstructions. This guarantees good functionality, but, on the other hand, it leads to microstomia [17].
- Abbé-Estlander flap: the technique is the same as that used for upper lip reconstruction.
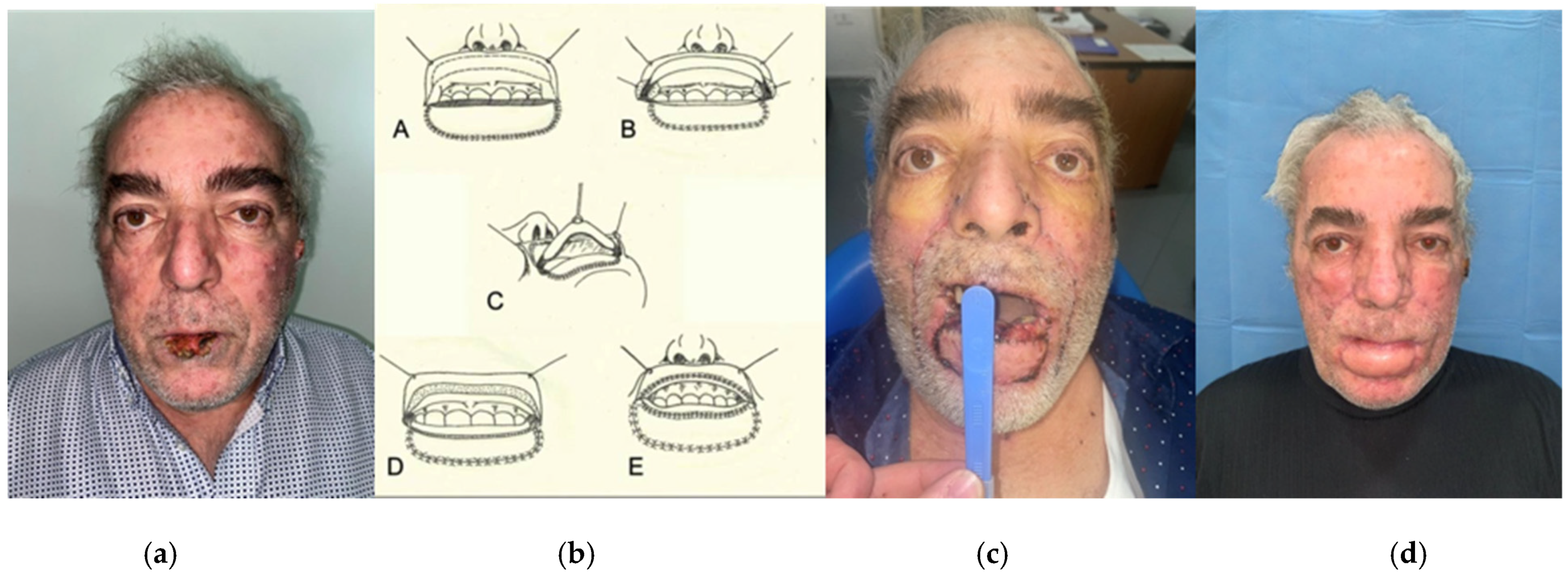
- Johanson step technique: used for the reconstruction of defects measuring at least 2 cm. This technique preserves sphincteric function and lip vascularization, but it is associated with microstomia [18].
- Gillies fan flap: it is a full-thickness, quadrangular flap that is moved as a fan around the juxta commissural region up to the defect. This is followed by commissuroplasty [17].
