
Talus Fractures in Snowboarders: A Case Series

Tahoe Orthopedics & Sports Medicine, Zephyr Cove, NV 89448, USA
*
Author to whom correspondence should be addressed.
Osteology 2022, 2(2), 106-111; https://doi.org/10.3390/osteology2020012
Submission received: 28 February 2022
/
Revised: 20 May 2022
/
Accepted: 23 May 2022
/
Published: 26 May 2022
(This article belongs to the Special Issue Current Trends in Foot & Ankle Surgery)
Abstract
:Fractures of the lateral process of the talus have been associated with snowboarding, so much so that they have earned the nickname “snowboarder’s ankle”; these typically occur with relatively low-energy injuries when compared with fractures of the talar head, neck, and body. We have observed that snowboarding portends a higher risk of talus fractures when compared with skiing and can include higher energy injury patterns. This study describes a series of talar head, neck, and body fractures caused by snowboarding, their treatment, and outcomes. A retrospective chart review was performed on all surgical cases collected from 2007 to 2012 to include talar head, neck, body, or lateral process fractures sustained while snowboarding. Radiographs were reviewed and the fractures were characterized. Questionnaires, including the Foot and Ankle Disability Index (FADI), were mailed to the patients. The pre-operative reports, surgical treatments, and outcomes were evaluated. Nine patients were identified with fractures of the talus caused by a snowboarding injury. One patient sustained an isolated talar head fracture, three sustained isolated talar neck fractures, one patient had an isolated talar body fracture, and two patients had isolated lateral process fractures. Two patients had a combination of talar injuries. At 2.5 years mean follow-up (range 6 months to 5 years), none of the patients developed avascular necrosis, nonunion/malunion, or required subsequent surgery. FADI scores indicated good to excellent results post-operatively.
1. Introduction
Snowboarding continues to be a popular winter sport in the United States, with approximately 7.5 million people participating annually over the previous decade [1]. The modern snowboard entered the mainstream in the early 1970s after technical advances were designed by Jake Burton and Tom Sims [2]. Snowboarders ride downhill standing perpendicular to a single board with both feet fixed in position by non-releasable bindings. After becoming an Olympic sport in 1998, increased participation in snowboarding led to the evolution of new injuries [3]. With both feet attached to a single board, the natural reaction during a fall is to protect oneself with outstretched arms [4]. Previously published data comparing snowboarding with alpine skiing injuries demonstrated that snowboarding accidents were typically less severe and showed significantly different injury patterns [5,6]. More upper extremity injuries were observed, specifically to the wrist [3,4,5,6].
Lower extremity injuries from snowboarding, specifically of the foot and ankle, stem from high-energy impacts. Of note is the recognition of fractures of the lateral process of the talus, referred to as “snowboarder’s ankle”, a fracture pattern previously thought to be rare [2]. The talus is the second largest tarsal bone, with approximately 60% covered by articular cartilage [7]. The talus vascular supply is formed by a network of anastomoses with contributions from the posterior tibial artery, the anterior tibial (dorsalis pedis) artery, and the perforating peroneal artery [8]. Knowledge of the blood supply is important when operating on talar fractures to minimize soft tissue stripping and damage to the blood supply, thus minimizing the potential for avascular necrosis.
The mechanism of injury for lateral process fractures has been described as dorsiflexion of the ankle and inversion of the hindfoot [2,9]. This fracture commonly occurs in snowboarders in the leading foot during a jump or an aerial maneuver [10]. In contrast, head, neck, and body talus fractures have been described in high-energy traumas such as falls from height or motor vehicle accidents [9]. These injuries can be difficult to diagnose on plain radiographs; therefore, computerized tomography (CT) imaging is needed for an accurate diagnoses and treatments [11,12,13]. In most cases, open reduction internal fixation (ORIF) is performed to obtain anatomic reduction in these complex fractures [14].
This study describes a series of patients with talar fractures secondary to snowboarding trauma that were surgically treated. Awareness of these injury patterns can lead to more rapid diagnoses and treatments with the goal of improved patient care.