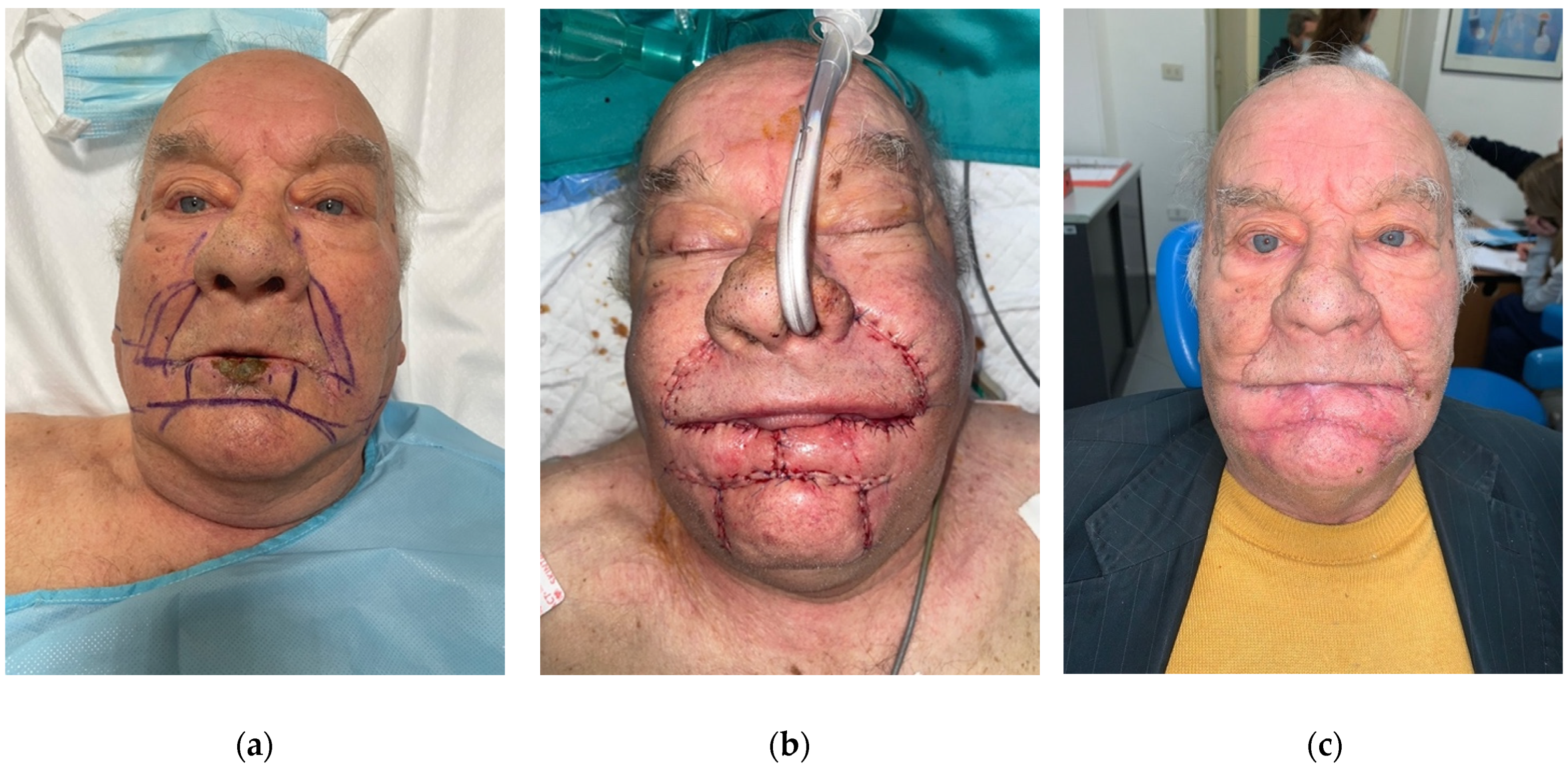
- Camille Bernard flap: this technique consists of two advancement malar flaps that used to repair the entire lower lip. In elderly patients, this procedure is facilitated by the laxity of the tissues. The functional results of this flap are mediocre: the inferior lip tends to regress, there is malocclusion, and loss of saliva from the mouth [19].
- Modified Camille Bernard flap: Webster modified the aforementioned technique in order to ameliorate the functional aspect. As mentioned, this technique leads to better functional outcomes, but there is still insufficient labial competence with important lower lip retraction. Moreover, it is often possible for the upper lip to be projected outward. Few techniques can compensate for this complication. One possible option is represented by placing a thick tongue flap to reconstruct the vermilion.
4.2. Lip Reconstruction in the COVID-19 Era
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lewis, A. Cummings Otolaryngology: Head and Neck Surgery, Fourth Edition. Head Neck 2007, 29, 522. [Google Scholar] [CrossRef]
- Pelo, S.; lo Muzio, L. IL Carcinoma Orale; GRILLIEDITORE: Manfredonia, Italy, 2009; Volume 1. [Google Scholar]
- Bessede, J.-P.; Sannajust, J.-P.; Vergnolles, V. Chirurgia Dei Tumori Delle Labbra. EMC Tec. Chir. Chir. ORL Cerv. Facc. 2007, 11, 1–22. [Google Scholar] [CrossRef]
- Gruppo di Lavoro, I.S.S. Prevenzione e Controllo delle Infezioni. In Rapporto ISS COVID-19—n. 2/2020 Rev.; Istituto Superiore di Sanità: Rome, Italy, 2020. [Google Scholar]
- Armocida, B.; Formenti, B.; Ussai, S.; Palestra, F.; Missoni, E. The Italian Health System and the COVID-19 Challenge. Lancet Public Health 2020, 5, e253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, M. COVID-19: Italy Confirms 11 Deaths as Cases Spread from North. BMJ 2020, 368, m757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuite, A.R.; Ng, V.; Rees, E.; Fisman, D. Estimation of COVID-19 Outbreak Size in Italy. Lancet Infect. Dis. 2020, 20, 537. [Google Scholar] [CrossRef] [Green Version]
- Day, A.T.; Sher, D.J.; Lee, R.C.; Truelson, J.M.; Myers, L.L.; Sumer, B.D.; Stankova, L.; Tillman, B.N.; Hughes, R.S.; Khan, S.A.; et al. Head and Neck Oncology during the COVID-19 Pandemic: Reconsidering Traditional Treatment Paradigms in Light of New Surgical and Other Multilevel Risks. Oral Oncol. 2020, 105, 104684. [Google Scholar] [CrossRef]
- Deo, S.V.S.; Kumar, S.; Kumar, N.; Saikia, J.; Bhoriwal, S.; Bhatnagar, S.; Sharma, A. Guiding Principles for Cancer Surgery during the COVID-19 Pandemic. Indian J. Surg. Oncol. 2020, 11, 3–10. [Google Scholar] [CrossRef]
- Colella, G.; Rauso, R.; de Cicco, D.; Boschetti, C.E.; Iorio, B.; Spuntarelli, C.; Franco, R.; Tartaro, G. Clinical Management of Squamous Cell Carcinoma of the Tongue: Patients Not Eligible for Free Flaps, a Systematic Review of the Literature. Expert Rev. Anticancer. Ther. 2021, 21, 9–22. [Google Scholar] [CrossRef]
- Direzione Generale Della Programmazione Sanitaria. Linee di Indirizzo per la Rimodulazione dell’attività Programmata Differibile in Corso di Emergenza da COVID-19; Ministero della Salute Italiano: Rome, Italy, 2020. [Google Scholar]
- Susarla, S.M.; Parmar, S.; Fernandes, R. COVID-19 and the Craniomaxillofacial Surgical Community. Craniomaxillofacial Trauma Reconstr. 2020, 13, 83. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.; Su, T.; Huang, L. Strategic Plan for Management in Oral and Maxillofacial Surgery during COVID-19 Epidemic. Oral Oncol. 2020, 105, 104715. [Google Scholar] [CrossRef]