2. Materials and Methods
This study was approved by the Barton Institutional Review Board (IRB), #11-108. A retrospective chart review was performed on all cases with a diagnosis of talar head, neck, body, or lateral process fractures from 2007 to 2012. Age, type of injury, date of operative procedure, and gender information were taken directly from the medical record (Table 1). Foot and Ankle Disability Index (FADI) outcome questionnaires were utilized to assess functional limitations related to foot and ankle conditions. The FADI outcome assessment has 26 items and a total score of 104, which represents no dysfunction (https://www.orthopaedicscore.com/scorepages/foot_and_ankle_disability_index_fadi.html (accessed on 1 May 2013)). IRB-approved consent forms were mailed to the patients identified with a diagnosis of talar head, neck, body, or lateral process fractures. Telephone interviews were attempted with all patients.
Initial patient evaluations were performed by emergency room physicians. Imaging studies (plain radiographs, computed tomography (CT) scans, or both) were reviewed by the consulting orthopedic surgeon. Three senior surgeons were involved in the care of these patients. Surgical fixation was determined by the consulted surgeon based on the fracture pattern. Typically, plates were used for more comminuted fractures, whereas cannulated screws were used for more length-stable patterns.
Surgical treatment was dictated by injury pattern and chosen by the treating surgeon. The surgical approach consisted of four cases with both medial and lateral incisions, two cases with lateral approach alone, one case with medial approach alone, and one case with a medial malleolar osteotomy followed by plate fixation and percutaneous posterior to anterior fixation. One case was diagnosed in a delayed fashion, and this treatment consisted of medial external fixation in the talus and percutaneous K-wires for the concomitant talonavicular dislocation. A tourniquet was used for all procedures. Post-operative treatment consisted of non-weight-bearing for approximately 12 weeks, followed by gradual progression of weight-bearing when the fractures demonstrated radiographic healing. Sequential follow-up was limited because six of the patients elected to follow-up near their hometown, which was a significant distance from our facility.
3. Results
We identified nine patients in which the cause of talus fracture was snowboarding. Patient information is listed in Table 1. Five of the nine patients had operative fixation on the same day of injury, whereas the remaining four were delayed because they were initially seen at alternate facilities and referred to our facility for definitive treatment. Of the four patients with delayed treatment, the surgeries were then completed 1 day, 1 week (2 patients), and 3 weeks following the original injuries.
Mean time of follow-up from the time of the surgery was 2.5 years (range 6 months to 5 years). The mean FADI score was 87.6 (range 84 to 92.5). Of the patients who completed the questionnaire, all fractures occurred in the leading leg: left leg if riding goofy (left foot forward), right leg if riding regular (right foot forward).
Three of the four patients who completed the FADI questionnaire had no pain at rest, although two of the four did have mild pain in general, and one experienced moderate pain. Four of the patients had slight difficulty with descending stairs and walking on uneven ground. Three had slight difficulty, and one patient had moderate difficulty coming up to their toes. Three of the four also had slight difficulty with heavy work and recreational activities.
None of these patients developed avascular necrosis or required further operative procedures, and all were able to return to work. One patient developed wound drainage six weeks post-operatively, which resolved with oral antibiotics and local wound care seven weeks post-operatively. In this study, same-day operative fixation did not appear to affect the development of wound complications. The mean surgical tourniquet time was 91 min. There were no open fractures in this series.