- Valentini, V.; Pucci, R.; Battisti, A.; Cassoni, A. Head and Neck Cancer Cannot Wait for This Pandemic to End: Risks, Challenges and Perspectives of Oral-Maxillofacial Surgeon during COVID-19. Oral Oncol. 2020, 106, 104758. [Google Scholar] [CrossRef]
- Webster, J.P. Crescentic Peri-Alar Cheek Excision for Upper Lip Flap Advancement with a Short History of Upper Lip Repair. Plast. Reconstr. Surg. 1946, 16, 434–464. [Google Scholar] [CrossRef]
- Smith, P.G.; Muntz, H.R.; Thawley, S.E. Local Myocutaneous Advancement Flaps Alternatives to Cross-Lip and Distant Flaps in the Reconstruction of Ablative Lip Defects. Arch. Otolaryngol. 1982, 108, 714–718. [Google Scholar] [CrossRef]
- Papgs. The Gillies Fan Flap. Restoration of Substance for Partial Loss of Upper Lip (Case Report). Acta Chir. Plast. 1969, 11, 210–213. [Google Scholar]
- Johanson, B.; Aspelund, E.; Breine, U.; Holmström, H. Surgical Treatment of Non-Traumatic Lower Lip Lesions with Special Reference to the Step Technique: A Follow-up on 149 Patients. Scand. J. Plast. Reconstr. Surg. 1974, 8, 232–240. [Google Scholar] [CrossRef]
- Moulonguet, P. Amputation of the Lip and Cheiloplasty According to the Camille Bernard Technic. J. Chir. 1954, 70, 826–830. [Google Scholar]
- Emerick, K.S. Free Flap Reconstruction of the Lip. Oper. Tech. Otolaryngol. Head Neck Surg. 2020, 31, 26–32. [Google Scholar] [CrossRef]
- Sakai, S.; Soeda, S.; Endo, T.; Ishii, M.; Uchiumi, E. A Compound Radial Artery Forearm Flap for the Reconstruction of Lip and Chin Defect. Br. J. Plast. Surg. 1989, 42, 337–338. [Google Scholar] [CrossRef] [PubMed]
- Sawhney, C.P. The Trustees of British Association of Plastic Surgeons. Br. J. Plast. Surg. 1986, 39, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Jeng, S.-F.; Kuo, Y.-R.; Wei, F.-C.; An, P.-C.; Su, C.-Y.; Chien, C.-Y.; Taiwan, C. Free Radial Forearm Flap with Adipofascial Tissue Extension for Reconstruction of Oral Cancer Defect. Ann. Plast. Surg. 2002, 49, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, S.; Gideroğlu, K.; Aydogdu, E.; Avci, G.; Akan, M.; Aköz, T. Composite Anterolateral Thigh-Fascia Lata Flap: A Good Alternative to Radial Forearm-Palmaris Longus Flap for Total Lower Lip Reconstruction. Plast. Reconstr. Surg. 2006, 117, 2033–2041. [Google Scholar] [CrossRef]
- Lin, Y.S.; Liu, W.C.; Lin, Y.S.; Chen, L.W.; Hsueh, J.H.; Yang, K.C. Double-Paddle Peroneal Flap for Extensive Lip Defect Reconstruction. Microsurgery 2017, 37, 558–563. [Google Scholar] [CrossRef]
- Bhama, P.K.; Weinberg, J.S.; Lindsay, R.W.; Hohman, M.H.; Cheney, M.L.; Hadlock, T.A. Objective Outcomes Analysis Following Microvascular Gracilis Transfer for Facial Reanimation: A Review of 10 Years’ Experience. JAMA Facial Plast. Surg. 2014, 16, 85–92. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Greenspan, J.S. Epidemiology of Oral and Oropharyngeal Cancers. In Textbook of Oral Cancer; Springer: Berlin/Heidelberg, Germany, 2020; Volume 1, pp. 5–21. [Google Scholar]