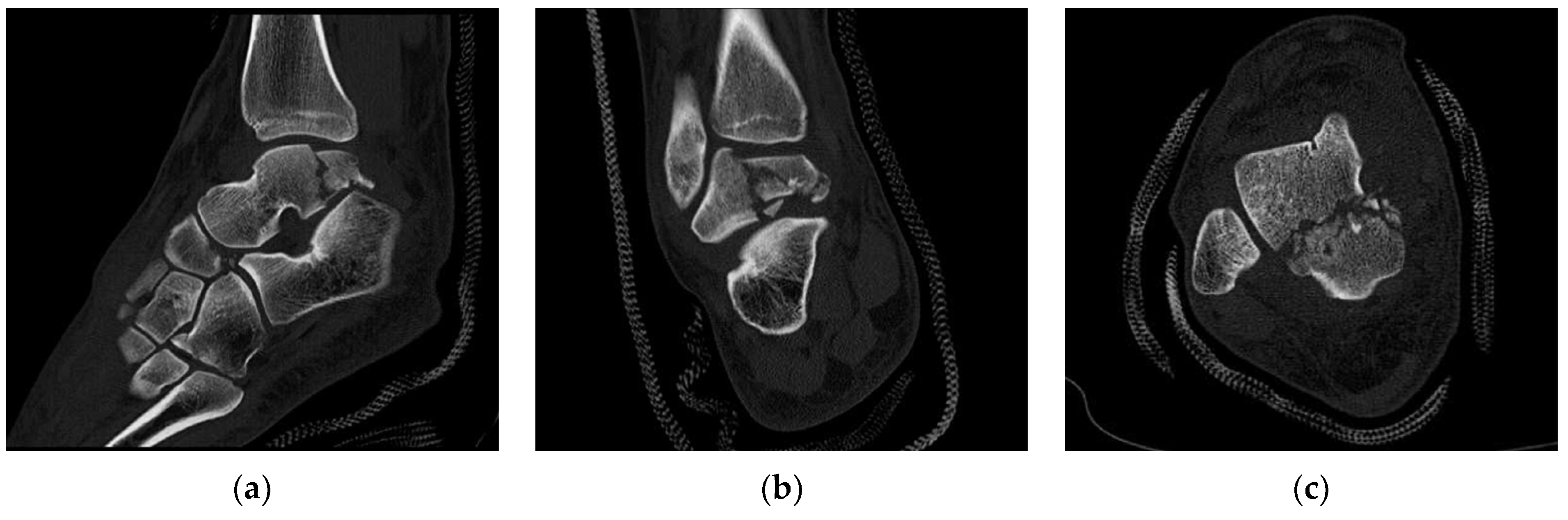
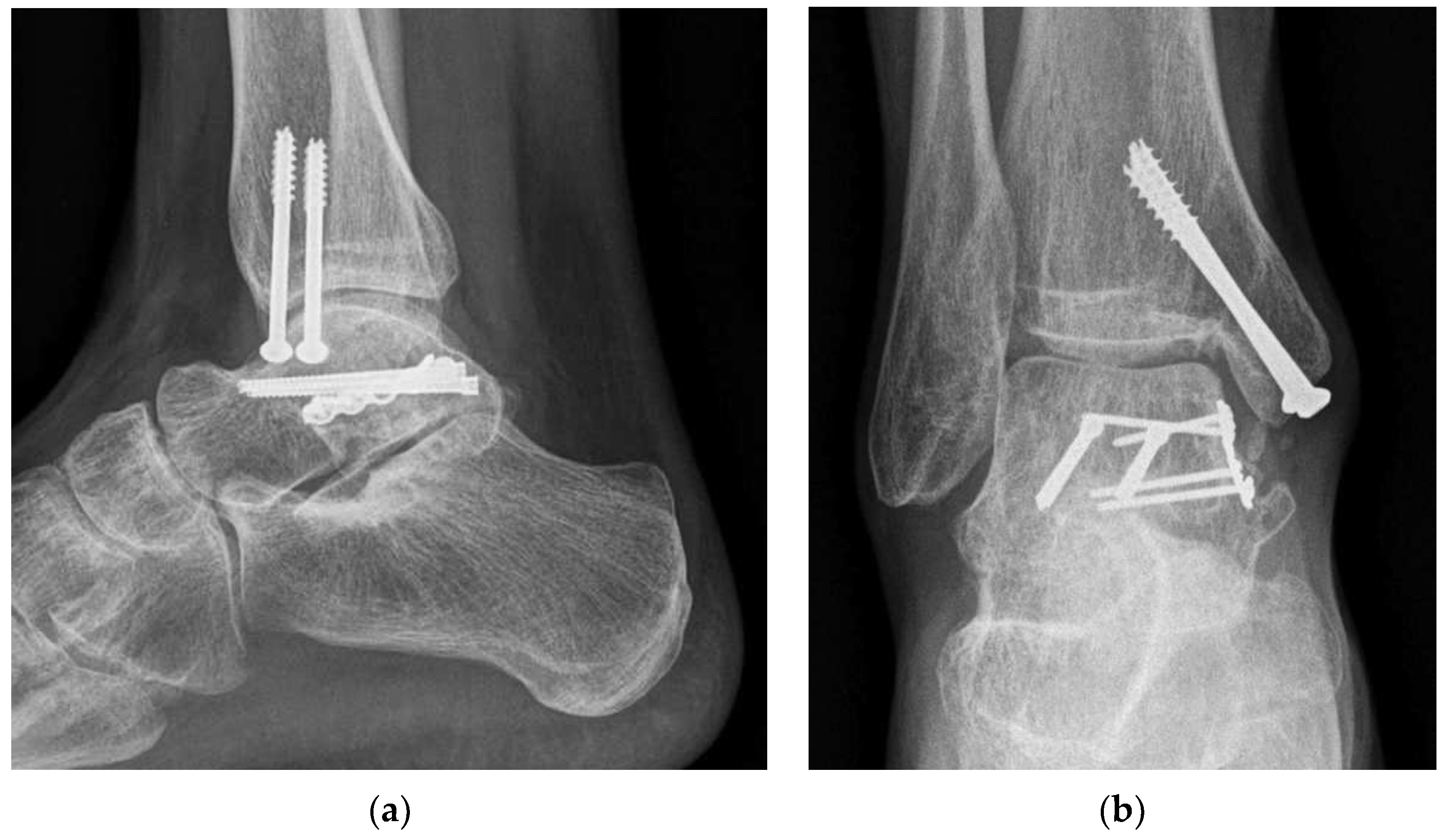
Figure 1 and Figure 2 illustrate a patient who presented with a talus fracture and was treated on the same day by the surgeon on call. CT scans showed a comminuted fracture of the posterior body of the talus (Figure 1). A medial approach was carried out, and a medial malleolar osteotomy at the tibia was performed to confer adequate exposure of the talus. The medial malleolus osteotomy site was repaired using cannulated screws. Small fragments were removed, and the larger fragments were repaired and fixed using a plate and screws (Figure 2). Post-operative radiographs at 10 months showed good healing of the fracture and good hardware position (Figure 3). At 18 months post-op operatively, the patient indicated mild pain during activity and no pain at rest. The patient reported no difficulty or slight difficulty for all activities on the FADI questionnaire, except squatting, which the patient reported as moderately difficult.
4. Discussion
Evaluation of our patients revealed that fractures of the lateral process were not the most common talar fractures caused by snowboarding. It is unclear why complex talus fractures were more prevalent than the typical lateral process of the talus. The level of energy involved in the injury process may have played a significant role. Lateral processes of talus fractures have typically been associated with lower-energy mechanisms as compared with high-energy talar neck and body fractures [15]. In this series, the patients were described as traveling at high speeds when they sustained their injury. This invariably contributed to the increase in more severe talus injuries. Additionally, because lateral process fractures tend to be confused with ankle sprains, snowboarders may have presented to an orthopedist located near their residence in a delayed fashion [16]. It is important that physicians maintain high suspicion for a talar fracture when a snowboarder presents with ankle pain.
The appearance of more severe ankle injuries is likely multifactorial. The literature supports the mechanism of injury as an important variable in determining the severity of the injury [17,18]. The continued popularity of snowboarding among a wide range of participants, along with high speeds of descent, terrain parks, and evolving equipment, may have an influence on these injuries.
Recent studies have evaluated the relationship between terrain parks and risk of injury [6,19], although have been unable to conclude whether increased time spent in the terrain park, where features have been specifically made for jumping purposes, increases the risk of injury. In addition, parks do not eliminate the opportunity to take jumps outside the terrain park. Establishing a relationship between parks and injury is therefore challenging.
Soft and hard boots are used while snowboarding. Previous studies examined the distribution of injuries with these equipment differences [2,18]. Hard boots appeared to have a protective factor for ankle fractures, excluding lateral process of the talus fractures. Soft boots demonstrated a significantly higher rate of lateral process fractures as compared with hard boots. More studies on biomechanical alignment of the foot and ankle can better explain the pattern of injury that we saw in our patient population.
Our study is limited in that it was a retrospective study with only a small number of patients. Our facility serves a highly transient population: the local residents and visitors to our small ski town. We are not always able to follow up patients two years after surgery, which is the preferred time to determine the incidence of osteoarthritis or avascular necrosis. However, Vallier et al. retrospectively reviewed talar neck fractures and found that avascular necrosis occurred within the first 10 months after the injury with a mean of 19 weeks [20]. The mean interval from date of surgery to the time of FADI questionnaire follow-up was 33 months, suggesting that avascular necrosis would have already been diagnosed in those patients who participated.