- de Cicco, D.; Tartaro, G.; Ciardiello, F.; Fasano, M.; Rauso, R.; Fiore, F.; Spuntarelli, C.; Troiano, A.; lo Giudice, G.; Colella, G. Health-Related Quality of Life in Oral Cancer Patients: Scoping Review and Critical Appraisal of Investigated Determinants. Cancers 2021, 13, 4398. [Google Scholar] [CrossRef]
- Sipido, K.R.; Antoñanzas, F.; Celis, J.; Degos, L.; Frackowiak, R.; Fuster, V.; Ganten, D.; Gay, S.; Hofstraat, H.; Holgate, S.T.; et al. Overcoming Fragmentation of Health Research in Europe: Lessons from COVID-19. Lancet 2020, 395, 1970–1971. [Google Scholar] [CrossRef]
- World Health Organization. Updated Country Preparedness and Response Status for COVID-19 as of 9 June 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- COVIDSurg Collaborative; Nepogodiev, D.; Bhangu, A. Elective Surgery Cancellations Due to the COVID-19 Pandemic: Global Predictive Modelling to Inform Surgical Recovery Plans. Br. J. Surg. 2020, 107, 1440–1449. [Google Scholar] [CrossRef]
- Gray, M.L.; Drake, V.E.; Desai, S.C. Resurgence of Regional Flaps for Head and Neck Reconstruction. Curr. Opin. Otolaryngol. Head Neck Surg. 2021, 29, 237–243. [Google Scholar] [CrossRef]
- Desai, S.C.; Seth, R. Shifting Paradigms in Head and Neck Reconstructive Surgery During the COVID-19 Crisis. Facial Plast. Surg. Aesthetic Med. 2020, 22, 152–154. [Google Scholar] [CrossRef]
- Shokri, T.; Saadi, R.A.; Liaw, J.; Bann, D.V.; Patel, V.A.; Goyal, N.; Lighthall, J.G. Facial Plastic and Reconstructive Surgery During the COVID-19 Pandemic: Implications in Craniomaxillofacial Trauma and Head and Neck Reconstruction. Ann. Plast. Surg. 2020, 85, S166–S170. [Google Scholar] [CrossRef]
- Pradhan, P.; Preetam, C.; Parida, P.K.; Samal, D.K. Changing Trend in the Management of Head Neck Cancers during the COVID-19 Pandemic. Eur. Arch. Otorhinolaryngol. 2022, 279, 1453–1460. [Google Scholar] [CrossRef]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.L. The Reconstruction of Two Large Full-Thickness Wounds of the Upper Lip with Different Operative Techniques: When Possible, a Local Flap Repair is Preferable to Reconstruction with Free Tissue Transfer. Dermatol. Surg. 2013, 39, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Urushidate, S.; Yokoi, K.; Higuma, Y.; Mikami, M.; Watanabe, Y.; Saito, M.; Saito, Y.; Yamauchi, M.; Yotsuyanagi, T. New Way to Raise the V-Y Advancement Flap for Reconstruction of the Lower Lip: Bipedicled Orbicularis Oris Musculocutaneous Flap Technique. J. Plast. Surg. Hand Surg. 2011, 45, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Dadhich, A.; Shah, S.; Saluja, H.; Tandon, P.; More, V. Karapandzic Flap for Esthetic and Functional Reconstruction of Large Defect of Lower Lip. Ann. Maxillofac. Surg. 2017, 7, 300. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, A.; Maghsoudnia, G.R.; Arshadi, A.A. Prospective Comparative Study of Lower Lip Defects Reconstruction with Different Local Flaps. J. Craniofac. Surg. 2011, 22, 2255–2259. [Google Scholar] [CrossRef]
- Coppit, G.L.; Lin, D.T.; Burkey, B.B. Current Concepts in Lip Reconstruction. Curr. Opin. Otolaryngol. Head Neck Surg. 2004, 12, 281–287. [Google Scholar] [CrossRef]
- Fujimori, R. “Gate Flap” for the Total Reconstruction of the Lower Lip. Br. J. Plast. Surg. 1980, 33, 340–345. [Google Scholar] [CrossRef]
- Gupta, S.; Chattopadhyay, D.; Murmu, M.B.; Gupta, S.; Singh, H.S. A New Technique for One-Stage Total Lower Lip Reconstruction: Achieving the Perfect Balance. Can. J. Plast. Surg. 2013, 21, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimi, A.; Kalantar Motamedi, M.H.; Ebrahimi, A.; Kazemi, M.; Shams, A.; Hashemzadeh, H. Lip Reconstruction after Tumor Ablation. World J. Plast. Surg. 2016, 5, 15–25. [Google Scholar]
- Ozdemir, R.; Ortak, T.; Koçer, U.; Celebioğlu, S.; Sensöz, O.; Tiftikcioglu, Y.O. Total Lower Lip Reconstruction Using Sensate Composite Radial Forearm Flap. J. Craniofac. Surg. 2003, 14, 393–405. [Google Scholar] [CrossRef]
- Shaikh, A.I.; Khan, A.H.; Tated, S.; Khubchandani, N. Functional and Aesthetic Outcome of Different Methods of Reconstruction of Full Thickness Lip Defects. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2022, 11, Doc02. [Google Scholar] [CrossRef]
- Bo, Q.; Lu, J.; Wang, Y.; Hu, Y.; Tang, S.; Yang, B. Application of Local Flaps in Repairing Total and Near-Total Lower Lip Defects of Young Patients. J. Craniofac. Surg. 2021, 32, 1860–1863. [Google Scholar] [CrossRef]
- Cakmak, M.A.; Cinal, H.; Barin, E.Z.; Sakat, M.S.; Karaduman, H.; Tan, O. Total Lower Lip Reconstruction with Functional Gracilis Free Muscle Flap. J. Craniofac. Surg. 2018, 29, 735–737. [Google Scholar] [CrossRef]
- Vanison, C.; Beckmann, N.; Smith, A. Recent Advances in Lip Reconstruction. Curr. Opin. Otolaryngol. Head Neck Surg. 2019, 27, 219–226. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Case n. | Age | Gender | Comorbidities | Diagnosis | Site | TNM | Treatment Choice |
|---|---|---|---|---|---|---|---|
| 1 | 50 | M | HTN | SCC | Lower lip involving right commisure | pT4aN0M0 | Radial Free Flap |
| 2 | 54 | M | None | SCC | Lower lip involving left commisure | pT3N1M0 | Radial Free Flap |
| 3 | 48 | M | None | SCC | Middle-lower lip | pT4aN2M0 | Radial Free Flap |
| 4 | 56 | F | HTN | SCC | Lower lip involving right commisure | pT3N0M0 | Radial Free Flap |
| 5 | 45 | M | None | SCC | Lower lip involving right commisure | pT4aN1M0 | Radial Free Flap |
| 6 | 62 | F | COPD | SCC | Lower lip involving right commisure | pT3N2M0 | Radial Free Flap |
| 7 | 52 | F | None | SCC | Lower lip involving left commisure | pT4aN1M0 | Radial Free Flap |
| 8 | 70 | M | COPD, HTN | SCC | Lower lip involving both commisures | pT4aN1M0 | Modified Camille/Bernard flap |
| 9 | 76 | M | T2D, HTN | SCC | Lower lip involving right commisure | pT3N1M0 | Bernard/Fusama flap |
| 10 | 69 | M | CAD | SCC | Lower lip involving left commisure | pT2N0M0 | Karapandzic flap |
| 11 | 54 | F | AF | SCC | Lower lip involving right commisure | pT2N0M0 | Karapandzic flap |