5. Conclusions
This case series is the first to describe a high prevalence of talar head/neck and body fractures in snowboarders. Although many studies have highlighted lateral process fractures of the talus and their association with snowboarding injuries, we observed that these injuries can include more complex injury patterns related to higher-energy mechanisms. Increasing the awareness of these types of injuries in snowboarders for emergency providers and the orthopedic community should aid in more timely diagnoses and treatments, as well as help improve outcomes.
Author Contributions
Conceptualization and supervision, K.E.S.; investigation, data curation, and writing: N.M.L. and C.P.-G.; methodology, validation, and formal analysis: B.L.S.; writing—review and editing. A.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Barton Institutional Review Board (protocol number 11-108, approved October 2011).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Number of Participants in Snowboarding in the United States from 2007–2017. Available online: https://www.statista.com/statistics/191319/participants-in-snowboarding-in-the-us-since-2007/ (accessed on 8 May 2022).
- Kirkpatrick, D.P.; Hunter, R.E.; Janes, P.C.; Mastrangelo, J.; Nicholas, R.A. The snowboarders foot and ankle. Am. J. Sports Med. 1998, 26, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Young, C.C.; Niedfeldt, M.W. Snowboarding injuries. Am. Fam. Physician 1999, 59, 131–136,141. [Google Scholar] [PubMed]
- Seleznev, A.; Shah, N.V.; Desai, R.; Le, C.; Cleary, P.; Naziri, Q.; Basu, N.N.; Freeman, B.J.; Urban, W.P.; Newman, J.M. Trends of snowboarding-related fractures that presented to emergency departments in the United States, 2010 to 2016. Ann. Transl. Med. 2018, 6, 200. [Google Scholar] [CrossRef] [PubMed]
- Sacco, D.E.; Sartorelli, D.H.; Vane, D.W. Evaluation of alpine skiing and snowboarding injury in a northeastern state. J. Trauma 1998, 44, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Endres, N.K.; Johnson, R.J.; Ettlinger, C.F.; Shealy, J.E. Snowboarding injuries: Trends over time and comparisons with alpine skiing injuries. Am. J. Sports Med. 2012, 40, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Sarrafian, S.K. Anatomy of the Foot and Ankle: Descriptive, Topographic, Function, 2nd ed.; J. B. Lippincott: Philadelphia, PA, USA, 1993. [Google Scholar]
- Browner, B.D. Skeletal Trauma: Basic Science, Management, and Reconstruction; Saunders: Philadelphia, PA, USA, 2003. [Google Scholar]
- Kramer, I.F.; Brouwers, L.; Brink, P.R.; Poeze, M. Snowboarder’s ankle. Case Rep. 2014, 2014, bcr2014204220. [Google Scholar]
- Von Knoch, F.; Reckord, U.; von Knoch, M.; Sommer, C. Fracture of the lateral process of the talus in snowboarders. J. Bone Jt. Surg. Br. 2007, 89, 772–777. [Google Scholar] [CrossRef] [Green Version]
- Heckman, J.D.; McLean, M.R. Fractures of the lateral process of the talus. Clin. Orthop. 1985, 199, 108–113. [Google Scholar] [CrossRef]
- Reber, P.; Steiner, W.; Noesberger, B. Fractures of the lateral process of the talus. Unfallchirurg 1991, 94, 153–156. [Google Scholar]
- Fournier, A.; Barba, N.; Steiger, V.; Lourdais, A.; Frin, J.M.; Williams, T.; Falaise, V.; Pineau, V.; De Chou, E.S.; Noailles, T.; et al. Total talar fracture—Long-term results of internal fixation of talar fractures. A multicentric study of 114 cases. Orthop. Traumatol. Surg. Res. 2012, 98, S48–S55. [Google Scholar] [CrossRef] [Green Version]