| 12 | 65 | F | None | SCC | Lower lip involving left commisure | pT4aN1M0 | Bernard/Fusama flap |
| 13 | 63 | M | None | Verrucous Carcinoma | Philtrum of upper lip | pT2N0M0 | Gillies flap |
| 14 | 55 | M | HTN | Verrucous Carcinoma | Right commisure | pT2N0M0 | Abbè/Staircase flap |
| 15 | 63 | M | T2D, CHF | SCC | Lower lip | pT4aN1M0 | Bernard/Gupta flap |
| 16 | 58 | F | CAD | SCC | Lower lip involving left commisure | pT3N1M0 | Karapandzic flap |
| 17 | 50 | M | None | SCC | Lower lip involving left commisure | pT3N1M0 | Modified Camille/Bernard flap |
| Locoregional Flap | Free Flap | |
|---|---|---|
| 1. Surgical Lenght | ||
| Mean | 3 h 58 min | 9 h 18 mim |
| SD | 2 h 20 min | 2 h 12 min |
| p-value | 0.0001 | |
| 2. Hospitalization time | ||
| Mean | 2.9 days | 7.14 days |
| SD | 0.8 days | 1.3 days |
| p-value | 0.0001 | |
| 3. ICU stay | ||
| Mean | 0.10 days | 1.00 days |
| SD | 0.32 days | 0.82 days |
| p-value | 0.006 | |
| Case n. | Surgical Length (h) | Hospitalisation Time (Days) | ICU (Days) | NG Tube | Tracheostomy |
|---|---|---|---|---|---|
| 1 | 7 h | 1 w | 1 d | Yes | No |
| 2 | 8 h | 6 d | None | Yes | No |
| 3 | 12 h | 1 w 1 d | 2 d | Yes | Yes |
| 4 | 7 h 30 min | 5 d | None | No | No |
| 5 | 9 h | 1 w | 1 d | Yes | Yes |
| 6 | 8 h | 1 w 1 d | 1 d | No | No |
| 7 | 10 h | 1 w 2 d | 2 d | Yes | No |
| 8 | 8 h | 4 d | 1 d | Yes | No |
| 9 | 3 h 30 min | 2 d | None | No | No |
| 10 | 4 h | 3 d | None | No | No |
| 11 | 3 h 30 min | 4 d | None | No | No |
| 12 | 3 h | 4 d | None | No | No |
| 13 | 4 h 30 min | 2 d | None | No | No |
| 14 | 2 h | 2 d | None | No | No |
| 15 | 1 h 30 min | 2 d | None | Yes | No |
| 16 | 3 h 30 min | 3 d | None | No | No |
| 17 | 2 h 20 min | 3 d | None | No | No |
| Post Operative Complications | Loco-Regional Flap | Free Flap |
|---|---|---|
| None | 6 | 4 |
| Infection | 0 | 0 |
| Orocutaneous fistula | 0 | 1 |
| Fullness or blunting of the involved oral commissure | 0 | 0 |
| Adequate mouth opening | 4 | 7 |
| Adequate blood supply | 9 | 6 |
| Adequate oral seal | 7 | 5 |
| Symmetrical mouth opening | 10 | 7 |
| Commissuroplasty | 6 | 0 |
| Wound dehiscence | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staglianò, S.; Tartaro, G.; Boschetti, C.E.; Guida, D.; Colella, G.; Rauso, R. Surgical Lip Cancer Reconstruction in the COVID-19 Era: Are Free Flaps or Loco-Regional Flaps Better? Surgeries 2023, 4, 108-119. https://doi.org/10.3390/surgeries4010012
Staglianò S, Tartaro G, Boschetti CE, Guida D, Colella G, Rauso R. Surgical Lip Cancer Reconstruction in the COVID-19 Era: Are Free Flaps or Loco-Regional Flaps Better? Surgeries. 2023; 4(1):108-119. https://doi.org/10.3390/surgeries4010012
Chicago/Turabian StyleStaglianò, Samuel, Gianpaolo Tartaro, Ciro Emiliano Boschetti, David Guida, Giuseppe Colella, and Raffaele Rauso. 2023. "Surgical Lip Cancer Reconstruction in the COVID-19 Era: Are Free Flaps or Loco-Regional Flaps Better?" Surgeries 4, no. 1: 108-119. https://doi.org/10.3390/surgeries4010012