- Shakked, R.J.; Tejwani, N.C. Surgical treatment of talus fractures. Orthop. Clin. N. Am. 2013, 44, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Rammelt, S.; Zwipp, H. Talar neck and body fractures. Injury 2009, 40, 120–135. [Google Scholar] [CrossRef] [PubMed]
- Helmig, K.; Treme, G.; Richter, D. Management of injuries in snowboarders: Rehabilitation and return to activity. Open Access J. Sports Med. 2018, 9, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasden, C.C.; McIntosh, S.E.; Keith, D.S.; McCowan, C. An analysis of skiing and snowboarding injuries on Utah slopes. J. Trauma 2009, 67, 1022–1026. [Google Scholar] [CrossRef] [PubMed]
- Bohyn, C.; Flores, D.V.; Murray, T.; Mohr, B.; Cresswell, M. Imaging Review of Snowboard Injuries. Semin. Musculoskelet. Radiol. 2022, 26, 54–68. [Google Scholar] [CrossRef] [PubMed]
- Moffat, C.; McIntosh, S.; Bringhurst, J.; Danenhauer, K.; Gilmore, N.; Hopkins, C.L. Terrain park injuries. West. J. Emerg. Med. 2009, 10, 257–262. [Google Scholar] [PubMed]
- Vallier, H.A.; Nork, S.E.; Barei, D.P.; Benirschke, S.K.; Sangeorzan, B.J. Talar neck fractures: Results and outcomes. J. Bone Jt. Surg. Am. 2004, 8, 1616–1624. [Google Scholar] [CrossRef]
Figure 1.
CT imaging of comminuted talar body fracture in a snowboarder: (a) sagittal CT; (b) coronal CT; and (c) axial CT.
Figure 1.
CT imaging of comminuted talar body fracture in a snowboarder: (a) sagittal CT; (b) coronal CT; and (c) axial CT.

Figure 2.
Intra-operative fluoroscopy images of talar body ORIF utilizing a medial malleolar osteotomy approach: (a) lateral image; and (b) antero-posterior image.
Figure 2.
Intra-operative fluoroscopy images of talar body ORIF utilizing a medial malleolar osteotomy approach: (a) lateral image; and (b) antero-posterior image.

Figure 3.
Radiographs 10 months post-operatively demonstrating complete fracture healing without avascular necrosis: (a) lateral image; and (b) antero-posterior image.
Figure 3.
Radiographs 10 months post-operatively demonstrating complete fracture healing without avascular necrosis: (a) lateral image; and (b) antero-posterior image.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Patient demographic and treatment data.
| PT | Age/ Gender | MOI | TT (min) | Approach | Talus Fx Location | Time to Surgery |
|---|---|---|---|---|---|---|
| 1 | 38 M | hit tree | 78 | Med/Lat | N | same day |
| 2 | 38 M | fall | 110 | Med/Lat | N | same day |
| 3 | 26 F | fall | 127 | Med | B | 1 day |
| 4 | 20 M | fall | 65 | Lat | LP | 1 week |
| 5 | 29 F | fall | 30 | Med | N | same day |
| 6 | 24 M | 60 ft jump | 106 | Med | H | 3 weeks |
| 7 | 24 M | fall | 135 | Med/Lat | N/B/LP | same day |
| 8 | 25 M | fall | 135 | Med/Lat | N/H | same day |
| 9 | 29 M | fall | 33 | Lat | LP | 1 week |
MOI—mechanism of injury; TT—tourniquet time; Med—medial, Lat—lateral. Location of the injury: H—head; N—neck; B—body; LP—lateral process.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Luger, N.M.; Pascual-Garrido, C.; Haus, A.; Swanson, B.L.; Swanson, K.E. Talus Fractures in Snowboarders: A Case Series. Osteology 2022, 2, 106-111. https://doi.org/10.3390/osteology2020012
AMA Style
Luger NM, Pascual-Garrido C, Haus A, Swanson BL, Swanson KE. Talus Fractures in Snowboarders: A Case Series. Osteology. 2022; 2(2):106-111. https://doi.org/10.3390/osteology2020012
Chicago/Turabian StyleLuger, Nancy M., Cecilia Pascual-Garrido, Andrew Haus, Britta L. Swanson, and Kyle E. Swanson. 2022. "Talus Fractures in Snowboarders: A Case Series" Osteology 2, no. 2: 106-111. https://doi.org/10.3390/osteology2020012